
Joined June 2017
- Tweets 812
- Following 428
- Followers 372
- Likes 1,271
37 Photos and videos








Pinned Tweet

9 Nov 2022
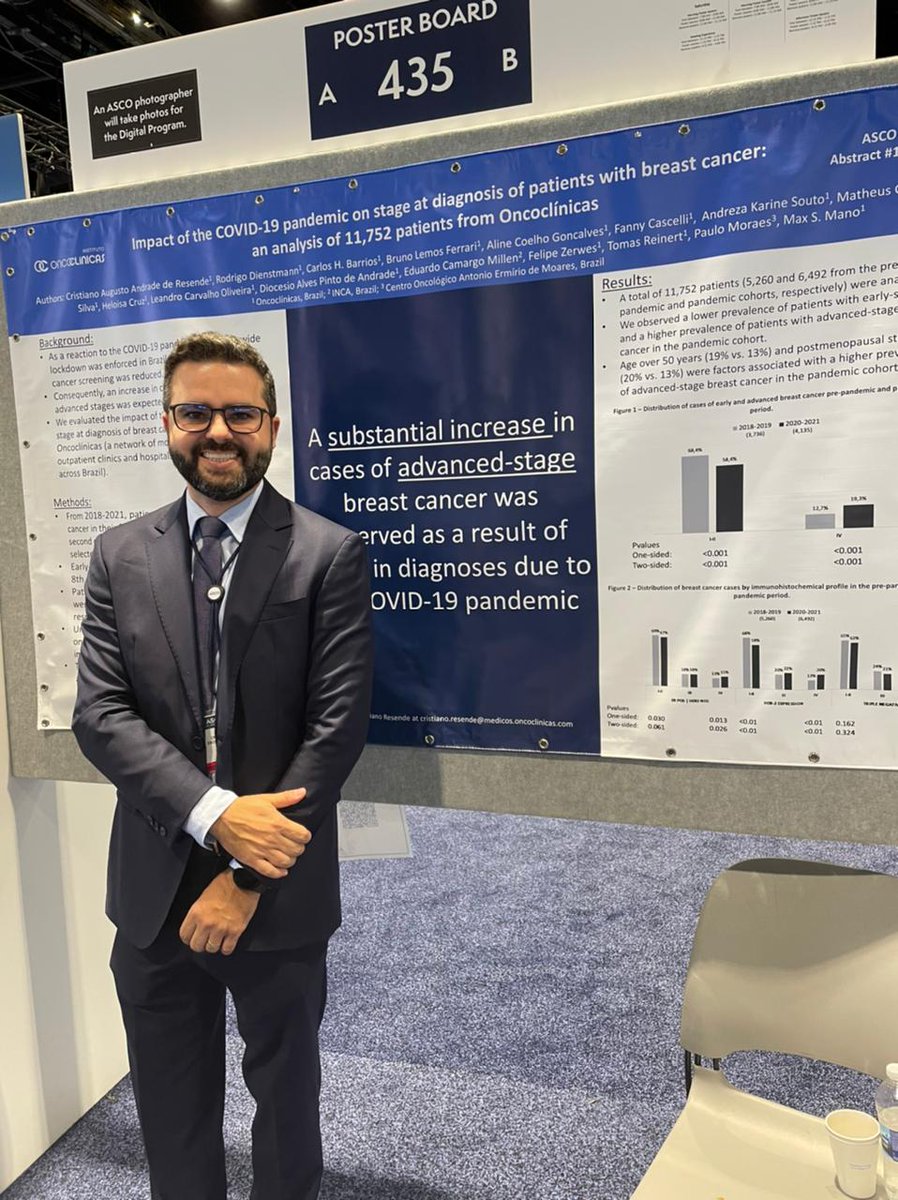
Impact of the COVID-19 Pandemic on Cancer Staging: An Analysis of Patients With Breast Cancer From a Community Practice in Brazil ascopubs.org/doi/abs/10.1200…
Finally our paper was published at @JCOGO_ASCO. I’m very grateful for this opportunity.
6
Dr. Cristiano Resende retweeted

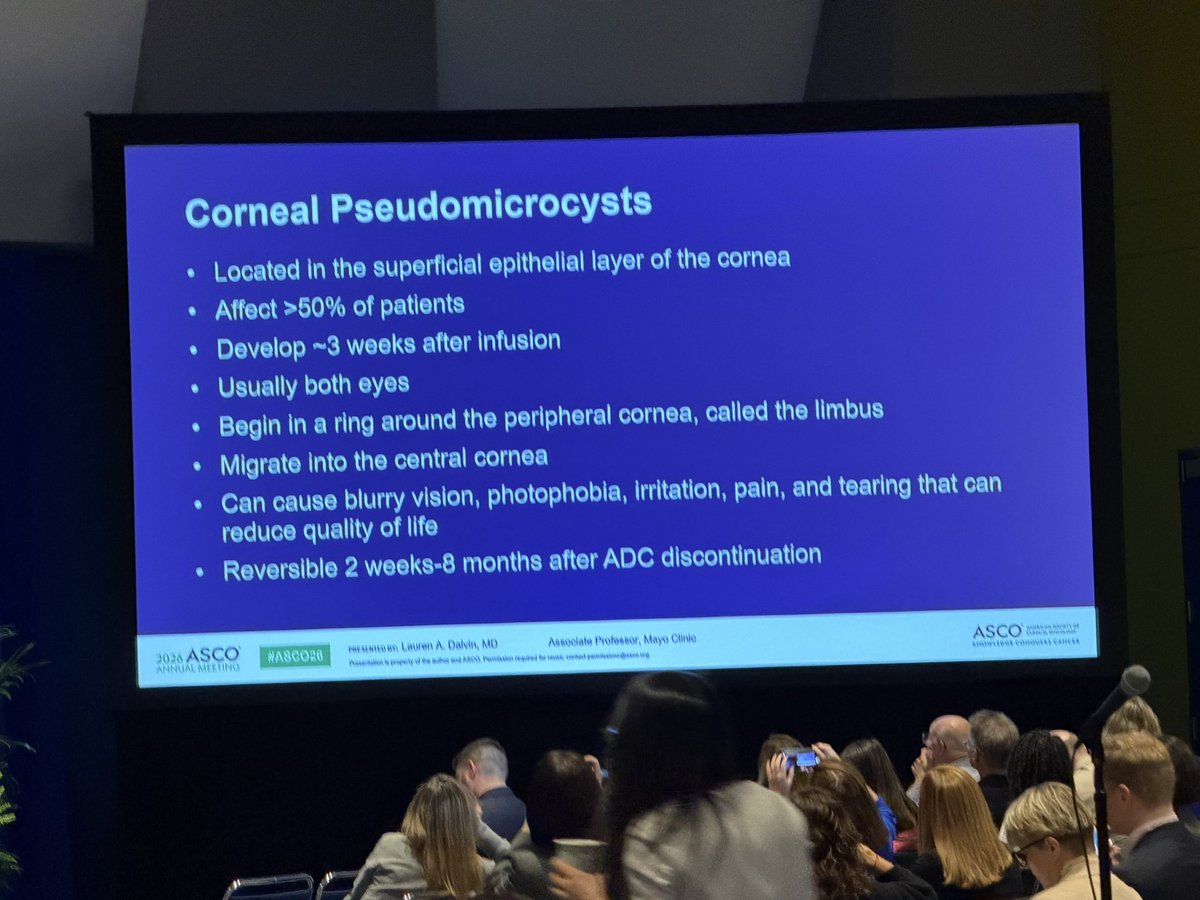
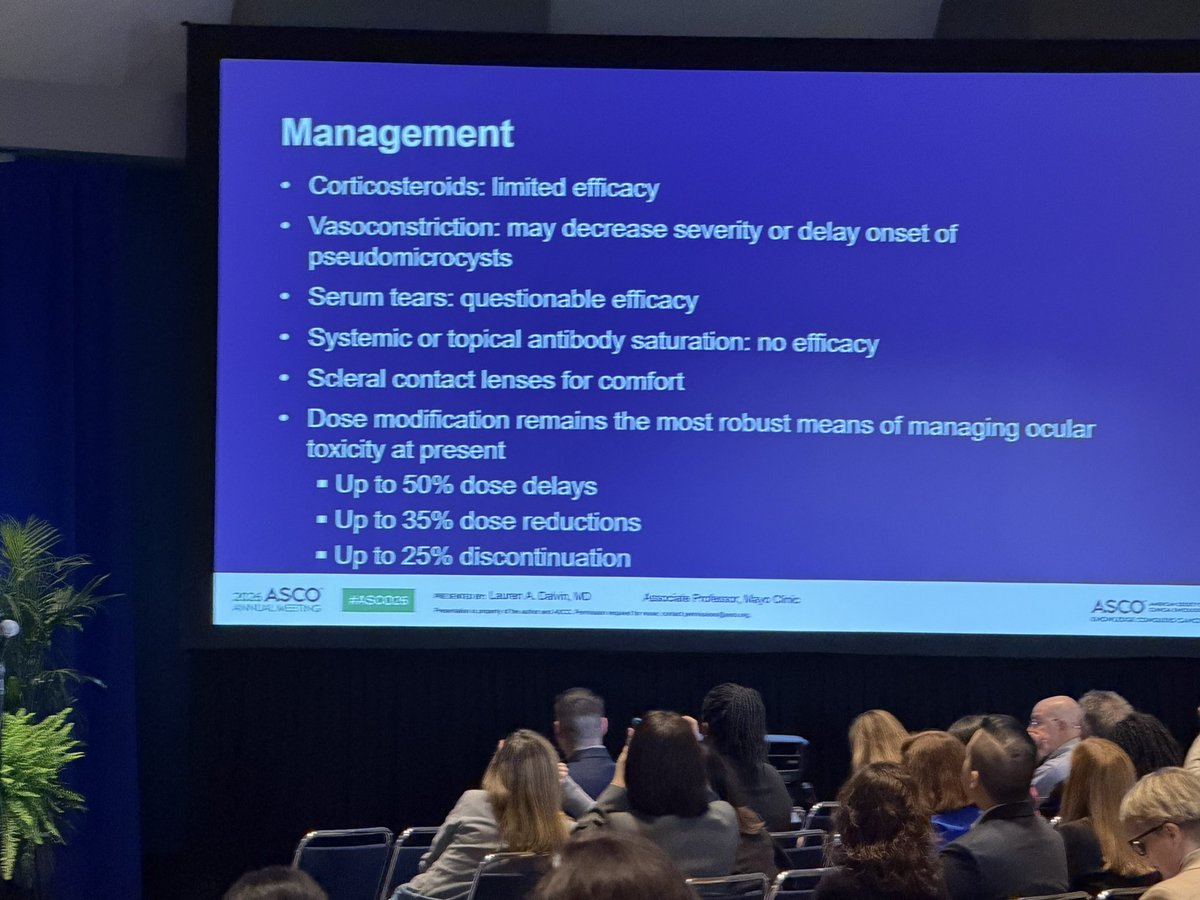
How many of you on ADCs have had 👁️ symptoms? Apparently up to 50% of people on ADCs get these tiny cysts on their corneas. A non-pharm way to decrease may be ice packs on eyes during infusion (missed 📸 that slide) #ASCO26
