Biostatistician, SAS-lover, R-learner, outcomes researcher, she/her. associate prof @harvardmed, biostatistician @BWHResearch @OrACORe_BWH
Joined February 2016
- Tweets 914
- Following 329
- Followers 526
- Likes 5,503
137 Photos and videos



Jamie Collins retweeted

7 Feb 2025
🔬 NIH’s new policy to cap indirect costs at 15% is a huge blow to research🧪
💰 Less funding for operations = fewer resources for science.
⚠️ Small institutions may struggle to sustain research.
🏛️ This could impact the future of NIH-funded projects.
🔗 grants.nih.gov/grants/guide/…
1
7
12
4,081
Jamie Collins retweeted

8 Feb 2025
🧵 Many “hot takes” about the reduction of @NIH indirect grant costs to 15%.
Let’s lay out the facts about the university grant management process & accounting. And then use this to project likely short and longer term impacts of the policy.

58
288
1,042
431,169
Jamie Collins retweeted

8 Feb 2025
Universities aren’t “siphoning” research funds—overhead (indirect costs) covers essential expenses like lab space, utilities, admin support, & compliance with federal regulations. Without it, research wouldn’t happen.
Federal agencies negotiate these rates, and they’re standard across institutions. Not a ripoff—just the cost of science. This move will weaken our biomedical prowess and many educational programs that create scientists you employ. #ResearchFunding #SciencePolicy #nih #science #stem #research #indirect
7
3
104
9,002
Jamie Collins retweeted

8 Feb 2025
It seems few people know what an “indirect cost” is or why it has to be 40-60%.
The reason the government forced universities to raise their indirect costs up to (typically) 40-60% was to force a huge amount of regulations on the universities while also minimizing the bookkeeping to comply with those regulations. This includes the work by contract managers, compliance lawyers, accountants, safety management, etc., who are required by the government per the terms of the contract. If universities had to allocate all those categories of labor to each contract hour-by-hour it would require too much bookkeeping, which would waste money. (I’m setting aside for now the question of whether or how much the regulations are wasting money and only discussing how you bookkeep the effort to comply with the regulations.)
So to save money, while also requiring universities to do these types of work, the government requires universities to roll those categories of labor into “cost pools” that must be allocated as a percent of the technical work in each of the contracts. While the actual “overhead” might be only 15%, these pooled labor charges that are required by the government are typically much more.
Second, the government doesn’t allow the universities to figure out their own indirect rates. These rates are determined by the federal government through audits every couple of years. The government then sends a document telling the university what rate to use for its cost pools. For example, the University of Colorado was told by the DHHS to use 54% (colorado.edu/controller/site…) and U. Nebraska was told by DHHS to use 55.5% (uofnelincoln.sharepoint.com/…). 40-60% is not only reasonable to fulfill the terms of the contract, it is the rate that the government tells the university it can charge for all the work the government requires the university to do.
So if the government wants to reduce the indirect rate to 15%, then it needs to do one of these two things:
Either
(A) eliminate all the federal regulations that force the universities to do those categories of work (compliance, accounting, management, safety management, tracking harmful chemicals, etc.)
Or,
(B) stop requiring universities to pool those real costs into the “indirect cost” category and allow universities to include them in the “direct costs” of the contract.
If the government chooses (A), then the safety rails have been entirely removed. (Even if the government lowers the regulations without entirely eliminating them, the costs they impose will still be real costs that probably come out to more than 15%.)
Or, if it chooses (B), then the direct costs will go way up and research will actually be less efficient because all the bookkeeping, not more efficient.
But if the government caps the indirect rate at 15% without doing either (A) or (B), then it will be impossible to do research for the federal government without going bankrupt. That’s the worst possible choice. It will kill research in the US. Is that what we want?
I can explain it for you but I can’t understand it for you. It’s up to the reader not to be ignorant.
91
288
1,005
136,004
Jamie Collins retweeted

20 Nov 2024
This study explored how #LLMs handle multiple clinical tasks at once, finding that performance decreases as the number of tasks and notes increases.
High-capacity models showed strong accuracy and efficiency, managing up to 50 tasks with significant cost savings, making them suitable for scaled healthcare applications.
nature.com/articles/s41746-0…
20
39
3,470

19 Nov 2024
I was honored to give the ARP distinguished lecture at #ACR24 -
AI in Rheumatology Practice — Unpacking the Toolkit. AI is here - we all need to understand its limitations and ensure its use is ethical and effective.
acrconvergencetoday.org/arp-…
2
2
20
712
19 Nov 2024
Nelson & Arbeeva. Narrative review of machine learning in rheumatic and musculoskeletal diseases for clinicians and researchers. The Journal of rheumatology. 2022.
Parikh et al. Addressing bias in artificial intelligence in health care. Jama. 2019.
80
19 Nov 2024
A few references:
He et al. The practical implementation of artificial intelligence technologies in medicine. Nature medicine. 2019.
McMaster et al. Artificial intelligence and deep learning for rheumatologists. Arthritis & Rheumatology. 2022.
57
Jamie Collins retweeted

