
Joined May 2016
- Tweets 8,159
- Following 196
- Followers 5,294
- Likes 12,125
429 Photos and videos














Jun 9
Thoughtful and reasonable assessment. Administrators should reflect on this.
@HeartOTXHeartMD what is your impression?
The Cath Lab Cliff: A Warning Sign of a System in Fracture on @cardiacinterv citoday.com/articles/2026-ma…
1
3
8
1,079
Jack Hall retweeted

Jun 3
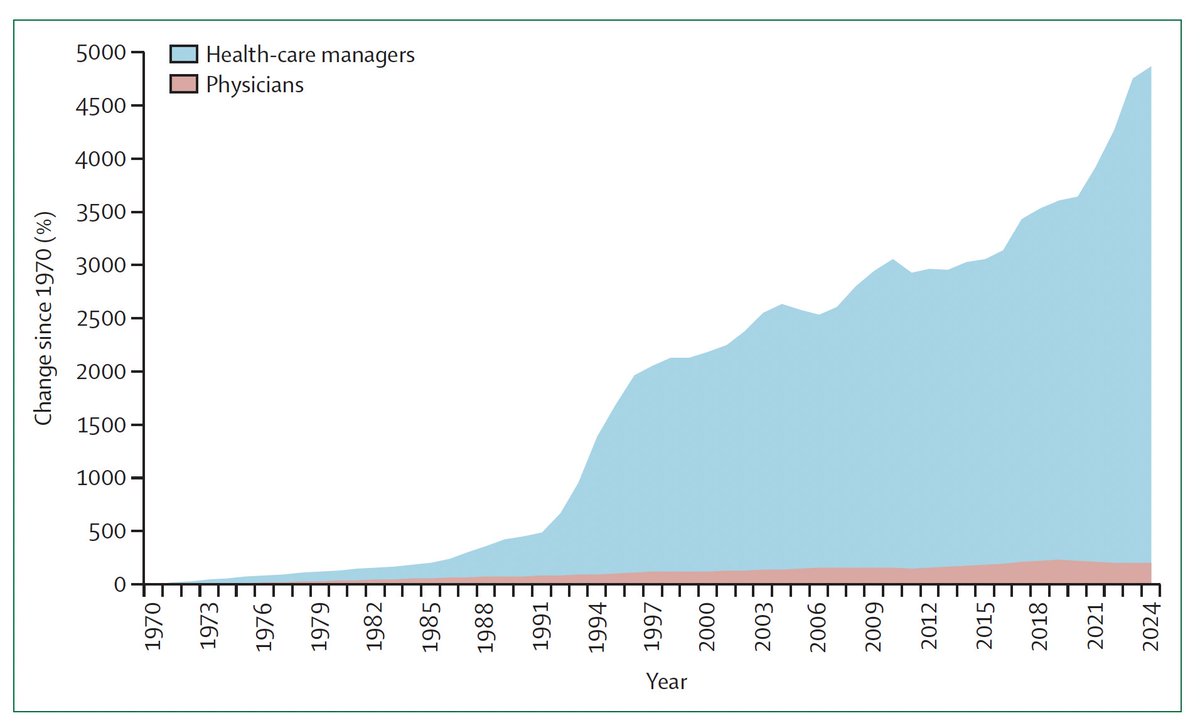
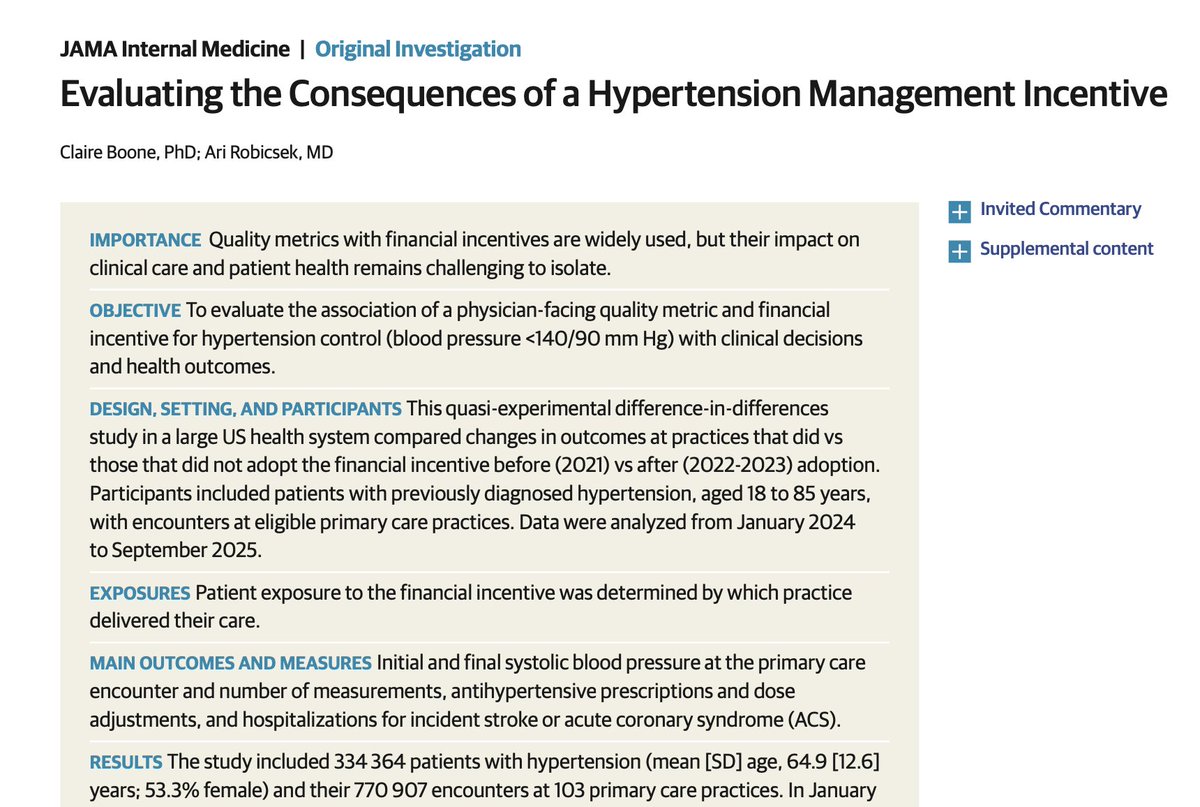
Extraordinary study in JAMA IM confirms what many of us have warned against: "pay-for-performance" incentives in medicine reward "teaching to the test" with potentially harmful results
In this quasi-experimental study, incentivizing doctors to control blood pressure (BP)...
1/X
11
34
110
79,765
Jack Hall retweeted
Jun 3
An absolutely beautiful result. This brings art back to PCI, "where, when, & how to" matter. Obviously, the restenosis rate is important as there is a lot of vessel at risk. Naysayers will point to costs, time, equipment utilized vs just "slapping" a stent in.
Well done.
1
2
644
Jack Hall retweeted

