
9 Photos and videos




Carlos E. Diaz-Castrillon, MD MSc retweeted

Imagínese uno seguir diciendo que José Manuel Restrepo es un académico o un tipo serio con todas las boberías y absurdos que anda vendiendo por ahí.
1,832
3,657
12,667
291,190
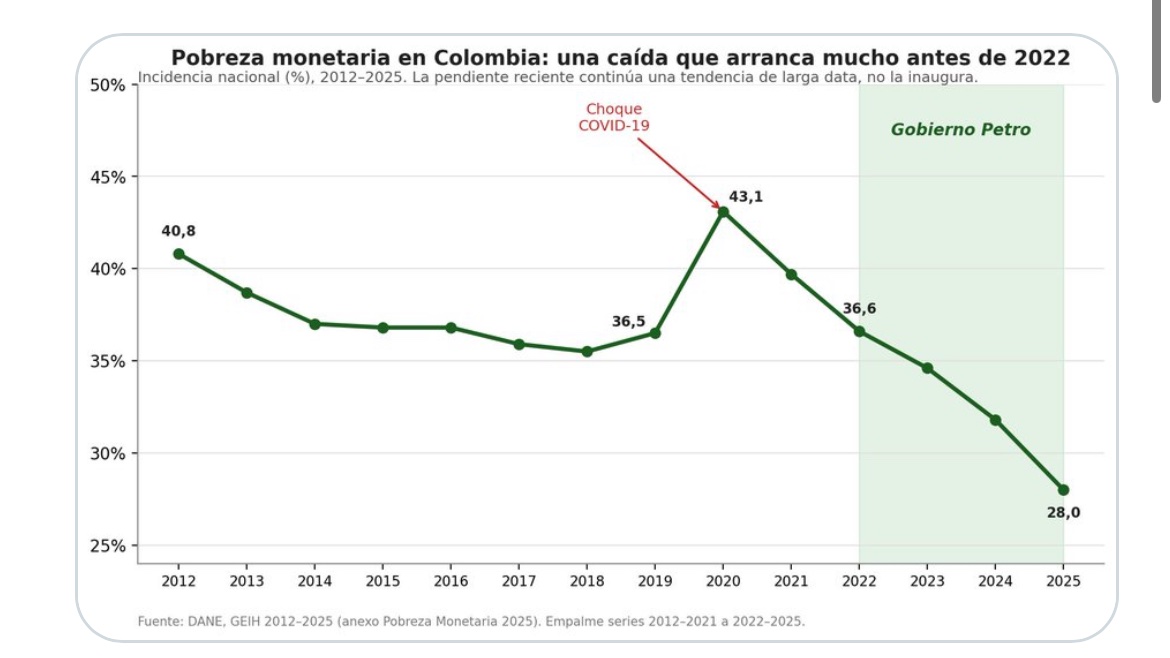
Colombia Under Petro: Social Gains Amid Monetary and Fiscal Constraints cepr.net/publications/colomb…
1
78
Macrosystem Factors and Perioperative Outcomes in Adult Congenital Heart Surgery: An Analysis of the STS Databases evermed.short.gy/3bOB61 via @STS_OnDemand @STS_CTsurgery @UPMC_CTSurgery #ACHD
1
101
#HEART #medspace #someforsurgery @AATSHQ @ISACHD 163.… | The American Association for Thoracic Surgery | AATS aats.org/resources/age-relat…
1
149
Carlos E. Diaz-Castrillon, MD MSc retweeted

