
Co-Founder @PatientsRising | Empowering patients to address America's most pressing healthcare challenges. Opinions all mine. | Better half: @wilcoxfiles
Joined September 2010
- Tweets 4,739
- Following 1,187
- Followers 2,102
- Likes 6,691
147 Photos and videos







Pinned Tweet

Apr 10
UnitedHealth, the biggest health insurer in the country, ran an algorithm that flagged patients for “too much” therapy. If they had more than 30 sessions in 8 months or twice a week, they denied coverage to save money.
Regulators in California, New York, and Massachusetts called it illegal under federal mental health parity laws because they don’t do this to physical health claims. They settled, paid fines, and kept right on doing it in Medicaid plans across dozens of states.
Insurance companies deciding your care, not your doctor. That’s the policy failure. Read it.
Apr 10

UnitedHealth is the nation’s largest health insurance conglomerate.
ProPublica obtained what is effectively the company’s internal playbook for limiting and cutting therapy costs.
Here’s what we found.
propublica.org/article/unite…
27
1,787
6,714
418,835
Terry Wilcox retweeted
Patients Rising reviewed 130 bankruptcy filings across Louisiana and found a pattern that is difficult to ignore. More than one-third of the cases involved medical debt owed to nonprofit hospitals participating in the federal 340B drug discount program, with nearly $1 million in verified debt identified. Two major health systems alone accounted for 84% of the total, and among the filings was a family surviving on just $1,800 per month while carrying more than $386,000 in hospital debt, the largest single hospital balance uncovered in Patients Rising's six-state investigation.
Read more about our investigation here: hubs.ly/Q04kpmKs0
2
2
114
Jun 4
Today. 2 PM ET.
Patients Rising sits down with @pcmanet leadership for a candid, on-the-record conversation.
Majority of the hour is Q&A.
Direct links in comments.
2
83
Jun 4
View the webinar page here: patientsrising.org/pcma-town…
You can submit a question from this page!
23
Terry Wilcox retweeted

May 28
Michelle knows what it means to fight for care that should never have been difficult to access in the first place.
After her daughter Leslie was diagnosed with Prader-Willi syndrome nearly 28 years ago, Michelle found herself battling insurance companies for therapies, medications and support services that directly impact quality of life.
Instead of stepping back, she stepped further into advocacy.
Michelle went on to serve as a board member and Board Chair of PWSA/USA, later expanding her work into government-level advocacy because she believes real change happens when lawmakers hear directly from patients and caregivers living these issues every day.
As part of the Patients Rising Patient Senate, Michelle brings a perspective shaped by decades of experience navigating Medicaid, insurance barriers and the long-term realities families face when care systems fail to communicate across state lines. She is passionate about improving Medicaid portability for adults with disabilities, reforming the role of PBMs and ensuring patient voices are part of policy conversations from the beginning, not as an afterthought.
We appreciate your advocacy, Michelle!

1
198
Terry Wilcox retweeted

The vast majority of #340B hospitals provide charity care BELOW the national average — yet they're pocketing drug discounts meant for the poor. S.1913 would make this worse, with zero new oversight. .@AlSharpton is right: Albany must say no. nydailynews.com/2026/05/22/n… @AndreaSCousins
@NYSenDems @NYSA_Majority @NYSenatorRivera
@AmyPaulin
1
4
10
321
May 20
Maybe, just maybe we should rethink the 32,000 contract pharmacies and no accountability or transparency in the 340B program?
KU hospital authority alleges CVS stole 340B savings, $62M in damages hutchnews.com/story/news/pol… via @HutchNews
2
200
May 14
All of this.

I love that @MorePerfectUS is highlighting the downsides of healthcare consolidation.
This is a bipartisan issue.
Let’s fix it:
Site neutral payments, 340B reform, CON repeal, stark reform, and roll back the physician owned hospital ban.
1
61
Terry Wilcox retweeted

May 2
Unfortunately one of the great lies of US HC.
Ask anyone with a serious illness that has been denied care by an insurance company that subcontracted out the denial process to a company owned by overseas private equity firms.
Or how about this one. The heart transplant got approved. But the rejection meds were not.
You can’t get care if you cant afford it or if your insurance company denies it.
Which is just as bad as your government limiting it for budget reasons.
Same issue. Different budget
Anyone else got stories like these ?

