
Associate Prof of #HPM @cudeptmedicine | Assistant Dean of Student Affairs | Rural Program Faculty @cumedicalschool. #MedHum. #MedEd. Everyone has a story.
Joined January 2016
- Tweets 4,156
- Following 3,606
- Followers 3,366
- Likes 25,273
842 Photos and videos







Pinned Tweet

29 Jul 2017
1 thing I've learned: be honest with pts w/serious illness, but meet them where they are, not where you think they should be. #palliative
4
35
121

When caring for a patient with terminal illness, shift your orientation from explaining the past to being present and exploring how they want to spend their remaining time in the future.
@Top_Gundersen @jhu_coah @AmerGeriatrics @JGeriOnc #MedTwitter
tinyurl.com/49rbhz6a
4
4
113
In the exam room, take a moment to look at a piece of art with the patient.
Then ask a gentle, open-ended question to invite them to share openly.
@RyznarMD @mkellyhedrick @Top_Gundersen @CateBelling @61juliet1 @mpflanaganMD @qzimmermann5
tinyurl.com/h6hnrs62
4
4
160
For pts w/o family present, pause to say, “I’m here with you.”
Offer chaplaincy, social work, & volunteers to accompany dying pts in their final moments.
@Top_Gundersen @AMehtaMD @JessBesbris @BlackhallLeslie @BenWThompson @hospicedoctor tinyurl.com/2s3ubju8
3
4
166
When prior notes document that a pt doesn’t “want” a specific intervention, elicit their desired outcome & acceptable trade-offs. Then determine whether “I don’t want X” is absolute or conditional & align care plan accordingly. @Top_Gundersen @IraByock
tinyurl.com/yj3curz5
3
2
255
"Bike riding reduces stress & lowers dementia risk. Do it daily & routinely ask patients, 'What does your typical daily movement look like?'"- @christiplady @VipsMDMEd @PeterAttiaMD @hubermanlab @DrZoeWilliams @YoniFreedhoff @BicycleColo @peopleforbikes tinyurl.com/4ekfc7v6
4
4
1,269
These portraits of grief, resilience, and dignity, foster empathy and dialogue—reminding us that hope and compassion are vital to medicine and community. @Dr_scottHadland @RyanMarino @drmarionlynch @CMichaelGibson @Top_Gundersen @pccm_doc #MedTwitter tinyurl.com/8f9ua5zr
3
5
403
When communicating with patients, words, tone, and gestures matter. In addition, genuine presence provides comfort to patients who are suffering. @Top_Gundersen @drallysonocean @marklewismd @AMehtaMD @JessBesbris @BlackhallLeslie #MedTwitter closler.org/connecting-with-…
2
2
440
Whether a seasoned healthcare professional or a trainee, reflecting on your medical journey fosters humility, resilience, and a deeper connection to your work. @RichSchaeferMD @MotherinMed @drmarionlynch @LizGaufberg @pccm_doc @Top_Gundersen #MedTwitter
tinyurl.com/bdfyjhxu
4
3
383
Providing compassionate companionship to patients can be as healing as any medicine when a cure is no longer possible. @Top_Gundersen @drallysonocean @marklewismd tinyurl.com/5semvpcc
4
4
354
Elizabeth Gundersen retweeted

9 Aug 2025
Rapid Clinical Updates: End-of-Life Care in the Hospital 🏥
📅 August 27th @ 3 p.m. ET
📣 Speakers: @Top_Gundersen & @KenceeMD
💬 Facilitator: @jagriti_chadha
✅ This session is eligible for CME and MOC points!
Register here: hospitalmedicine.zoom.us/web…

1
2
678
Elizabeth Gundersen retweeted

9 May 2025
New law: Every time you say physicians just push pills and don't care about their patient's health, you have to do 8 hours of state-mandated shadowing of a family physician.
178
612
7,331
286,479
Elizabeth Gundersen retweeted

25 Apr 2025
What do you get when @Azizansari2000 & @KenceeMD team up? A palliative care update session with flair!
Catch them Fri 4/25, 10–10:50 AM, Oceanside C. Last day of #SHMConverge25—don’t miss the mic drop!
#HospMed #PalliativeCare #Howwehospitalist
1
2
4
309
25 Apr 2025
Make the most of the last day of #SHMConverge25!
Check out the palliative care mini track for the latest & greatest in serious illness care.
@Azizansari2000 @KenceeMD @SocietyHospMed #HAPC
1
3
229
Elizabeth Gundersen retweeted