May 30
Thomas Sowell: “It is amazing that people who think we cannot afford to pay for doctors, hospitals, and medication somehow think that we can afford to pay for doctors, hospitals, medication and a government bureaucracy to administer it.”

6
93
312
4,786
May 24
Thoughts and prayers for all who gave the "last full measure" for our country.
And thank you to all who served and are serving!
119
Jack Hall retweeted

When I was an intern I developed massive acute bronchospasm from exposure to cat dander. I ended up intubated in the ICU at one of my program’s teaching hospitals. Thanks to high dose steroids, I was extubated the next day. The nurse then handed me the phone to answer a call.
27
20
833
403,066
Jack Hall retweeted

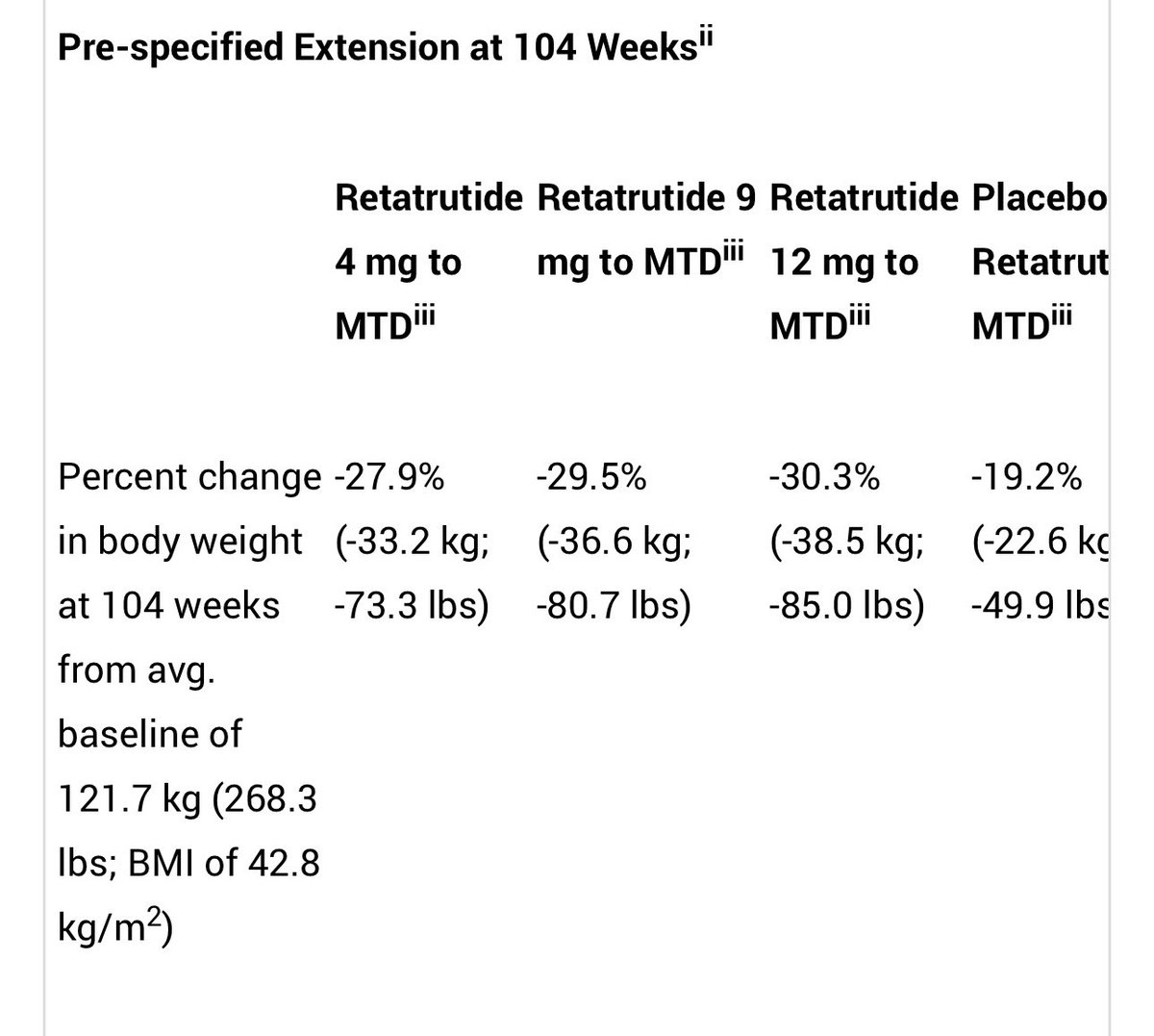
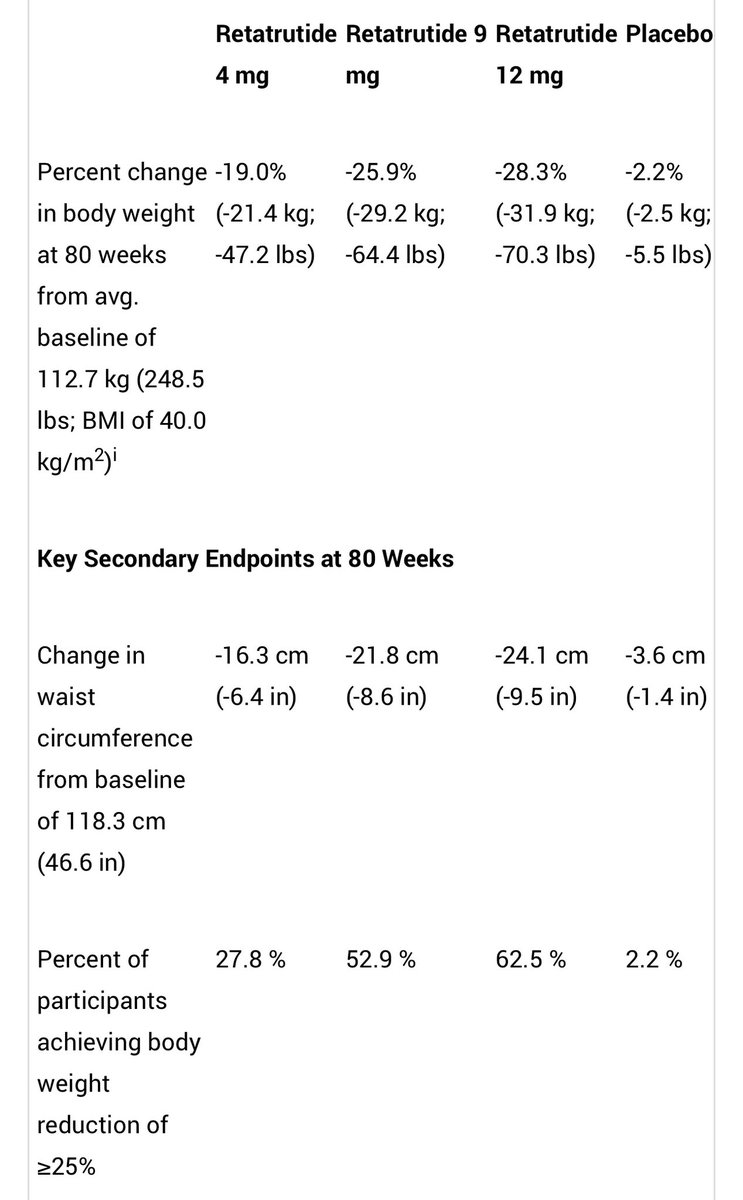
