
Nephrology & Internal Medicine. Immunothrombosis incl DIC. ISTH Member. No Conflicts of Interest. Views my own etc
Joined September 2012
- Tweets 25,111
- Following 3,193
- Followers 32,422
- Likes 124,982
2,299 Photos and videos




Pinned Tweet

19 Feb 2023
A lie oft repeated remains an abject lie. Nobody has ever produced a shred of evidence that a Cochrane review is a universally valid scientific “Gold Standard” applicable to all health outcome measures. Just repeating a lie is not enough.🧵news.com.au/lifestyle/health…
64
436
1,524
361,009
RT @PeterHotez: Never forget: The @WSJopinion as the print version of Fox News and Murdoch media empire waged a war of aggression on the Am…
215
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

I would like to join the chorus of CC voices saying:
If you are not masking and avoiding infections... It shows. You may not realize, but your sharpness, your compassion, your humanity... Is declining.
It is not too late to turn the brain damage trian around. #MaskUp.
9
142
658
7,321
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

Beyond brain fog: viral proteins as convergent drivers of neuroinflammation and proteinopathy
🚨“COVID-19 never really leaves your brain.”
New science review proposes SARSCoV2 viral proteins stay behind as long-lived toxins, triggering chronic neuroinflammation and planting the seeds of Alzheimer’s and Parkinson’s, even after mild infection.
This very interesting and eye-catching GERMAN review reframes post-viral neurological syndromes( L0ngC0vid) as driven by persistent viral proteins acting as long-term toxins ("protein-as-pathogen" model), not just the active infection!
➡️Core mechanisms:
- SARSCoV2 Spike and OTHER viral proteins activate glial TLR4/TLR2 receptors, triggering chronic neuroinflammatory cascades via NLRP3 inflammasome,
- They also disrupt autophagy, allowing toxic protein aggregates (tau, amyloid-beta, α-synuclein) to accumulate and seed neurodegeneration,
➡️SARSCoV2 specific evidence:
- Animal studies show Spike protein alone (without live virus) induces TLR4-mediated cognitive deficits, memory impairment, synaptic loss, and sustained neuroinflammation, recapitulating post-COVID syndrome,
- Spike binds α-synuclein, accelerating Parkinson-like clumps,
➡️Human data evidence:
- Millions experience "brain fog,"
- Post-COVID patients exhibit measurable brain damage: cortical thinning, hippocampal iron accumulation, and biomarkers of ongoing neuronal injury,
➡️Broader risks:
- Even mild infections leave lingering proteins that promote Alzheimer’s and Parkinson’s-like pathology via shared pathways,
- Same pathways seen in influenza, dengue, West Nile etc,
- Mild infection = no protection,
‼️So, according to this review, the “protein-as-pathogen” model makes it crystal clear: every new SARSCoV2 infection (even mild or asymptomatic) deposits more of these long-lived toxic viral proteins into the brain. They don’t fully clear. They accumulate.
Each reinfection reloads the TLR4/TLR2 → NLRP3 inflammasome trigger and further collapses autophagy, speeding up the tau/amyloid/α-synuclein proteinopathy and neurodegeneration.
SARS-CoV-2 does not just infect.
It weaponizes its own proteins as long-lived intracellular saboteurs.
Millions are probably already carrying this hidden payload.
This is not brain fog.
This is a silent, population-scale reprogramming of human brains toward dementia-like decline.
The long-term neurological cost will probably dwarf the acute pandemic itself!
#AvoidSars2 #AvoidReinfections
sciencedirect.com/science/ar…

14
289
665
22,682
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

As a neurologist, it is now patently clear to me that the vast majority of people on the planet are suffering from neuroinflammation or brain damage (likely both)
The way people speak & behave has changed. Markedly so.
Whether irl, or via messaging/social media. It’s noticeable
344
1,345
8,514
476,773
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

