
Interventional Cardiologist, CTO-PCI, CHIP, Peripheral vascular disease, acute PE. Views & opinions are my own.
Joined February 2021
- Tweets 2,438
- Following 372
- Followers 1,089
- Likes 3,905
232 Photos and videos












May 16
Ops check and Garmin database updates. #Outreach in Gillette, WY, Philip, SD, and hopefully another site in ND or NE within the next 2-3 months.

2
15
1,478
May 11
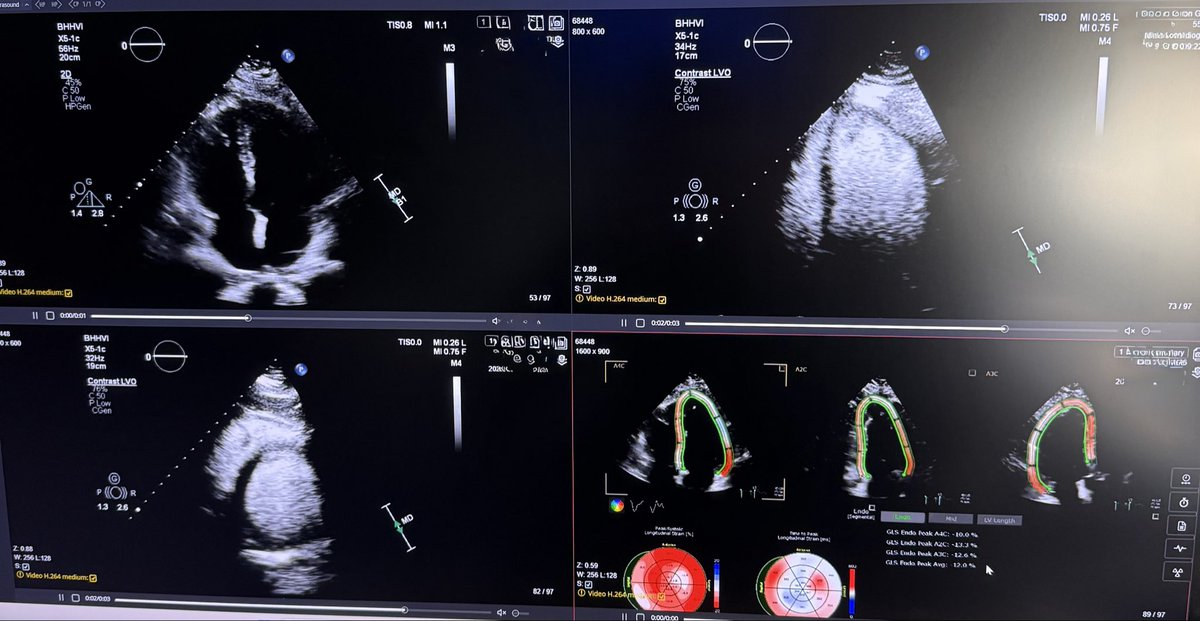
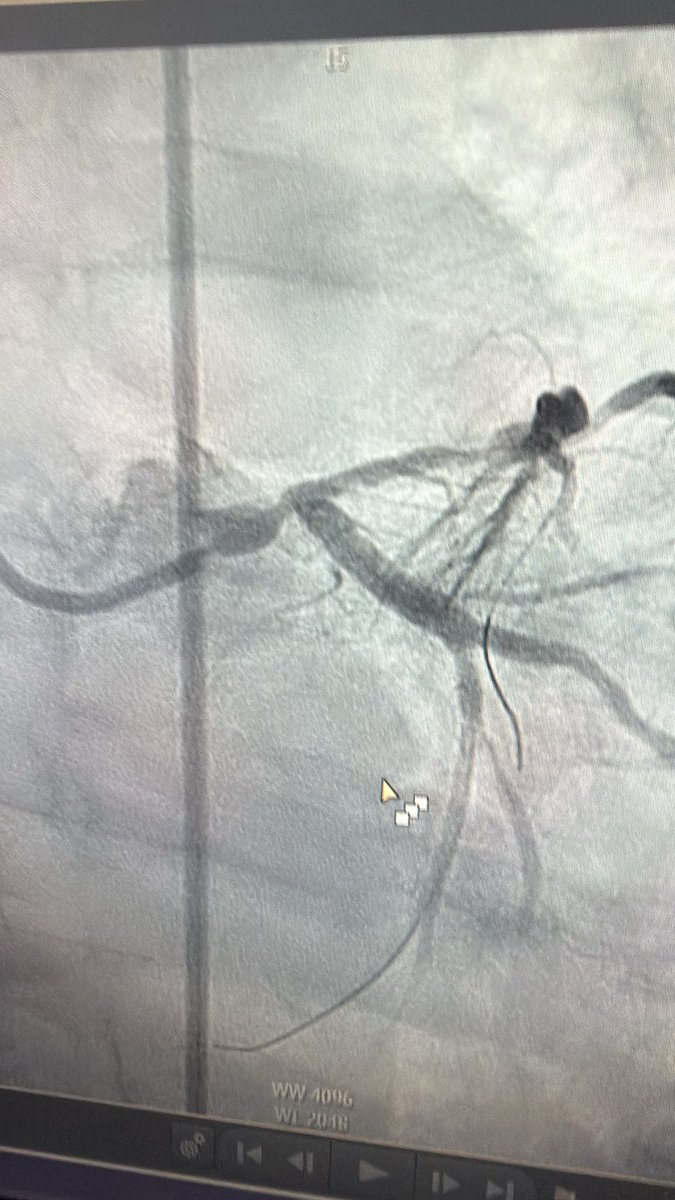
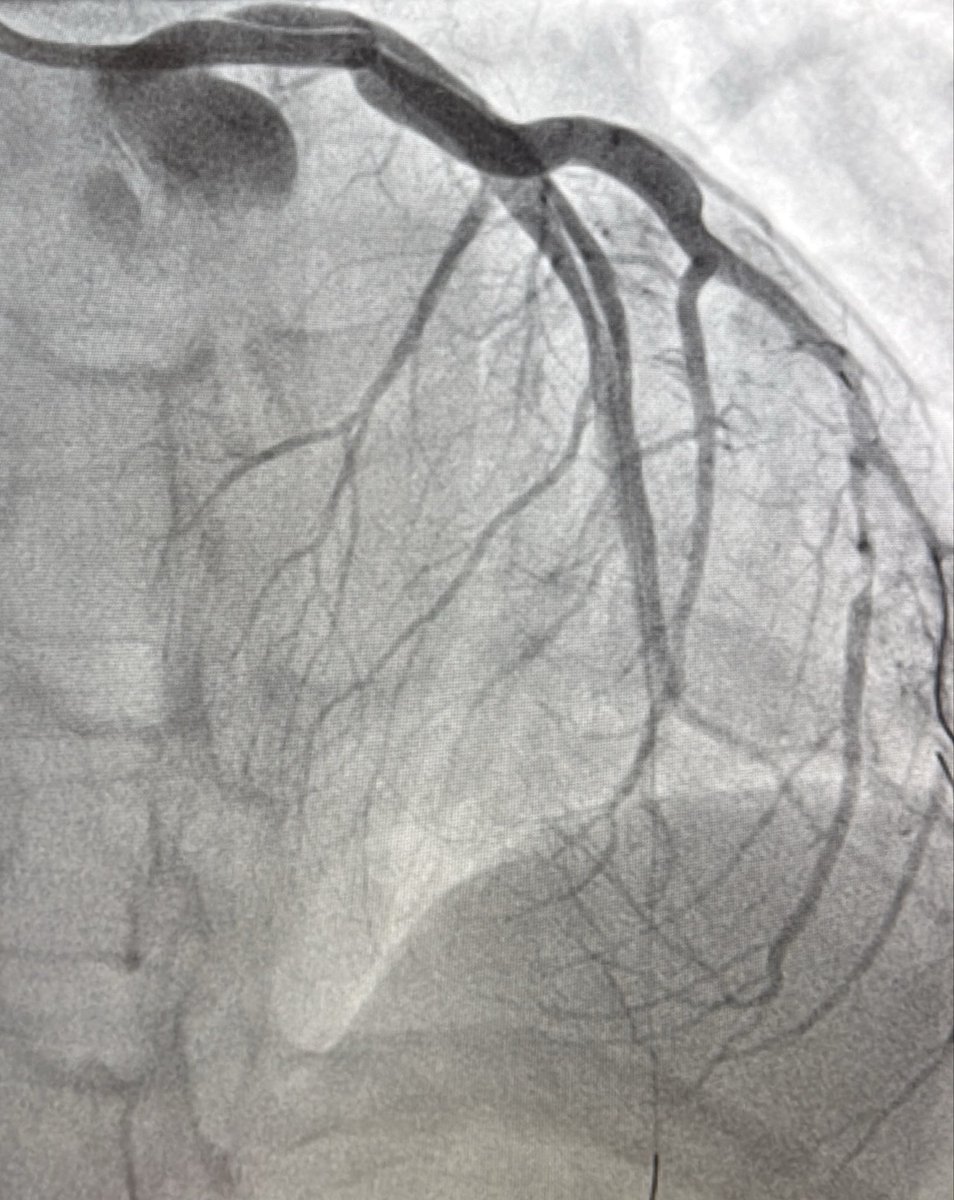
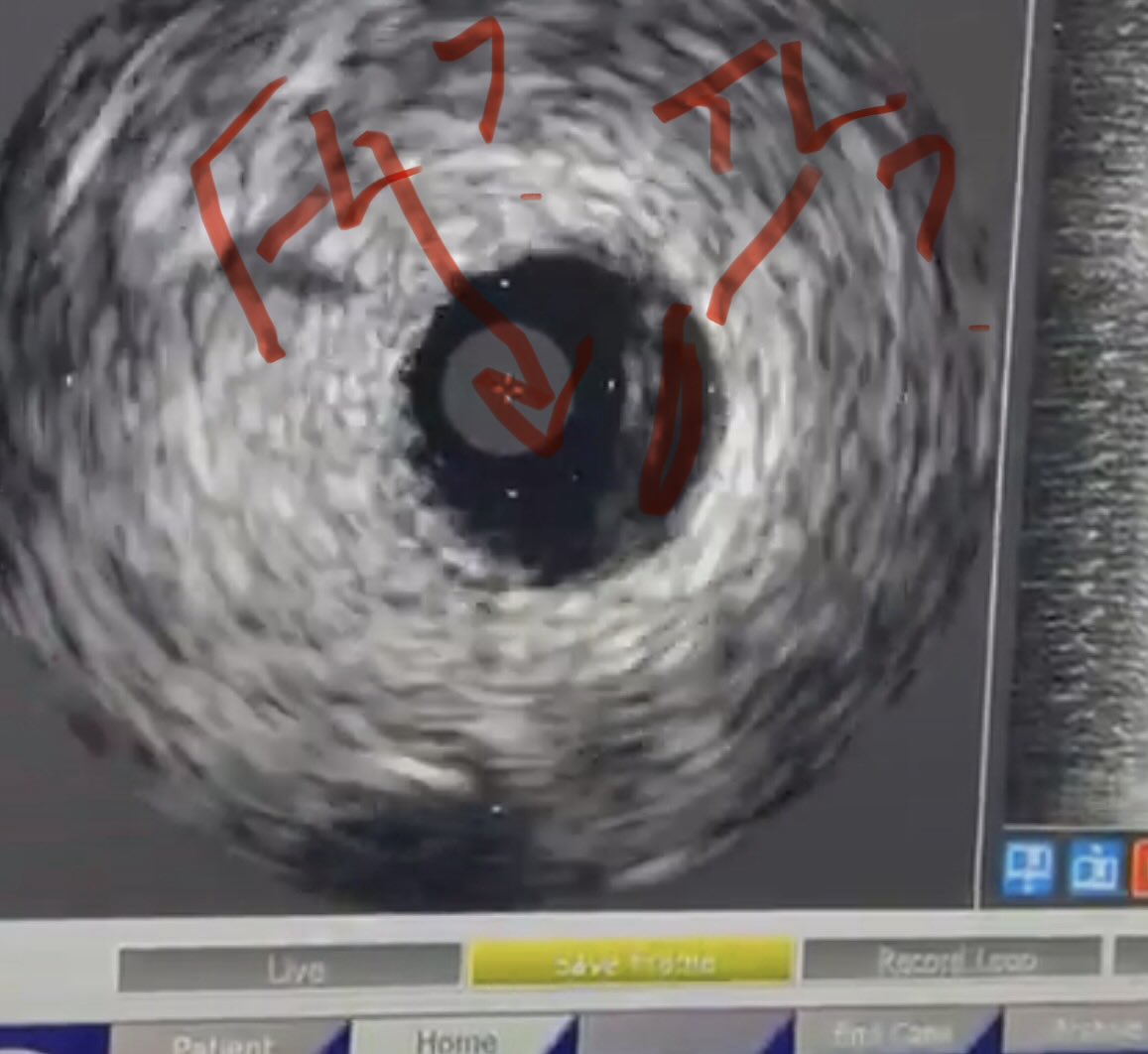
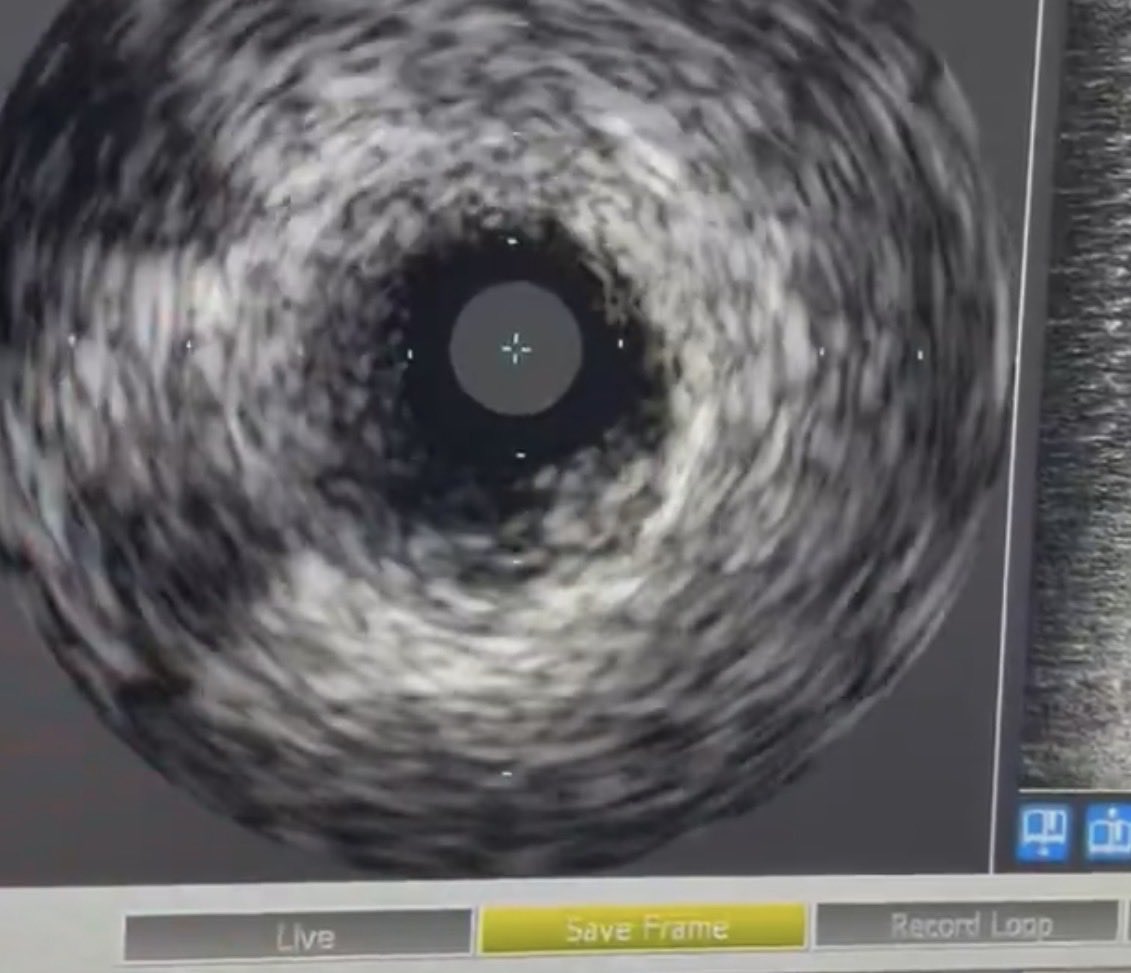
How to manage this? Elderly male, adm for PNA, on Abx, underlying ILD. Trop 6k, EF normal on Echo. EDP = 9. #stringsign @agtruesdell @drAliyor @cardiojaydoc02 @IntervnCardio @TomVargheseJr @DrIHHashmi1 @sandeep_jalli @realarainmd @jl35wilsonMD @Hragy @evandrofilhobr


6
3
16
6,276
May 9
Heading to work—beautiful sunrise. As an outpatient heart & vascular specialist, I travel to maintain acute MI/shock skills. #weekendwarrior
15
2,575
Tom Wilson retweeted

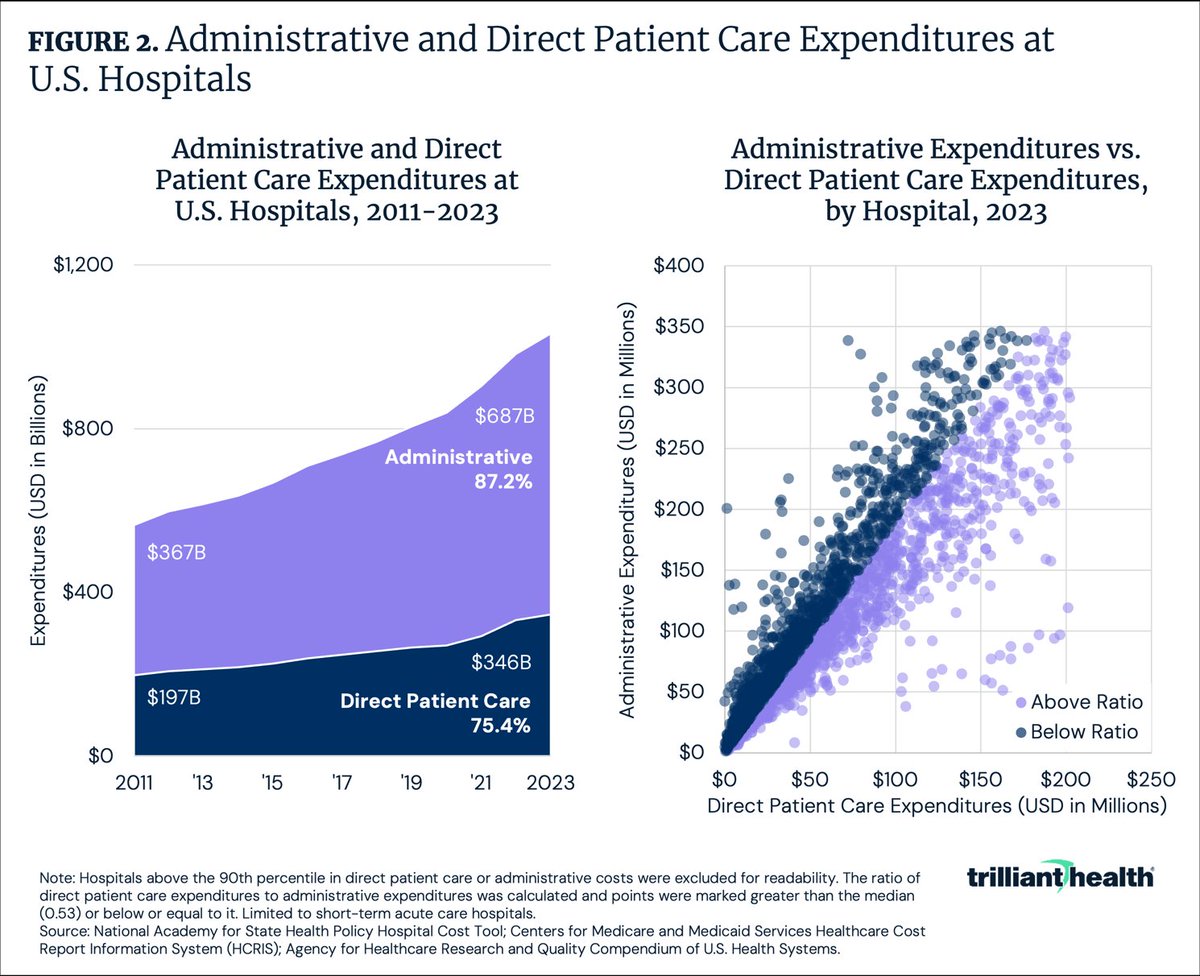
Healthcare administration costs should never exceed patient care costs.