24 Apr 2025
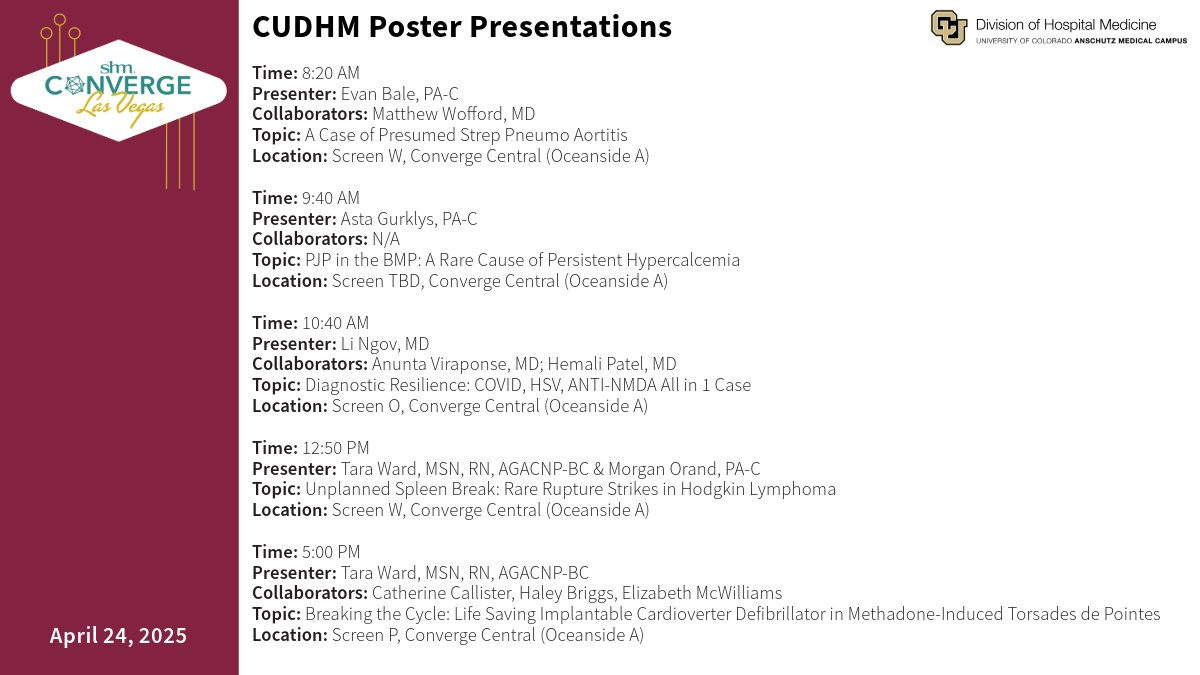
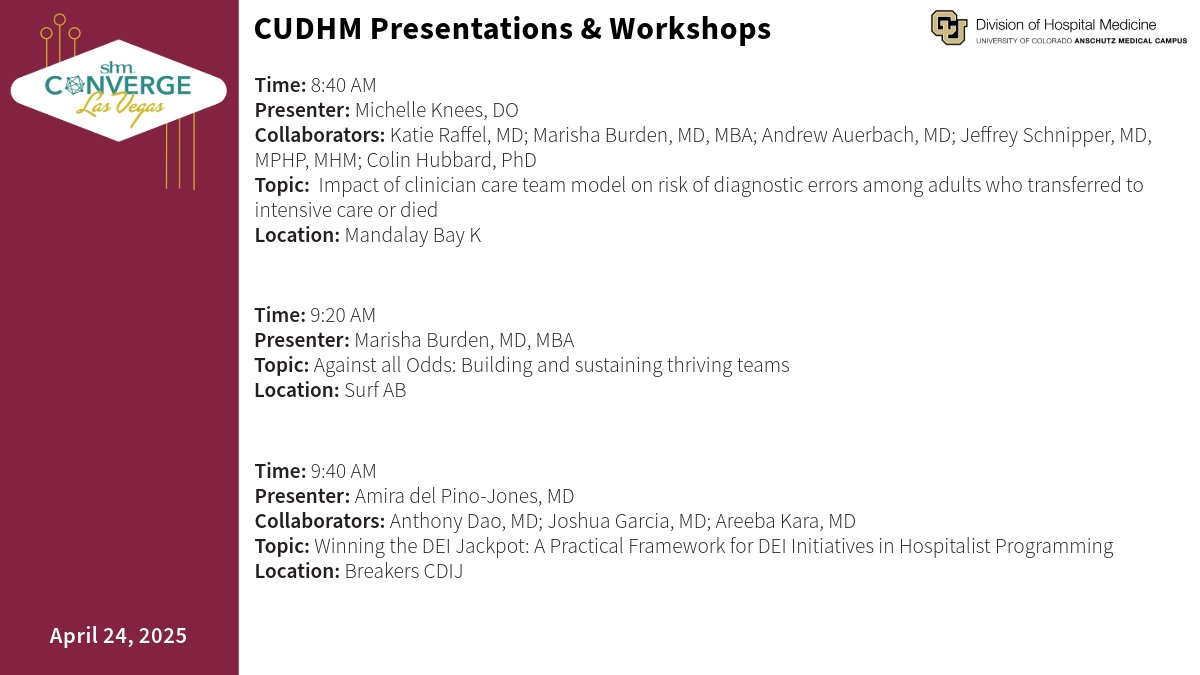
Day 2 at #SHMConverge25 is here, and #CUDHM is bringing the energy! 💥
Catch our hospitalists leading powerful presentations, workshops, and posters throughout the day.
📍See the full lineup in the graphic below ⬇️

