
Structural Interventional Cardiologist | @ACCintouch | @scaielm | @SCAI | @OslerResidency | @MayoClinicCV | she/they 🏳️🌈
Joined March 2018
- Tweets 1,622
- Following 406
- Followers 2,076
- Likes 1,727
153 Photos and videos












Pinned Tweet

3 Dec 2025
Thrilled to serve as Co-Director of the next @scaielm cohort with @jaygirimd!
See you all next week in Miami at @SCAI Fellows, and then Montreal this Spring (structural tract will be sweet, led by @mszerlip) Not a member yet? Time to join! @SrihariNaiduMD @JDawnAbbott1
22 Nov 2025

It’s time. 15 years ago @SCAI launched @scaielm with @crfheart & @ACCinTouch to train future leaders in interventional cardiology.
It worked. @JDawnAbbott1 will be the first grad to become president!
R u next?
@sahilparikhmd @NavinKapur4 @DougDrachmanMD @SuzanneJBaron


5
24
13,152
The high level science @MyJSCAI continues to demonstrate best practices among cardiology journals. Don't miss this issue.

🆕📢JSCAI’s latest special issue “Strategies to Promote Health Equity in #IC” is now live. #HealthEquity isn’t optional — it’s essential.
Guest edited by @MCoylewright, @MayraGuerreroMD & @_WayneBatchelor, the issue highlights actionable strategies to advance #equity across #InterventionalCardiology
📚jscai.org/issue/S2772-9303(2…
2
6
546
#ACC26 This was an incredibly impactful session- while I love geeking out on all the technical details in my field #IC- I recognize that often the most challenging task- and requiring more preparation and skill- are the conversations we have with our patients as we guide them down complex #shareddecisionmaking paths. True experts deliver here on those needed skills. @jae_patton @KadijahPorterMD @SammyElmariahMD @VietHeartPA

What a great discussion on how to make patient centric introductions, what matters most to patients, and navigating delivery of unfavorable medical information
#ACC26 @SammyElmariahMD @jae_patton @KadijahPorterMD @MCoylewright

5
274
This is a critical time for #IC @SCAI and confident in the care and commitment Dr Dawn Abbott has always shared with her interventional community. @scaielm
You’re all in great hands. Dr Abbott truly merges education and academics and being 💯 in the trenches as a very busy operator.
Plus first @scaielm to take the helm @SCAI
We’re all behind you Dawn.
I’m here … call any of us past presidents if needed!

3
6
849
AI is an important part of our #structuralheart future, but cannot replace what we get back from close collaboration and friendship with colleagues. Great to work with you again @smuktas !
May 18

Enjoyed being a part of this important discussion in structural heart innovation. Thanks for your leadership @MCoylewright!
2
344
megan coylewright md mph retweeted

🥊 It’s debate ⏰ time. See top 🫀 cardiology minds go head-to-head on today’s toughest questions at #HeartofCardio 2026 in Miami Beach. 🔗 heartofcardio.com/
Join dream team: @ba_steinberg | @ChiadiNdumele | @MCoylewright | @AJBloodMD | @manesh_patelMD | @HeartDocSadiya | @garshick
2
3
898
megan coylewright md mph retweeted