Retatrutide, a first-in-class GIP, GLP-1, and glucagon triple hormone receptor agonist, was studied in adults with obesity & at least one weight-related comorbidity and without diabetes.
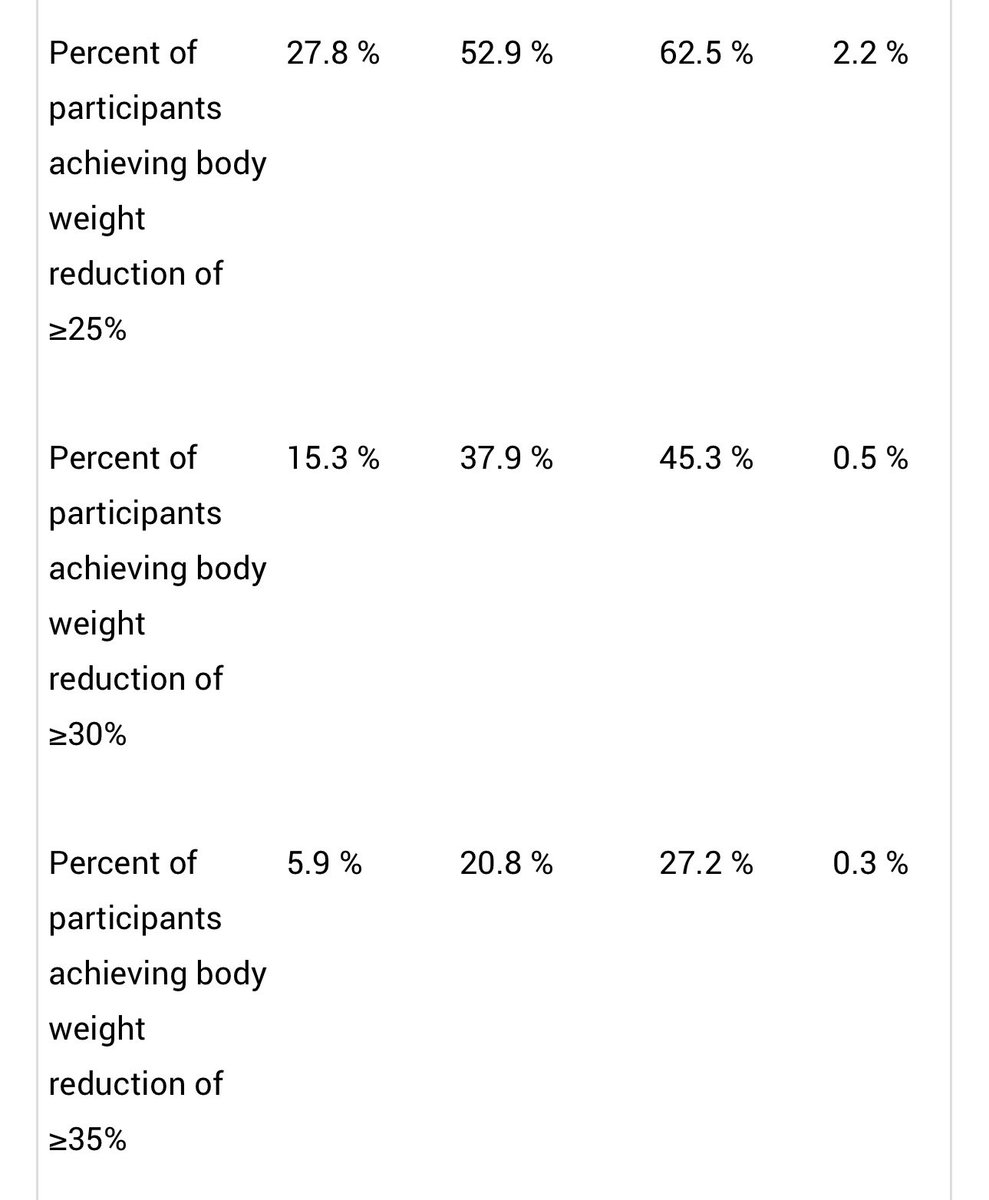
Pts on 12 mg retatrutide lost an average of 70.3 lbs (28.3%) over 80 weeks with 45.3% of participants achieving ≥30% weight loss.
Individuals with a baseline BMI ≥35 who participated in a study extension continued to lose weight, and achieved up to an average of 85.0 lbs (30.3%) weight loss at 104 weeks.
investor.lilly.com/news-rele…
3
23
51
5,077
Jack Hall retweeted
The mean age of physicians who leave clinical practice in the US is now 48.1 years, 9 years younger than observed in a similar cohort in 2008.
The biggest causes cited were stress and the hassles of practice.
11% of women decided not to even enter practice.
What are your thoughts about this?
thepermanentejournal.org/doi…
106
145
553
498,143
Jack Hall retweeted