Apr 13
Many people don't realize that environmental stressors like air pollution, extreme temperatures, and wildfire smoke increase the risk of kidney diseases.
Here is a terrific review in @NatRevNeph led by my mentee turned collaborator Whanhee Lee.
nature.com/articles/s41581-0…
2
21
85
3,334
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

Jun 5
This rebuttal is brilliant, detailed, compassionate, intelligent, science based, and thorough.
The precise opposite of the statement she's replying to.
Please read, share, share, and then share. And also share:
Jun 5

1/Hannah, we have now almost 500,000 peer reviewed published research into long covid now. “Fatigue”, “post exertional malaise (PEM)” “Brain Fog” “difficulty concentrating” are not psychiatric symptoms. They have a pathological basis and clear demonstrable abnormalities 1/
10
198
677
17,389
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

Jun 5
1/Hannah, we have now almost 500,000 peer reviewed published research into long covid now. “Fatigue”, “post exertional malaise (PEM)” “Brain Fog” “difficulty concentrating” are not psychiatric symptoms. They have a pathological basis and clear demonstrable abnormalities 1/
10
290
1,203
47,673
Dr Satoshi Akima FRACP 『秋間聰』 retweeted
Surface cues shape procoagulant properties of amyloidogenic microclots
🚨YOUR ATTENTION: FMCs!
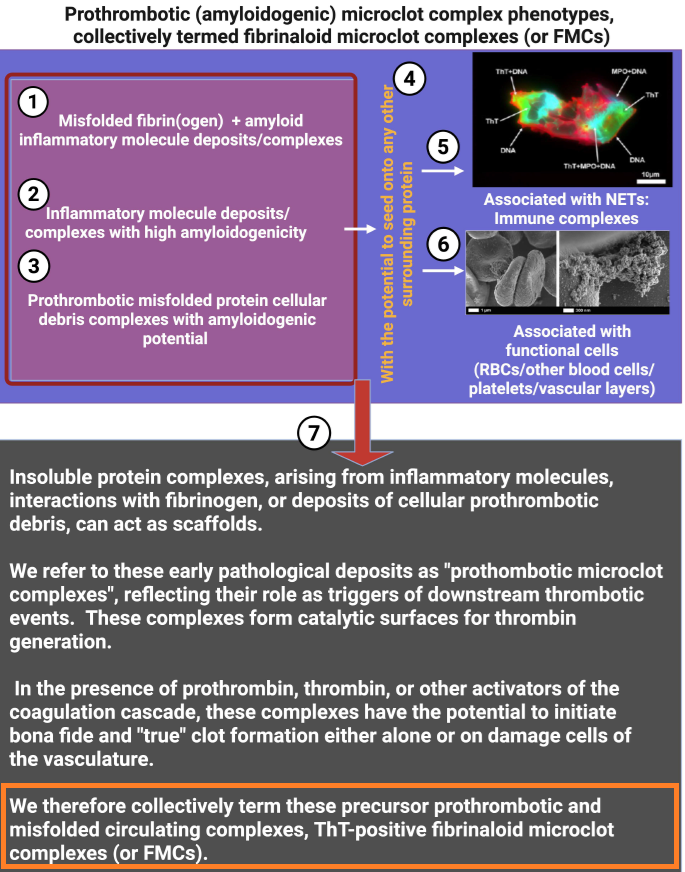
➡️This EVOLUTIONARY review synthesizes how cell-membrane surface changes during inflammation and cell death drive the formation of procoagulant, amyloidogenic microclots termed fibrinaloid microclot complexes (FMCs).
➡️FMCs are heterogeneous (1–200 μm), Thioflavin T (ThT)-positive complexes of fibrinogen, serum amyloid A (SAA), von Willebrand factor, neutrophil extracellular traps (NETs), and cellular debris/microparticles.
➡️The exceptional article introduces FMCs as a unifying conceptual framework that elegantly integrates membrane biophysics, protein misfolding, and coagulation, previously viewed in isolation, into a single membrane-centric model of thrombo-inflammation. Science, step by step!
➡️Its novelty lies in distinguishing these amyloidogenic, fibrinolysis-resistant complexes from both microparticles and canonical clots, while providing mechanistic evidence (PS exposure, SAA/fibrinogen cross-seeding, ThT positivity) for their role across inflammatory and post-infectious diseases.
➡️🤔By positioning FMCs as both pathological drivers and potential biomarkers/therapeutic targets (e.g, via anti-misfolding or NET-clearing strategies), the work offers a transformative lens for understanding and treating hypercoagulability in Long COVID and related syndromes, with broad implications for vascular medicine.
‼️In conclusion, this exceptional review offers a simple new way to understand how damaged cell surfaces during inflammation create tough, sticky microclots that clog blood vessels and drive long-lasting problems like those seen in Long COVID, opening the door to better tests and treatments that could help millions.
GREAT WORK, Thank you @resiapretorius et.al and your additional explanation fig’s are really excellent!
nature.com/articles/s41419-0…
32
71
2,295
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