33
177
635
66,460
Tom Wilson retweeted

Mar 20
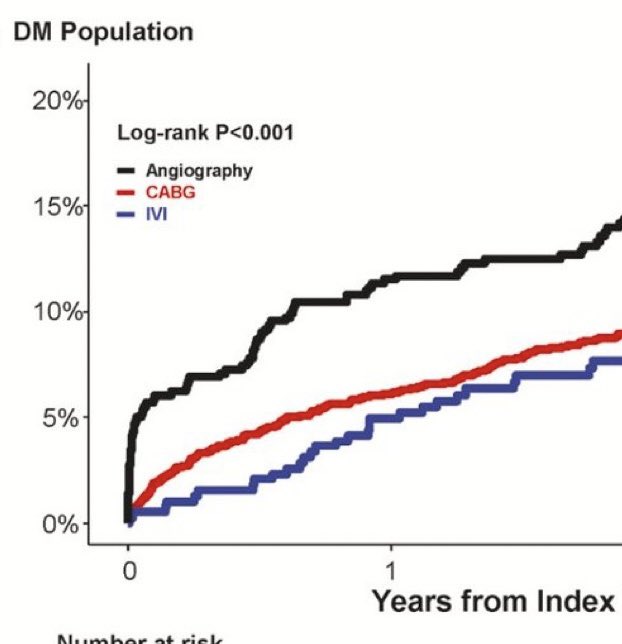
Study conclusion: Angiography guided PCI was associated with significantly higher risk for MACE, However, IVI-guided PCI had comparable risk with CABG in DM patients.
But there's a methodological concern hiding in the study design that the authors didn't discuss:
Immortal time bias.
1/
Mar 20

Thank you for the wonderful explanation. Two (more!) naive questions about immortal time bias.
With re: to this particular analysis, where CABG pts were part of a registry but the PCI cohorts were part of an RCT, is it fair to say that:
1) Immortal time bias should favor PCI (if at all) here since there was no delay to treatment in the CABG arm? Presumably the pts had surgery exactly at the start of the follow up period.
2) Immortal time bias is unlikely to explain the difference bet. angio and IVI guided PCI because the assigned treatment was delivered immediately after randomization?
Perhaps there are other confounding factors to explain the early high event rate in the angio PCI arm? 🤔
3
15
53
22,742
Tom Wilson retweeted

Mar 14
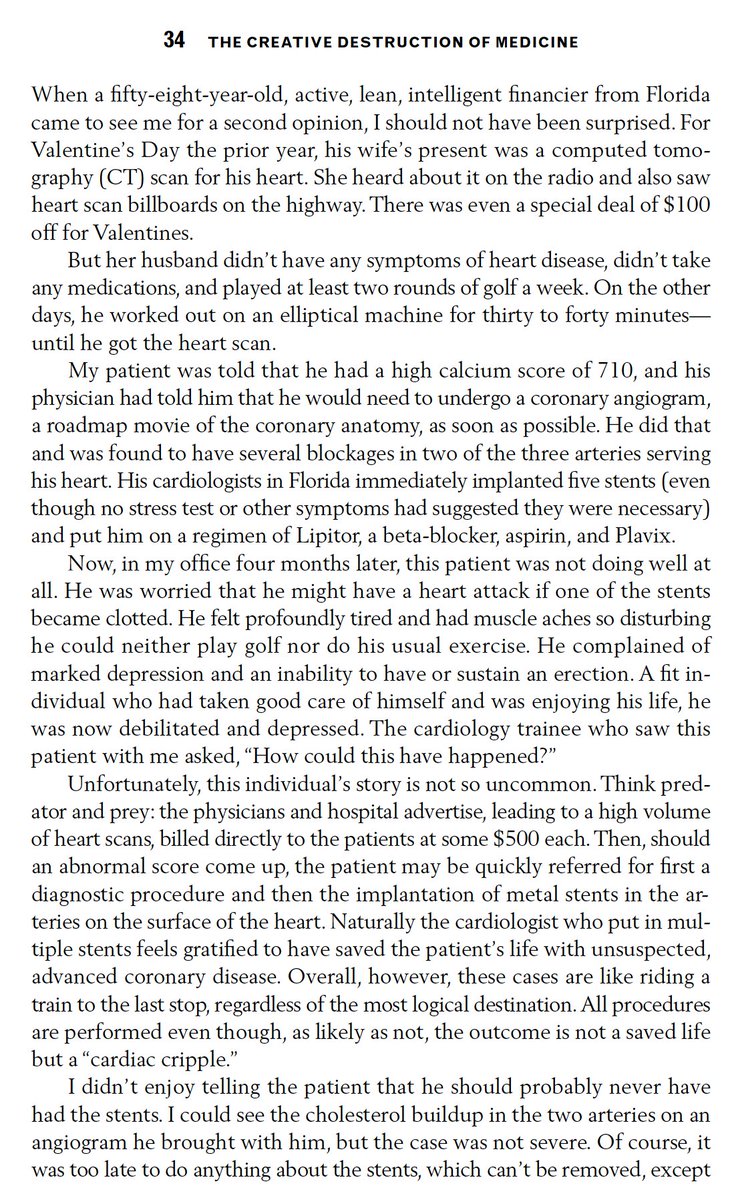
I have been outspoken on the massive misuse of CAC testing for a long time (excerpt from my book in 2011) and have never ordered one.