2
10
23
1,872
Dr. Cristiano Resende retweeted

May 30
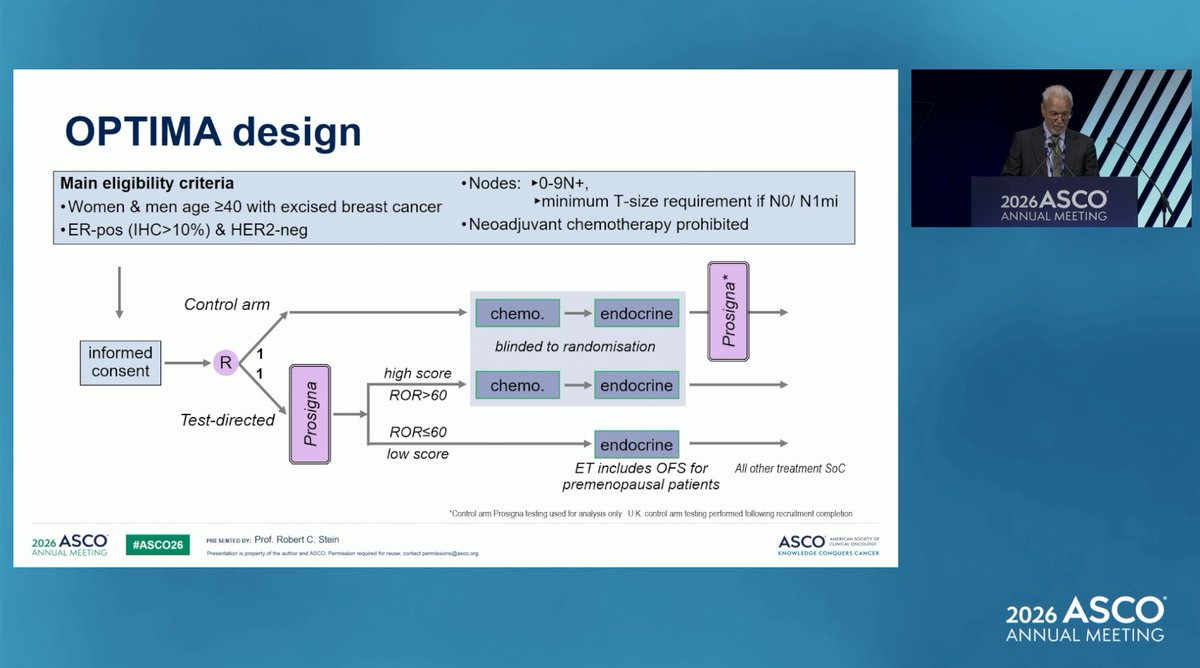
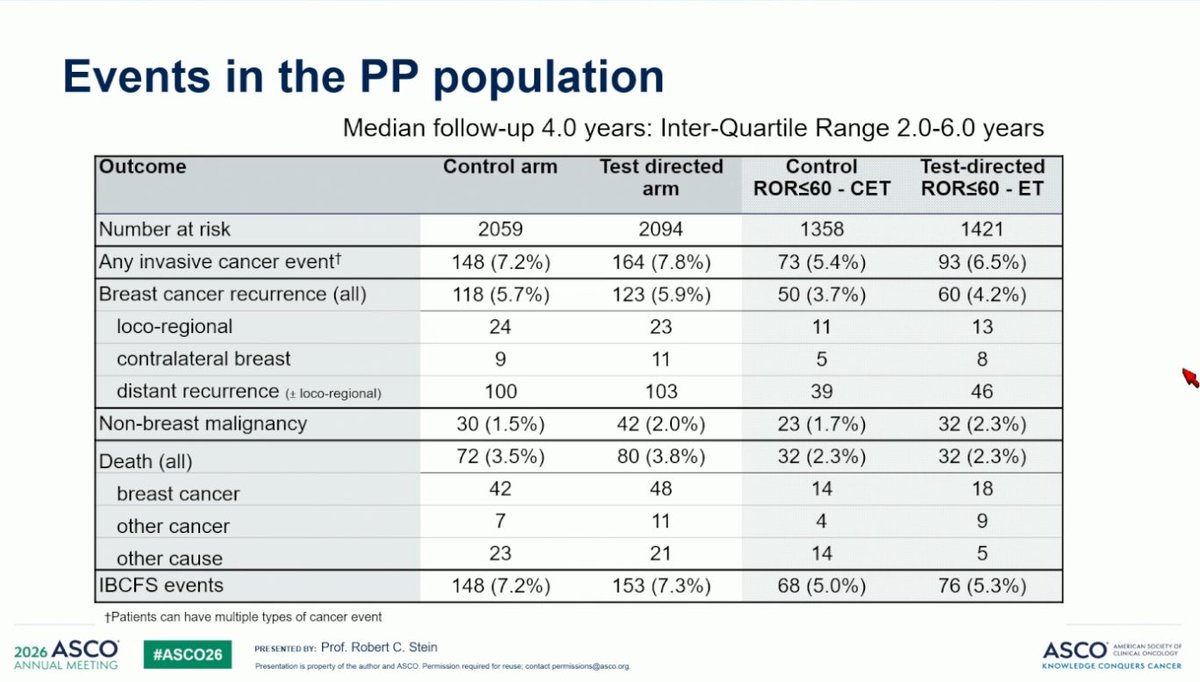
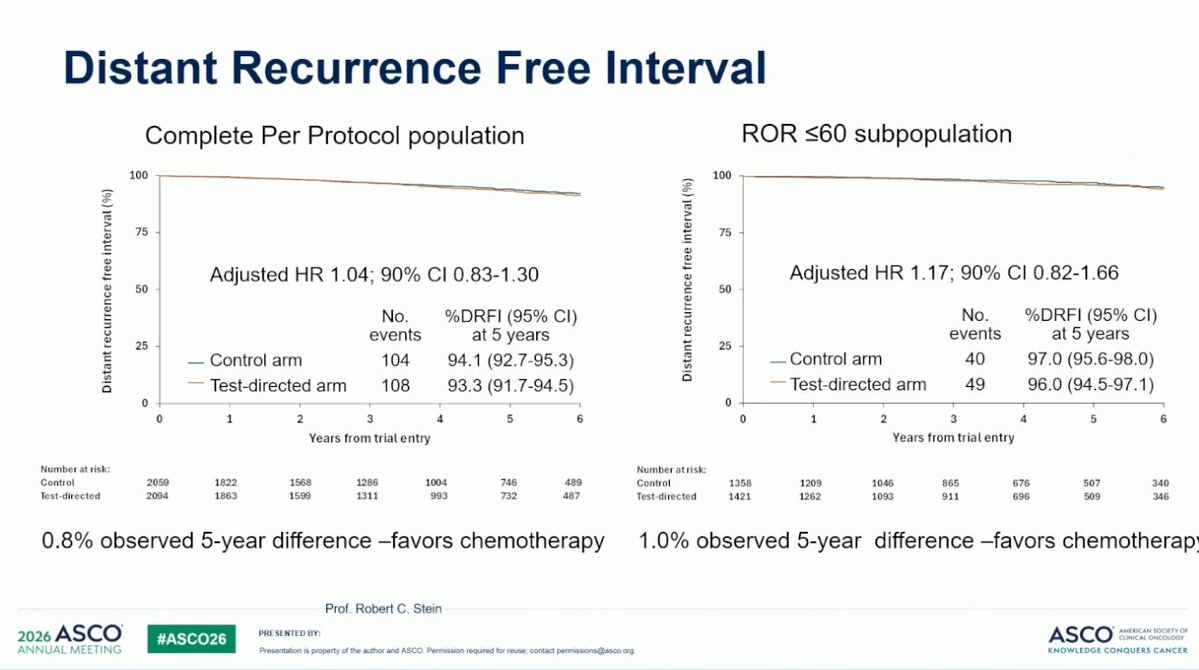
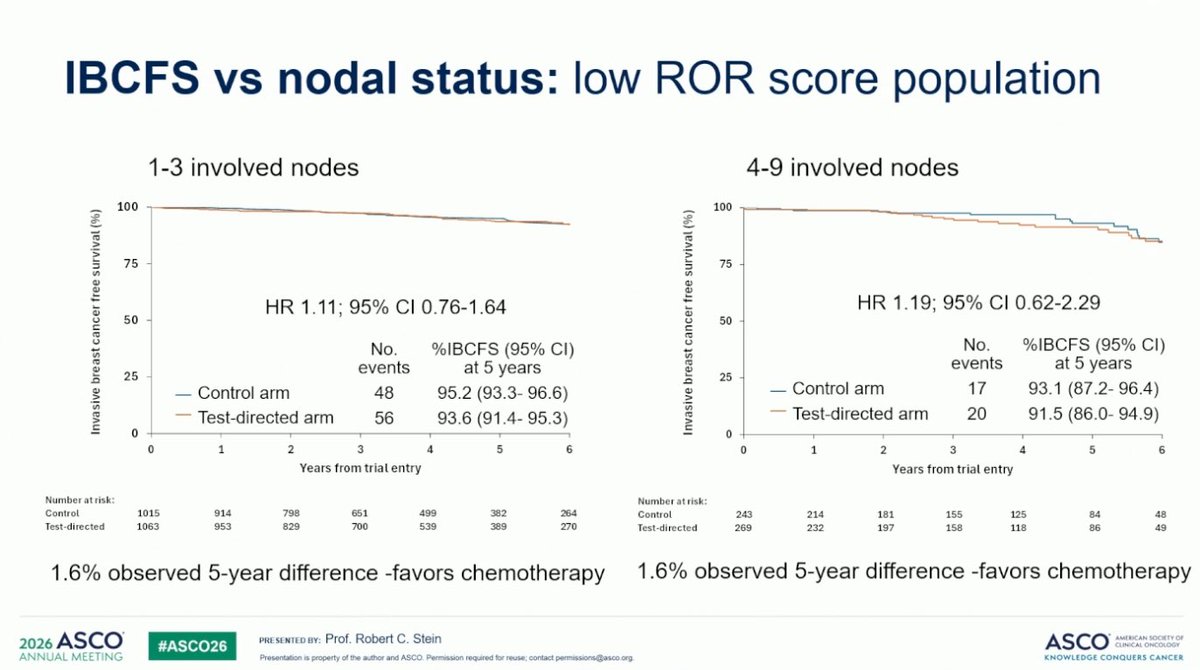
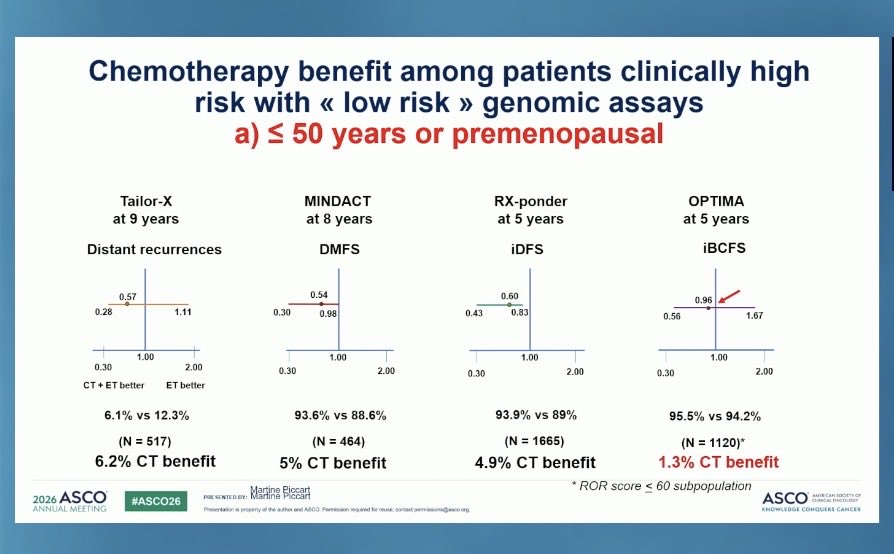
The OPTIMA trial addresses a huge unmet need, and the data, although with short follow up, are striking. Premenopausal patients with N tumors and PAM50 ROR<60 do not appear to benefit from chemo, in the setting of adequate OFS. A step forward toward sparing unnecessary chemo.
3
29
63
4,244
Dr. Cristiano Resende retweeted
May 30
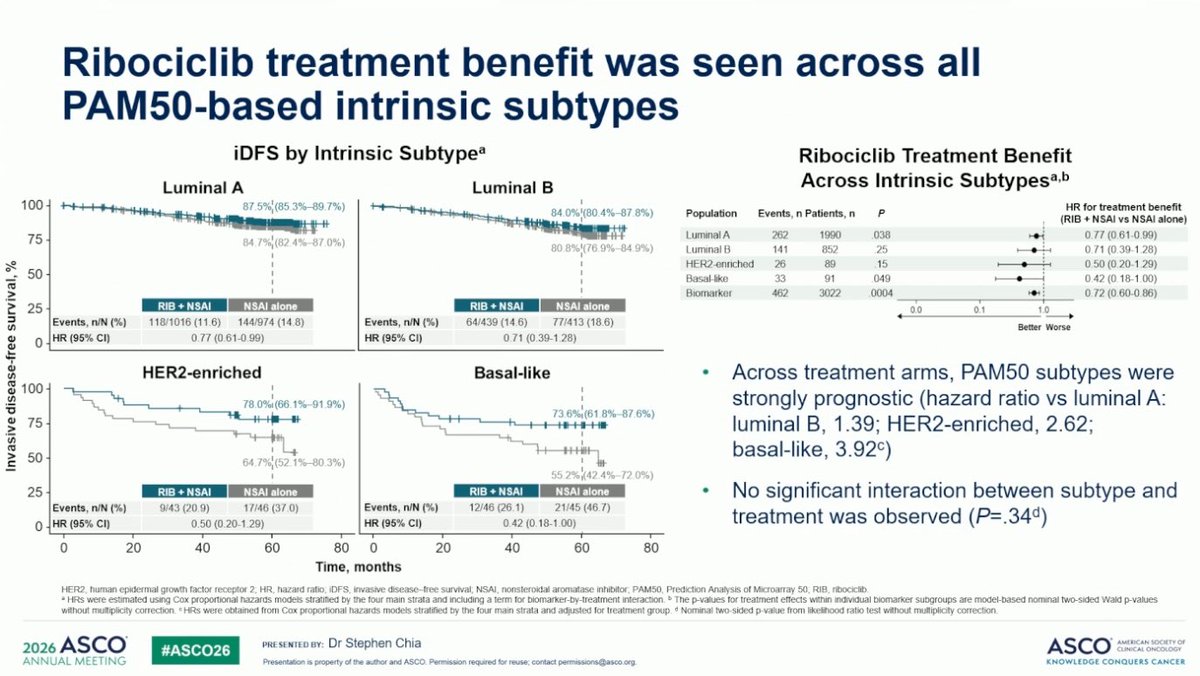