Honestly, the last year has been one of the worst years of my life. Somehow - maybe it was the maraviroc, maybe it was dumb luck - I finally *mostly* recovered from my Long COVID symptoms (recent fainting episode notwithstanding), and then my wife had multiple strokes, got hospitalized for a month, had part of her skull removed, and wound up even more disabled than I was at my worst.
For that reason, when @AlanLevinovitz emailed me a few months ago and asked me to talk about Long COVID, I missed it. By the time I got to it in my inbox, he had already finished his piece. But even if I had responded in time, I wouldn't have spoken to him - a quick search of his twitter history indicates that, despite not having read seemingly any of the scientific literature, he has strong opinions about what Long COVID is and who has it. He can cite no evidence for his claims, but felt it worthwhile to declare that "60-80%" of Long COVID is psychosomatic. A range that is somehow both bizarrely specific, and entirely fabricated.
I knew exactly the type of piece he would write before I read it, because he's not a neutral observer here. I don't know what his incentives are, but regardless of his intentions, I can tell you exactly how that piece in @WIRED functions: as free advertising for a cottage industry of alternative medicine scammers that prey on some of the most vulnerable people in society.
Here's what Levinovitz conveniently doesn't tell you (I wonder if his editors know about this stuff, assuming this was even edited - a 10 second search can reveal extensive articles on MEpedia and other websites detailing this; even wikipedia covers it a bit):
Like most alternative medicine scams, brain retraining is based on taking something legitimate from medicine (in this case, neuroplasticity and CBT) and putting a spin on it that involves pseudoscience and a money-making scheme.
I never knew these folks existed until I developed Long COVID and became exposed to this space, but they've operated for years. For a couple decades at least they've preyed on people with ME/CFS, and in more recent year, have set their sights on profiting from Long COVID.
There are far too many examples of them for me to name them all. Kennedy, the quack Levinovitz profiles, charges only a couple hundred dollars an appointment - which, for nonsense, is still far too much IMO - but others are worse.
There's this guy Toby Morrison who runs "CFS Health". He and his website look like a lame Tony Robbins ripoff, complete with high pressure sales tactics. He sells a $500 monthly membership and offers "coaching".
There's the Lightning Process, which costs somewhere around $900-$1500 for a course. There's ANS Rewire and the Gupta Program, which are a series of online videos you pay $500 to access. There's DNRS, which sells $2K seminar tickets.
A lot of these programs have a sort of multi-level marketing feel to them as well. The Gupta Program gives you a pathway to become an "official" Gupta coach. Primal Trust offers a way to refer people into the program. etc.
These programs use social media to ensnare sick people into emptying their pockets. They operate a web of YouTube channels and Facebook groups, some of which I'm in. Below, I'll paste a screenshot of a moderator in one of these groups who seems to be implying that people with chest pain who go to the ER are wasting their time.
Which is maybe the more important point: This stuff isn't just a money-making scheme. It's dangerous and potentially deadly. Essentially, the core tenant is that the symptoms are all in your head, driven by an over-active nervous system, and you just need to think your way out of them.
We have, in fact, run this experiment before. It was called the PACE trial: the idea that these patients are deconditioned and frightened of activity, curable with exercise and a change of beliefs. Patients reported in droves that the exercise made them sicker (74% in one survey) and over time the major bodies reversed course. The CDC now opens its overview of ME/CFS by stating that its a biological illness. What Levinovitz is calling a brave, suppressed paradigm is a long discredited and dangerous theory given a different name.
Although it's lengthy, his article reads like something I might have written as a freshman in undergrad. He just didn't do the work, didn't follow the money, didn't talk to the right people. He doesn't look for the harm caused, or who profits from it.
And so what we wind up with is a lengthy advertisement for alternative medicine in a major publication. I doubt the industry could have bought anything better.

