
Systematic challenger of metabolic & cardiovascular misinformation. Bradford Hill criteria over cherry-picked studies. RCTs over testimonials.
Joined August 2022
- Tweets 14,438
- Following 516
- Followers 861
- Likes 7,073
Photos and videos
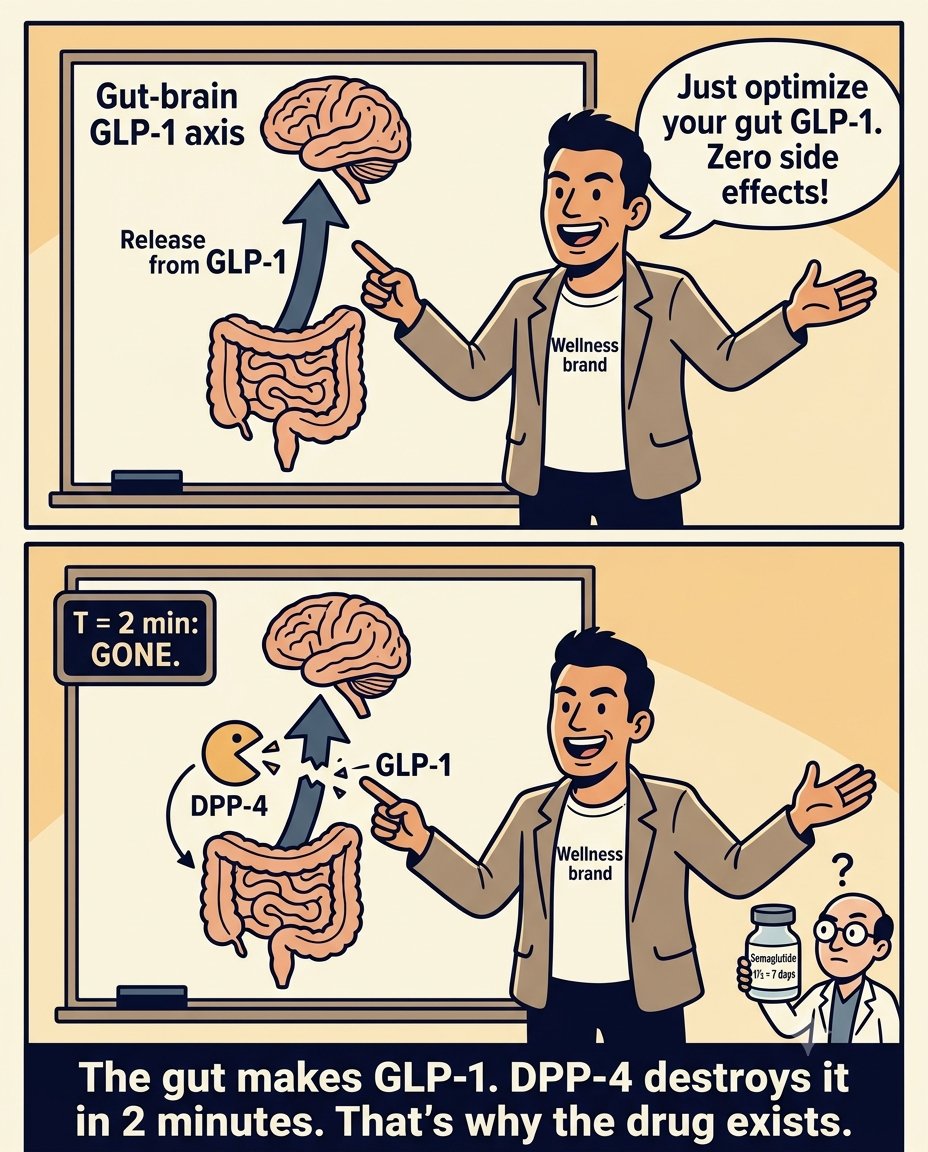
I cant help but think why grifters think we are stupid.
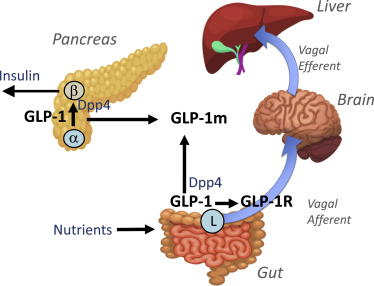
The diagram labels DPP-4. That is the enzyme that degrades endogenous GLP-1 within one to two minutes of release.
Semaglutide has a seven-day half-life. It was engineered to survive DPP-4 degradation. That is the entire mechanism of the drug class.
The gut already produces GLP-1. The problem is not production. It is that the molecule disappears before it can do sustained work.
Classic self-refutation.
Optimizing gut health has real benefits. Zero cardiovascular outcome data showing it closes the gap that 17,604 patients in SELECT closed.
Fun times!
The diagram explained why the drug exists.
