
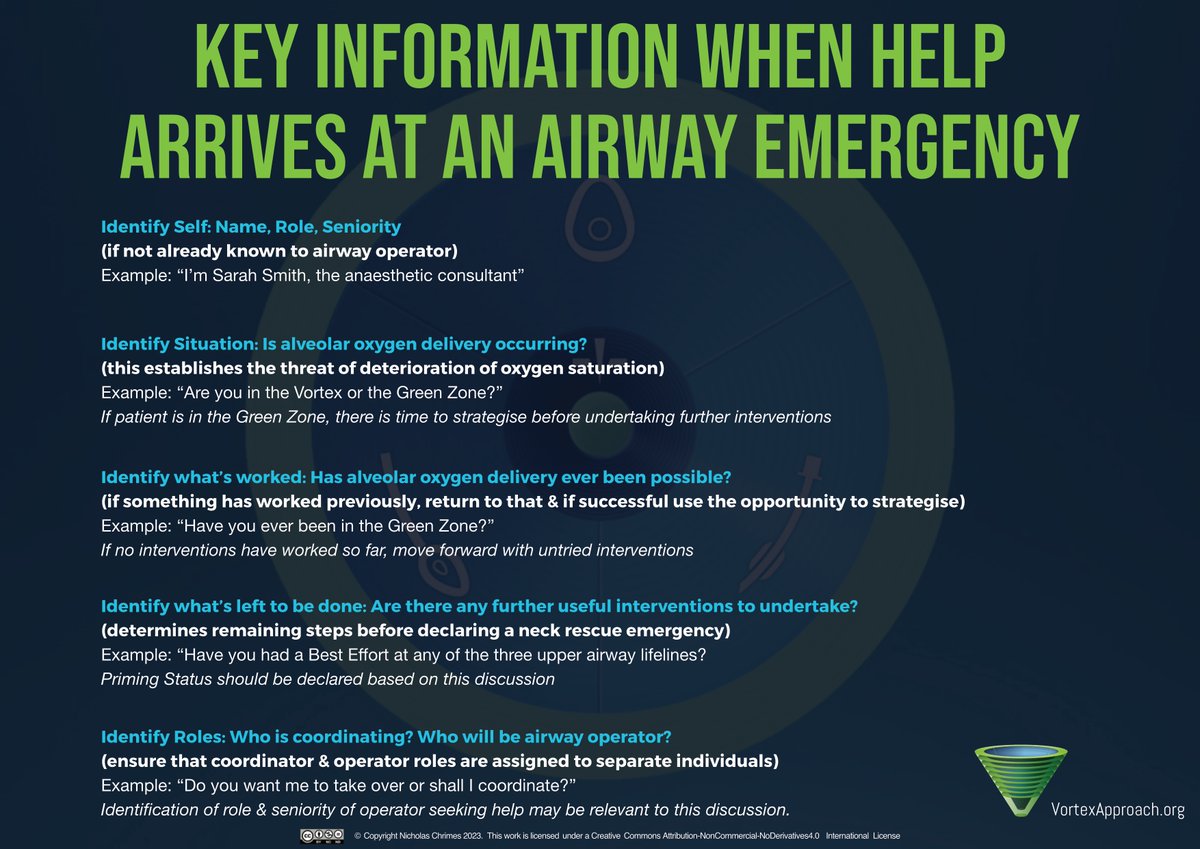
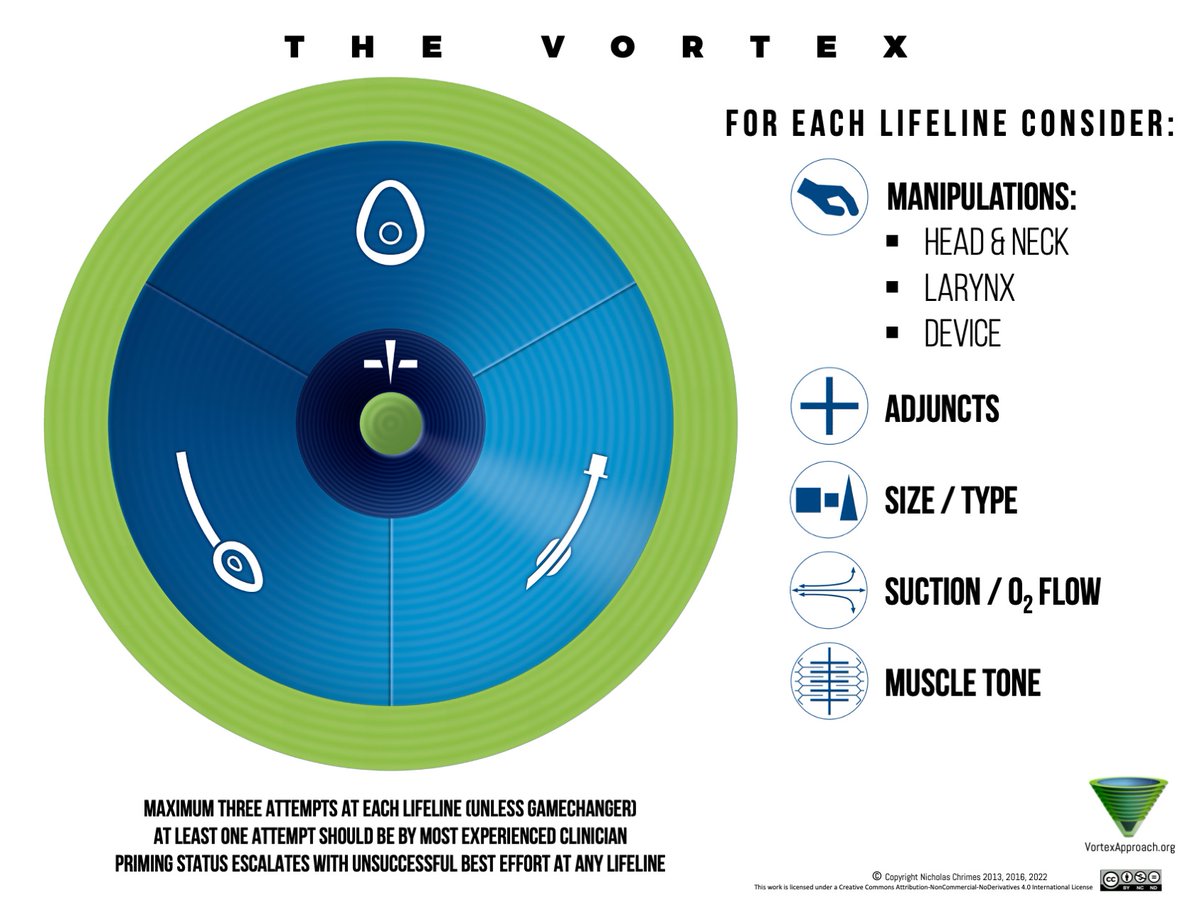
Implementation tool for airway Mx by @NicholasChrimes. Addresses human factors considerations to facilitate real time use by teams during a crisis.
Joined September 2014
- Tweets 1,465
- Following 206
- Followers 3,746
- Likes 144
91 Photos and videos