32
30
126
165,343
Mar 10
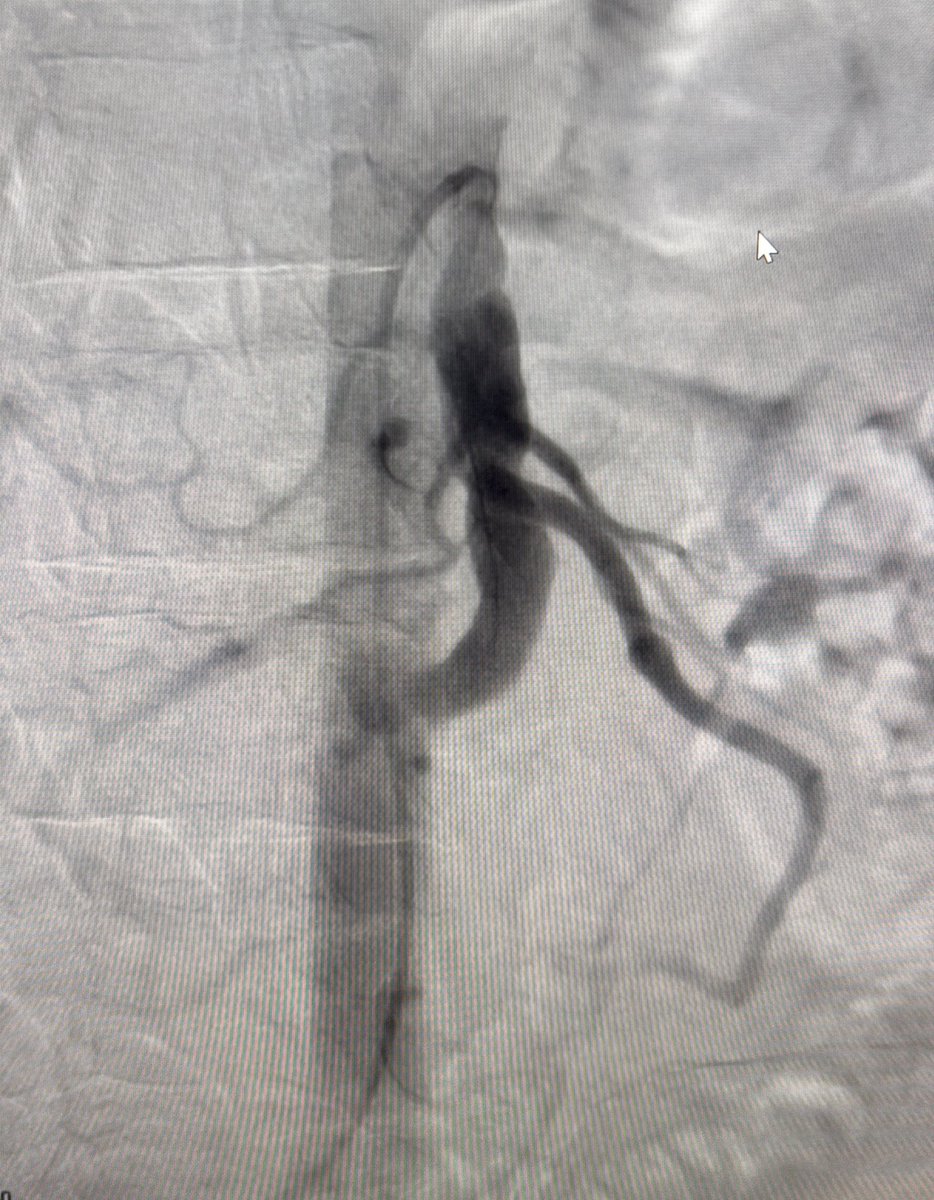
@farkomd @_backtable @JayMathewsMD @DrRajeshG1 @KPujdak @realarainmd @cardiojaydoc02 @SripalBangalore @IR_Doctor 70M, h/o SMA aneurysm w surg repair x2 (2010/18) at tertiary care center. Back w ASx enlarging SMA aneurysm. Next step? Pt has not done well w/ Surgery. Endo option?
10
2
19
2,482
Mar 10
1
1
399
Feb 25
It’s always challenging seeing a patient for the last time. But encouraging to see a supportive and loving family helping a mother live graciously outside of a nursing home.
429
Feb 17
#cardiotwitter @cingolani_oscar @cardiojaydoc02 @CMichaelGibson @JayMathewsMD @AntoniousAttall @SrihariNaiduMD 60s Male see on “urgent” basis. PA did CAC—6k. Told the patient “3000 in the widowmaker.” Said Cath was needed. No clear Sx, was told to cancel Vacation w friends. Now I tell him at mos one could argue a stress test could be ordered. Had FHx as well. Now I’m accused of “not doing enough” after spending 30m explaining everything about a CAC.
17
6
63
29,406
Tom Wilson retweeted
Feb 9
"The term [provider] should not be used to describe physicians, nor should physicians use it to describe themselves, their team members, or their trainees."
acpjournals.org/doi/10.7326/… @AnnalsofIM @ACPIMPhysicians
92
416
1,682
286,603
Jan 27
1st RDN case in South Dakota, MT, WY. Resistant HTN is a killer. Lowering SBP by 10 mmHg makes a difference! Why hasn’t this become more mainstream? Reimbursement in all likelihood. Thank you @MedtronicCRDN. Simple, easy, quick. Both myself & @jl35wilsonMD at Black Hills Heart & Vascular are making 🌊. Thank you to the team at BHSH here in Rapid City, SD.

3
2
20
1,925
27 Nov 2025
Tyler Childress, Gavin Adcock, Tucker Westmore headlining the TG playlist tonight. What else to add? @jl35wilsonMD @txsportsdoc @Allison_Dupont @drjohnm @DrJayMohan @AntoniousAttall @AndrewJSauer
1
8
1,619
Tom Wilson retweeted

14 Nov 2025
🚀 Calcium Score & CCTA: Key Highlights from the 2025 AHA Scientific Statement (DOI: 10.1161/CIR.0000000000001394)
Non-obstructive CAD in Chest Pain Patients
🧊 1. CAC = Atherosclerotic Burden, Not Just a Number
CAC is one of the strongest predictors of future ASCVD risk—better than biomarkers or stenosis alone.
📉 CAC = 0 → high NPV for obstructive CAD (but not zero risk: ~10% still have non-calcified plaque, especially if young or high-risk).