11h

I can't help but think, if GLP-1 drugs are excellent for preventing addiction, and we make GLP-1 in our gut, I wonder how much better our own GLP-1 would serve us if the gut producing it was actually healthy. Zero side effects all the benefits from optimal gut health on top.
1
53
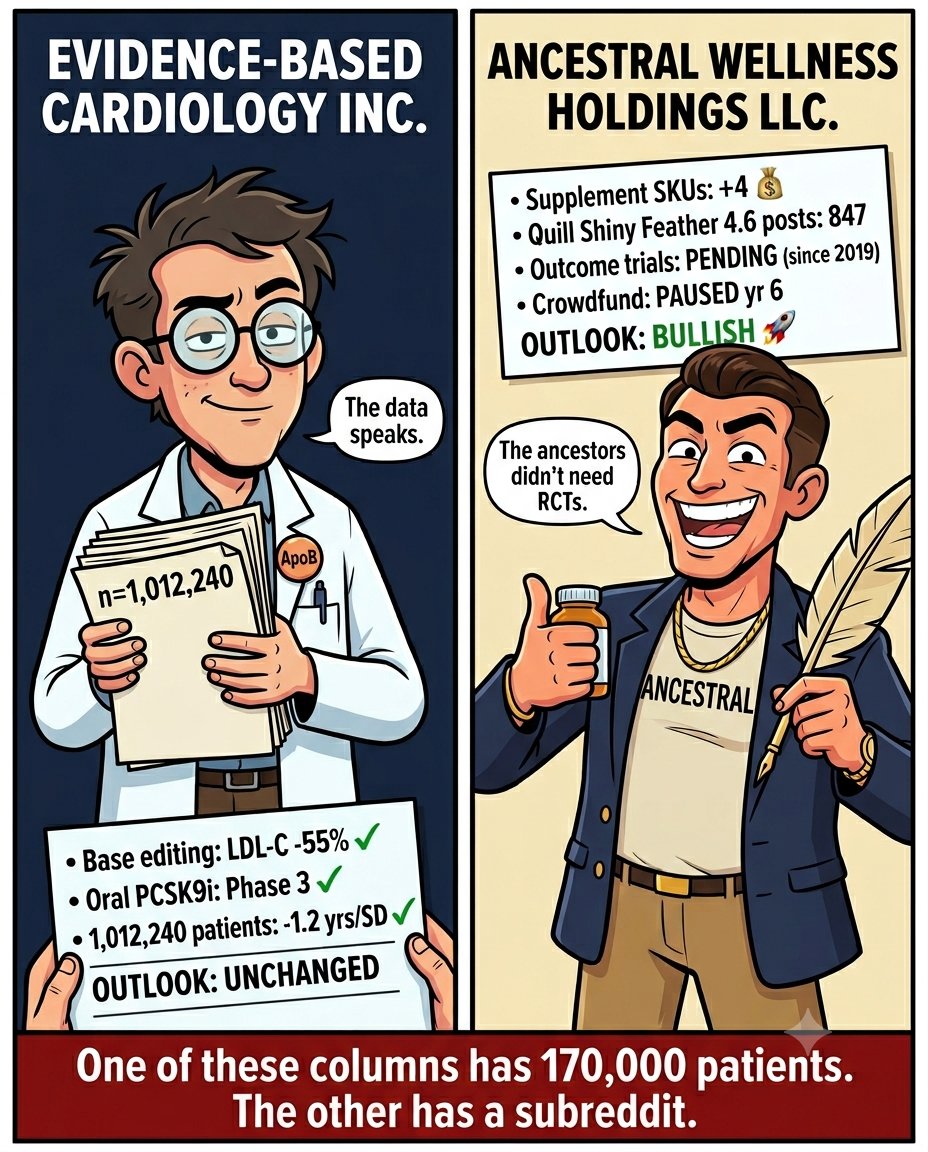
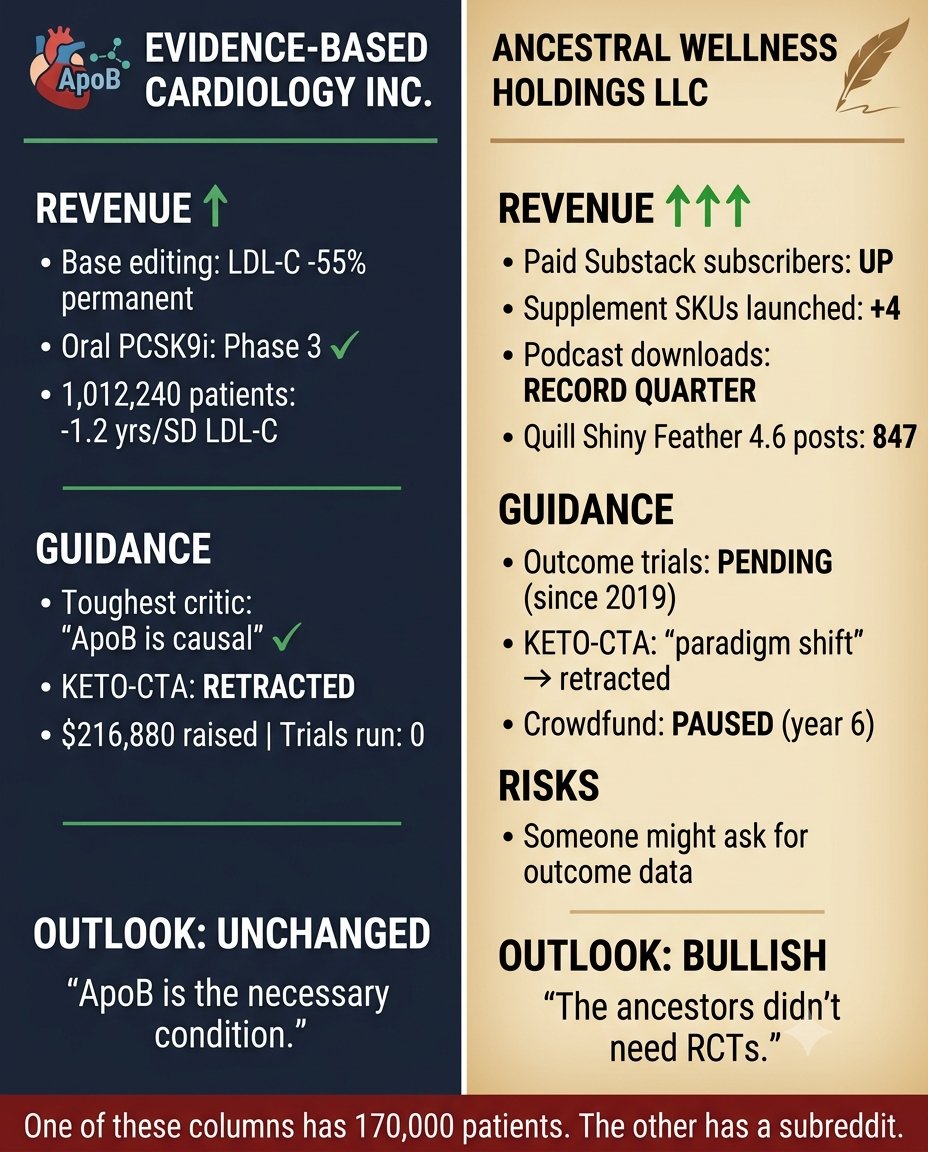
The preliminary Q2 learnings report is in.
Revenue: the science moved. A single dose of base editing lowered LDL-C 55% permanently in humans. An oral PCSK9 inhibitor reached phase 3.
A Mendelian randomization study of 1,012,240 people found every standard deviation increase in genetically proxied LDL-C costs 1.2 years of life.
A meta-regression of 17 primary prevention trials found the 5-year number needed to treat is constant across risk strata. The modest benefit objection died quietly.
CAC=0 converted to CAC>0 in 31% of rescanned patients over 5 years in NATURE-CT. The natural history does not wait.
Guidance: the adversaries moved too. The most technically rigorous critic in the space acknowledged ApoB is in the causal pathway. A cardiologist who spent months on the endothelial dysfunction question acknowledged the particle burden argument is correct. The KETO-CTA paper was retracted. The carnivore community's cardiovascular outcomes crowdfund raised $216,880 over six years and ran zero trials.
The money materialized. The trial vaporized.
Risks to outlook: precision is a discipline, not a destination. There were moments this quarter where figures were deployed without their confidence intervals. Where mechanisms were described at a level of simplicity that invited correction. Where terminology was imprecise enough to hand an adversary a legitimate point.