The Vortex Approach retweeted

SAS President @EllardLouise will be part of the faculty for #SASNoosa2026
Join us at the Elysium Noosa Resort Fri 28th Aug (don't forget the Airway SIG meeting on Thu 27th Aug at the same venue)
Details: sas-sas2026-annual-meeting.e…
Airway SIG details: anzca.edu.au/events-and-cour…

4
3
313
The Vortex Approach retweeted
We're excited to welcome @cliffreid as one of our keynote speakers at #SASNoosa2026. Join us at the Elysium Noosa Resort Fri 28th Aug (& don't forget the Airway SIG meeting on Thu 27th).
Workshops, panel discussions, guideline launches & more.
Details: sas-sas2026-annual-meeting.e…
5
5
863
The Vortex Approach retweeted
Thrilled to have @dasairway President, Prof @altgm as a keynote speaker at #SASNoosa2026.
His small group discussion session on Airway Leads with @DrRaniChahal has already SOLD OUT!
Elysium Noosa Resort Fri 28th Aug (Airway SIG meeting 27th Aug)
Details sas-sas2026-annual-meeting.e…
7
6
754
The Vortex Approach retweeted
Australia & New Zealand's leading airway education organisations come together for the 1st time for back-to-back meetings at the Elysium Resort Noosa.
Registration:
SIG Meeting: anzca.edu.au/events-and-cour…
SAS Meeting: sas-sas2026-annual-meeting.e…

4
1
269
The Vortex Approach retweeted
A few places still available for our Gosford Airway Workshop this Saturday morning (& optional Airway Ally workshop on Friday afternoon for airway assistants).
Station Leads:
Neck Rescue: Adam Rehak
HAVL/VAFI: @NicholasChrimes
Trachy/lary emergencies : Jon Gatward