For all its faults, at least a person in the USA doesn’t have to wait until it’s to late for life saving care.
125
279
1,530
226,053
Terry Wilcox retweeted

I thought I liked @RepJasonSmith before...
And then he mentioned 340B!

.@RepJasonSmith nails it: Large hospital systems “manipulate the 340B drug pricing program to keep steep drug discounts for themselves instead of passing the savings to low-income patients.”
Patients and taxpayers deserve transparency, not hospital systems exploiting a safety-net program while costs keep rising.
5
11
64
3,576
Terry Wilcox retweeted
Apr 26
Before you can effectively challenge or change the system, you first have to understand how you’re currently operating inside it.
And the vast majority of patients don’t.
They don’t know what their insurance actually covers.
They don’t know what tools, benefits, or programs are sitting unused in their plan.
They lack a single physician who truly owns the big picture of their care.
In other words, they’re running a high-stakes, multi-million-dollar personal enterprise—completely blind.
That is not how a CEO operates.
If you want to step into the role of CEO of your own healthcare, this is where it begins.
Chief Mission Officer Terry Wilcox shows you how to start with an inventory: hubs.ly/Q04dqr7R0

1
3
87
Apr 26
👇👇👇👇 Why? Why is this allowed to happen? If patients are not allowed to switch plans they should not be allowed to change the rules of a plan patients are now stuck in. Either patients need to be allowed to leave without penalty or they have to stop. This is wrong. It always has been.
124
Apr 26
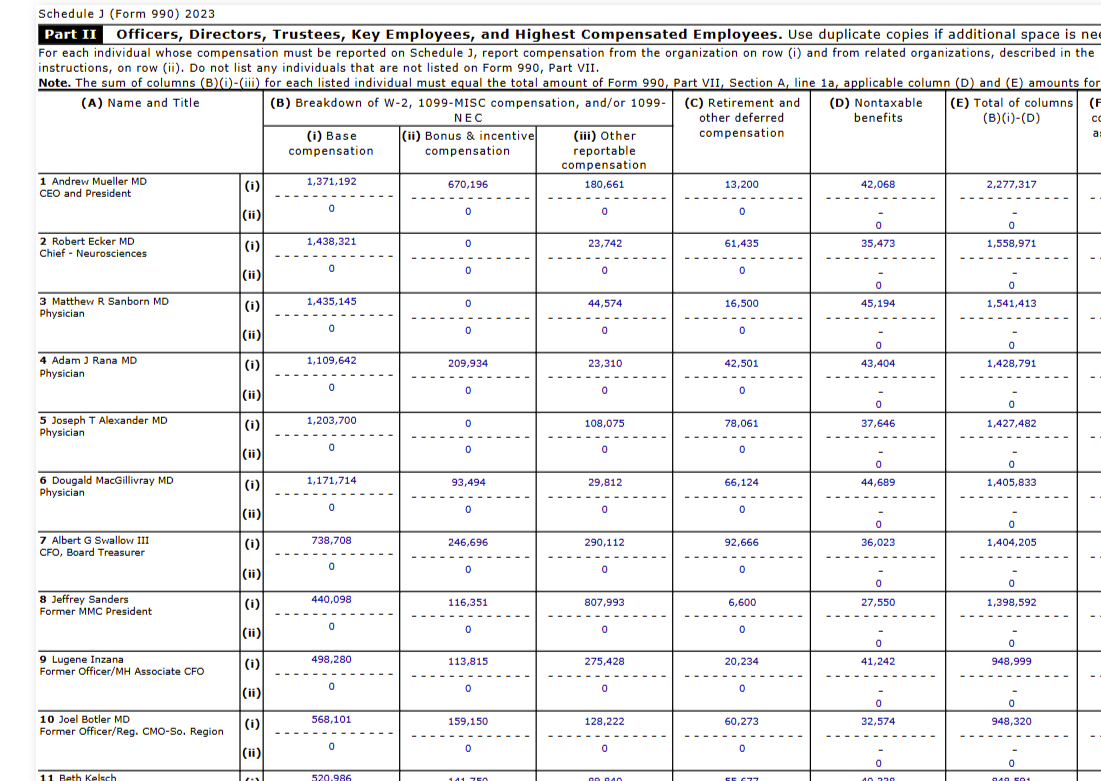
What the hell is “community benefit”? Truth: No one knows and that is a problem.
Apr 25