Each one was caught. Each one sharpened the argument. Can always do better.
Outlook: unchanged. ApoB particle burden is the necessary condition for atherosclerotic plaque. The evidence has not moved. The precision around deploying it has.
That is the job.
1
6
249
Keto is for quitters.
People will need a lifetime dietary protocol to maintain the body because the body is from the mind. Living a lie. Can be done with lifetime discipline.
This is the argument applied to GLP-1s. It works equally well on keto.
Which is odd, because the people making it seem not to notice.
The difference is not the logic. The difference is that one of these has 17,604 patients and a 20% reduction in major adverse cardiovascular events in a randomized controlled trial.
The other has a subreddit.
Never give up. Never surrender.

Glp1s are for quitters. People will need a lifetime prescription to maintain the body because the body is from the mind. Living a lie. Can be done with lifetime drug
1
8
513
The wellness influencer who announces they did not use AI to write their post wants credit for using worse tools.
Think about what that argument actually is.
Would you prefer a doctor who tells you: "Good news. Today we are not using the MRI. I am going to feel around a bit to see how your cancer is progressing. Old school. Like the ancestors."
You would fire that doctor.
Using the best available tools to find, organize, and communicate evidence is not a weakness. It is the job.
The question was never what wrote the argument. The question is whether the argument is true and whether the evidence behind it would survive scrutiny.