🔥 CAC ≥1000 = extreme risk → annual CV mortality similar to 2ndry prevention populations.
📊 CAC → intensity of preventive therapy: from lifestyle (CAC 0) → to statins (CAC ≥100) → to high-intensity LLT aspirin (CAC ≥300).
🧮 2. CAC for Risk Upgrading & Therapy Decisions
CAC ≥100 or ≥75th percentile supports starting statins even in borderline/intermediate-risk patients.
- hidden high-risk phenotypes (eg, DM or preDM patients with CAC ≥100).
🌈 CAC from non-gated PET/SPECT CT is increasingly used and correlates well with dedicated CAC scans.
🫀 3. CCTA: The New Backbone of Chest Pain Evaluation
The 2021 Chest Pain Guidelines expanded CCTA → leading to a surge in detecting nonobstructive CAD (NOCA).
CCTA is essential because:
- plaque beyond the lumen (including noncalcified plaque).
- vessels down to ~2 mm (even smaller with photon-counting CT).
- high-risk plaque features (LAP, positive remodeling, spotty calcification).
👁️ CCTA reveals that up to 50% of symptomatic patients have NOCA.
🧨 4. High-Risk Plaque on CCTA = High Future Event Risk
High-risk markers include:
📦 High total plaque volume
🟣 Low-attenuation plaque (>4%)
➕ ≥2 high-risk features (per CAD-RADS 2.0)
🔥 Pericoronary adipose tissue (PCAT) inflammation
These features predict MI better than stenosis, shifting the paradigm from stenosis-centric to plaque-centric care.
📈 5. CCTA-Based Risk Staging (CAD-RADS 2.0 Plaque Volume)
Stage 0 → no plaque
Stage 1–2 → increasing plaque burden
Stage 3 → high-risk NOCA
🎯 Treatment intensity escalates with plaque volume, not stenosis alone.