Registrations are open for our Gosford Airway Workshop Sat 9th May.
3 x 90 min stations:
HAVL/VAFI
Trache/Lary Emergencies
Neck Rescue
More details here: sasevents.eventsair.site

4
5
500
The Vortex Approach retweeted

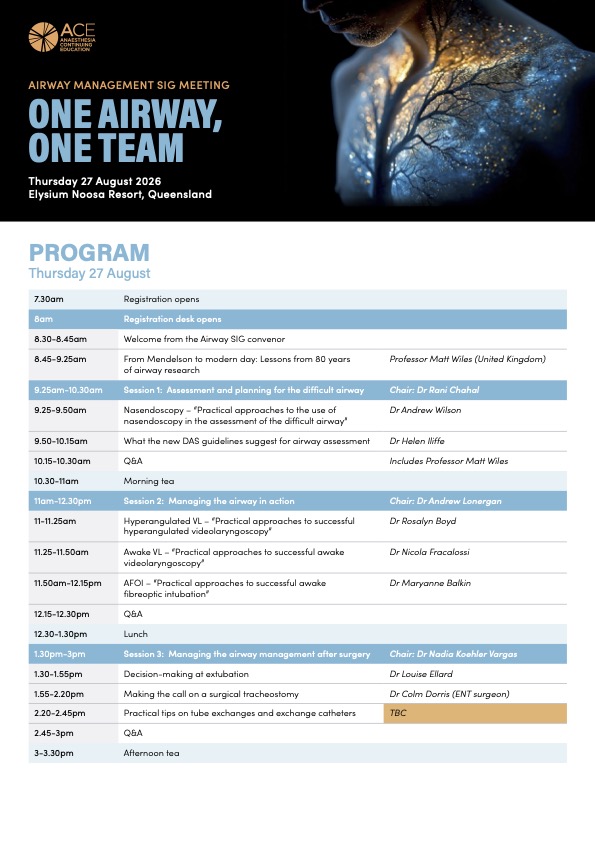
At the SIG meeting @EllardLouise will be presenting the PUMA extubation guidelines. The next day at the @SafeAirway annual meeting @NicholasChrimes & @AndyHiggsGAA will launch another PUMA guideline.
2 days of PUMA goodness from @ANZCA @ASA_Australia @TheNZSA & @SafeAirway!
Separate registrations required:
Airway management SIG Meeting: anzca.edu.au/events-and-cour…
SAS Annual Meeting: sas-sas2026-annual-meeting.e…
5
849
The Vortex Approach retweeted
Australia & New Zealand's leading airway education organisations come together for the 1st time for back-to-back meetings at the Elysium Resort Noosa.
Speakers include @altgm @STHJournalClub @cliffreid @DrRaniChahal @EllardLouise @NicholasChrimes @iliff_helen @AndyHiggsGAA

1
9
9
1,078
The Vortex Approach retweeted
Our Melbourne airway workshop yesterday was a huge success!
Limited places still available for Gosford on Sat 9th May.
Registrations for Darwin on Sat 13th Jun are now open!
Registration also open for annual meeting in Noosa on Fri 28th Aug.
safeairwaysociety.org/sas-ev…

4
7
519
The Vortex Approach retweeted
Registrations are open for #SASNoosa2026!
Great faculty including keynotes @dasairway President @altgm and @SydneyHEMS's @cliffreid.
Check out the program & register here: sas-sas2026-annual-meeting.e…
1
3
2
1,100
The Vortex Approach retweeted

Cricoid pressure facts from @doctimcook
There’s no RCT evidence it reduces aspiration risk but there’s also no RCT evidence that ANY component of RSI reduces aspiration risk.
Meanwhile, CP does have a reasonable amount of other experimental evidence that it works. No other component of RSI has ANY evidence at all!
22 Nov 2025

The evidence is uncertain
There is logic to its use inasmuch as
-aspiration is a significant complication and efforts to prevent it merit careful examination
-cricoid occludes the upper GI tract (hypopharynx)
-the metrics for correct cricoid are well defined
3 kg
one hand
unable to sustain > 5 mins
-it’s easy to teach (closed 50 ml syringe, compress air from 50-32 ml) achieves good accuracy /-0.5 kg which keeps in effective and safe range
-when applied correctly it has either nil or minimal impact on airway management
-if its causing a problem, take it off and you’ve lot nothing
The biggest challenge is
-teaching it correctly
-correctly identifying cricoid ( we should use more USS)
-misinformation and a view that absence of evidence equals evidence of absence of benefit
Embrace and accept uncertainty
So I use RSI in high risk cases
3
10
27
6,608
The Vortex Approach retweeted
“In the present day, unrecognised oesophageal intubation is a blight on airway management. It causes regular airway deaths, all of which are entirely avoidable and most of which are likely either never identified or never reported”
From @doctimcook. Free full text in @ResusJournal
Feb 10
Delighted to see this editorial published in Resuscitation
Described as hard hitting it addresses
- the ongoing and unacceptable high rates of unrecognised oesophageal intubation in some out of hospital settings
- current methods to reduce this
- future opportunities to make this even more failsafe
authors.elsevier.com/a/1matS…
7
11
2,220
The Vortex Approach retweeted