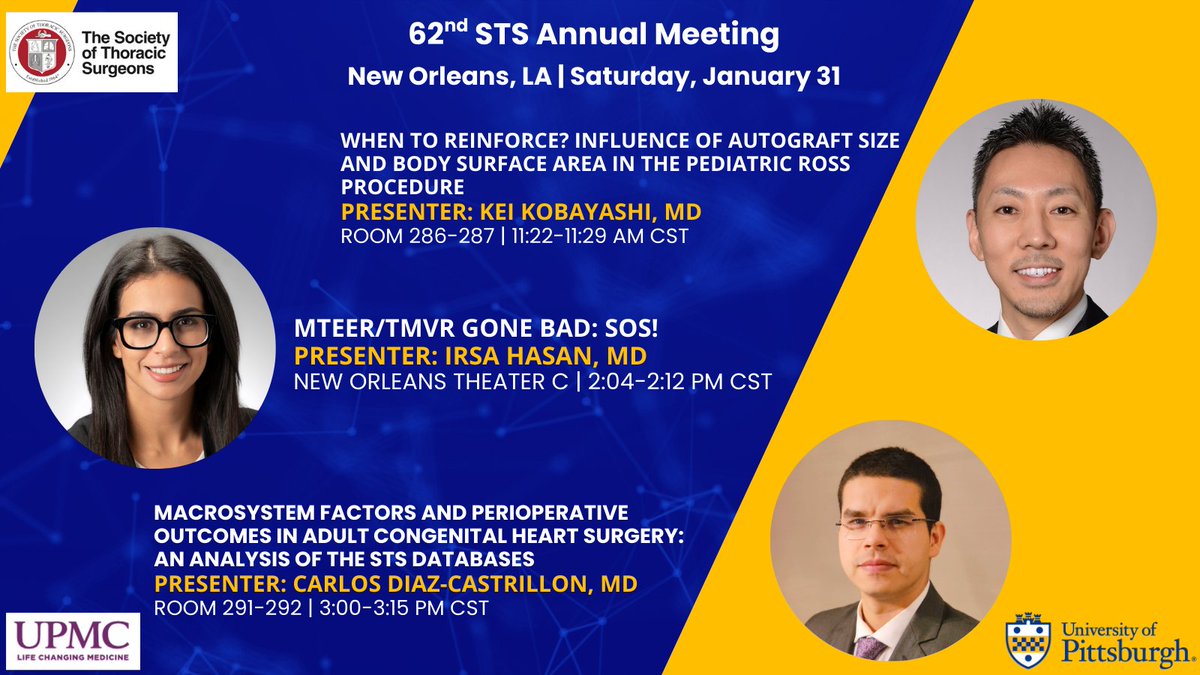
Drs. Kei Kobayashi, Irsa Hasan and Carlos Diaz-Castrillon represent UPMC CT Surgery at the 62nd STS Annual Meeting on Sat 1/31/26
New Orleans Ernest N. Morial Convention Center
@Irsa_Hasan @cediazc @STS_CTsurgery @UPMCPhysicianEd @HviUpmc #STS2026
4
17
1,017

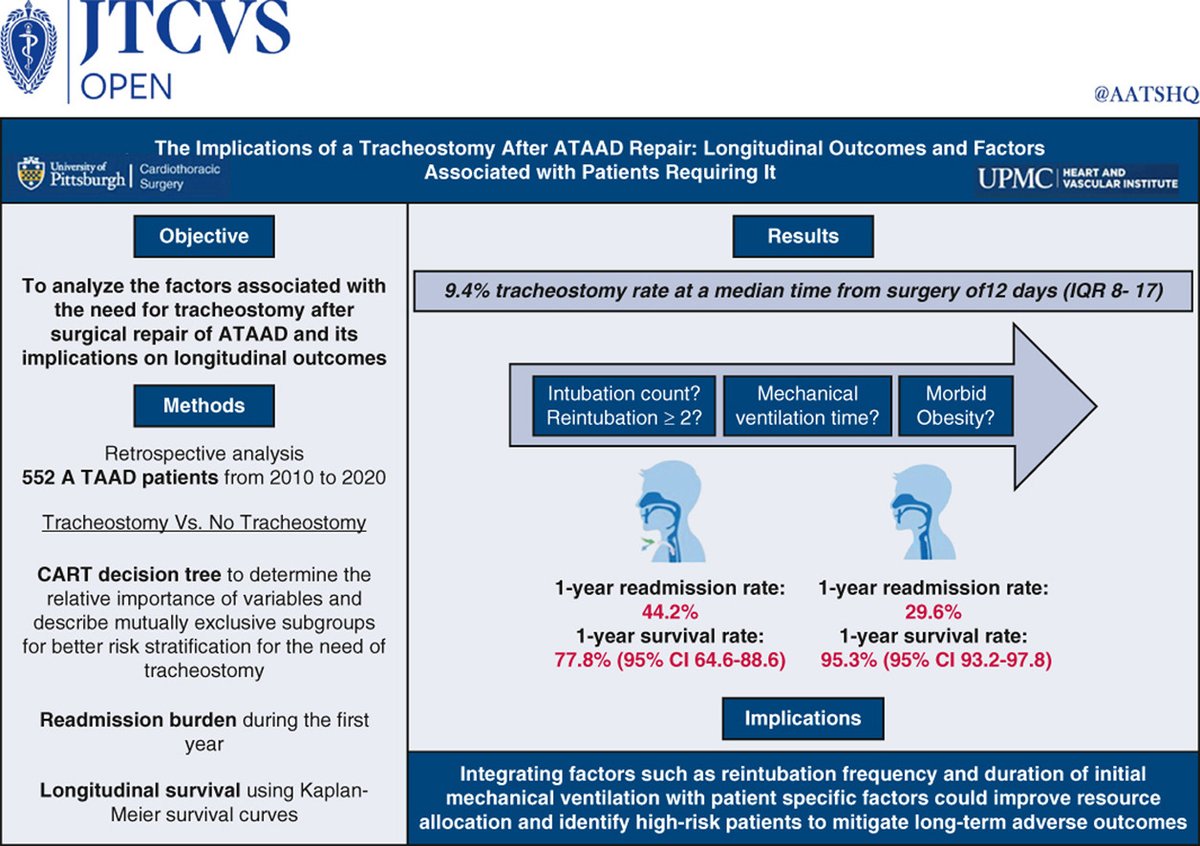
What are the implications of tracheostomy after acute type A aortic dissection repair? Learn about the longitudinal outcomes and factors associated with patients requiring it by reading this #JTCVS Open study published by researchers at @UPMC_CTSurgery: doi.org/10.1016/j.xjon.2025.…
6
18
2,672
Carlos E. Diaz-Castrillon, MD MSc retweeted