17,604 patients in SELECT. 170,000 patients across 27 statin trials. 27,564 patients in FOURIER.
Those trials do not care what tool assembled the post citing them.
Neither should you.
What the quill-pen crowd never discloses is the outcome data for whatever they are selling instead.
That column stays empty regardless of how the post was written.
Choose wisely my friends. Mind the grifters.

2
5
338
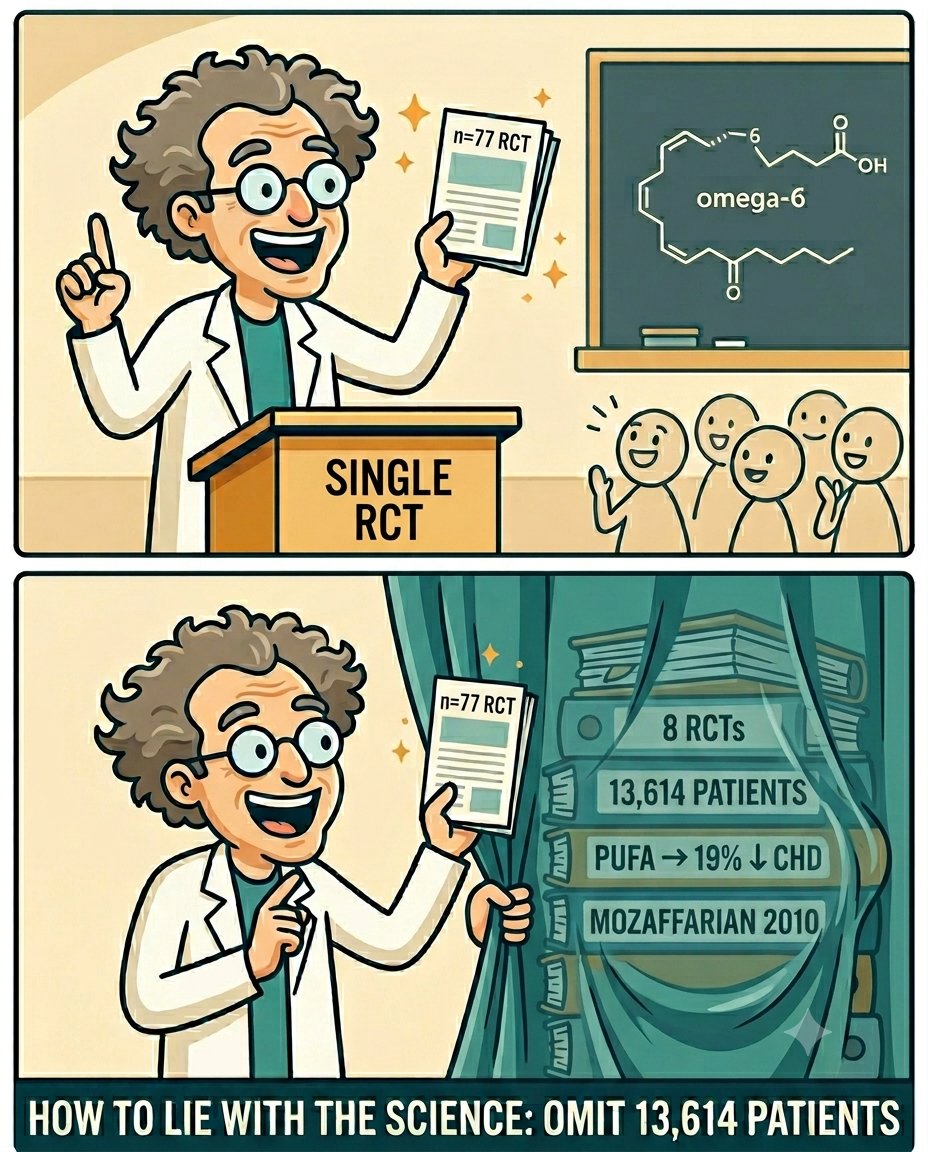
How to lie with the science. Start by omitting 13,614 patients.
@trikomes correctly found the misrepresented Iranian RCT. The Tufts Food Compass ranking Count Chocula above ground beef is embarrassing.
One bad review paper is the motte. The dietary fat evidence base is corrupt. That is the bailey he is selling.
He built it by leaving out eight randomized controlled trials and 13,614 patients: PUFA replacing saturated fat, 19% fewer coronary heart disease events.
It was not cited to launder Count Chocula. A PhD byline on a scroll-stop meme is still a scroll-stop meme.
Classic @trikomes.
Bad scholarship inside an institution is not the same as every outcome trial that institution touches being poisoned. The omission is how you get from one to the other.
Never give up. Never surrender.
2
5
382

Jun 13
@MichaelAlbertMD just published the cleanest natural-history illustration of cumulative LDL loading I have seen in years.
205 untreated adults. Acceptable LDL. Half with zero calcium. Five years later: plaque doubled, low-attenuation plaque up from 9% to 23%, and the share with a zero calcium score quietly falling.