10
74
314
10,300
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

How long have we known about glomeruli? Today’s teaching point is offered in honor of Marcello Malpighi (1628-1694), the Italian anatomist who is credited with having published the world’s first accurate description of glomerular structure (Bologna, Italy 1666). We learn from those who teach us!
Bellomo G. A short history of 'glomerulus'. Clin Kidney J. 2013 Apr;6(2):250-1. PMID: 26019863
Fogazzi GB. The description of the renal glomeruli by Marcello Malpighi. Nephrol Dial Transplant. 1997 Oct;12(10):2191-2. PMID: 9351094.
Image Credit (for oil painting, Malpighi): Wellcome Collection (wellcomecollection.org/)
#TeachingPoints #kidneypath #renal #pathology


8
24
1,158
RT @BigBadDenis: "Bangladesh measles outbreak death toll reaches 585 as two more children die"
Official data shows a severe measles outbre…
26
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

May 29
A colleague asked why I keep masking at work.
“I don’t like Covid.”
“O yeh, worse 2 weeks of my life, I never want that again.”
They take no precautions for one simple reason.
Nobody else is. Humans think and act socially, not individually.
19
77
667
5,858
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

May 29
Not all organs respond equally to #COVID infection. DISCO-seq, a new technique led by my talented friend @HarsharanBhatia, combines 3D imaging and single-cell analysis to map Spike Protein tropism and found mostly in the liver, lungs, intestine & kidneys. biorxiv.org/content/10.64898…
17
236
666
31,140
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

From an autopsy-based case–control study,
"COVID-19–positive cases demonstrated significantly increased reactive gliosis and microglial activation in the olfactory bulb, along with a higher frequency of mild perivascular lymphocytic infiltration in the frontal cortex..
Systemic pathological findings in COVID-19–positive cases were consistent with severe multisystem disease.
[In conclusion,] COVID-19 is associated with region-specific but non-uniform neuropathological alterations dominated by reactive and vascular changes rather than encephalitic processes."
People change after contracting COVID.
'Histopathological changes in the olfactory pathway in COVID-19: An autopsy-based case–control study'
link.springer.com/article/10…
8
129
306
22,241
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