Jan 20
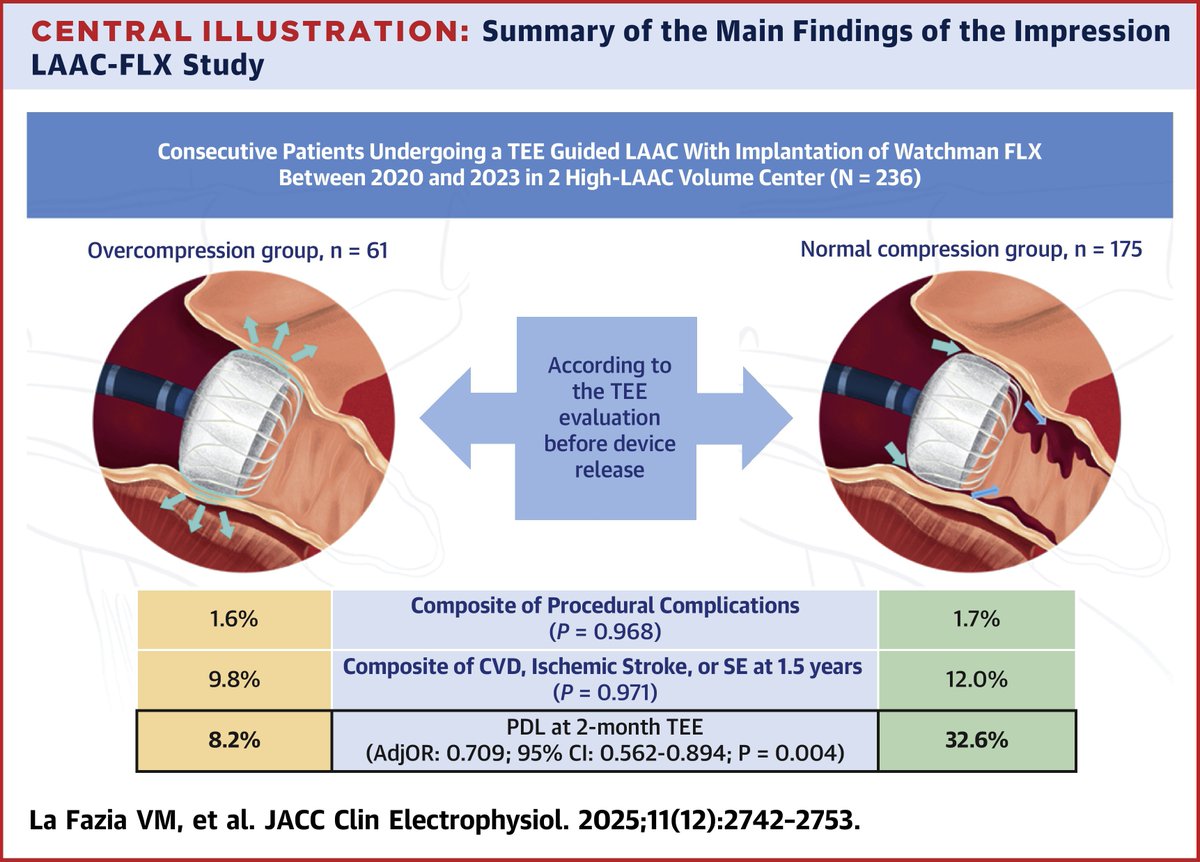
In this dual-center cohort of TEE-guided LAAC, the overcompression group was independently associated to a higher rate of LAA occlusion at TEE follow-up.
Get the details in #JACCCEP: jacc.org/doi/10.1016/j.jacep…
1
13
44
4,620
megan coylewright md mph retweeted

Jan 18
🚀 The Pulse is live — and women in cardiology are showing up.
Hundreds are already using @WomenAs1’s new platform to connect, find opportunities, and stay at the forefront of science. 💫
No surprise that Career Opportunities is leading the way 👀
How are you using The Pulse? 👇
🔗 womenasonepulse.org
#ThePulse #WomenInCardiology #WomenInMedicine #Leadership 💜
Jan 18

Hundreds of women in cardiology are signed up to The Pulse, strengthening connection, collaboration, and opportunity for women physicians across the globe.
Which feature of The Pulse do you think will help you most as a healthcare professional?
🔗 womenasonepulse.org
2
3
1,003
When all cardiologists are equitably and visibly valued for what they bring to the table, it can impact an entire field. Without it, we fail to attract top talent.
Jan 20

Study finds workplace cultures with aggressive competition & male norms signal that women are less valued, even w/o overt discrimination. Women cope by distancing themselves from other women in order to fit in or be taken seriously.
psypost.org/women-tend-to-do…
1
2
653
megan coylewright md mph retweeted

Dangers of a Sedentary Lifestyle on the Heart youtu.be/kF_GwL9G-Qo?si=WbQ2… via @YouTube
It has been a decade and the information is still solid. 👊🏾
cardiosmart.org/assets/infog…
#CardioSmart @ACCinTouch @Intermountain @AAPAorg @APAC_Cardiology @UtahAPA