May 18
Last year was so proud to see the Radial Access Sleeve to make the innovation section at Europcr . NAPs making a difference too

May 18

“Innovators Day is not only for physicians.”
In this interview with @CurioJonathan, @AndreaScotti21 explains how #PCRID brings together physicians, entrepreneurs, innovators and investors to discuss the future of cardiovascular innovation. 🚀🫀
#EuroPCR #PCRID
4
13
3,094
Jack Hall retweeted

The Market Has Already Delivered Its Verdict. Only Organized Medicine Has Not.
The institutions that actually credential and reimburse physicians have spent the last three years reaching a conclusion about Maintenance of Certification that organized medicine refuses to acknowledge. These are not the specialty boards, not the AMA, and not the organizations that profit from mandatory participation. They are the bodies that determine whether hospitals and health plans operate with national accreditation, the federal agencies that govern competition in healthcare markets, and the commercial insurers that cover the majority of working Americans. Their verdict is documented in formal credentialing policy changes, updated accreditation standards, federal regulatory guidance naming unnecessary physician recertification as a potential antitrust violation, and bylaw amendments now adopted by more than 250 hospitals and health systems. It is not close and it is not preliminary.
Every major national accreditation body has formally recognized NBPAS as meeting its standards. The Joint Commission designated NBPAS as a Designated Equivalent Source Agency effective July 1, 2022, adding it to the glossary of accreditation manuals covering hospitals, ambulatory care, behavioral health, critical access hospitals, and office-based surgery facilities. The National Committee for Quality Assurance included NBPAS in its 2022 Health Plan Accreditation Standards and Guidelines. URAC, DNV, the Center for Improvement in Healthcare Quality, and the Accreditation Commission for Health Care have all confirmed that NBPAS meets their standards. Their collective recognition of NBPAS means that no credentialing or accreditation standard requires ABMS recertification as a condition of hospital or health plan operation. The ABMS gate is not an accreditation requirement. It is a private preference enforced through institutional inertia. ABMS's response to the Joint Commission's independent designation was to distribute what it called a toolkit created specifically to address what ABMS characterized as NBPAS's false inferences that an NBPAS certificate is equivalent to ABMS certification. The Joint Commission made that designation based on its own standards. ABMS responded by mounting a coordinated institutional campaign to undermine hospital recognition of an organization the nation's premier accreditor had just formally approved.
The federal signal arrived in April 2024, but its foundation had been laid seven months earlier. NBPAS formally filed a complaint with the FTC in September 2023, arguing that ABMS and its constituent boards were using monopoly power to exclude competitors from the continuing certification market. In April 2024, the FTC, DOJ, and HHS jointly launched HealthyCompetition.gov, a portal for public reporting of anticompetitive practices in healthcare, and explicitly listed unnecessary healthcare provider recertification or accreditation requirements as an example of potentially anticompetitive conduct that may raise the costs of practicing medicine and reduce the number of healthcare practitioners. The sequence is clear. NBPAS filed the complaint. Seven months later, the federal government launched a portal naming the exact conduct NBPAS had identified. Three months after that, in July 2024, CMS updated its guidance on End Stage Renal Disease Medical Directors to formally accept NBPAS-certified nephrologists, including in rural areas and federally-designated Health Professional Shortage Areas. The federal government identified mandatory physician recertification as a potential antitrust violation and then changed its own clinical guidance in the same direction within the same year.
The three largest commercial insurers have followed. UnitedHealthcare, the largest health insurer in the United States, formally confirmed in a letter to NBPAS that its credentialing policies do not require participation in MOC programs, that physicians certified by NBPAS may be credentialed under its existing policies, and that physician competency is best demonstrated through initial board certification, ongoing clinical practice, and a commitment to lifelong learning. That statement is a precise repudiation of the ABMS mandatory recertification model, delivered in writing by the organization that insures more Americans than any other. Elevance Health, formerly Anthem, operates Blue Cross Blue Shield plans in 14 states and covers more than 115 million lives. Elevance accepts NBPAS under its alternative credentialing criteria for physicians with ten or more years of clinical experience. Health Care Service Corporation, the largest customer-owned health insurer in the United States, operating Blue Cross Blue Shield plans in Illinois, Montana, New Mexico, Oklahoma, and Texas, formally accepts NBPAS board certification. Blue Cross Blue Shield of Massachusetts, a five-star NCQA-rated plan, has accepted NBPAS. The American Thoracic Society has added NBPAS as a recognized board certification option in its professional database.
Hospital adoption is accelerating entirely through physician-led bylaw amendments, requiring no legislation and no institutional permission beyond a Medical Executive Committee vote. NBPAS is now recognized by more than 250 hospitals and health systems nationwide. Forty-four hospitals added NBPAS to their bylaws in 2025 alone. Named institutions include HCA Florida Woodmont Hospital, Ascension Saint Thomas hospitals in Tennessee, WVU Medicine, hospitals in the ScionHealth network, Hackensack Meridian Health in New Jersey, and St. Joseph's Health Hospital in Syracuse. Most hospitals, as NBPAS has documented, simply were not aware that an alternative existed.