11 Nov 2024
✈️We are thrilled to announce the introduction of the OARSI 2025 World Congress Travel Support Award for Early Career Investigators for #OARSI2025!
Apply during the abstract submission process (includes submission of 1 page letter and short CV). congress.oarsi.org/awards
10
11
1,348
17 Nov 2024
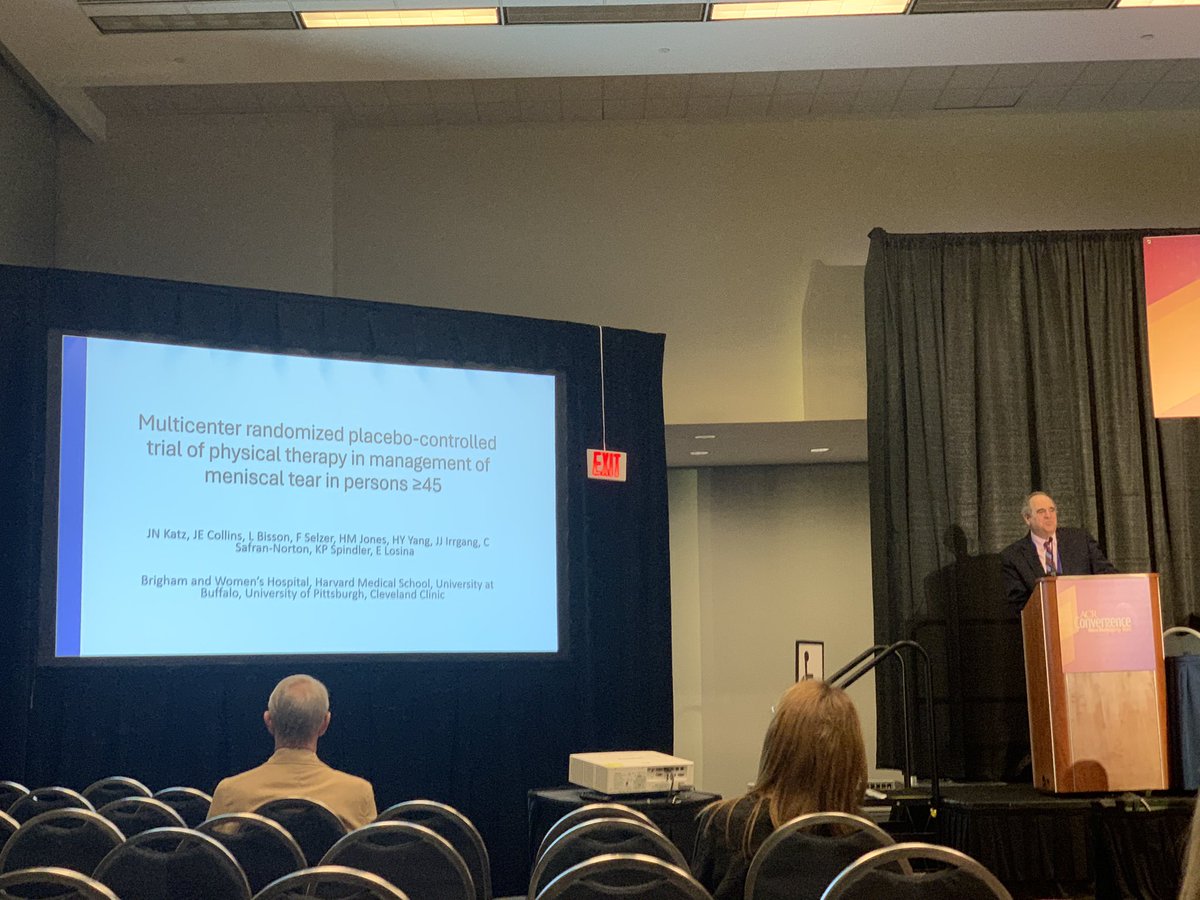
We are so excited to have Dr. Jeff Katz present the results of the @OrACORe_BWH TeMPO trial at #ACR24!
Abstract # 1665: Multicenter Randomized Controlled Trial of Physical Therapy (PT) or Sham PT in Persons with Knee Pain, Meniscal Tear, and Osteoarthritic Imaging Changes
1
2
7
705
9 Sep 2024
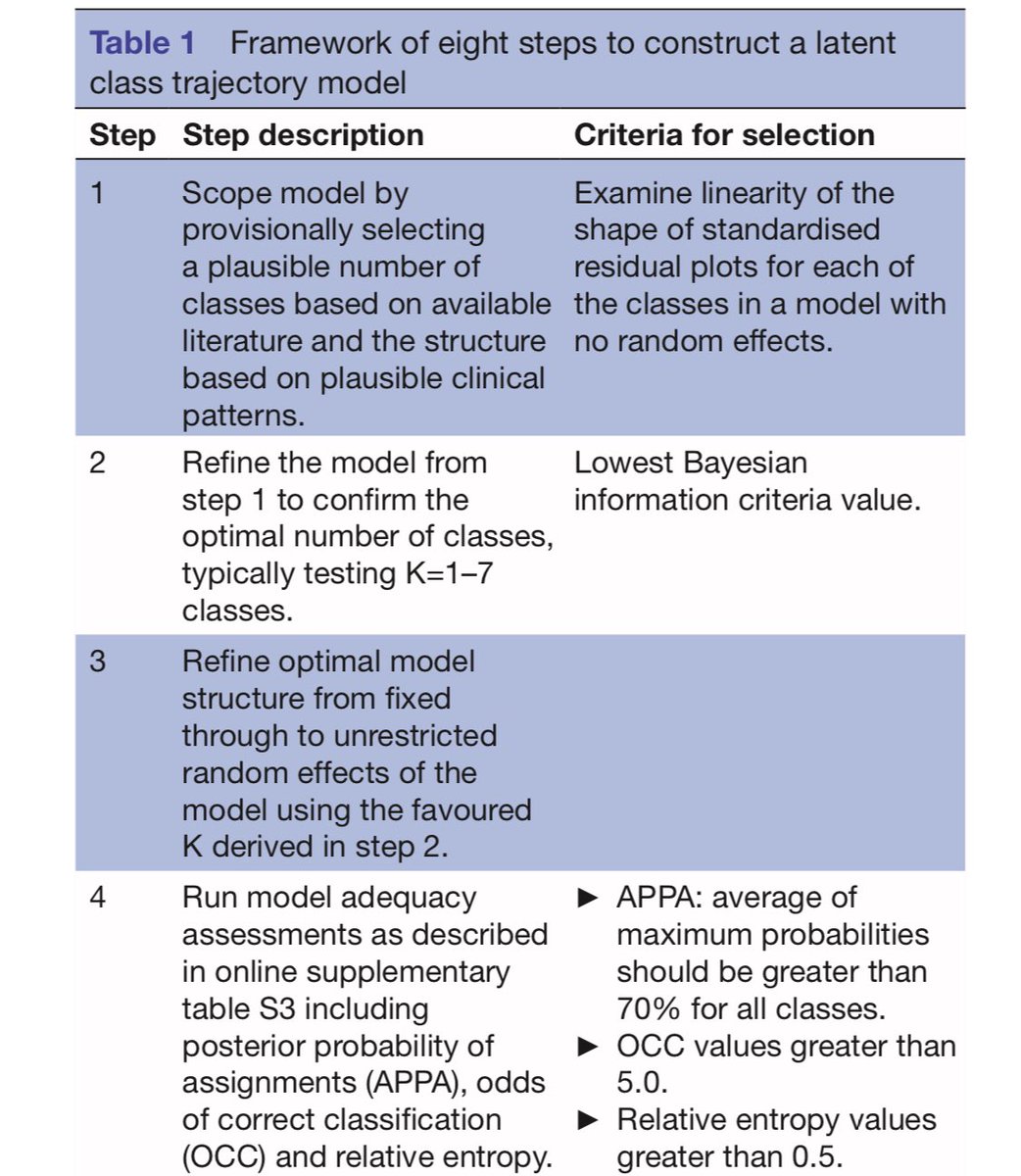
New from me and @OrACORe_BWH RA Samantha Chin in @jrheum - Clustering Methods in Rheumatic and Musculoskeletal Diseases Research: An Educational Guide to Best Research Practices
jrheum.org/content/early/202…
2
17
798
Jamie Collins retweeted