2
3
305
megan coylewright md mph retweeted

16 Nov 2025
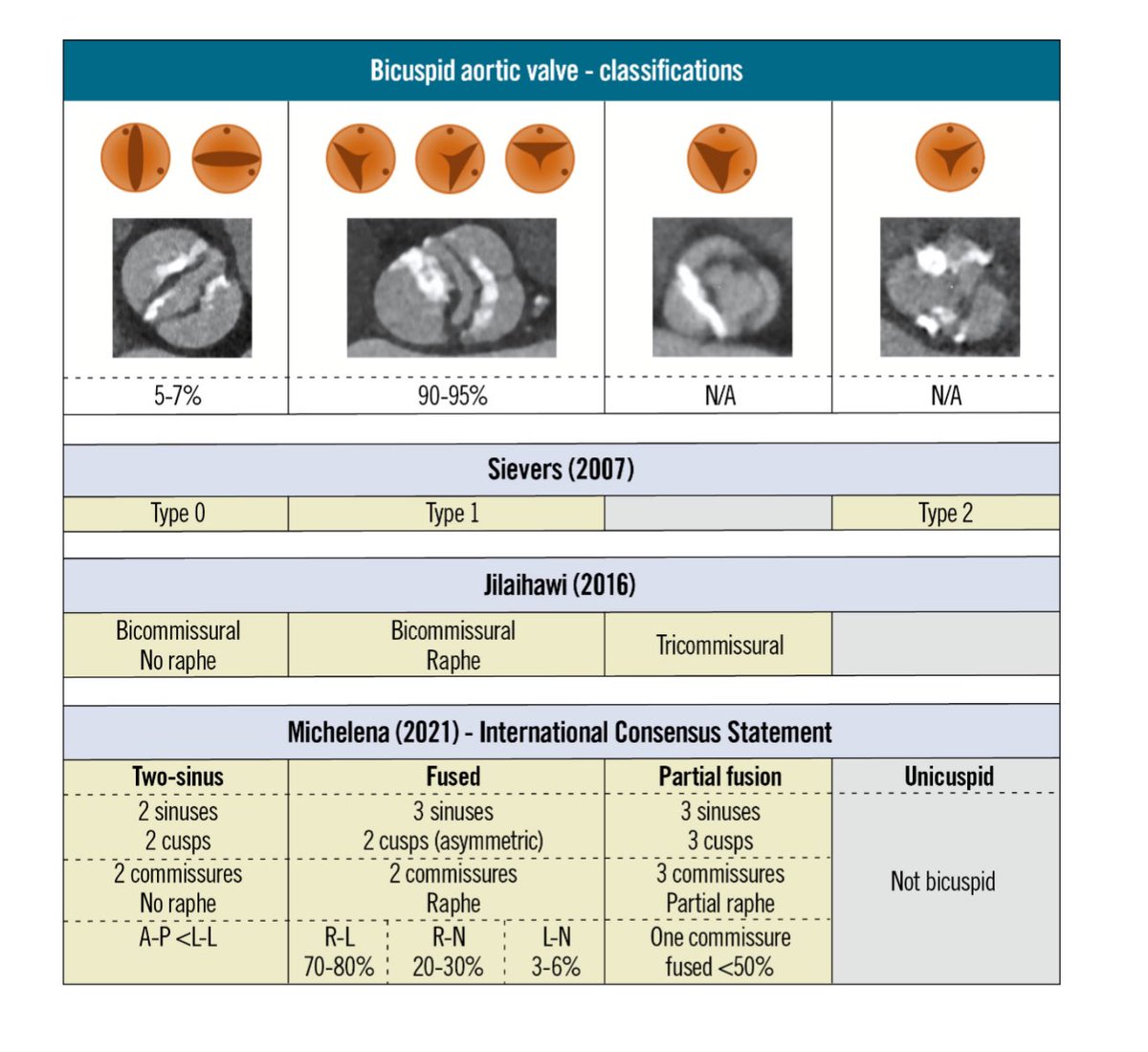
Cardiac Imaging Pearls in Bicuspid AS
From EuroIntervention:
eurointervention.pcronline.c…
1️⃣ CT is King for BAV TAVR
•Essential for defining raphe, leaflet morphology, calcium burden, annular shape, and ascending aorta size.
•Identify heavy/rigid raphe → predicts expansion issues PVL risk.
2️⃣ Measure More Than the Annulus
•BAV = elliptical, asymmetric.
•Consider supra-annular sizing or “virtual raphe ring” when annulus doesn’t tell the whole story.
3️⃣ Calcium Mapping Matter
•High calcium → higher risk of malexpansion, rupture, stroke.
4️⃣ Delineate the Aorta
•BAV often comes with root & ascending aorta dilation.
•CT aortography crucial for deciding TAVR vs SAVR when aortopathy present.
5️⃣ Coronary Heights in BAV Are Tricky
•Asymmetric cusp fusion can distort coronary takeoff. High/ eccentric take off
•Carefully assess coronary height sinus size.
6️⃣ Echo Complements CT
•TTE: Hemodynamics, gradient confirmation, LV function, AR degree.
•TEE: Intra-procedural alignment & PVL detection especially in challenging anatomy.
7️⃣ Post-TAVR Imaging is Not Optional
•BAV valves may expand asymmetrically → follow-up echo ± CT for durability and PVL assessment.
#Echofirst #YesCCT #CVimaging
5
49
174
14,624
Intracardiac echo for LAAO is effective vs TEE. Let's make room in the lab for other therapies that require GA! Reminders for mod sedation: LA pressure >12, no snoring or deep breaths, & attention when catheters open to air. Our work here:
jacc.org/doi/10.1016/j.jcin.…
1
5
333
Small, intimate meetings have a wonderful vibe of collegiality, laughter, a little gentle teasing, and some of the most impactful education as we get vulnerable to share what we learn in this challenging work. Thank you to all who joined, and espectially @OPCILive @CathElectroSurg Brian Whisenant for hosting!