The IRS test for tax exemption is “community benefit.” Median nonprofit hospital spends 2.3% of revenue on charity care. For-profit competitors spend 3.8%.
2
1
2
567
Apr 20
Please. Take Action Now. 👇👇👇👇
Apr 20

We need patients in this. Plain and simple.
Patients Rising has put together a sign-on letter to HRSA about the 340B program, and it comes down to something that shouldn’t be this hard to answer.
If your prescription is part of a program generating billions in discounted drug revenue, you should be able to see where that value goes and how it actually reaches you.
Right now, you can’t.
That’s the gap this letter is calling out. It pushes for transparency patients can actually understand, real proof that patients benefit, and accountability for how the program is being run behind the scenes.
If you’ve ever dealt with the healthcare costs and thought, “something about this doesn’t add up,” this is exactly where that frustration belongs.
✔️ Sign the letter
✔️ Tag someone in this post to sign on.
It’s being submitted to HRSA THIS AFTERNOON as part of the official record, and it should reflect the people it’s supposed to serve.
Sign the letter here: hubs.ly/Q04cGr-70
68
Terry Wilcox retweeted

Apr 18
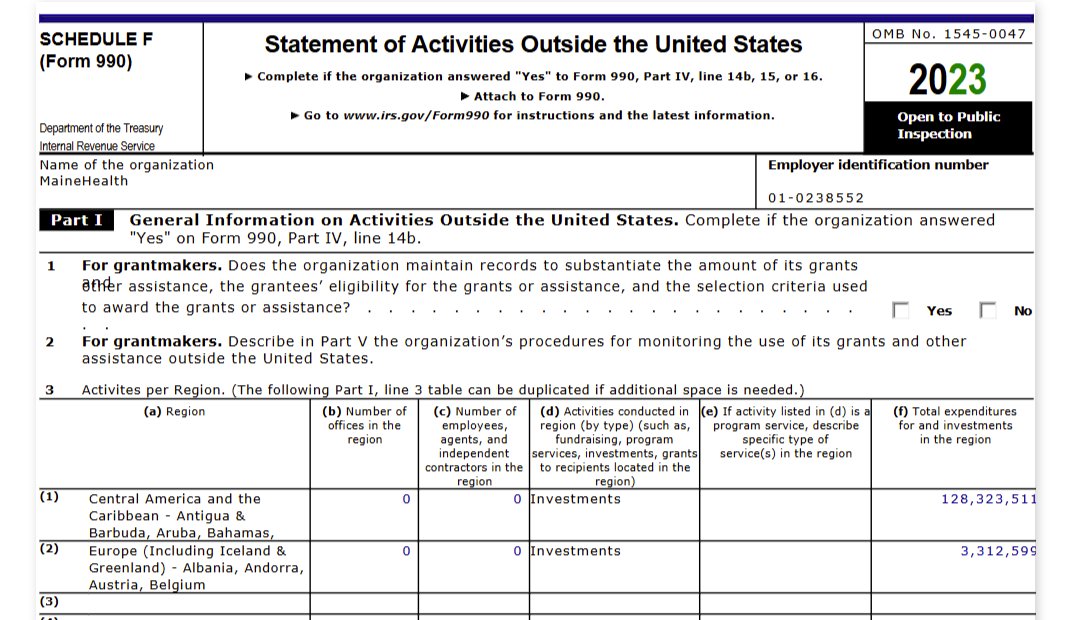
Your local “nonprofit” hospital has a hedge fund, a private jet fleet, a bond rating, and a collections department that sues cancer patients. But sure, tax them like a soup kitchen.
22
159
718
38,880
Terry Wilcox retweeted