Interesting PAM50 sub-analysis from NATALEE, presented by Stephen Chia, showing a clear prognostic , but not predictive, role for PAM50 subtypes. Benefit from adjuvant ribociclib observed across subtypes and risk scores, with larger delta in HER2-E and basal-like tumors. #ASCO26
4
15
35
2,703
Dr. Cristiano Resende retweeted
May 30
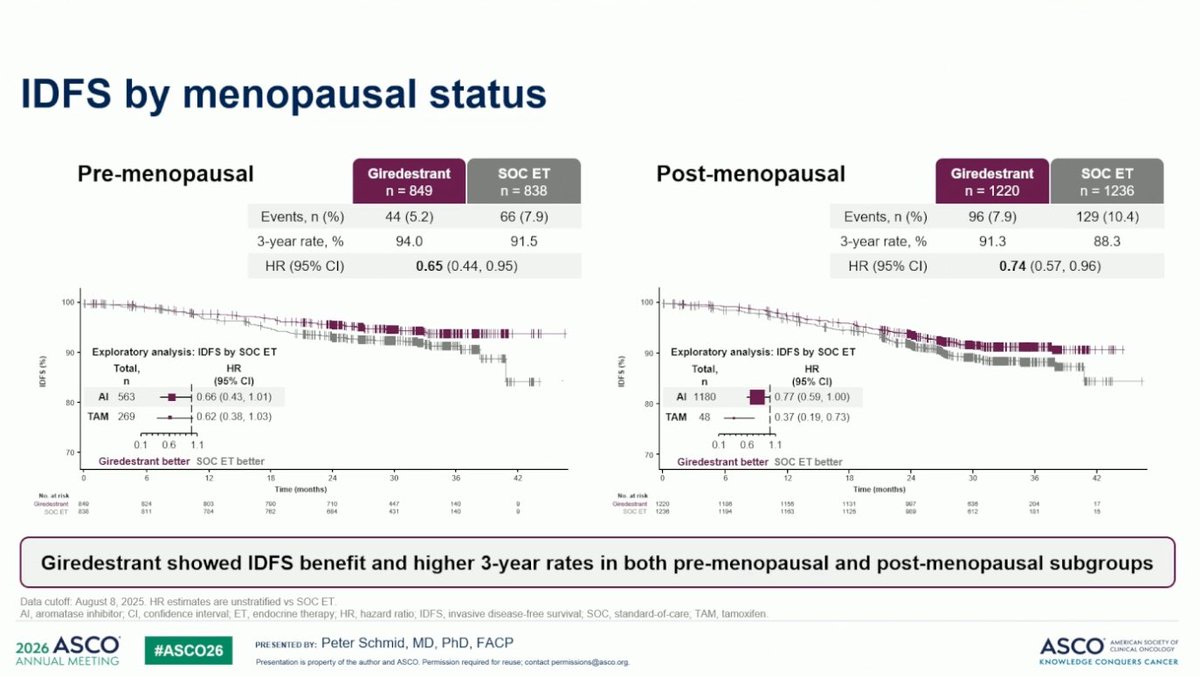
Benefit of adjuvant giredestrant over SoC endocrine treatment was observed irrespective of menopausal status, with a trend towards larger benefit in premenopausal patients. Comparable tox with giredestrant vs AI also seen irrespective of menopausal status (ie unrelated to OFS)
2
17
39
4,267

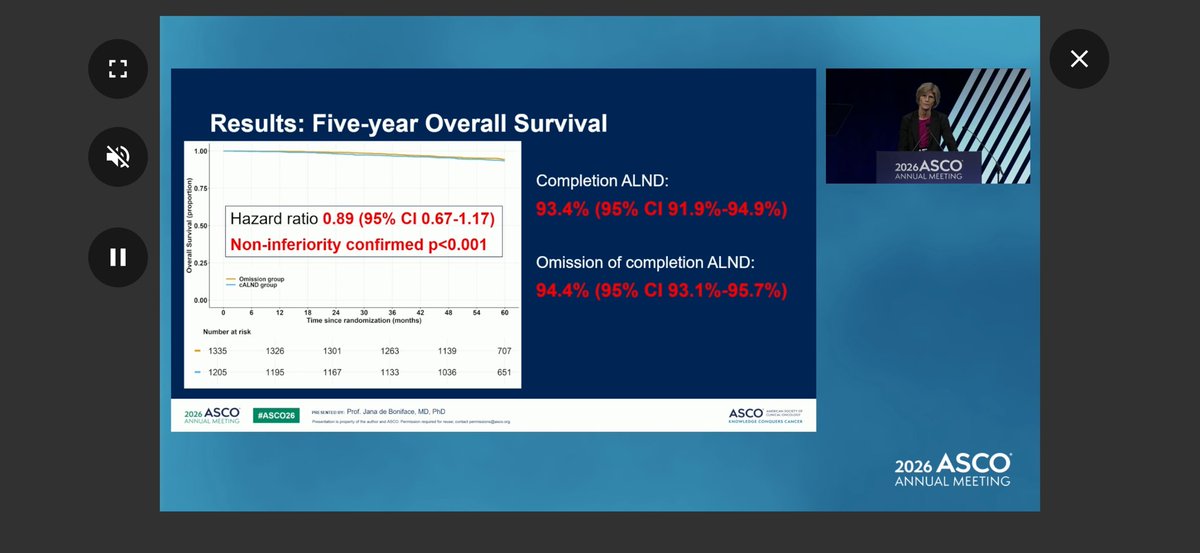