The single most instructive holdout is Blue Cross Blue Shield of Michigan. Despite a physician-led campaign of more than 40 formal requests, intervention from Governor Whitmer's office, and a direct response request from the Michigan Department of Insurance and Financial Services, BCBSM refused to remove its MOC requirement. BCBSM holds more than 80 percent of the commercial insurance market in Michigan. That market concentration means a single insurer's refusal to recognize NBPAS functions as an effective statewide prohibition regardless of what any hospital bylaw or state legislature has done. Dr. Robert Vanderbrook is a solo family medicine physician in Clare, Michigan, practicing in a federally-designated Health Professional Shortage Area, which is a community the federal government has formally identified as lacking adequate physician access. BCBSM removed him from its networks because he chose NBPAS over ABFM recertification. Many of his patients refused to go elsewhere and opted to pay out of pocket to continue seeing him regardless of the financial strain. The BCBSM position is not an argument for the ABMS patient safety rationale. It is an illustration of what market-dominant enforcement of a discredited mandatory program looks like when it lands on a real physician in a real community that cannot afford to lose him.
The state legislative map tells the same story the market has told. Fifteen states have now passed laws limiting or restricting MOC requirements as a condition of physician practice. Six of them (Oklahoma, Texas, Georgia, South Carolina, Arkansas, and Tennessee) have passed comprehensive legislation prohibiting state licensing boards, insurance providers, and hospitals from requiring MOC participation as a condition of licensure, hospital privileges, or insurance panel participation. Oklahoma was first in 2016. Texas followed, with a bill signed by Governor Greg Abbott and sponsored by two physician-legislators: Senator Dawn Buckingham, MD, and Representative Greg Bonnen, MD. Georgia, South Carolina, and Arkansas followed. Nine additional states (Washington, Arizona, North Carolina, Kentucky, Missouri, Maine, Maryland, and others) have passed starter legislation, typically beginning with the licensure provision and building from there. More than a dozen others have introduced legislation that is pending or has expired in prior sessions. The pattern is consistent: a state begins with a narrow bill, builds legislative familiarity with the issue, and returns the following session with broader protections. The AMA's formal policy position has not changed. The enforcement infrastructure beneath it is being systematically removed, one state at a time.
Texas is the most instructive case study because it shows both the momentum and the remaining friction in a single legislative cycle. Texas SB 2207, which would have allowed NBPAS-certified physicians to truthfully advertise as board certified with full disclosure of their certifying board's name, passed the Senate Health and Human Services Committee unanimously at 7-0, passed the full Texas Senate 29-2, and passed the House Public Health Committee 9-1. The bill did not reach a House floor vote before the session ended. In a session where more than 7,000 bills were introduced and only 437 became law, SB 2207 ran out of calendar time rather than political support. The TMA's official policy states it opposes mandatory MOC requirements for licensing, health plan contracting, and hospital credentialing, citing excessive cost, time away from patients, and lack of sufficient research documenting benefits to patient care. Notwithstanding that official position, the TMA testified against SB 2207 before the House Public Health Committee on May 12, 2025, a hearing that ran through the night and concluded testimony at 2:30 in the morning. Physicians who had driven hours to testify in support could not wait out the schedule.
At the TMA's House of Delegates meeting in April 2026, physician members introduced Resolution 202, which would have required the TMA to support efforts to amend Texas Medical Board advertising rules to allow NBPAS-certified physicians to advertise as board certified. The resolution came within two percentage points: 48 percent in favor, 52 percent opposed. That vote is a leading indicator. Nearly half of the TMA's own physician delegates voted to require their association to stop opposing legislation their colleagues in the Texas Senate supported 29-2. The trajectory of that number across future sessions is the story. The AMA holds its formal policy. The states are moving regardless and within the state medical associations themselves, the physician membership is closing the gap between what organized medicine says and what practicing physicians actually want.
The policy argument for Congress, state legislatures, and hospital medical staffs is now straightforward. The market, the federal regulators, and every national accreditation body have reached their verdict. The largest commercial insurers have concluded in writing that mandatory ABMS MOC is not necessary for physician credentialing. The FTC and DOJ have named unnecessary physician recertification as a potential antitrust violation. The Joint Commission, NCQA, URAC, and DNV have all recognized the alternative. Two hundred and fifty hospitals have made the bylaw amendment. Fifteen states have passed legislation. The only institutions still treating ABMS MOC as the exclusive and mandatory pathway are the ABMS itself, the AMA, and a handful of insurers with sufficient market dominance to enforce a requirement the rest of the market has abandoned. What remains is not a debate about evidence or patient safety. That debate is over. What remains is finishing the work.