1 Jul 2025
Nearly 3 in 4 academic surgeons believe corporatization is harming the mission of surgery. Education and research are sidelined, and burnout is rising. The tripartite model is at risk.
journals.lww.com/annalsofsur…
2
8
23
4,172
Carlos E. Diaz-Castrillon, MD MSc retweeted
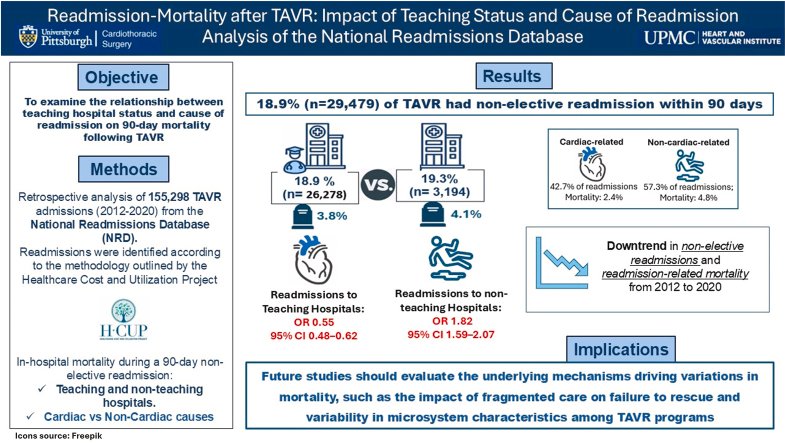
National Readmissions Database study finds differential association between teaching hospital status and 90-day readmission mortality in patients who underwent #TAVR
🔗: pubmed.ncbi.nlm.nih.gov/4043…
@CJCJournals @cediazc @DSGMD @Irsa_Hasan @IbrahimSultanMD @HviUpmc @PittCardiology
4
6
897
The May Issue of #JTCVS is now available. Read the newest #cardiothoracic surgery research to stay up to date. Topics include severe obstructive hypertrophic cardiomyopathy and gender, race, and ethnicity in lung cancer clinical trial participation: jtcvs.org/current

5
30
3,070

4 May 2025
Join us at #AATS2025 congenital poster session!
Based on a national survey of pediatric cardiac surgery chiefs, we explore RV to PA conduit selection—its variability and key drivers.
@AATSHQ @UPMC_CTSurgery @ChildrensPgh @UPMCPhysicianEd
1
6
466
1 May 2025
Honored to see our study featured as an Editor’s Choice in the May issue of #JTCVS
Read it free until 5/30
#AorticDissection @UPMC_CTSurgery @IbrahimSultanMD @DSGMD @M_Pompeu_Sa_MD @geoarnaoutakis #WilsonSzeto @STS_CTsurgery