Tomorrow in Salt Lake City: Day 1 of the 2nd annual OPCI Structural Complications Summit! 👏opci.events/event/structural…
We look forward to welcoming our esteemed faculty along with interventionalists and fellows from across the U.S. to build best practices on how to avoid and manage complications as well as explore opportunities for innovation. ❤️🔥📈
@jubinjoseph @PaulMahoneyMD @WallyOmarMD
@IsidaByku @GiorgioMedranda @CraigBasman
@WallyOmarMD @JasonFoerst @CathElectroSurg

1
2
13
1,642

📢There is one week left to submit late-breaking science for #SCAI2026! Showcase your recent discoveries at one of #InterventionalCardiology's largest events to help improve the field and patient outcomes.
Submit late-breaking science by January 21➡️ scai.confex.com/scai/2026/cf…
#CardioX #Research
5
11
953
Amy Poehler just won a Golden Globe for podcasting (so good). youtube.com/watch?v=Bz1O2EL2… Mix up your podcast diet with content on interventional cardiology! #JSCAIBEATS Join my conversation on device positioning in TAVR procedures with @ParasuramMD
Spotify: bit.ly/3Zc3Mu8
Apple: bit.ly/4sFK0F0
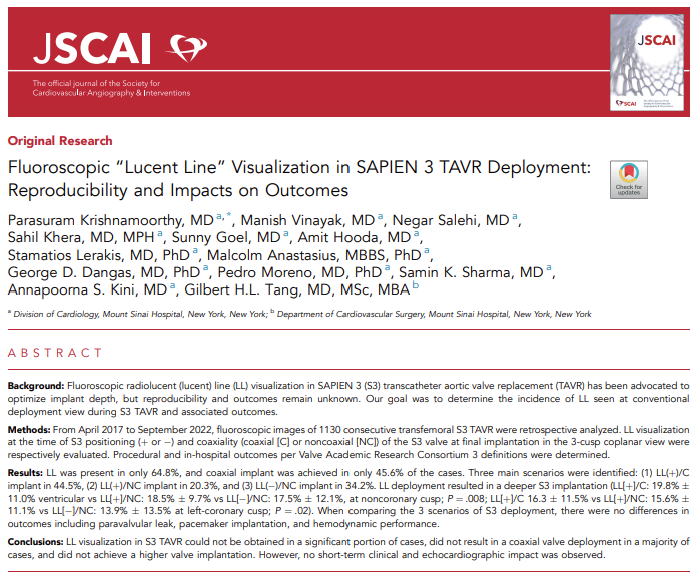
🎧🗣️ #JSCAIBEATS | Lucent Line & #TAVR
@MCoylewright & @ParasuramMD break down real-world data published in #JSCAI on lucent line visualization during SAPIEN 3 TAVR & what the findings mean for implant technique — without compromising patient outcomes.
Spotify: bit.ly/3Zc3Mu8
Apple: bit.ly/4sFK0F0
2
10
1,858
28 Dec 2025
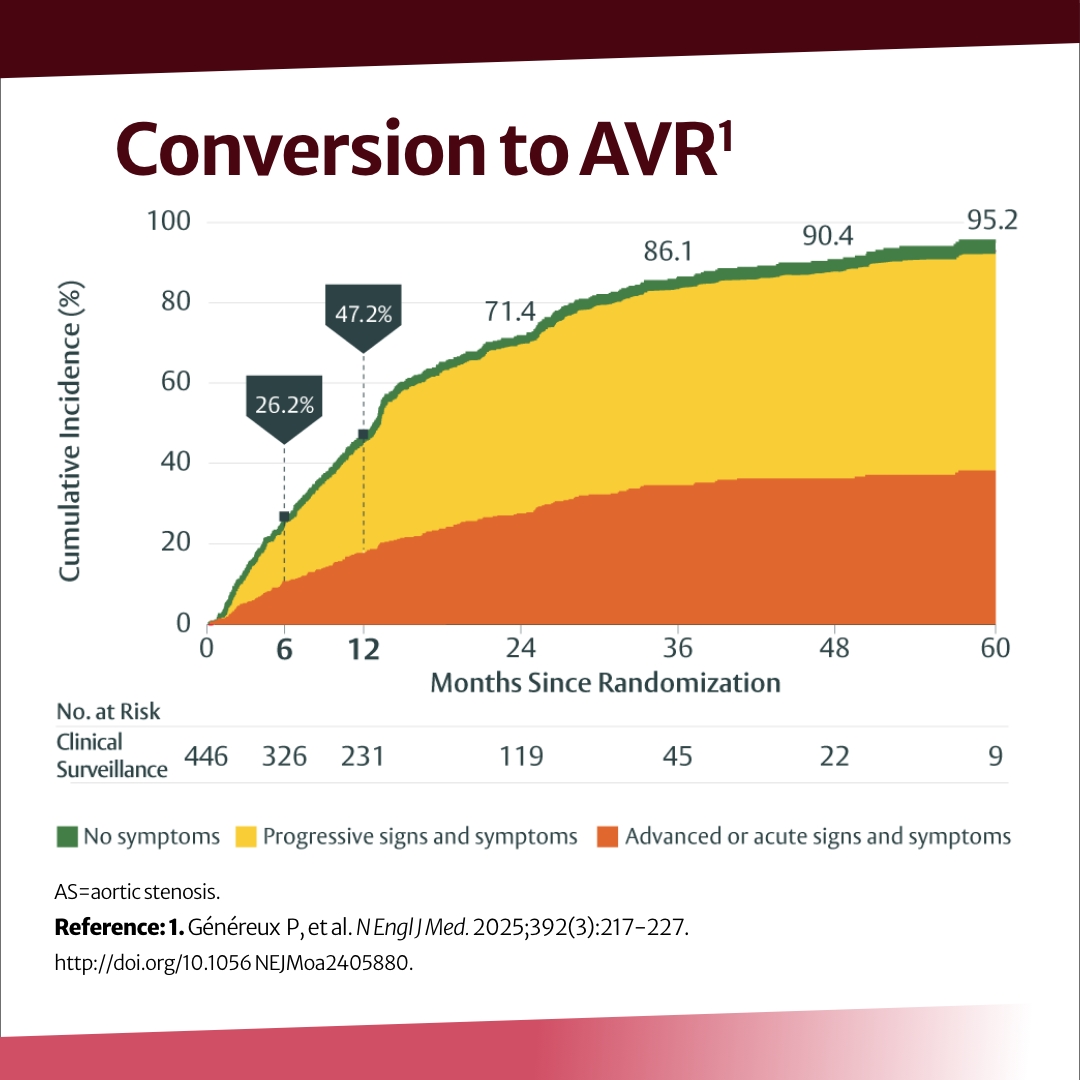
"Trials that prioritise patient-centred endpoints—functional recovery, independence, symptom relief—are essential for restoring relevance." Time to restore the art of medicine- made more potent when power differentials are named and navigated. #shareddecisionmaking
28 Dec 2025

