
Genomics company changing patient care through molecular diagnostics and the Molecular Microscope® (MMDx®) service.
- Tweets 208
- Following 232
- Followers 118
- Likes 138








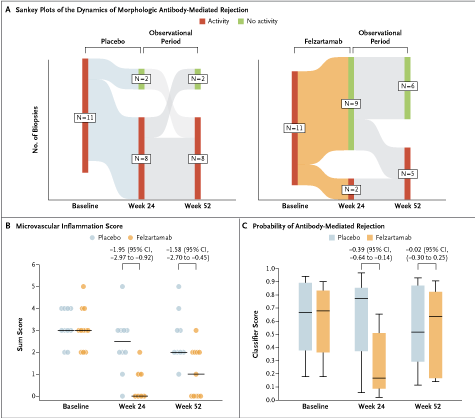
ALT Panel A: Sankey plots of the dynamics of morphologic antibody-mediated rejection (active or chronic active) as compared with no activity (chronic inactive or no rejection) in the felzartamab and placebo groups across biopsy samples obtained at baseline, week 24, and week 52. Panel B: The microvascular inflammation score (a sum score of glomerulitis and peritubular capillaritis) in biopsy samples according to the Banff classification at baseline, week 24, and week 52. Panel C: Molecular score reflecting the probability of antibody-mediated rejection in biopsy samples obtained at baseline, week 24, and week 52.
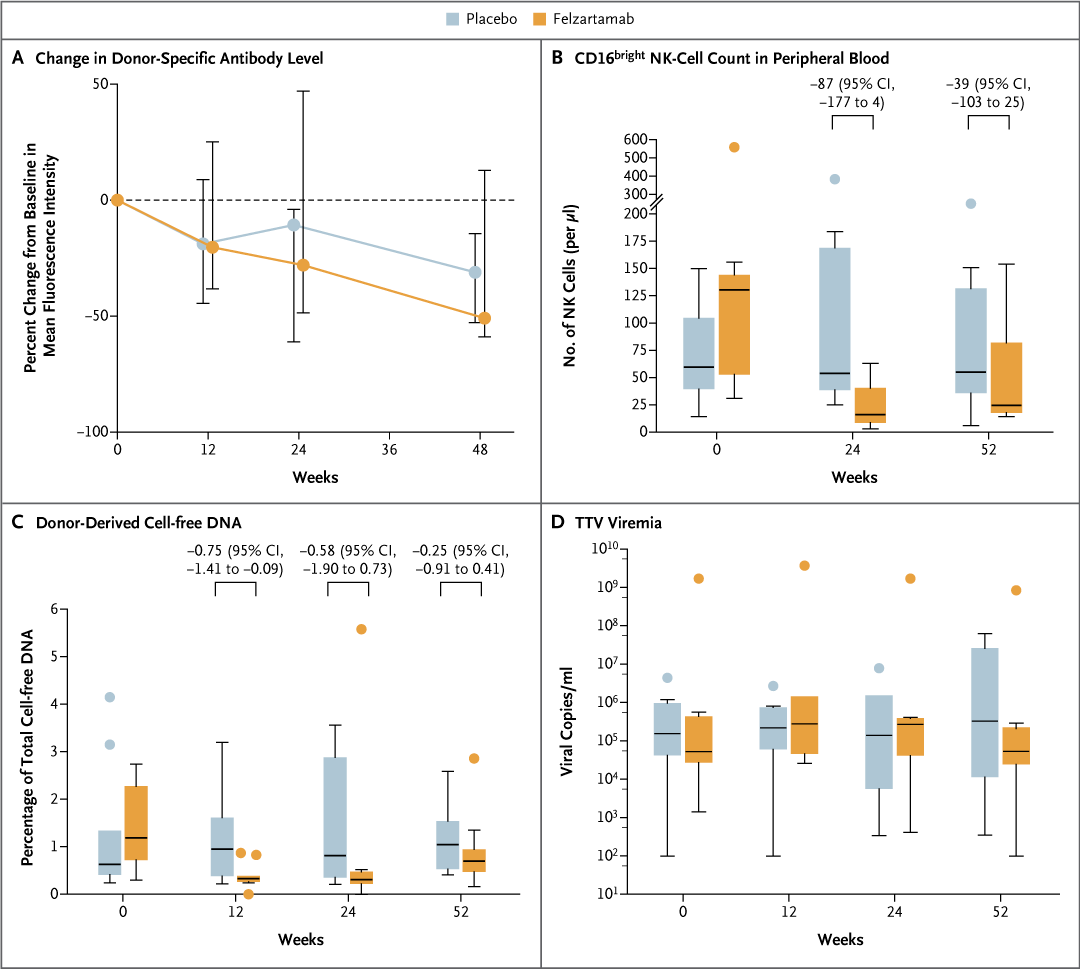
ALT Panel A: Graph with line plots and I bars showing the percent change in the mean fluorescence intensity of donor-specific antibody in the two trial groups. Panel B: Box plot of peripheral-blood CD16bright NK-cell counts. Panel C: Box plot of the fraction of donor-derived cell-free DNA. Panel D: Box plot of the number of copies of torque teno virus (TTV).