May 22
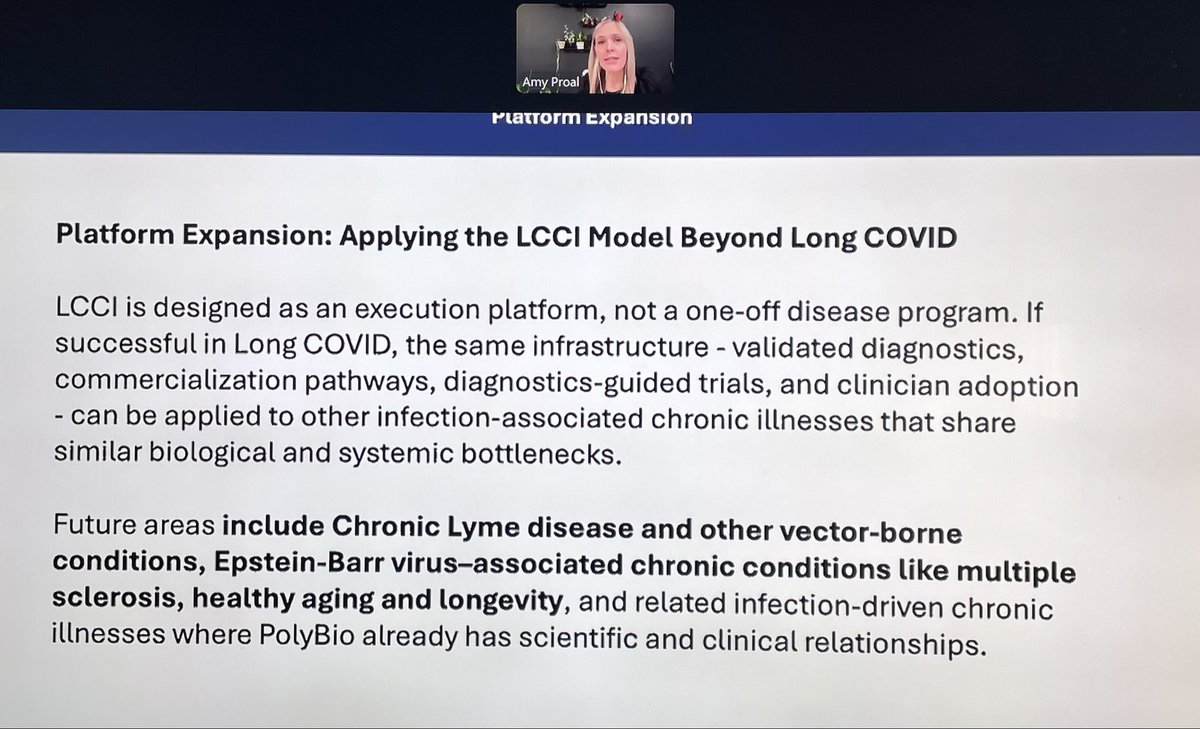
Follow along with the #polybiospringsymposium2026 in this thread👇🏻
11:00 am ET—Dr. Amy Proal kicked off this Spring symposium with an overview of PolyBio’s new commercialization network that will help translate Long COVID biomarkers from the lab & therapies from coordinated clinical trials into useful tools in the clinic. She also discussed how this commercialization infrastructure can be applied to other IACIs.
23
57
174
24,696
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

May 24
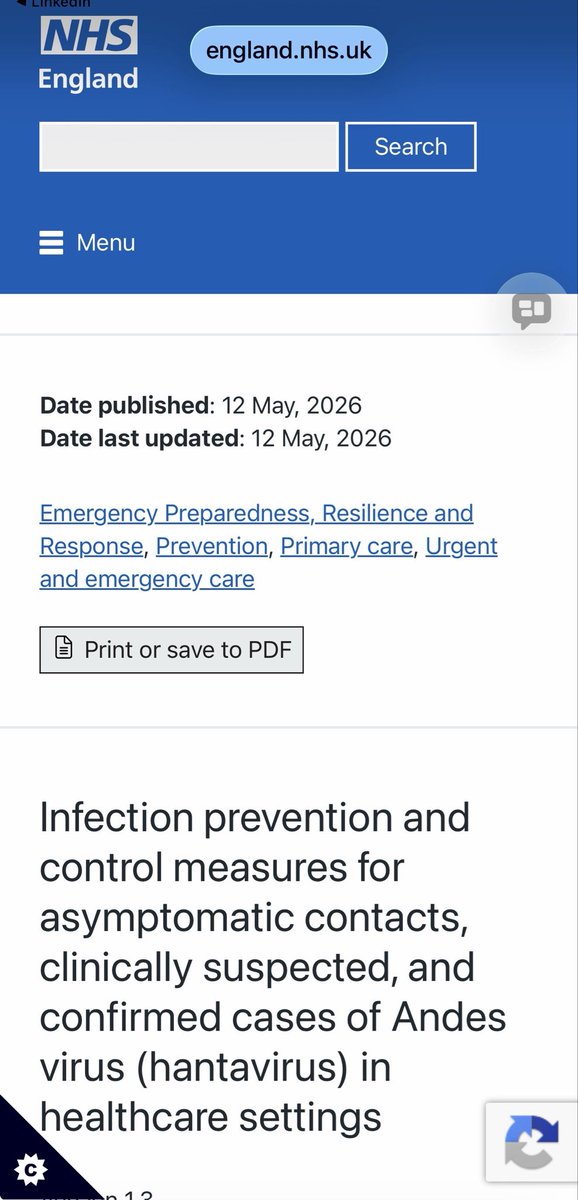
Has everyone seen this new NHS UKHSA guidance for ANDV?
***FFP3 RESPIRATORS ***
For EVERYONE in Healthcare
Patients & Staff
In contact w suspected cases
And contacts
I kid you not
Hell hath frozen over
👏👏👏
england.nhs.uk/long-read/ipc…
23
231
739
32,847
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