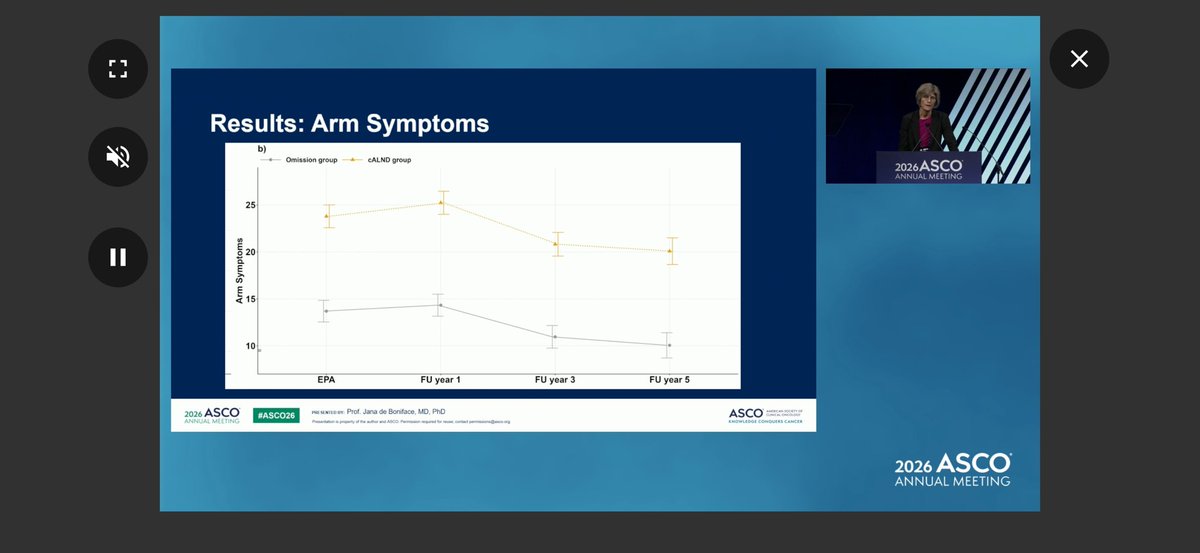
#asco26 Updated results from SENOMAC. AXLND with 1-2 nodes &clin N Neg on exam in HR EBC does not improve dse outcome and impacts QOL (4ever). Most with one N , 34% ENE, all received RT. @OncoAlert

16
36
2,822
Dr. Cristiano Resende retweeted

May 30
Dr Piccart reinforces that OPTIMA for the first time prospectively shows the chemo benefit for premenopausal low GEP women, is mostly due to chemotherapy induced ovarian suppression.
2
37
79
8,552
Dr. Cristiano Resende retweeted
May 30
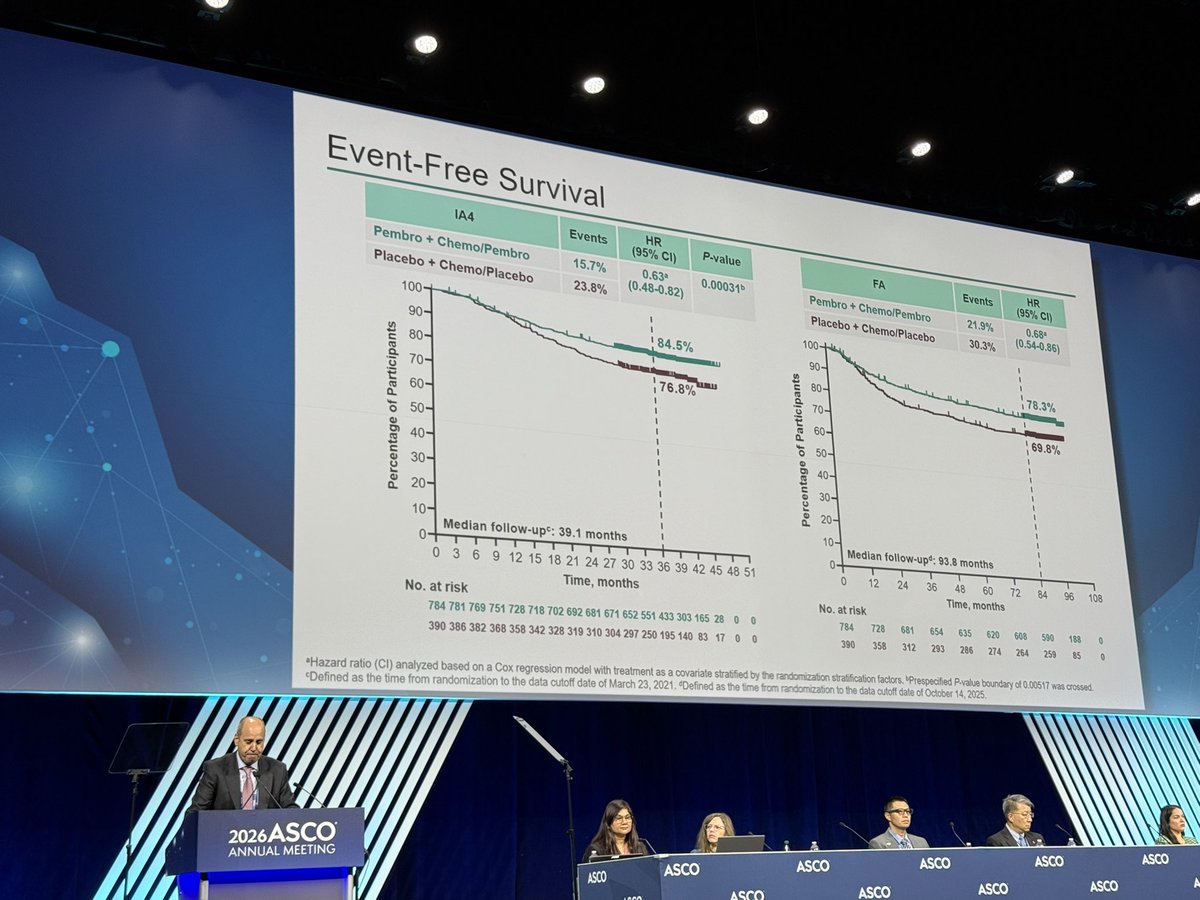
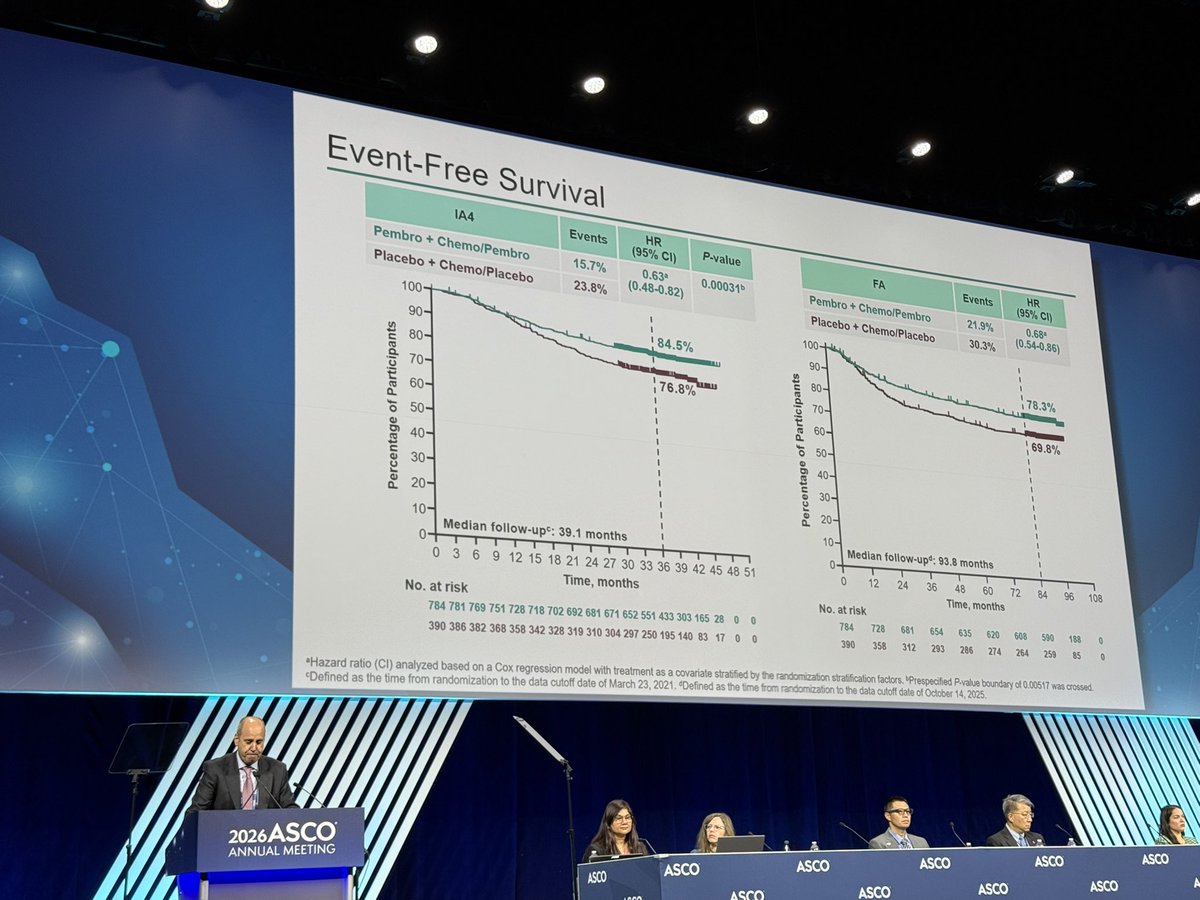
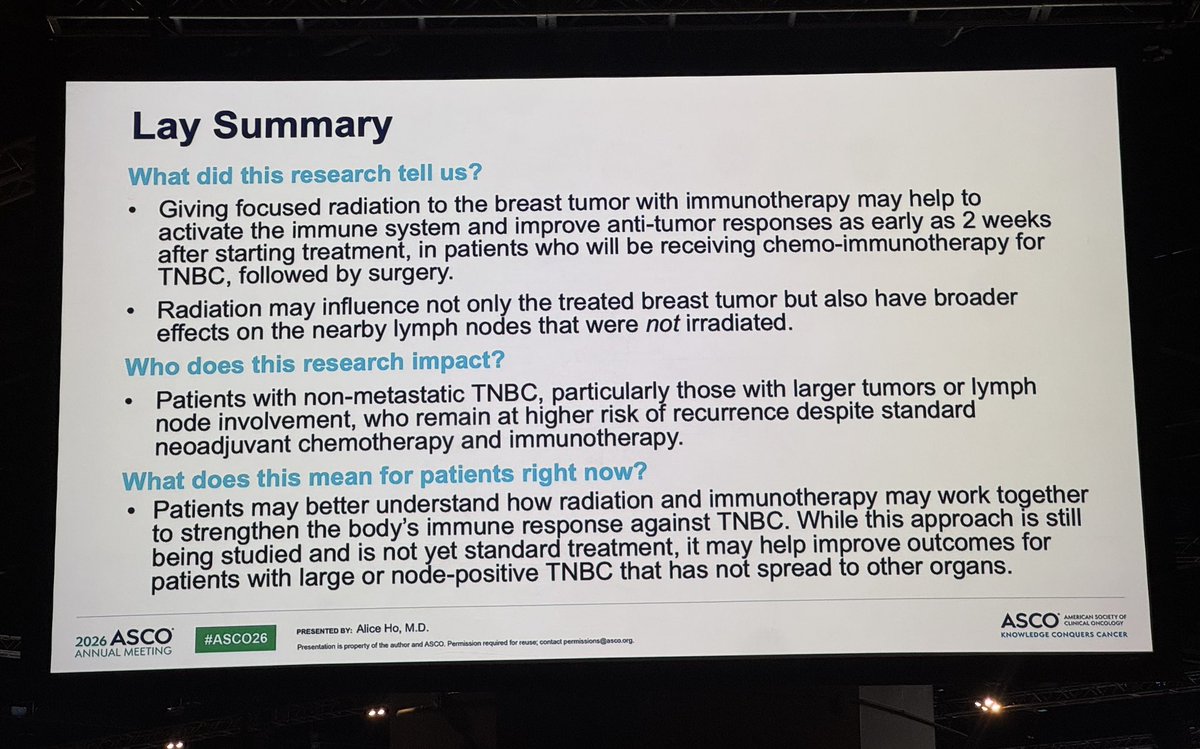