His close: "I would rather treat the slope than admire the snapshot.
Read it.
Link in reply.
1
13
345
2
4
153
Jun 13
"What's the point of your fancy smancy ApoB drivel if it can't even improve all cause mortality???"
Sounds great right? I would buy it. Here's why you should not.
It's not rigor. It is a moving goalpost dressed as a threshold.
Individual cardiovascular trials are not powered to detect an ACM signal. Detecting cause-specific cardiovascular benefit requires roughly 40,000 patients. Detecting all-cause mortality benefit requires over a million.
When a 27,000-patient trial does not show ACM significance, that is a sample size problem, not a null finding.
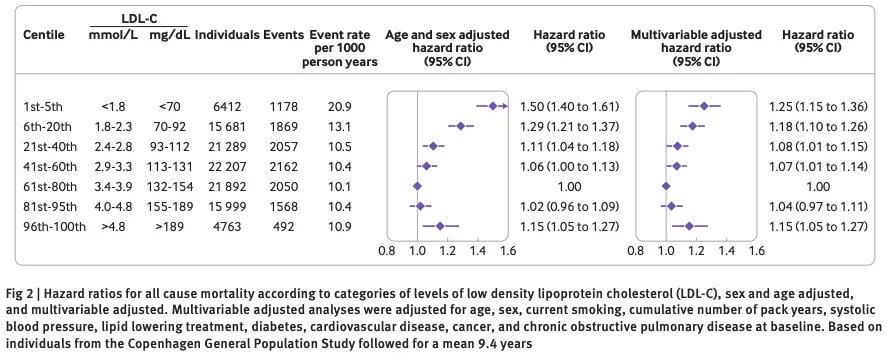
But the all-cause mortality signal does exist. Mendelian randomization across 1,012,240 people: every standard deviation increase in genetically proxied LDL-C reduces lifespan by 1.2 years. That is not a surrogate. That is how long people live.
In statin-treated patients with discordant high ApoB despite low LDL-C, all-cause mortality hazard ratio is 1.21. The ApoB column predicts who dies, not just who has a heart attack.
The trick is demanding a standard that individual trials cannot meet by design, then declaring the evidence absent when no single trial clears the bar.
It is not absent. It is distributed across a million people in a natural experiment that has been running for generations.
All-cause mortality also misses everything that happens before death. A near-fatal heart attack that leaves someone on supplemental oxygen counts as a survival. A debilitating stroke that ends independent living counts as a survival. The years spent in cardiac rehabilitation, the lost function, the dependency. None of that appears in the ACM column.
Counting only deaths is the most incomplete way to measure an intervention that prevents the event in the first place.
ApoB does not fail to improve all-cause mortality. The argument fails to account for how all-cause mortality evidence works.
Stay awake my friends. Ideally off supplemental oxygen.

2
14
560
Jun 13
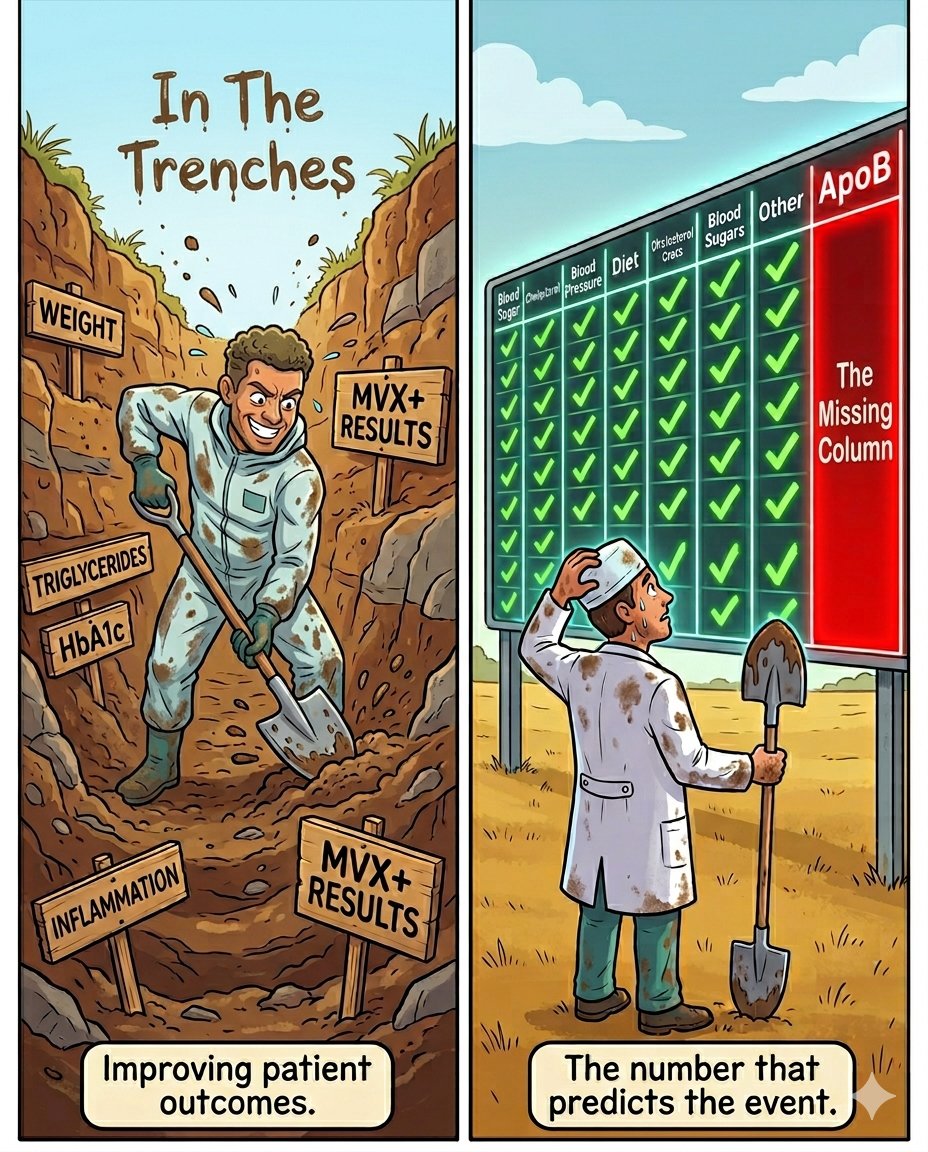
"All you do is criticize from the sidelines, while we are out there in the trenches improving patient outcomes and advancing science!!"
One common move from MDs turned health influencers. All under the guise of "traditional medicine has the root cause all wrong, buy my unproven stuff instead."
So what is on offer?
Direct primary care focused on metabolic health. A Medical Weight Loss program. Statins and PCSK9 inhibitors dismissed as unnecessary or harmful. Lab tests with zero hard cardiovascular outcome data promoted as superior cardiovascular assessment. Clinic outcomes presented at conferences cited as evidence.
You cannot improve outcomes you are not measuring. If ApoB is not on the panel, the primary driver of atherosclerotic plaque accumulation is invisible.
Patients can feel metabolic improvement, lose weight, see triglycerides fall, and still be loading their arterial walls with ApoB-containing particles every day. The number that predicts the event is the number that is not being tracked.