July's #EditorsChoice Paper
🤔 What is the impact of depressive symptoms on cost 💰 in patients with knee osteoarthritis?
@oracore_bwh @colljamie
Read more at doi.org/m5f8 || @OARSInews @ProfDavidHunter

7
12
1,071
Jamie Collins retweeted

25 Jun 2024
Arthroscopic Partial Meniscectomy in Patients With Kellgren-Lawrence Grade 3 Osteoarthritis Shows Clinically Meaningful Improvement in Outcomes - Arthroscopy, Sports Medicine, and Rehabilitation arthroscopysportsmedicineand…
2
9
570
11 Jun 2024
It's the 20th anniversary of the @NIH-sponsored Summer Institute in Biostatistics! We're celebrating today at @BUSPH!
bu.edu/sph/conversations/edu…
3
119
13 May 2024
work from @OrACORe_BWH: Impact of depressive symptoms on direct medical cost among Medicare recipients with knee osteoarthritis - Osteoarthritis and Cartilage
oarsijournal.com/article/S10…
2
6
509
Jamie Collins retweeted

8 May 2024
The deadline is extended so don't miss your chance #early #career #osteoarthritis #investigators!
The @OARSInews @OARSI_ECI peer mentoring program is not just unique but also a great opportunity for professional development and building your network!
25 Apr 2024

Early OA-career investigator alert!
Applications for the second edition of the @OARSInews @OARSI_ECI peer mentoring program is up an you can apply trough the QR code below.
A unique opportunity to receive constructive feedback to further develop your peer reviewing skills!

6
7
1,216