"futility becomes proceduralised"
@Open_HeartBMJ
openheart.bmj.com/content/12…
If u read anything during the holidays, make it this article..have technological advancements skewed our judgement? I'd venture n say our patients too...much harder to discuss futility today than a decade ago
@perc_surgeon
@HeartOTXHeartMD
@tristonsmithmd
@FaisalLatifMD @ChamsiPash @MCoylewright @aalahmadmd
@adnanalkhouli @NadeenFaza
2
7
1,493
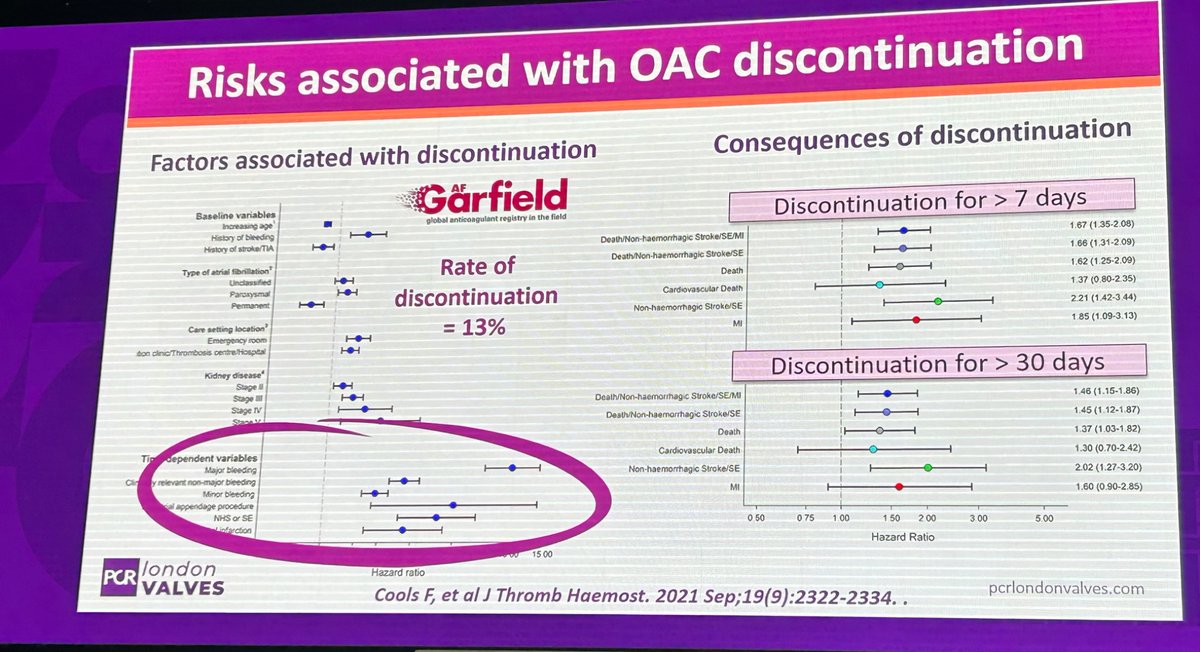
28 Dec 2025