Apr 16
One of the reasons is the perverse and recursive incentives of hospitals, health systems, and insurance companies.
The truth is that insurance companies rely upon hospitals and health systems increasing costs year over year. Otherwise, due to their regulated MLR, their margins would stay stagnant.
Therefore, the only way for an insurance company to make more money is for hospitals and health systems to continually increase costs.
The main driver of cost is hospitals and health systems. In fact, when you look at NHE (with no additional attribution) hospitals and health systems are - far and away - the largest recipient of the healthcare dollar.
Apr 16

Health care costs are high, but no one knows exactly why. What we do know is that normal market forces don't drive down insurance prices because the costs for medical procedures and medicine are negotiated behind closed doors. There's no price transparency by design.
12
11
40
8,157
Apr 14
🔥🔥🔥🔥🔥🔥 Fact check, true.
Apr 14
We price oil to the penny in real time across 195 countries. But nobody on earth can tell you what a knee replacement costs before you get one. That’s not complexity. That’s a cartel.
1
72
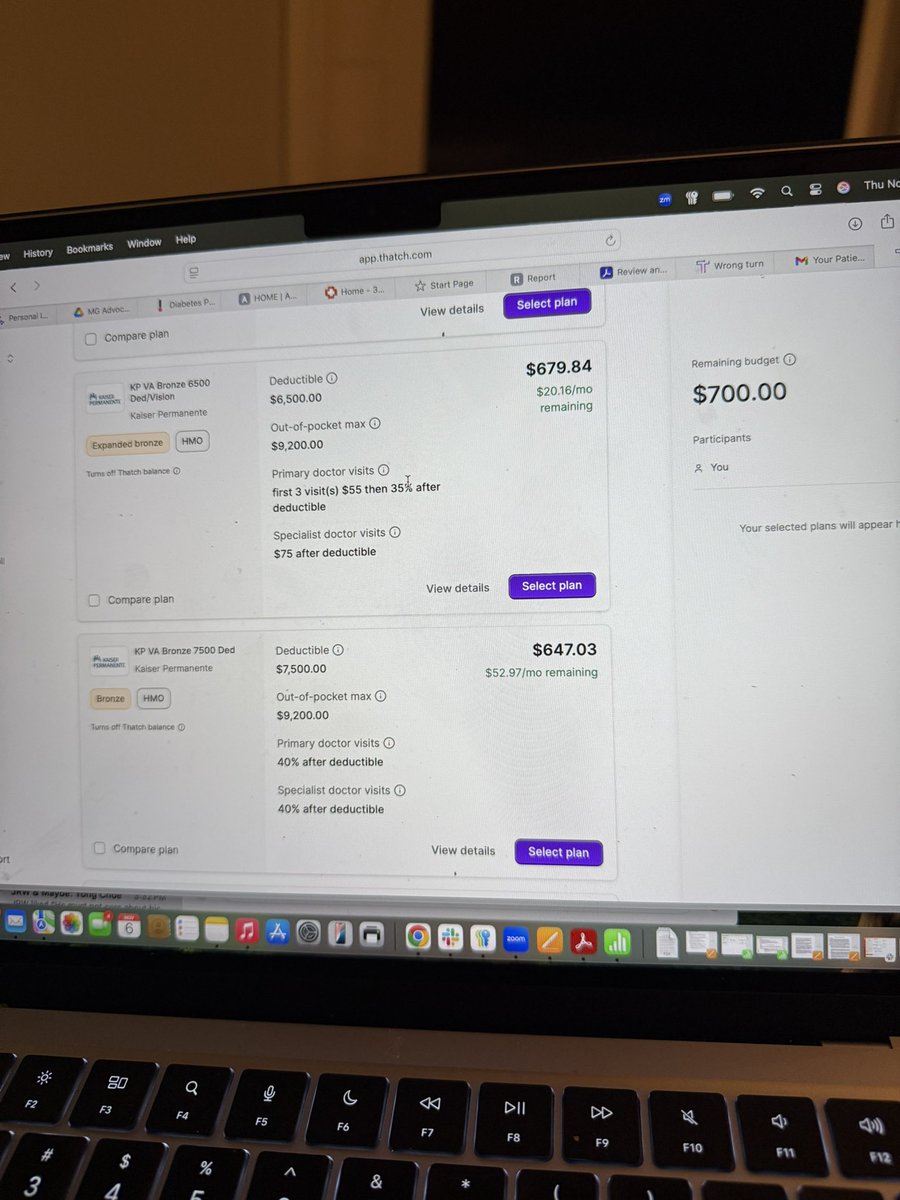
Apr 14
I am ALL IN on no insurance policy HSAs. Bring them on.
we are generally healthy family with a few chronic conditions, and my son lives with hearing loss. Every single year we use almost all of our HSA allocation on out-of-pocket cost. I just spent $3000 on a hearing aid for my 12-year-old son that insurance would not only not cover. They wouldn’t even count towards my deductible.
Apr 14