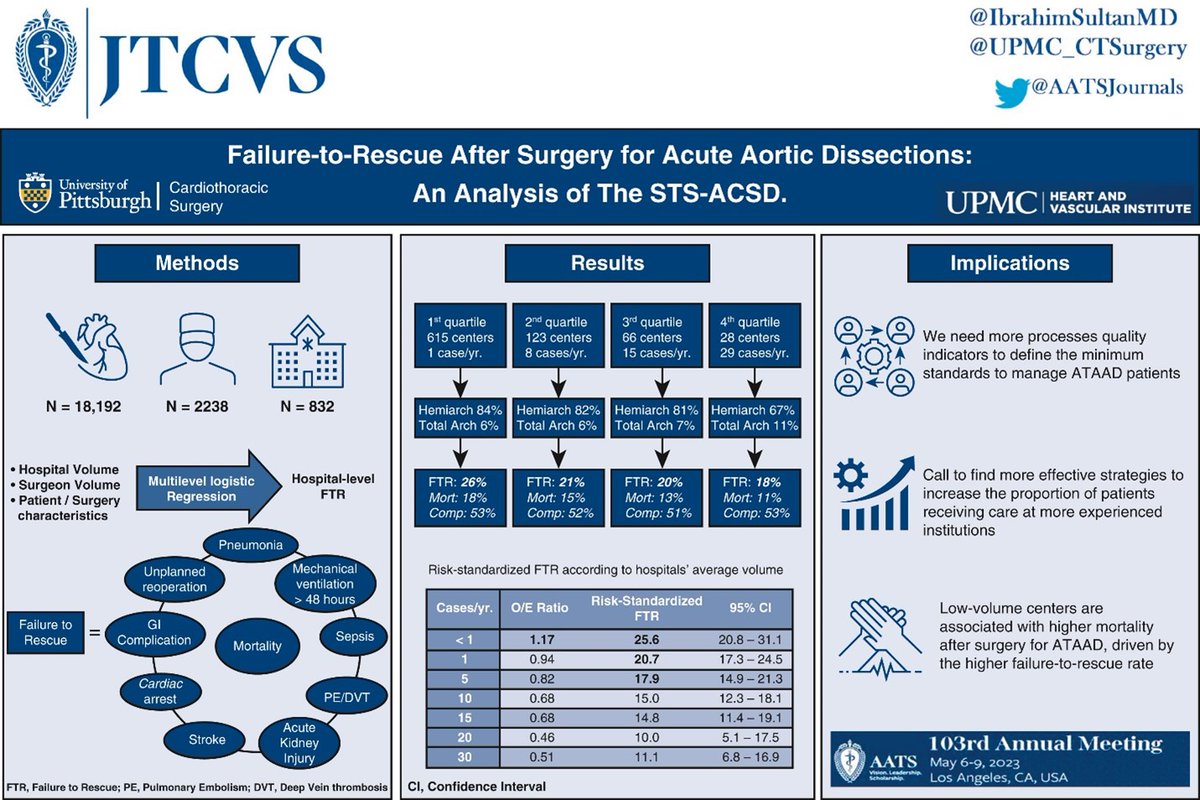
Free until 5/30: The burden of major complications on failure to rescue after surgery for acute type A #aortic dissection. Researchers analyzed more than 19,000 patients to reach their conclusion. Read this Editor's Choice article now in #JTCVS: doi.org/10.1016/j.jtcvs.2024…

1
3
15
1,682
1 May 2025
#AATS2025
Join us at the "Congenital Scientific Session: Adult Congenital Heart Disease"! We'll be discussing how age impacts outcomes and resource utilization in #ACHD undergoing valve replacement in the U.S.
@UPMC_CTSurgery @AATSHQ
2
16
1,334
Carlos E. Diaz-Castrillon, MD MSc retweeted