🔄 6. CAC CCTA = The Most Powerful Combination
CAC quantifies calcified burden → great for long-term risk and therapy escalation.
CCTA quantifies total plaque (calcified noncalcified) → great for short-term event risk.
💡 7. Why This Matters
Most ACS events originate from nonobstructive lesions.
📢 The statement pushes clinicians to:
Detect early plaque (especially noncalcified).
Classify risk by plaque burden inflammation.
Intensify therapy before stenosis develops.
#PCCT #Atherosclerosis #PhotonCountingCT #CCT #yesCCT
10
150
370
31,090
Tom Wilson retweeted

27 Oct 2025
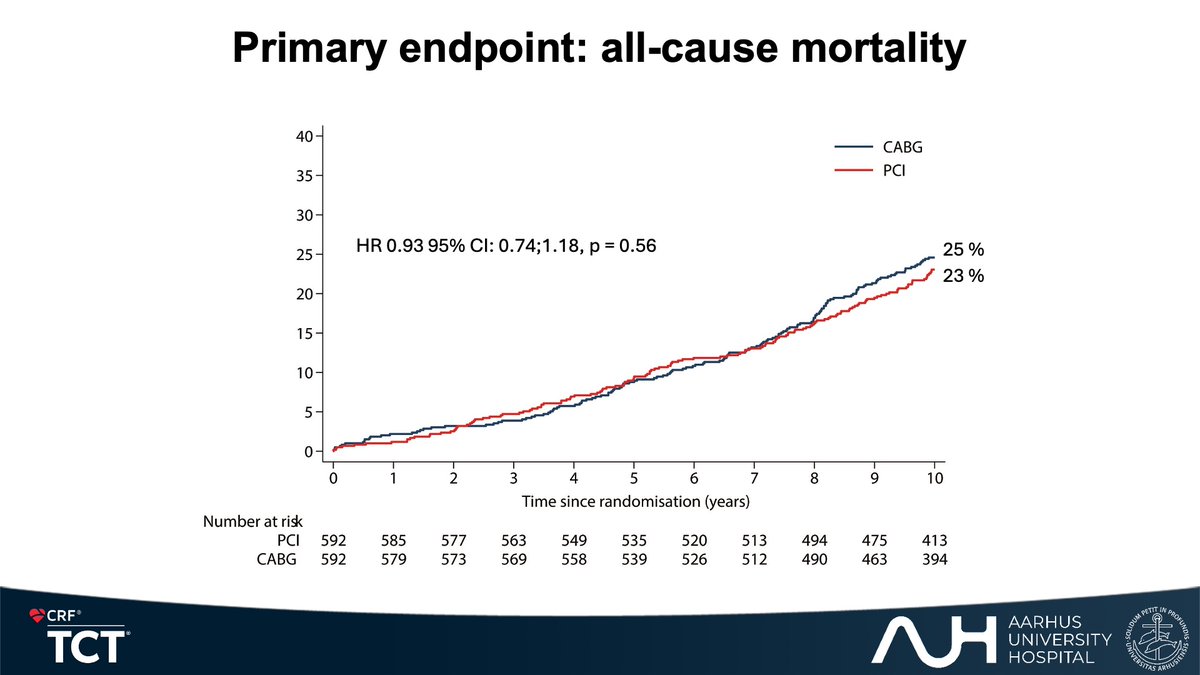
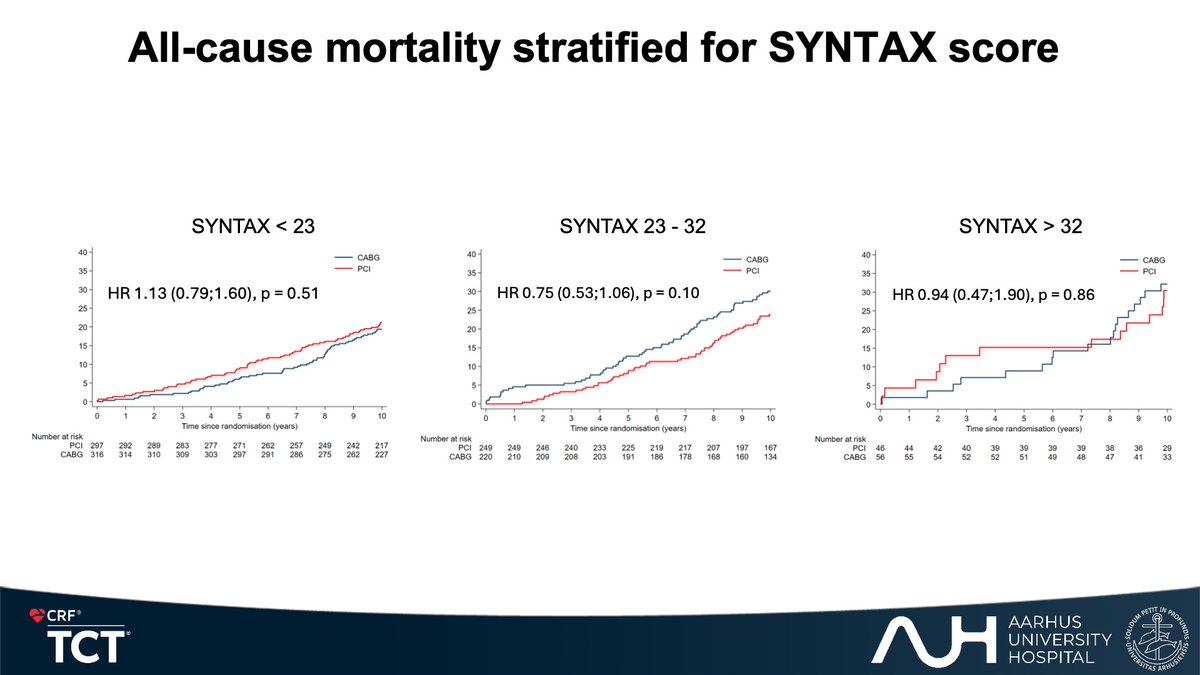
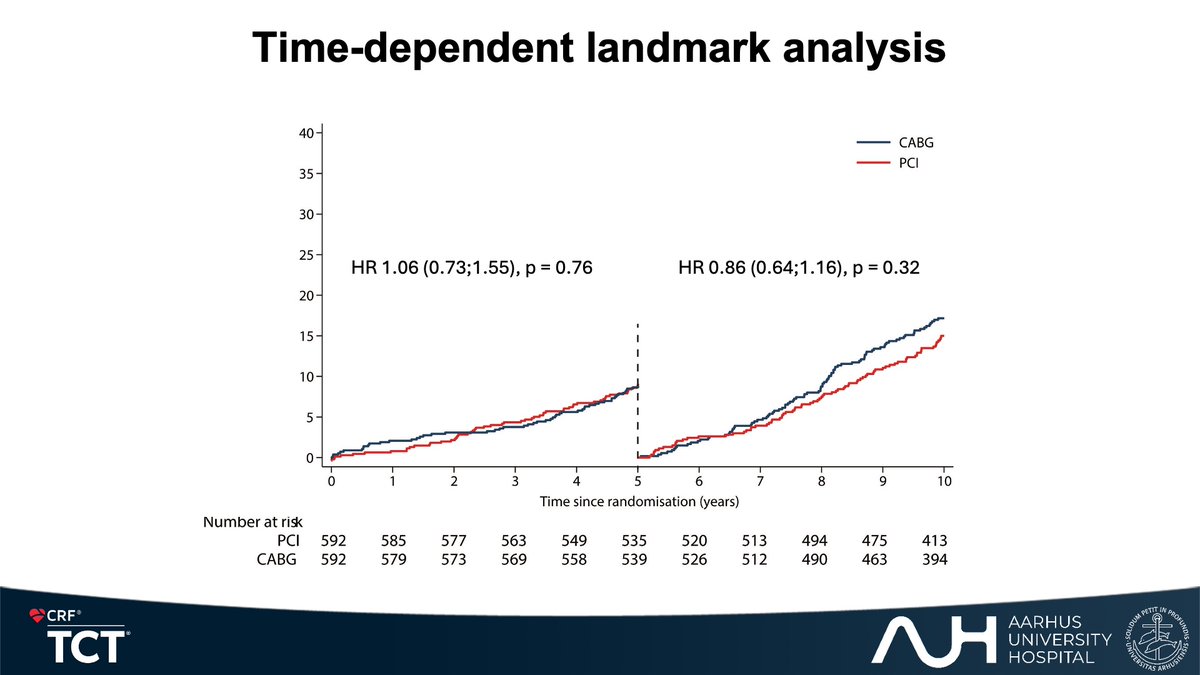
Ten-year outcome in the NOBLE trial
🫀Today, we presented that there is no difference in all-cause mortality ten years after randomization to PCI or CABG in patients with unprotected LMCA disease.
For more info contact @h_evald or me - always eager to interact!
6
24
85
5,978

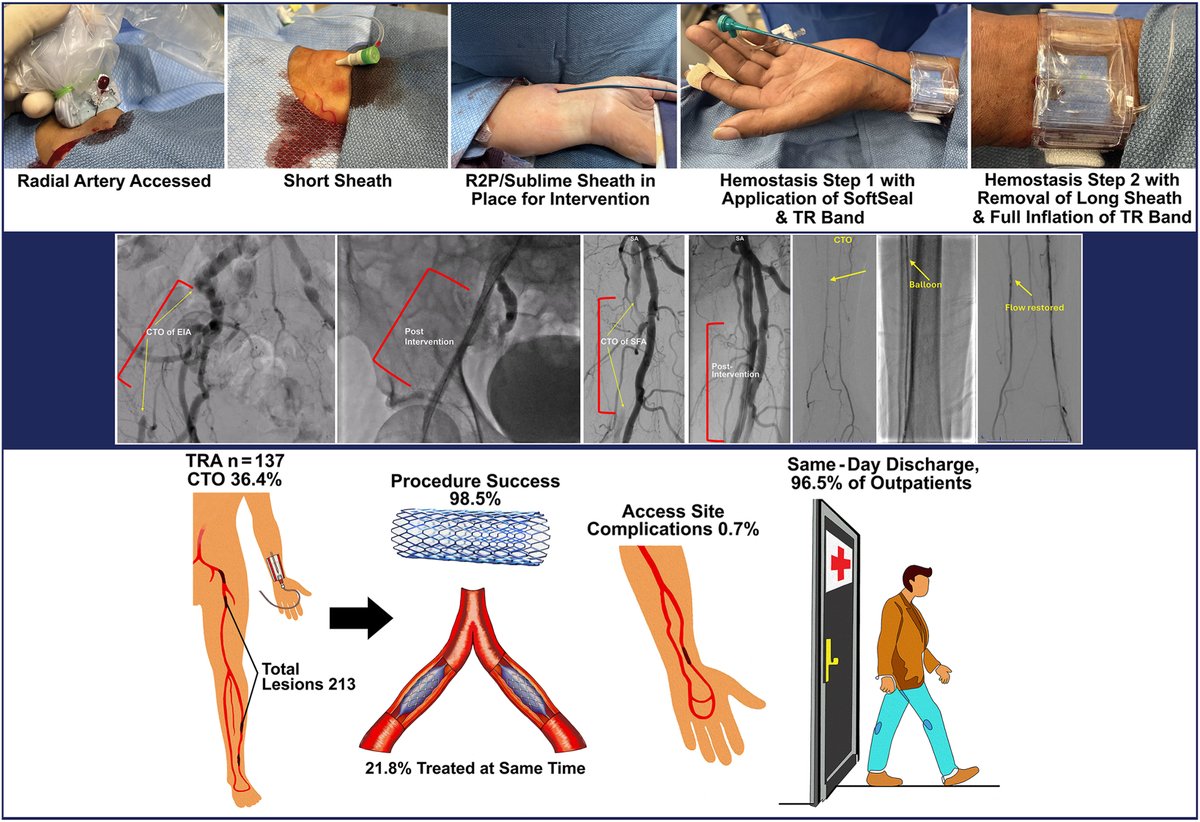
📖#Transradial access is viable & potentially superior alternative to femoral or brachial access for #PVI, offering reduced complication rates and enhanced patient outcomes #RadialFirst
In 137 patients (213 lesions):
✅ 98.5% procedural success
✅ 2.1% complication rate
✅ 96.5% same-day discharge
➡️jscai.org/article/S2772-9303…
@fuadfehmi @MohamedOsmanMD
#PeripheralVascularIntervention
1
19
63
6,067
Tom Wilson retweeted

15 Sep 2025
#CTO #HDR #MAT #MHA #singleaccess #EuroCTO #EUROACTOS2025
Live CTO CASE. RCA CTO How to do #HDR .