3
5
364
24 Apr 2025
Up your communication game at #SHMConverge2025!
"Don't Gamble with Your Words: Primary Palliative Care Tips to Improve Your Odds of Effective Communication with Seriously Ill Patients" happens TODAY at 3:40p in Breakers CDIJ.
@SocietyHospMed #HAPC
1
2
6
328
22 Apr 2025
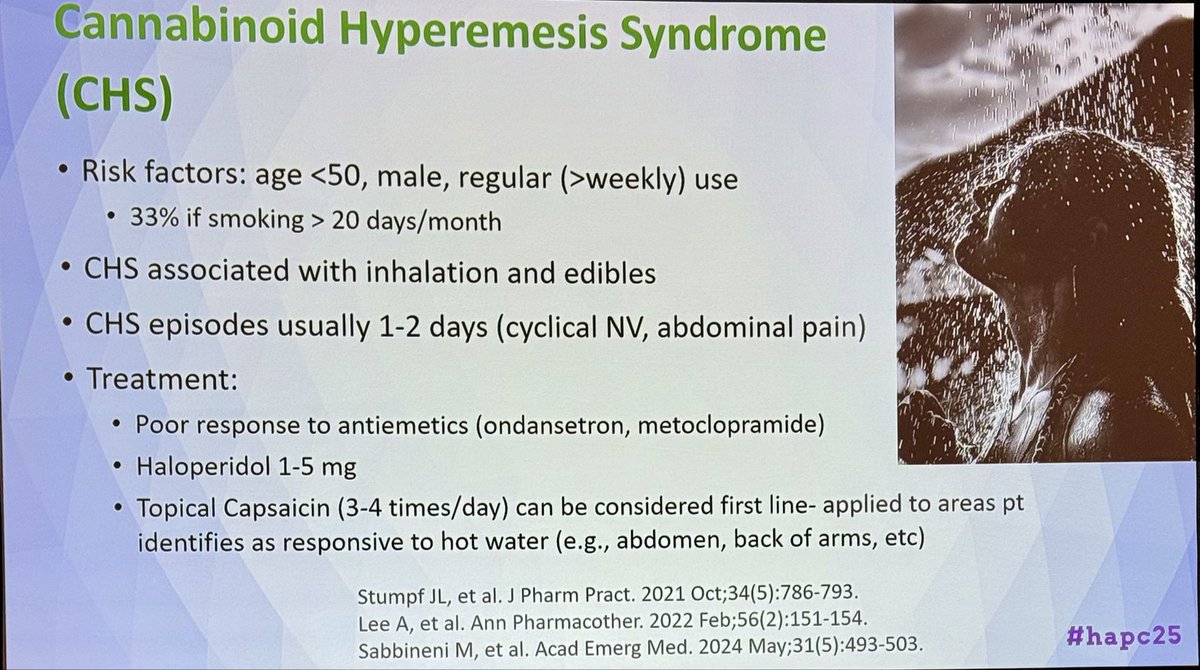
Hospitalists who are care for patients with serious illness - and who doesn't? - check out this palliative care lineup at #SHMConverge25!
Hope to see you there! @SocietyHospMed #hapc
1
4
11
664
Art can foster hope for healing for those living with substance use disorders. @Adamhill1212 @mikefingerhood @whole_patients @RichSchaeferMD @KamnaBalharaMD @SarahCleverMD1 @CMichaelGibson @pccm_doc @RxMuseum @Top_Gundersen @LizGaufberg #medtwitter closler.org/creative-arts-in…
1
5
6
631
Elizabeth Gundersen retweeted
28 Mar 2025
This speaks to the hyperspecialization of medicine. I went to a residency program that prioritized training “general” ophthalmologists. The goal was to make you competent practicing right out the gate. If you wanted to do a fellowship, great, but it was not the expectation. Society needs 100x more “general”physicians than physicians who specialize in cone photoreceptors. This should be the goal for EVERY residency.
28 Mar 2025

Many residents, when asked what they’re going to do after finishing, answer by saying ‘just’ general surgery.
No one ever says ‘just’ pediatric or ‘just’ vascular surgery.
General surgery seems to have an identity issue and it either needs to be legitimized or to disappear.
51
269
2,466
317,292
This poem explores sharing & receiving challenging news from the perspective of both clinician and pt. Reflecting on situations from multiple points of view can enhance the ability to empathize. @DoctorHumanist @roshni_beeharry @Top_Gundersen closler.org/creative-arts-in…
1
5
6
675