8-year results from KEYNOTE-522 presented by @JavierCortesMD. Adding perioperative pembro to neoadjuvant chemo prevents ~10% recurrences and ~7% deaths from TNBC. A tough neoadjuvant regimen, but one that clearly saves lives. No TILs data presented yet, unfortunately. #ASCO26
23
55
3,642
Dr. Cristiano Resende retweeted

The final analysis of KEYNOTE-522 will be presented at ASCO 2026.
Please, present subgroup analyses according to TIL levels.
This is essential to deepen our understanding and help move the field forward as a scientific community.
@OncoAlert

3
6
18
5,001
Dr. Cristiano Resende retweeted
May 31
Subgroup analysis from ASCENT-04 presented by @stolaney1. Consistent PFS benefit from SG/pembro (vs chemo/pembro) across Trop2 expression, tBRCA status and HER2 IHC status. #ASCO26

16
37
2,619
Dr. Cristiano Resende retweeted
May 31
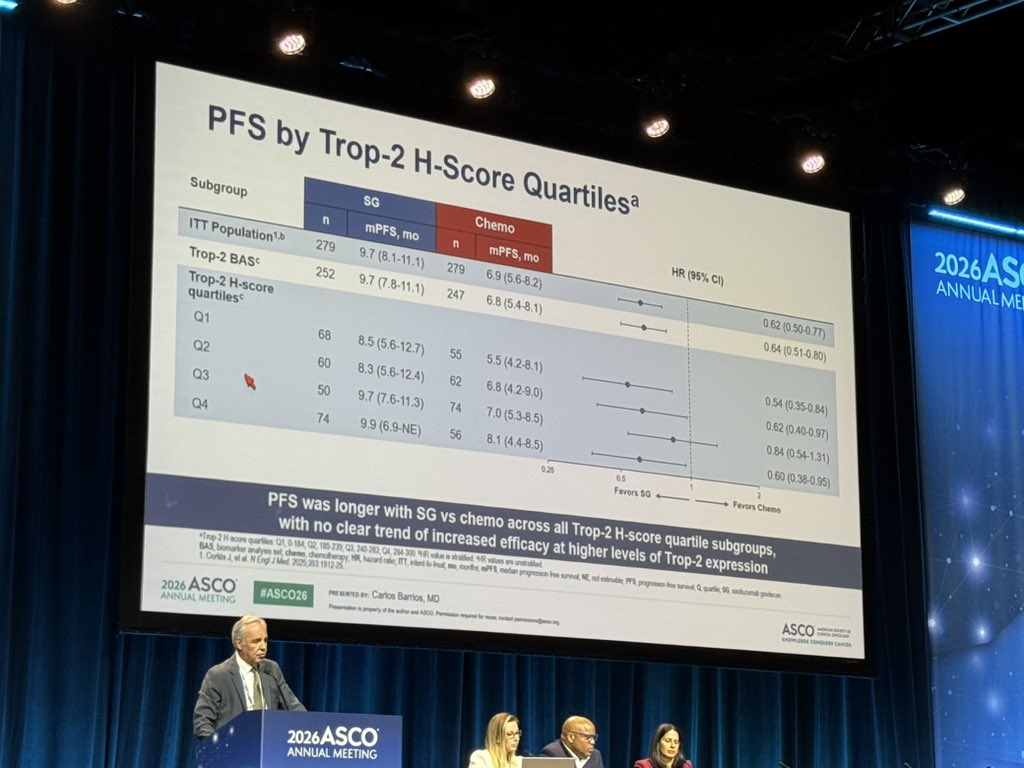
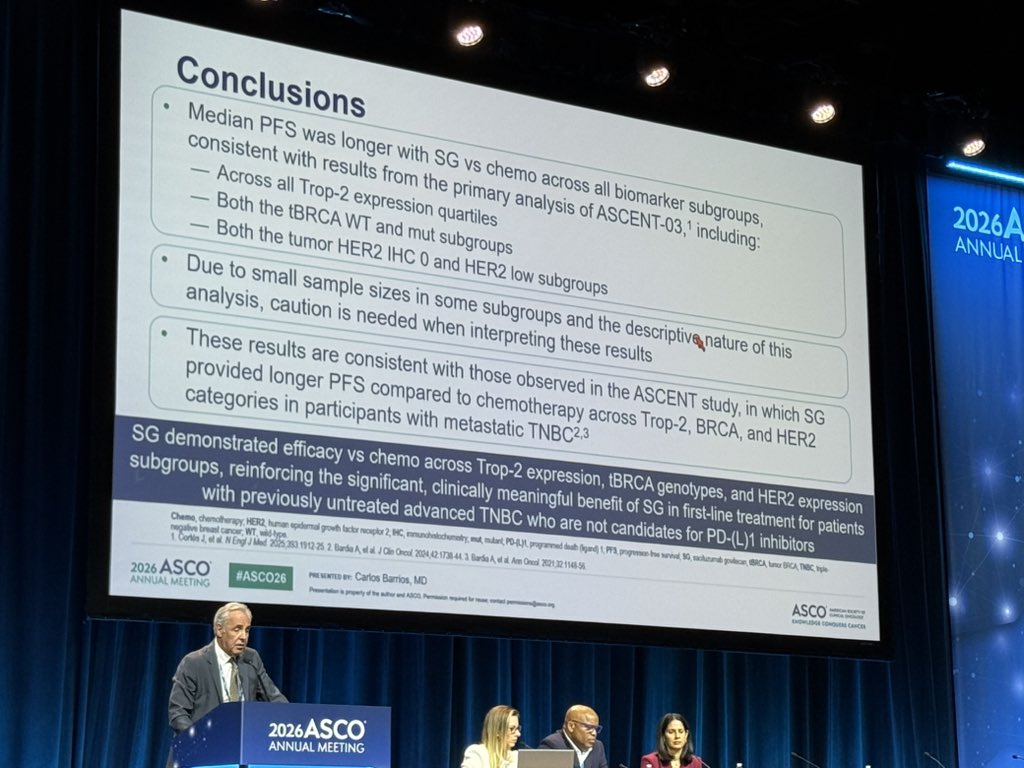
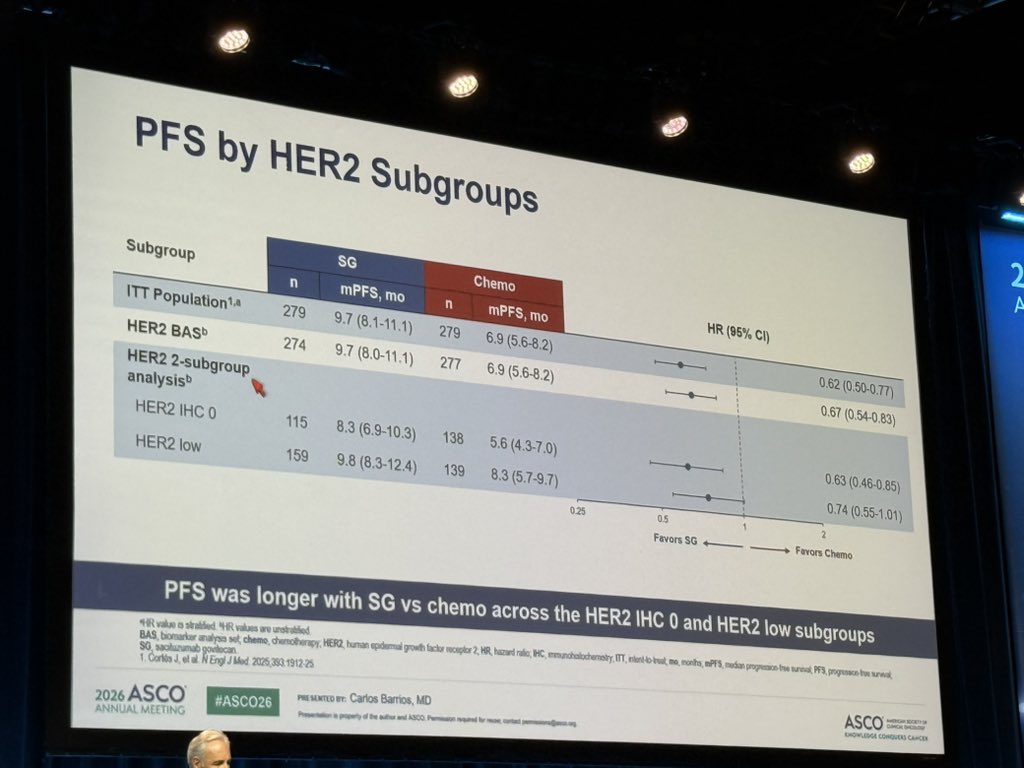
Similar to ASCENT-04, subgroup analysis from ASCENT-03 shows consistent PFS benefit with SG vs chemo across Trop2 expression, tBRCA status and HER2-status. Presented by Carlos Barrios #ASCO26

1
12
23
4,752
Dr. Cristiano Resende retweeted
May 31
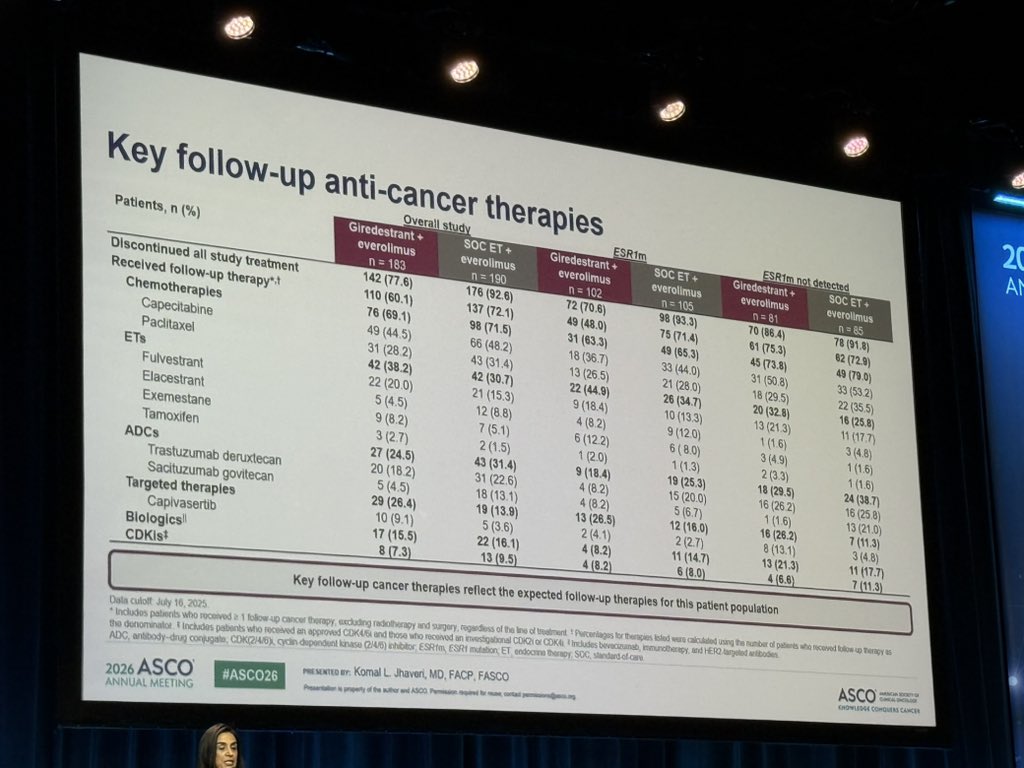
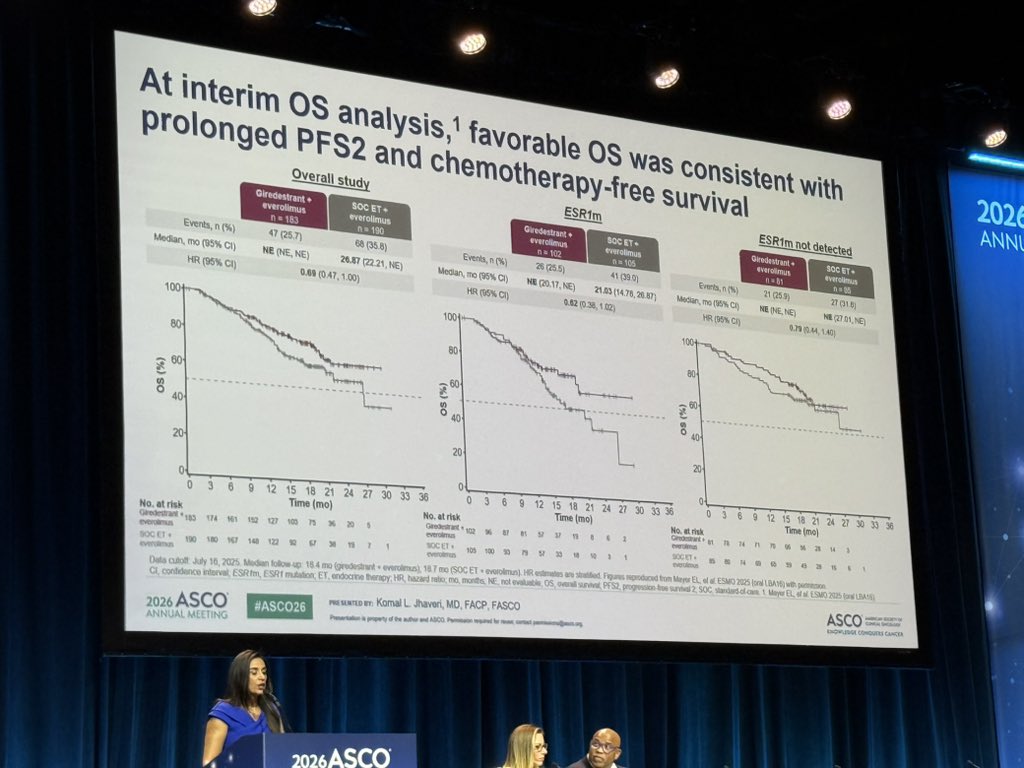
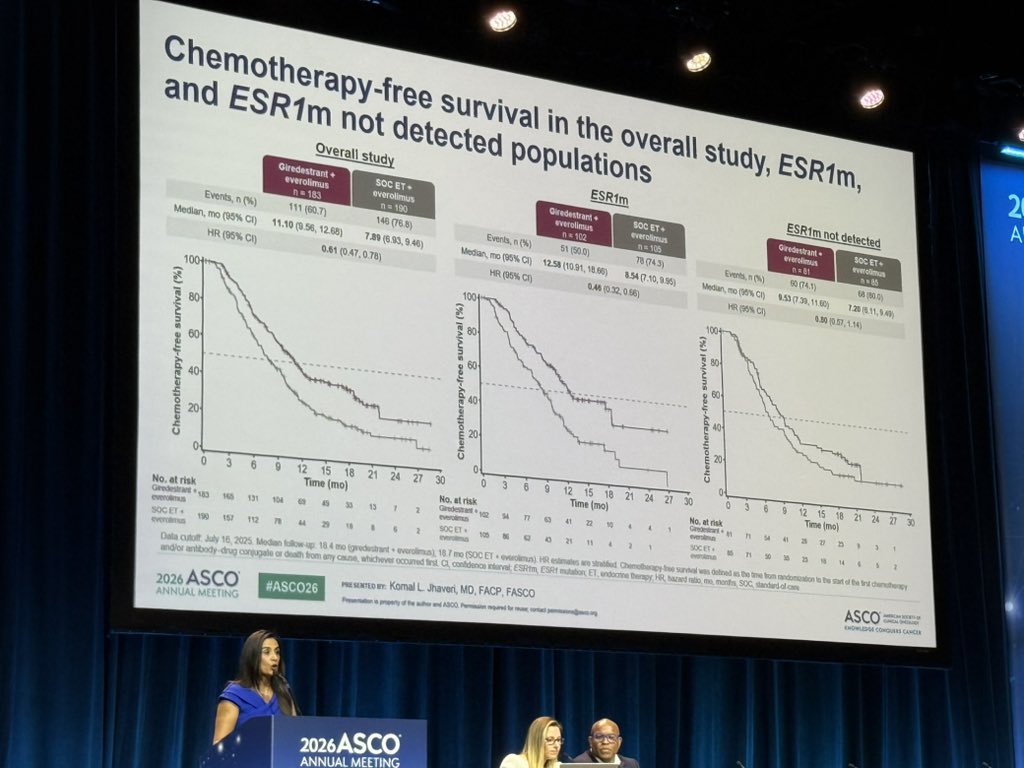
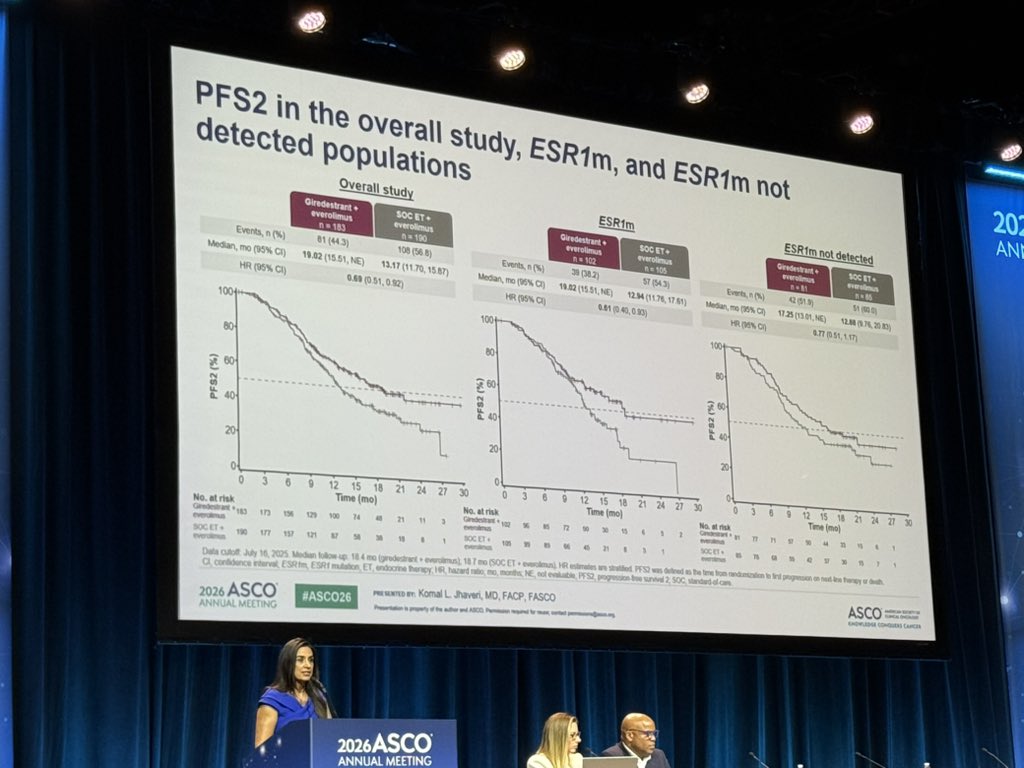