Pilot 200→HDR→sionblack→HDR→sionblack→HDR→sionblack→CB Stent DCB
@realarainmd @cto_chip_japan @DaitaroK @calcbreaker @UmihikoKaneko @SKuramitsu0511 @tadano98 @rotamonster @OpolskiMP @jcspratt @KambisMashayek1 @LAzzaliniMD @AgostoniPF @skat_ct @mornei2011 @uziyahya46 @DrBIqbal @Bernard_TW_Wong #MedTwitter @akbarul @K_DeSilva @evandrofilhobr @MichaelMegalyMD @asaadnakhle @SCVC2023 @girishviswa1 @baijazvascular @ErwMulia @jbspadoni @GTawade84 @drAliyor @SandyCTO #cardiotwitter @PCRonline @SCAI @ikki1127 @CtoEuro @SPyxaras @JuradoRomanAl @JiunnWen_Lin @MLCTOAcademy @shci_sec @drdharmarajk @sapporohunt @ogoktekin
7
12
60
4,871
3 Sep 2025
Where can I find a high quality white coat? Most (nearly all) are polyester, of poor quality, and uncomfortable. I don’t use them every day but still need one. #cardiotwitter
1
4
642
Tom Wilson retweeted

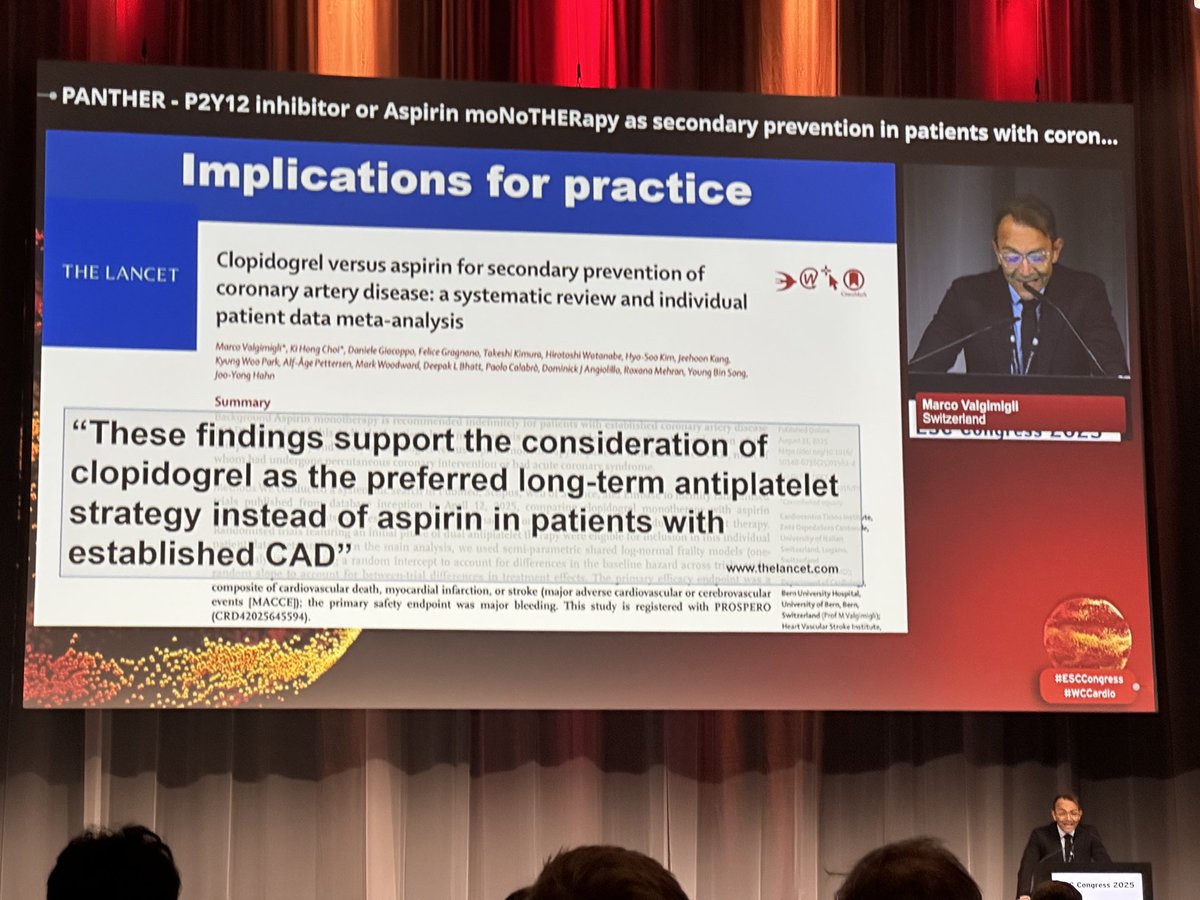
1 Sep 2025
Practice-changing meta-analysis presented by @vlgmrc at #ESCCongress2025 and published in @TheLancet.
8
81
304
36,249
15 Aug 2025
Morning commute. 0500 departure. Always a privilege to watch the sunrise at FL210. Maybe catch the sunset on the way back home?

1
5
723