1
14
15
1,393
Jack Hall retweeted

Do you use 4fr catheters for coronary angiogram @SCAI @SCAI_WIN @DrMahirElder @chadialraies @BinitaShahMD @Allison_Dupont @SVRaoMD @arnoldseto @MortonKern @JDawnAbbott1 @SrihariNaiduMD @mirvatalasnag @nadia_sutton @Radial_ICG @samirpancholy @MCoylewright
38%
Never used
6%
Use it often
29%
Good bail out option
26%
Don’t want to use it
68 votes • Final results
1
2
1
1,198
Jack Hall retweeted

Imagine your surgeon preparing for your operation.
They see you in pre-op, answer your questions, calm your fears, examine you, confirm the plan, and go get ready for the case. They review the imaging and think through the critical parts of the operation.
Then a nurse interrupts them:
“Doctor, your pre-op documentation isn’t good enough. You can’t just say you discussed the risks and benefits. You need a full H&P.”
The surgeon points out that the H&P was already done in clinic. The note is right there in the chart.
“No. That note is 31 days old. It has to be within 30 days. But it’s fine if you just copy and paste that old note.”
Think about how insane that is.
There is no new clinical information. There is no patient benefit. There is no improvement in safety or quality. The only thing being demanded is duplication. A pointless bureaucratic ritual to satisfy the machine.
So now you have a frustrated surgeon, a delayed case, a bloated chart, and one more example of modern medicine confusing clerical box-checking with patient care.
This is exactly what is wrong with the system. Endless note bloat. Pointless duplication. Administrative nonsense dressed up as professionalism. If there are no changes, there are no changes. Forcing a doctor to re-paste an unchanged H&P adds absolutely nothing for the patient.
And the most insulting part is the tone. That smug, condescending “of course you have to do it this way” attitude, as if this is self-evidently necessary instead of obviously stupid.
At this point, a lot of doctors would probably take a substantial pay cut to never touch a computer again. Cut the salary and use the savings to hire people to do the computer garbage. Epic. CDI queries. Coding queries. H&P updates. Order entry. Case booking. Inbox nonsense. All of it.
Never touch Epic again. Never answer another coding query. Never update another unchanged H&P. Never place another order that a clerk or protocolized team could enter. Never do another ounce of hospital data-entry cosplay.
Just let us be goddamn doctors instead of highly trained documentation technicians.
115
132
949
140,505
Jack Hall retweeted

I think this emerging era of coronary: DCB, hemodynamics, CTO practice, and imaging is revolutionary in uncovering so much WOW on vascular biology. Exciting, iterative, collaborative.
2
11
885
Jack Hall retweeted

The most advanced AI diagnostic tool is physical exam from a physician trained on tens of thousands of patients.
22
19
188
13,212
Jack Hall retweeted

Kaiser LA wants to pay board-certified cardiologists $218.65/hr to work overnights and weekends.
Don’t take this job. It’s hurts all of us.
428
86
1,609
2,349,153
Apr 2
Thank you for this @hjluks !
@HeartOTXHeartMD good stuff John
Apr 2