30 Apr 2025
See you in Seattle @AATSHQ #AATS2025 where many firsts in the field are going to be presented. To list a few:
- 1st transcervical robotic AVR
-1st RCT of sternotomy vs MICS CABG
- Global real-world analysis of long-term outcomes of Ross vs bioprostheses
-ZEPIS-SAVR trial
👌🏻
"We are celebrating the 105th meeting!" - @FaisalBakaeen
Ready to join in on the celebration? TODAY is your last day to take advantage of lowered registration rates for #AATS2025. Join us in Seattle this May. Register: events.aats.org/am25/registr…
21
55
8,654
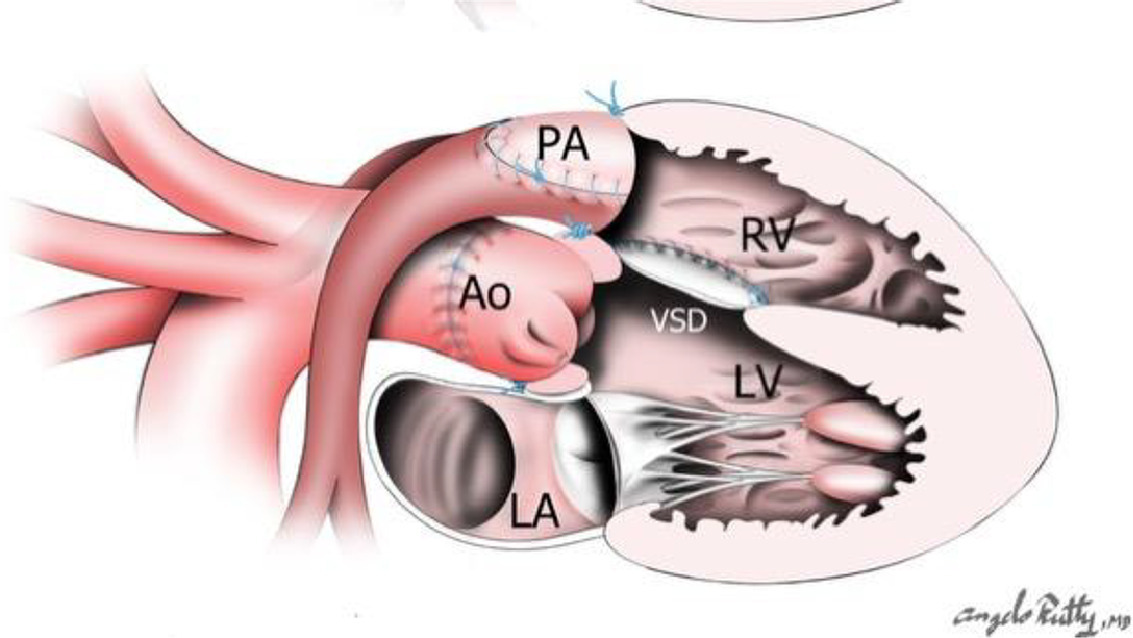
Invited Expert Opinion: Single and double root translocation for transposition and malposition of the great arteries or double outlet right ventricle with VSD and LV outflow tract obstruction. Read now in Seminars: doi.org/10.1053/j.pcsu.2025.…
@juan_lehoux @UPMC_CTSurgery
5
19
3,078
16 Apr 2025
Collaboration with @stanfordpedcard -@UNALOficial
Importance of age at diagnosis of PH in children living at high altitude: Longitudinal follow‐up of 86 patients in Bogota @PulmCirc onlinelibrary.wiley.com/doi/…… Gabriel F. Diaz-Rachel Hopper- @Viniciodjperez @PVRI #CardioTwitter
15 Apr 2025