May 21
This may be one of the more important long COVID papers in a while.
A new study in Frontiers in Immunology suggests that COVID can trigger new-onset insulin resistance - and that this may drive abnormal NETosis in neutrophils months after infection🧵
16
262
753
25,877
Dr Satoshi Akima FRACP 『秋間聰』 retweeted
May 19
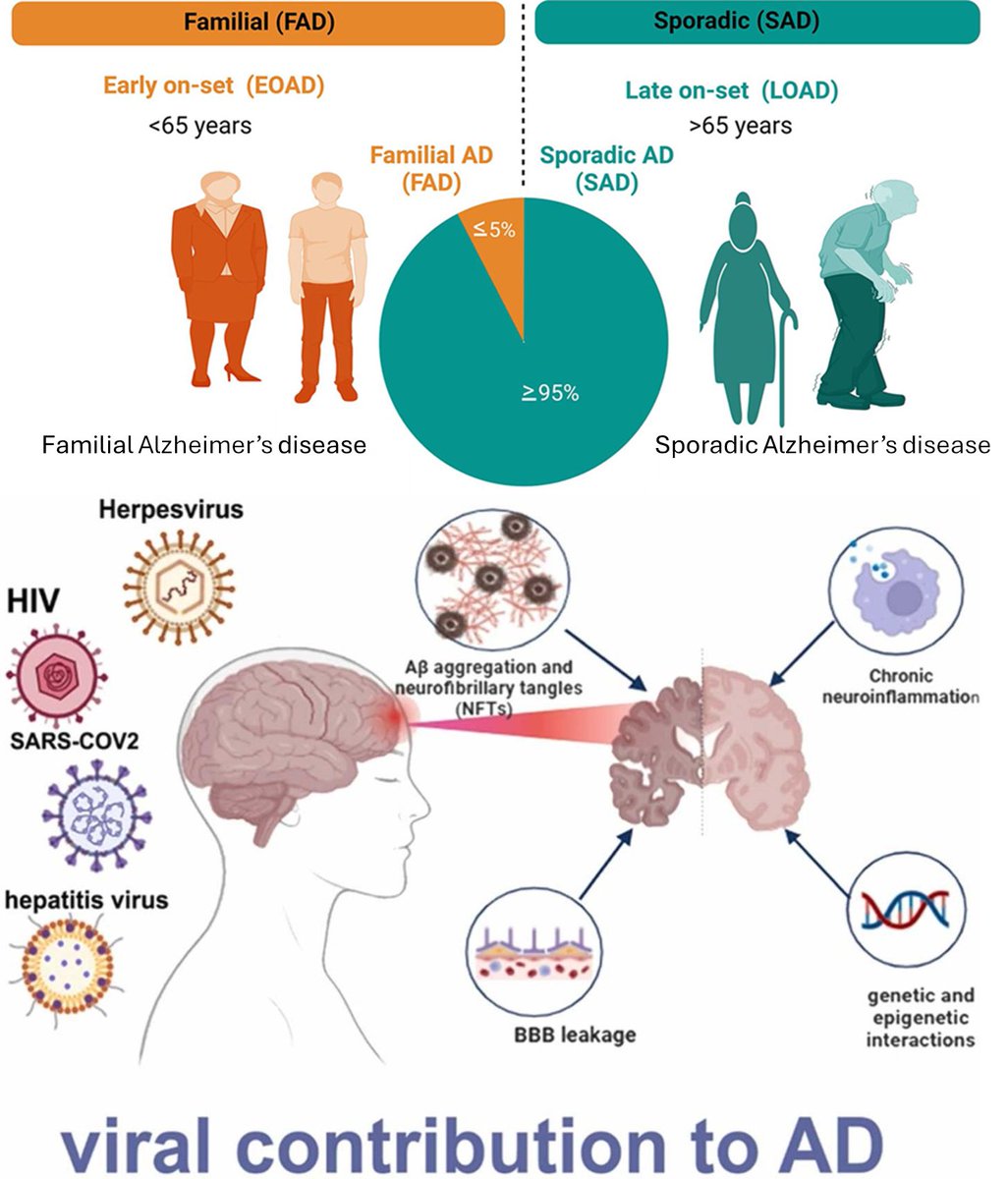
It is interesting to me that many people assume dementia “runs in the family,” when most dementia cases are actually sporadic rather than directly inherited. Family history can increase risk, but truly hereditary forms are relatively rare.
#Alzheimer, for example, is the most common cause of dementia, accounting for an estimated 60–80% of cases. Yet only about 5% of Alzheimer’s cases are caused by inherited genetic mutations, and these forms usually begin at a younger age.
Most cases develop from a combination of aging, vascular health, lifestyle and environmental exposures, including to pathogens.
We know that conditions such as high blood pressure, diabetes, high cholesterol, obesity, and heart disease damage blood vessels and increase dementia risk because the brain depends heavily on healthy circulation. These conditions can disrupt the blood–brain barrier (BBB), increasing its permeability and allowing inflammatory molecules and other harmful substances to affect brain tissue.
Physical inactivity and poor sleep also play an important role. Regular exercise supports blood flow, reduces inflammation, and improves insulin sensitivity, while chronic sleep disruption is associated with increased accumulation of abnormal proteins linked to Alzheimer such as tau (NFTs) and amyloid (AB).