I hear this every week in my office:
"Doc, my heart rate hits 150 during squats — that's cardio, right?"
No. And if your cardiologist hasn't explained why, keep reading. 🧵
1
2
4
705
Mar 25
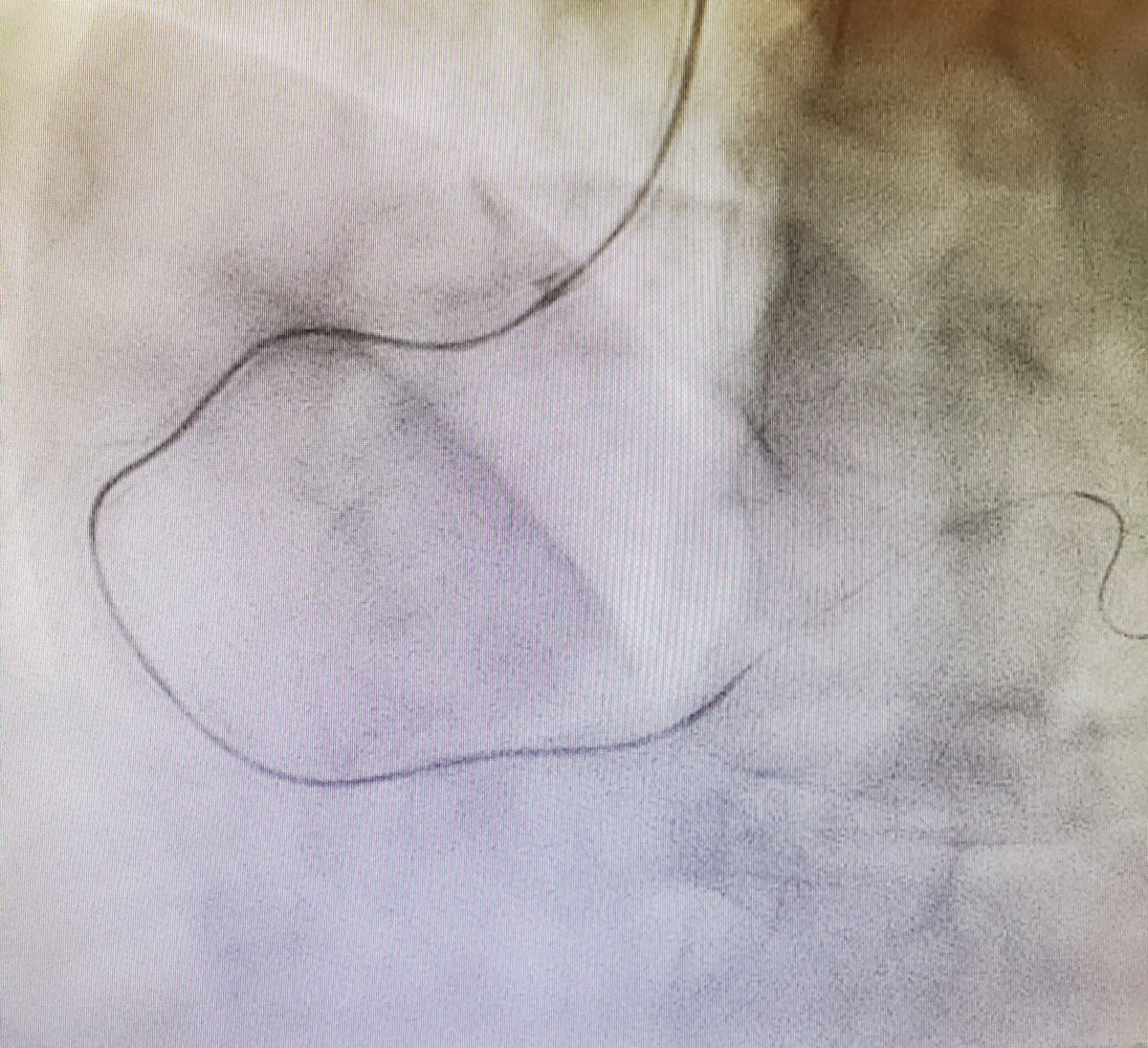
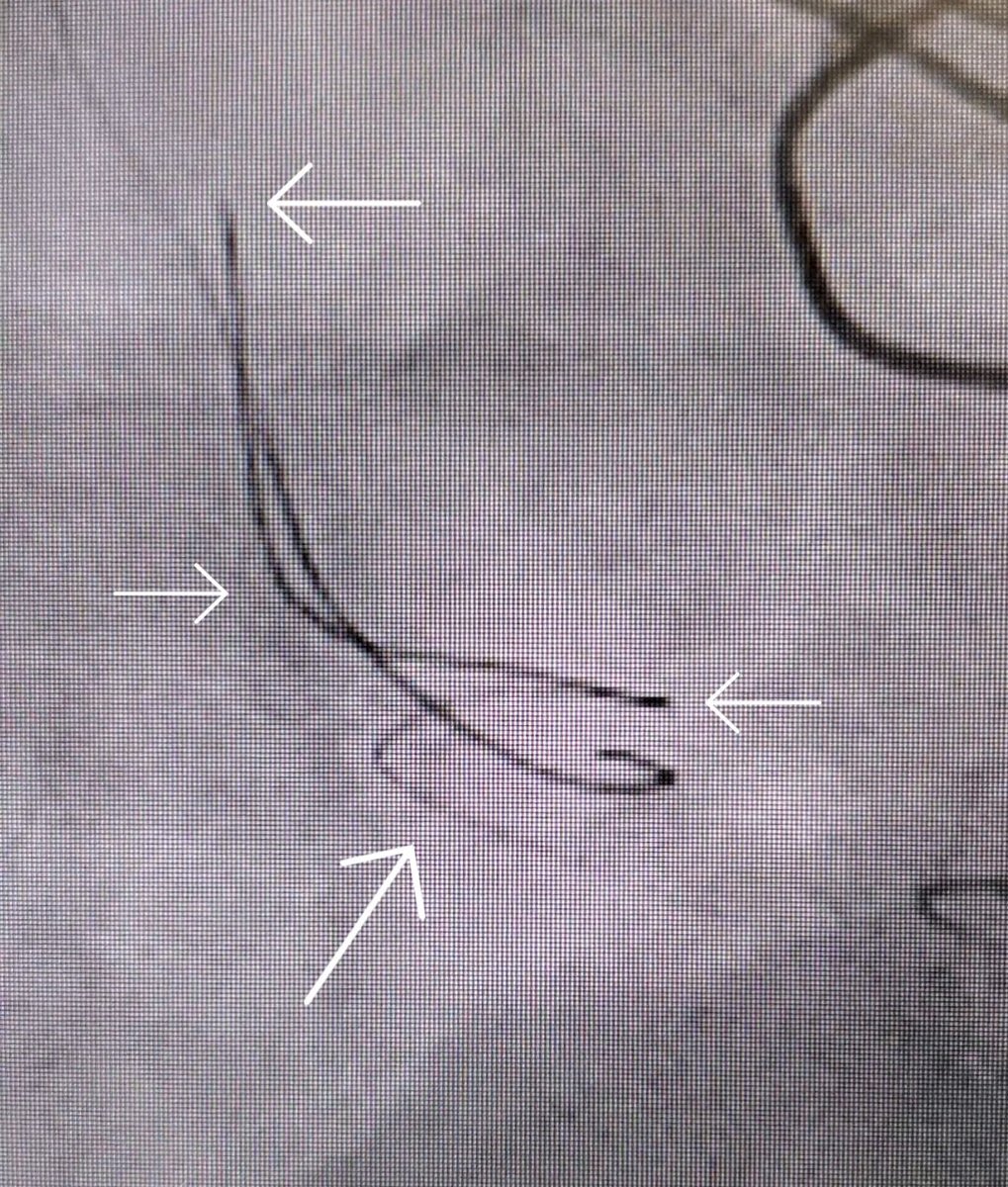
My cherry has been popped. Read about it, looked at imaging but never have found one in the wild.
23
27
211
75,387
Mar 28
A follow up. He is scheduled for Left Main reimplantation in 2 weeks. Preoperatively, a coronary CTA was ordered as the surgeon wants to know if the distance to the reimplantation site.
CCTA shows an anomalous circumflex, retro aortic!
1
240
Mar 28
It shouldn't be an issue. I can imagine as the patient aged if he developed pulmonary hypertension the flow could reverse. If he had a pulmonary embolus that could be disastrous as well.
203