Feb 10
Delighted to see this editorial published in Resuscitation
Described as hard hitting it addresses
- the ongoing and unacceptable high rates of unrecognised oesophageal intubation in some out of hospital settings
- current methods to reduce this
- future opportunities to make this even more failsafe
authors.elsevier.com/a/1matS…
3
21
55
7,002
The Vortex Approach retweeted
Registrations are open for the Melbourne & Gosford stops on our 2026 #AirwayWorkshopRoadshow.
3 x 90min stations
HAVL & VAFI
Trache/Lary Emergencies
Neck Rescue
Secure your place here: sasevents.eventsair.site/reg…
2
262
The Vortex Approach retweeted
Deaths from unrecognised oesophageal intubation continue to occur. We are all vulnerable to making this error. Ensure your department is familiar with the guidelines for preventing a tragic outcome.
Free full text in @Anaes_Journal
associationofanaesthetists-p…

The full Coroner's Report on yet another case of unrecognised oesophageal intubation.
agd.nt.gov.au/__data/assets/…
6
8
1,998
The Vortex Approach retweeted
Save the date for #SASNoosa26.
Held in collaboration with the @ANZCA @ASA_Australia @TheNZSA Airway Management SIG meeting, get ready for 2 days of high quality airway education 27th & 28th Aug in Noosa Heads, QLD

3
5
692
The Vortex Approach retweeted
Feb 6
Why not use RSI for all patients on a GLP1 agonist?
First - because (as per my previous tweet) the risk of aspiration is >600-fold lower than the risk of having a full stomach
Second because RSI is not a benign technique
- increases risk of failed intubation 8-fold
- increases risk of anaesthetic overdose (CVS instability etc)
-increases risk of anaesthetic under dose (awareness)
Etc etc etc
If using muscle relaxants and TT when otherwise would be using an SGA
-increases risk of airway complications at insertion and removal from use of TT
-increases risk of anaphylaxis from NMBA
-and awareness (from NMBA)
So I think quite a few reasons to pause before deciding swathes of folk need RSI
3
15
52
7,509
The Vortex Approach retweeted
Great point about not endlessly suctioning in pulmonary oedema. Common error in my experience.
Suction in this situation is to reveal the glottis, not clear fluid from the lower airway.
Clearing lower airway of pulmonary oedema fluid requires application of *positive* not negative pressure.
Once you can identify the glottis, get the patient intubated & ventilated w PEEP rather than pfaffing around trying to vacuum up pulmonary oedema fluid (which will keep coming until there’s no plasma left)!
8 Oct 2025

From TBS25, Mega-talent and future legend Luca Ünlü on the dark art of managing the contaminated airway!
youtu.be/EpW_U1RcV6Q?si=oMFQ… via @YouTube
1
4
10
2,121
The Vortex Approach retweeted
Feb 4
Great to see this published
Emergency Front of Neck Airway registry (eFONAr)
Coming to the UK soon
@elboghdadly @dr_imranahmad @altgm (@NicholasChrimes)
bjaopen.org/article/S2772-60…
2
10
33
3,733
The Vortex Approach retweeted
Save the date for the @SafeAirway 2026 Annual Meeting.
Held in collaboration with the @ANZCA @ASA_Australia @TheNZSA Airway Management SIG meeting the shared theme is 'One Airway, One Team'.
Register interest here for alerts when registrations open.
sasevents.eventsair.site/con…

5
5
715
The Vortex Approach retweeted
Registrations are now open for the @SafeAirwaySociety's Gosford Airway Workshop. Come learn HAVL, VAFI, Neck Rescue & management of tracheostomy/laryngectomy emergencies on NSW's sunny Central Coast.
Qualifies for @ANZCA & @CICMANZ CPD
Register here: sasevents.eventsair.site/reg…

5
4
1,625