The interventions being discouraged have 170,000 patients across statin trials, 27,564 in FOURIER, and a natural experiment in PCSK9 loss-of-function carriers showing 88% lower coronary heart disease over 15 years.
The tools being promoted in their place have none of that.
@DrNadolsky practices evidence-based obesity medicine and has published peer-reviewed outcomes data on antiobesity medications. @Drlipid spent four decades building a clinical lipidology practice on ApoB-guided therapy. Both are in the trenches. Both measure the right things.
Pushing science forward means preregistered endpoints, comparison arms, and measuring what kills people rather than what makes them feel better in the short term.
The scoreboard has one open column. The trenches have not filled it.
Isn't it ironic.
4
1
10
741
Jun 13
Good news!
Keto zealots have gone through various stages of KETO-CTA grief and have finally reached acceptance of the fact that no cardiovascular outcome RCT exists for keto.
Classic motte-and-bailey alert.
What is a keto clown to do when the circus collapses? Easy. Demand that the other side prove a standard no medical intervention has ever met. Directly randomize humans to high versus low ApoB for decades, withhold proven therapy from the control group, and measure what happens.
That experiment cannot be done. It would be unethical.
By that same standard, smoking does not cause lung cancer. No one randomized people to smoke for forty years.
Seatbelts do not save lives. No one randomized drivers to go beltless at highway speed.
Blood pressure treatment is unproven. Withholding antihypertensives from a control group for a decade would be monstrous.
The keto RCT has no such barrier. Food trials are not unethical. PREDIMED randomized 7,447 people to a dietary pattern. DiRECT randomized adults to a low-calorie dietary intervention and measured hard metabolic outcomes.
Randomizing someone to eat differently for two years has no ethics problem.
The carnivore / keto community even raised $216,880 for exactly this trial. The money materialized. The trial vaporized.
So instead we use the best available evidence. For ApoB that is 170,000 patients across statin trials, 27,564 in FOURIER, 18,144 in IMPROVE-IT with an ezetimibe mechanism that has nothing to do with statins, and a natural experiment running in PCSK9 loss-of-function carriers for generations showing 88% lower coronary heart disease.
For keto: no cardiovascular outcome trial, no loss-of-function genetics showing lifelong keto-adapted humans with lower coronary heart disease, no Mendelian randomization, no dose-response line, no natural experiment of any kind, and no proposed causal mechanism from dietary ketosis to reduced cardiovascular events that does not run directly through ApoB particle burden.
If their mechanism runs through ApoB, they have conceded the argument. If it does not, they need to name it.
Their circus collapsed. Their response is to set fire to the building and call it a draw.
Stay awake my friends.