We have the data to inform shared decision making for stroke prevention in afib- and the evidence further suggests use of a decision aid in the conversation improves quality of decision making.
Drugs vs. Device: heartrhythmjournal.com/artic…
256
27 Dec 2025
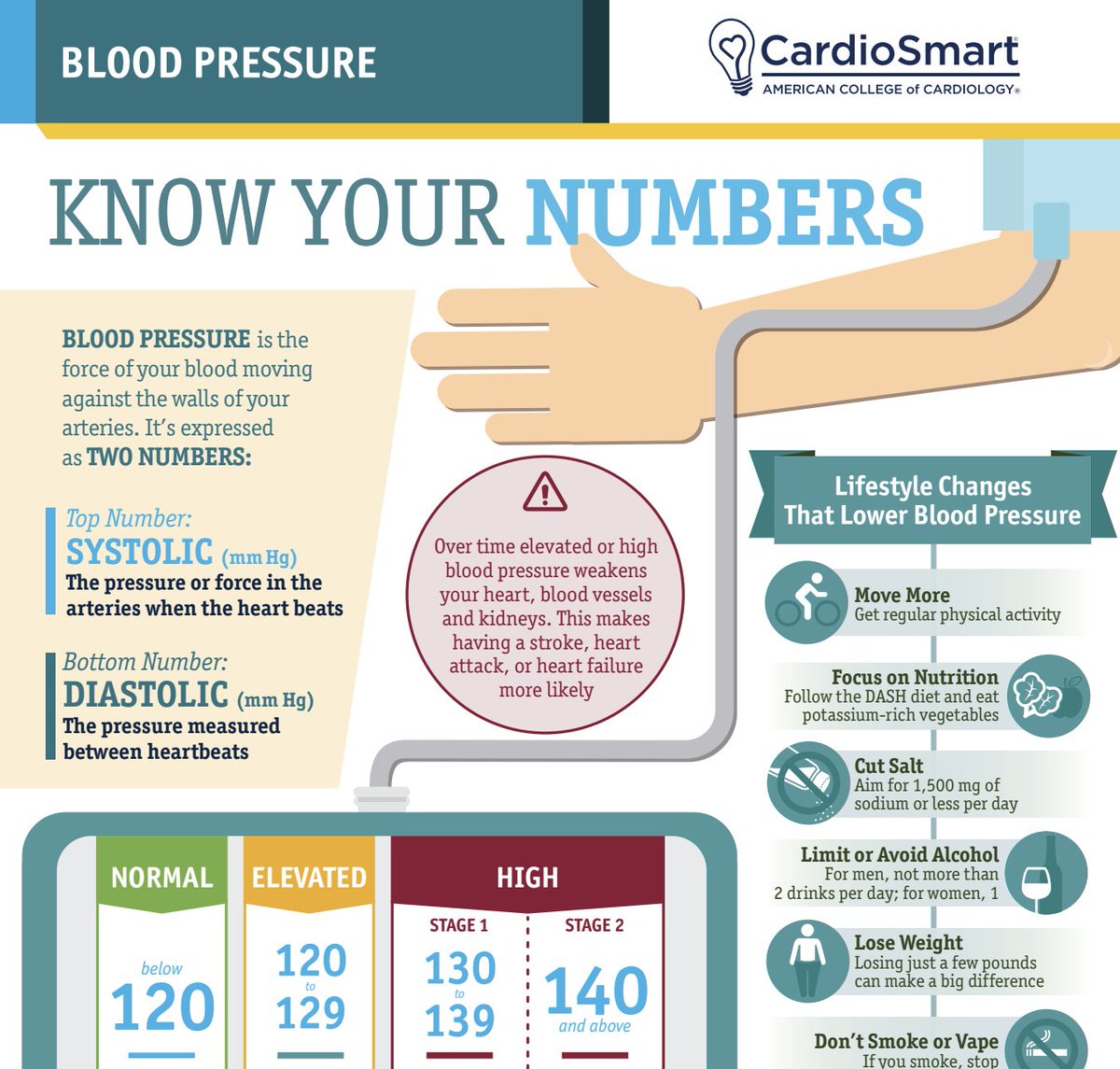
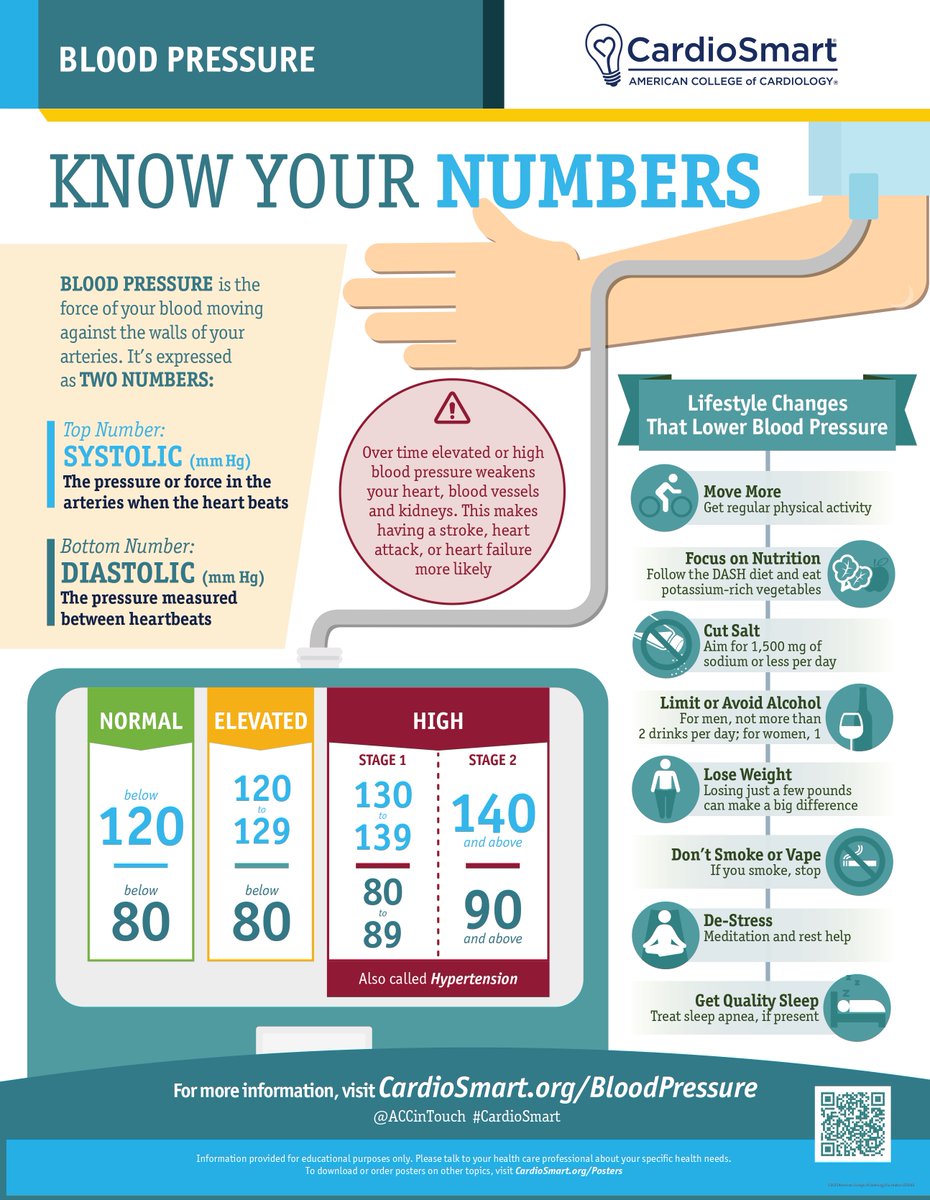
Blood pressure control reduces stroke, heart attack, congestive heart failure... with simple first steps. Hand this out to all patients walking into your clinic! They will be surprised at what the evidence shows...120/80 or below leads to better health. @ACCinTouch
26 Dec 2025