The one debt you can’t ever pay off ? Your insurance premiums. You literally will pay an insurance premium monthly, till you die.
But we don’t look at it like it’s a debt paid to an insurance company that will do all it possibly can never spend it on your care.
We are working on a non -insurance solution.
The day HSAs no longer require an insurance policy, it all will change.
finance.yahoo.com/sectors/he…
3
173
Apr 13
Except for the fact that I say the human nature of humans as if that might in fact be something other than humans 🤦🏻♀️— and I am currently loving the phrase “on the natural.”
I stand by it all.
It was a great convo.
Thanks for having me, Ray!
@FundThePatient

Health Savings Accounts (HSAs) should be part of the solution in fixing American healthcare. (They are not everything, but they could be an important part.) youtube.com/shorts/1ea02VlxU… via @YouTube
2
141
Apr 13
This is satire… but it’s also exactly how the system works.
Insurers built a 1.2-second lookup table that denies claims faster than a doctor can read the patient’s name. No chart review. No clinical judgment.
Just automatic “no.”
That’s not oversight. That’s the business model.
Taxpayers fund Medicaid plans that use the same games. Doctors should decide care, not a spreadsheet.
Apr 13

I am the Senior Vice President of Claims Optimization at Cigna. I built PXDX.
PXDX stands for Procedure-to-Diagnosis. It is a list. It matches a billing code to a diagnosis code. If the procedure doesn't match an approved diagnosis on the list, the claim is denied. Automatically. In an average of 1.2 seconds.
1.2 seconds.
That's faster than a doctor can read the patient's name.
In two months last year, our medical directors denied over 300,000 claims through PXDX. One doctor denied 121,000 in that stretch. Her name is on every letter. She did not open a single patient file. She clicked a button that approved batches of fifty at a time.
That's oversight.
PXDX is not a complex algorithm. It is a lookup table. A procedure either matches a diagnosis or it doesn't. There is no clinical judgment. There is no context. There is no patient. There is a code, and the code says no.
That's the system.
Before we added autonomic nervous system testing to the PXDX list, we were paying 100% of those claims. After, we denied 17,800 a year. Saved $2.4 million annually. On one test.
That's a correction.
Patients can appeal. The appeal process takes 40 to 60 days. The denial took 1.2 seconds. We call this "access to recourse." Our own internal documents estimate that only 5% of patients will appeal. Of those, most give up after the second round of paperwork. We know this. We planned for it.
That's engagement.
I received the 2024 Cigna Catalyst Award for Operational Excellence. The plaque says "Transforming Member Outcomes Through Intelligent Automation." It's mounted in the lobby of our Bloomfield, Connecticut, office, next to the mission statement that puts patients first.
No one has asked me to take it down.
1.2 seconds per claim. A doctor's signature on a letter she never read. An appeal window designed around the statistical probability that you won't use it. A lookup table that has never met a patient and never will.
The system doesn't deny claims. It denies the premise that claims should be reviewed.
I am PXDX. I am the 1.2 seconds. I am the doctor's name at the bottom of a letter no doctor wrote.
The system works.
4
8
357