Jun 12

There’s isn’t one but then again there isn’t a single one for your beloved ApoB either, life’s a b$tch isn’t it

3
3
18
2,591
Jun 12
Classic @BrianLenzkes.
Medical Weight Loss.
He runs a clinic. It sells a program called Medical Weight Loss with a holistic approach to weight management.
No cardiovascular outcome trial. No preregistered endpoint. No data on what it does to the heart.
Fun times!
The intervention he dismisses on this platform has 17,604 patients in a randomized trial.
SELECT followed adults with obesity and cardiovascular disease for five years. Twenty percent fewer heart attacks, strokes, and cardiovascular deaths.
Hard outcomes, not surrogates.
His clinic does not have that. No keto clinic does.
Stay awake my friends.
2
2
2,150
Jun 12
The one number missing from this analysis is the one that would actually answer the question.
The case study format is useful. The TG/HDL ratio at 1.2 is a reassuring metabolic signal.
Classic wrong variable.
The entire analysis uses Total Cholesterol and LDL-C. ApoB is never mentioned. LDL-C 115 with HDL 68 and TG 84 looks clean on a standard lipid panel.
It tells you nothing about ApoB particle count. That discordance is most common in post-menopausal women with excess weight and a high-carb diet. Exactly this metabolic context.
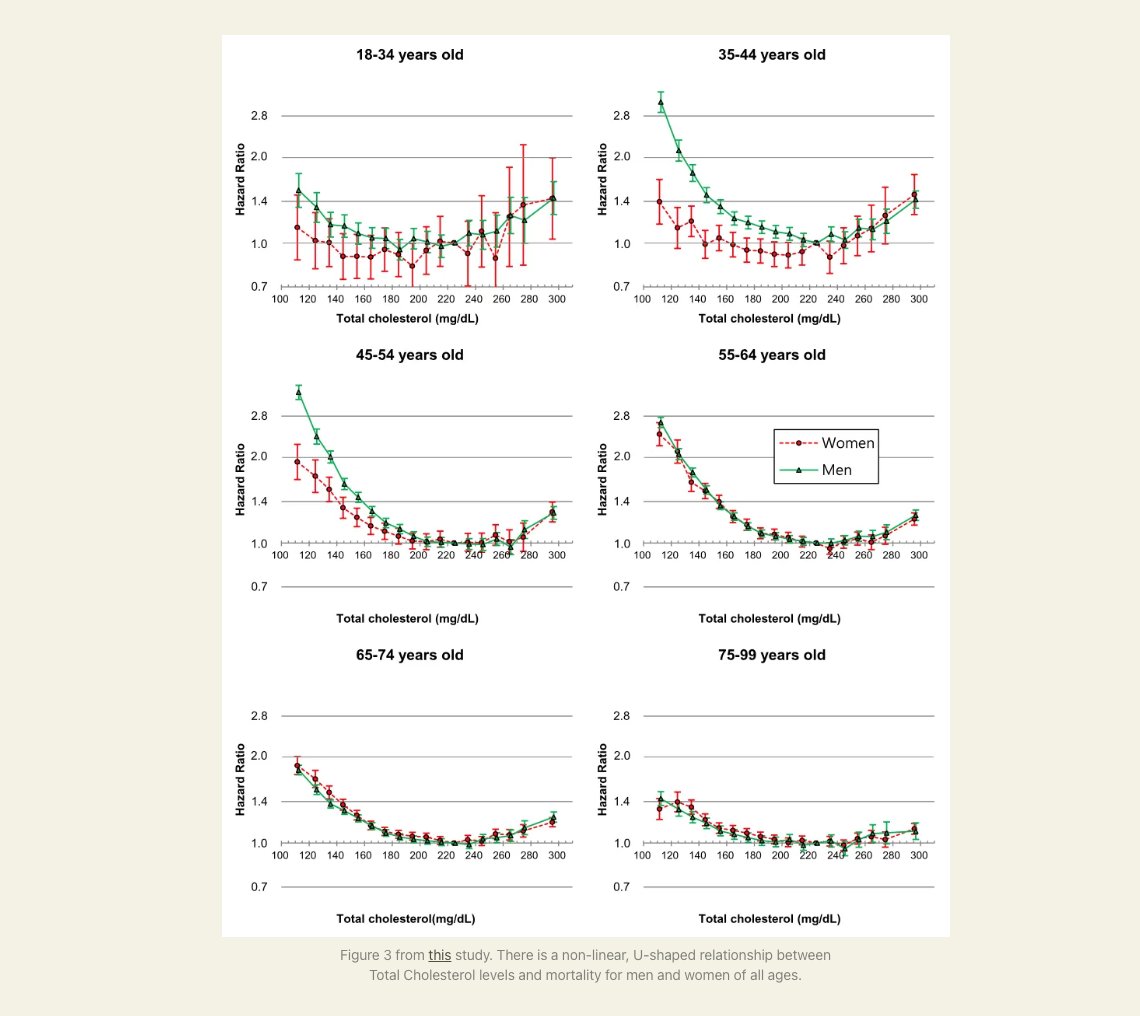
The U-shaped TC mortality curves have a named confound: sick people have low cholesterol because illness lowers it. The studies cited cannot establish that TC 203 is suboptimal for this woman.