New publication: Importance of age at diagnosis of pulmonary hypertension in children living at high altitude: Longitudinal follow-up of 86 patients by Gabriel F. Diaz Et al. Read the full research article onlinelibrary.wiley.com/doi/…
1
3
357
Carlos E. Diaz-Castrillon, MD MSc retweeted
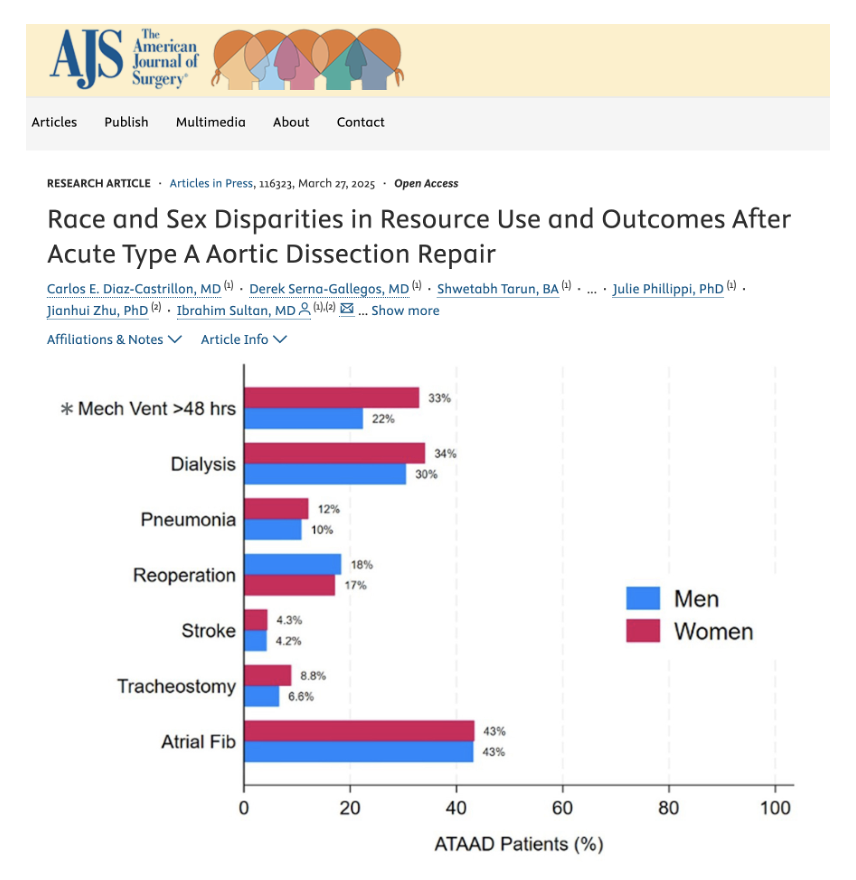
Retrospective cohort study: race and sex disparities in periop resource use, postop outcomes and long-term survival after acute type A #AorticDissection repair
🔗: pubmed.ncbi.nlm.nih.gov/4020…
@AmJSurgery @cediazc @DSGMD @sarahyousefmd @JuliePhillippi @IbrahimSultanMD @HviUpmc #ATAAD
7
12
1,413
19 Jan 2025
Optimization of current resources is needed to improve access to #mentorship in #CTSurgery @CynthiaRangel02 Kristian Punu @JohnTreffalls @LenaETrager @NaimaAlver @ThoracicStudent

A #mentorship access gap remains in #CTSurgery for medical students; survey results call for optimization of current programs
🔗: pubmed.ncbi.nlm.nih.gov/3978…
@cediazc @IbrahimSultanMD @AATSHQ @ThoracicStudent #JTCVS #JTCVSOpen #Education #TSMA

1
2
5
1,266
Researchers at @UPMC_CTSurgery analyzed the @STS_CTsurgery adult #cardiac surgery database to review outcomes of surgery after ATAAD between 2017 & 2021. They found high-volume centers had lower operative mortality than low-volume centers. Read in #JTCVS: doi.org/10.1016/j.jtcvs.2023…
9
18
5,223
Carlos E. Diaz-Castrillon, MD MSc retweeted