#CardioSmart’s updated infographic explains BP readings in clear, simple language & includes lifestyle changes that can help ↘️ BP. Use it at the point of care to support conversations about heart health with patients. ➡️ bit.ly/4mJQUVJ#cvPrev
3
590
megan coylewright md mph retweeted

25 Dec 2025
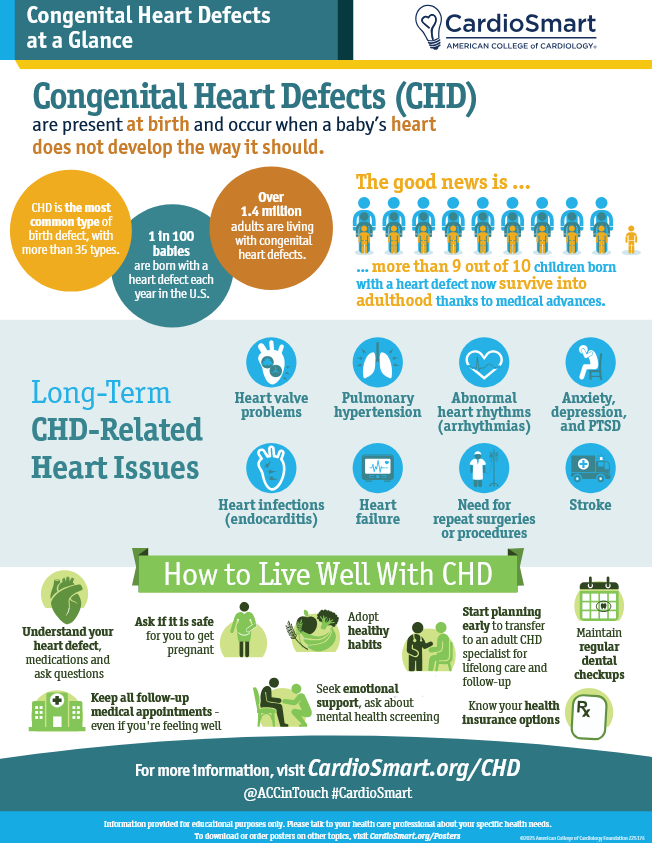
Guide your patients in understanding congenital heart defects, long-term impacts, and healthy living with #CHD using this 🆕 #CardioSmart infographic. 👇
Explore the #CHD CardioSmart hub for more ➡️ bit.ly/4j8V1Kw
#CardioX #ACHD
3
10
35
4,989
27 Dec 2025
RT @MCoylewright: The NCD is now re-opened for TAVR.
"We are particularly interested in comments that include scientific evidence, specifi…
7