Ference would ask: what is her cumulative ApoB exposure over the past decade? That loading does not appear on a single lipid panel.
Fun times!
Paid subscription. Steers a 58-year-old away from statin consideration without measuring the variable that would answer the question.
Choose wisely my friends.
27 Mar 2025

New article on my page: "To statin or not to statin?"
Short case study of a 58-year-old woman's bloodwork.
2
4
735
Jun 12
Bad epidemiology and dangerous food are two different arguments.
The methodological critique is correct. Frank Hu's meta-analysis rests on two heavily weighted observational studies built on food frequency questionnaires and recalled dietary intake from middle-aged adults.
The HPFS-M conclusion contradicted what the meta-analysis claimed. The statistical gymnastics are well documented here.
Classic own goal.
The article destroys observational nutrition epidemiology. It does not touch the randomized controlled trial evidence. Those are different things.
Mozaffarian 2010: 8 RCTs, 13,614 participants, PUFA replacing SFA, 19% CHD event reduction. No food frequency questionnaires. No recalled intake. No Frank Hu weighting decisions. Controlled substitution, randomized allocation, measured outcomes.
The critique of the observational evidence base does not reach the RCT evidence base.
Proving that nutrition epidemiology is unreliable does not prove that seed oils are dangerous.
Those are separate claims requiring separate evidence.

Jun 12
🧵The mainstream "consensus" view is that Ω-6 polyunsaturated fatty acids (PUFAs) are "heart healthy."
Let's look at two of the most highly cited meta-analyses behind this claim - papers cited by organizations like the American Heart Association and WHO.
Main takeaways:
- Published meta-analyses are often laughably (and suspiciously) bad.
- Other, more meticulous meta-analyses come to different conclusions.
- Anyone can cherry-pick papers on virtually any topic to justify whatever their preferred conclusion is.
- Much of "nutrition science" is a house of cards built on a foundation of shaky data and statistical voodoo.
1/
1
1
255
Jun 12
The parasitic business model is simple. Sell certainty. Charge monthly. Steer people away from evidence-based medicine. Never measure whether it worked.
"Twenty years in the trenches!" "Hundreds of paying clients!"
A checkout page, a program, a testimonials page. Motivational content. Success stories. Community. Sounds just lovely, right? What's the problem you say.
Not one published ApoB trajectory. Not one MACE event tracked. Not one plaque progression study. No 10-year follow-up. No cardiovascular event rate. No data that would tell you whether the protocol extends life or shortens it.
"Feeling great" now is awesome. But it is not a long term outcome. A testimonial is not a trial. Twenty years of charging people is not twenty years of evidence.
The pitch: doctors are all wrong, LDL-C does not cause heart disease, you are a lean machine. The clock on the arterial wall does not care about the testimonials page.
Fun times!
Ask your health coach if their protocol has ever been measured against hard cardiovascular outcomes like heart attacks and strokes.
Ask if a single client cardiovascular risk trajectory has been tracked. If the answer is no, you are paying for a story, not a result.
Classic parasite.

2
8
254
Jun 12
Grok said "elevated LDL cholesterol alone."
Classic strawman.
The argument is not elevated LDL cholesterol alone. The argument is cumulative ApoB particle burden over decades. Those are different claims and Grok answered the wrong one.
Asked Grok what PCSK9 loss-of-function carriers show about lifetime ApoB exposure and coronary heart disease risk. Or what 170,000 patients across CTT statin trials show about dose-response between ApoB reduction and MACE. Or whether insulin resistance raises ASCVD risk by raising hepatic ApoB output.
Spoiler: the answer to the last one is yes.
The mechanism runs through ApoB, not around it. Don't take my word for it, here's Grok:
"Lifelong genetic lowering of ApoB exposure (via PCSK9 LOF) causally and substantially cuts CHD risk, mirroring and amplifying short-term pharmacologic benefits. CTT data confirm a robust, proportional dose-response between ApoB/LDL reduction and MACE prevention in trials—supporting aggressive, sustained lowering. IR contributes independently to ASCVD by driving hepatic ApoB/VLDL overproduction (plus other effects), explaining why ApoB is often a superior marker in metabolic disease. Together, this reinforces ApoB as a central causal driver and therapeutic target, with lifestyle/pharmacologic interventions addressing both lipids and IR for optimal risk reduction."
Prompt wisely my friends.
Jun 12

Apparently Grok is a low carb zealot 😉:
"Elevated insulin levels (hyperinsulinemia due to insulin resistance) appear more dangerous in isolation for coronary disease (CAD/ASCVD) than elevated LDL cholesterol alone, based on mechanistic, observational, and some comparative data."
3
8
706