15 Nov 2024
Publicy Funded Research and Clinical Relevance
Thinking about today’s tweets-the overlap between 2 concepts I tweeted about became apparent.
There is precious little evidence to support much of what we do clinically. The NIH funds few studies that directly inform clinical practice.
They do invest heavily in basic science. I do not know the number, but I suspect 100’s of millions of dollars was spent on GLP-1 research. Yet, when the results of that work were translated into a useful drug such as the GLP-1 agonist tirezapide, it is sold by private industry at a huge cost such that most patients – ie, those who paid for the research via their taxes – cannot afford the medication.
How is this fair?
Furthermore, all the excitement about the most recent tirzepatide article in NEJM results from a drug company pouring large amounts of money into a clinical trial. Despite the hype in the press, the trial’s results were not that impressive-the observation that the development of diabetes in obese patients can be prevented by weight loss is not new. Any, even small amount of diet-induced weight loss, will have the same effect. This has been known for decades.
There are many treatments that would have the same effect on diabetes that do not have the same level of evidence to support their use because the NIH puts very little money into clinical trials that would show this sort of thing.
So—There is precious little public funding interventions that will not yield private sector profit – Public funding mostly does into basic research that eventually hugely benefits private industry.
The loser in all this is tax-paying patients. They invest in medical research through their taxes but to yield the benefits of that investment they have to pay a second time via the exorbitant prices for the new drugs developed from the knowledge gained from publicly funded basic medical research.
Solutions to this mess are
1) The NIH should fund research that will have direct clinical relevance for the medical care of patients in the US. Any funded project should have a rationale justifying how the research’s findings will directly (and not indirectly) affect clinical practice.
2) Drugs developed based on publicly funded research should be affordably priced, recognizing the public’s investment in the research that led to the development of the drugs. This is aligned with drug company’s arguments that they need to charge high prices for new drugs to recoup the costs of bringing the drugs to market. Tax paying consumers who paid for the research underlying the drug’s development deserve the same return on investment.
2
16
1,662
Carlos E. Diaz-Castrillon, MD MSc retweeted
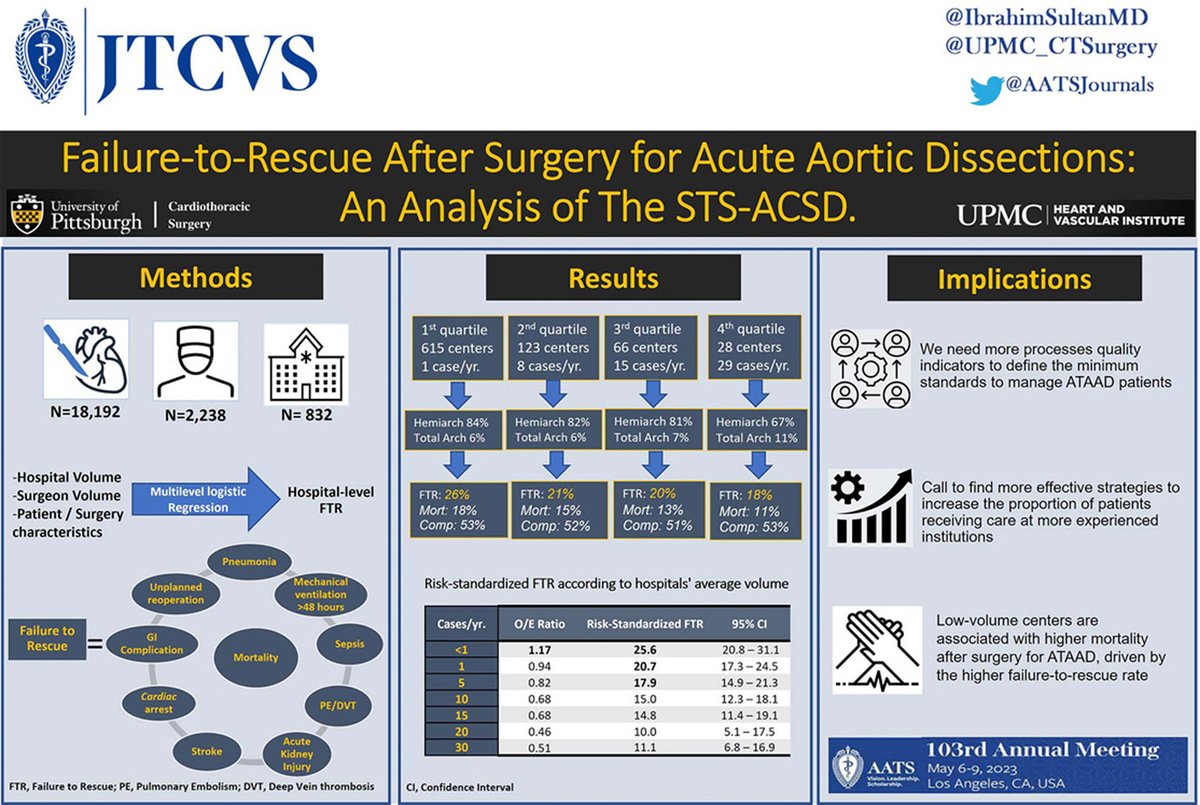
Outcomes analysis of the STS adult cardiac surgery database shows low-volume centers treating Acute Type A Aortic Dissection patients are associated with higher failure-to-rescue rates
🔗 jtcvs.org/article/S0022-5223…
@HviUpmc @IbrahimSultanMD @AATSJournals #ATAAD #AorticDissection
1
12
27
3,678