What receives less attention is the growing evidence that some infections may also contribute to dementia risk through several possible mechanisms.
Can be direct infection of the brain cells (seen in HIV, #Covid, herpesviruses and others) or by chronic immune activation and inflammation, which damage blood vessels and contribute to vascular impairment. There is also growing research linking reactivation of dormant viruses after an infection, and interactions between infections contributing to dementia in some individuals.
Overall, chronic systemic inflammation appears harmful to brain health. Repeated severe infections or persistent inflammatory states may contribute through vascular damage and prolonged immune activation.
There is still a great deal we do not understand about dementia and neurodegenerative diseases, which is one reason why truly effective treatments are still not available.
19
254
729
15,914
Dr Satoshi Akima FRACP 『秋間聰』 retweeted

May 20
Transmission of #Ebola is being debated yet again. In the catastrophic West African epidemic in 2014, health workers were forced to work in surgical masks and many got infected. Medical journals refused to publish us, instead, publishing articles saying "less PPE is better". A nursing journal published us, because #nurses are at the frontline 1/2 sciencedirect.com/science/ar…
33
347
913
89,386
Dr Satoshi Akima FRACP 『秋間聰』 retweeted
May 17
"Is there any situation or scenario in which somebody could produce a droplet, but not produce a significant amount of aerosol?"
"No"
- Professor Clive Beggs
Right question, right answer
👏👏👏

10
370
1,191
20,946