Promising PFS2 and OS data from evERA presented by @jhaveri_komal, showing clear improvement in outcomes with giredestrant/everolimus vs SoC ET/everolimus in ESR1mut disease, with a promising signal in ESR1wt patients as well. #ASCO26
1
16
37
2,387

Dr. Cristiano Resende retweeted
May 31
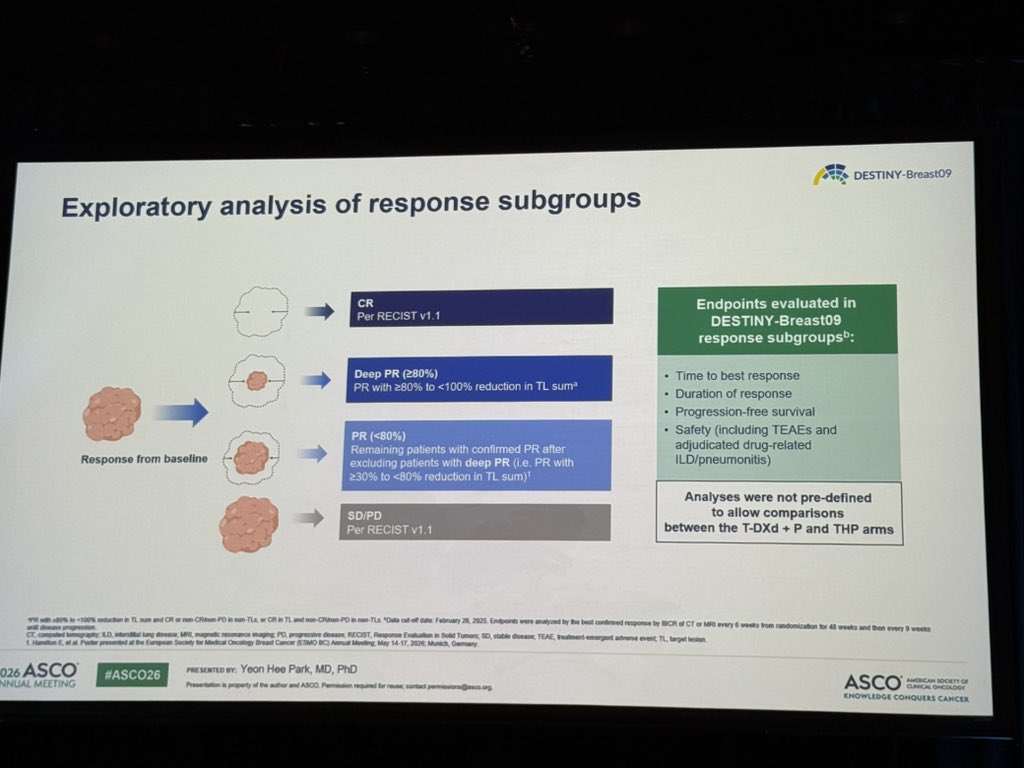
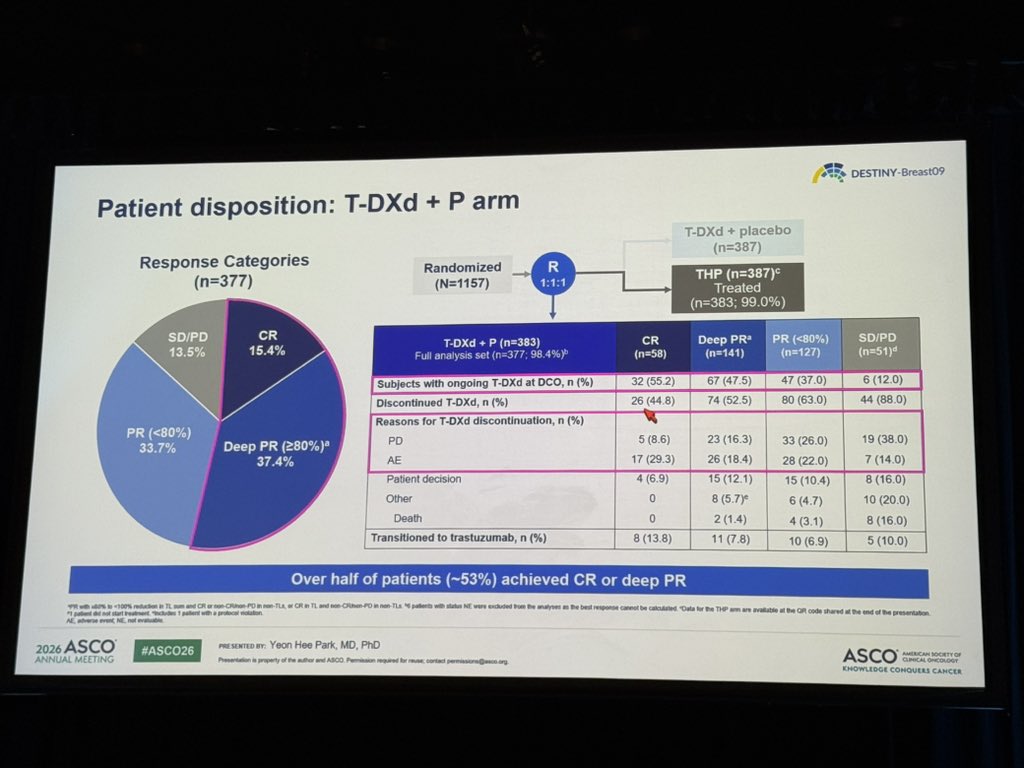
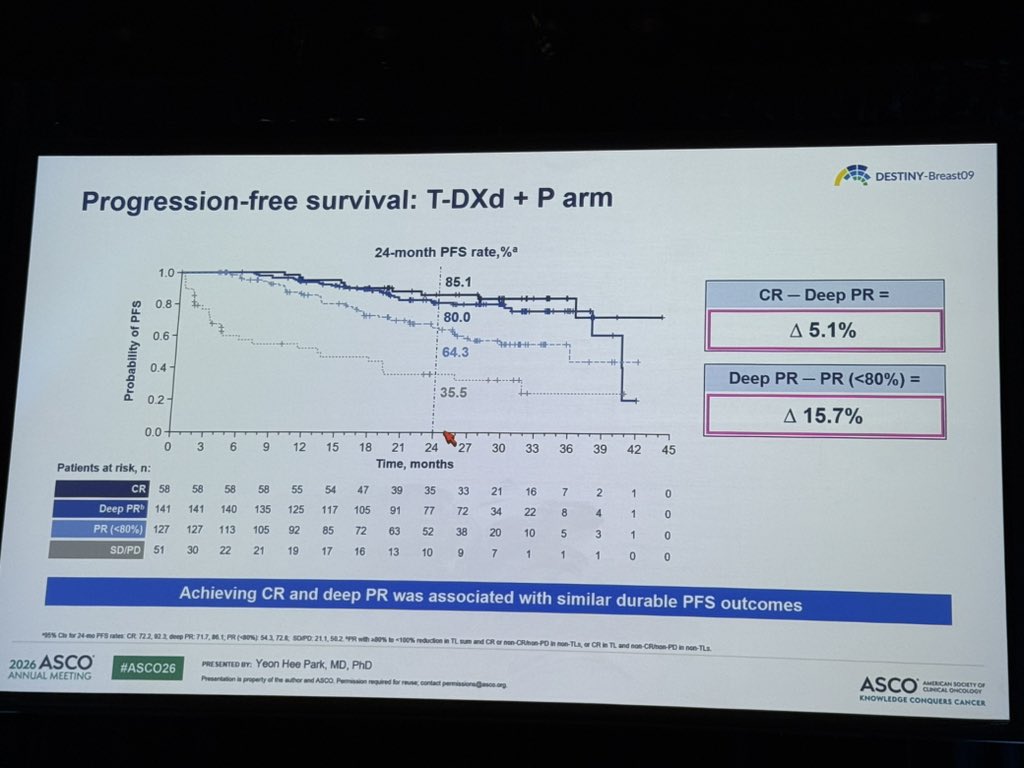
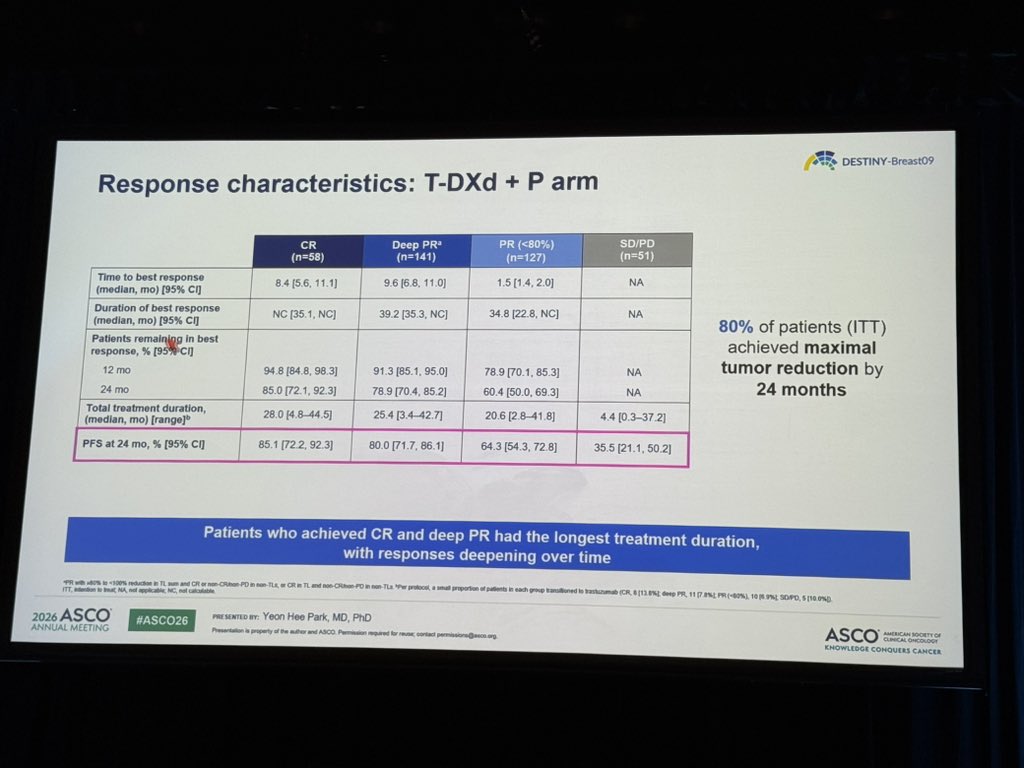
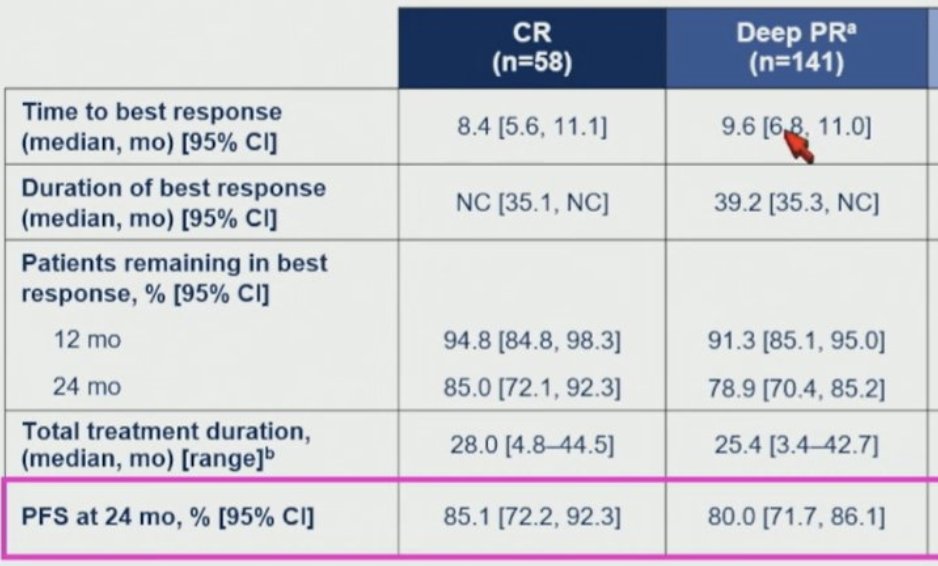
Interesting sub-analysis of DB09, showing tremendous (and comparable) outcomes with 1L T-DXd/P among patients with HER2 MBC that achieve a CR or a deep PR. Median maximum tumor reduction observed at 11 months. #ASCO26
2
26
64
9,000
Dr. Cristiano Resende retweeted
Jun 1
My take:
- we don’t treat metastatic disease to shrink the tumor, but to prolong OS and maintain/improve QoL
- that said, some patients with HER2 do get cured. Could longer T-DXd increase that rate? TBD
- shared decision making is KEY to personalize the duration of 1L T-DXd/P!!
May 31

This analysis is powerful: patients who reach CR do so at ~8.4 months, stay on T-DXd for ~28 months, and many responses are still ongoing at cutoff. This really makes us question whether T-DXd needs to be continued beyond CR or deep PR, or if we should transition to a more easily tolerated maintenance approach instead. Ongoing trials like DIMITHER and other induction-maintenance studies will help answer this.
2
4
40
8,188
Dr. Cristiano Resende retweeted

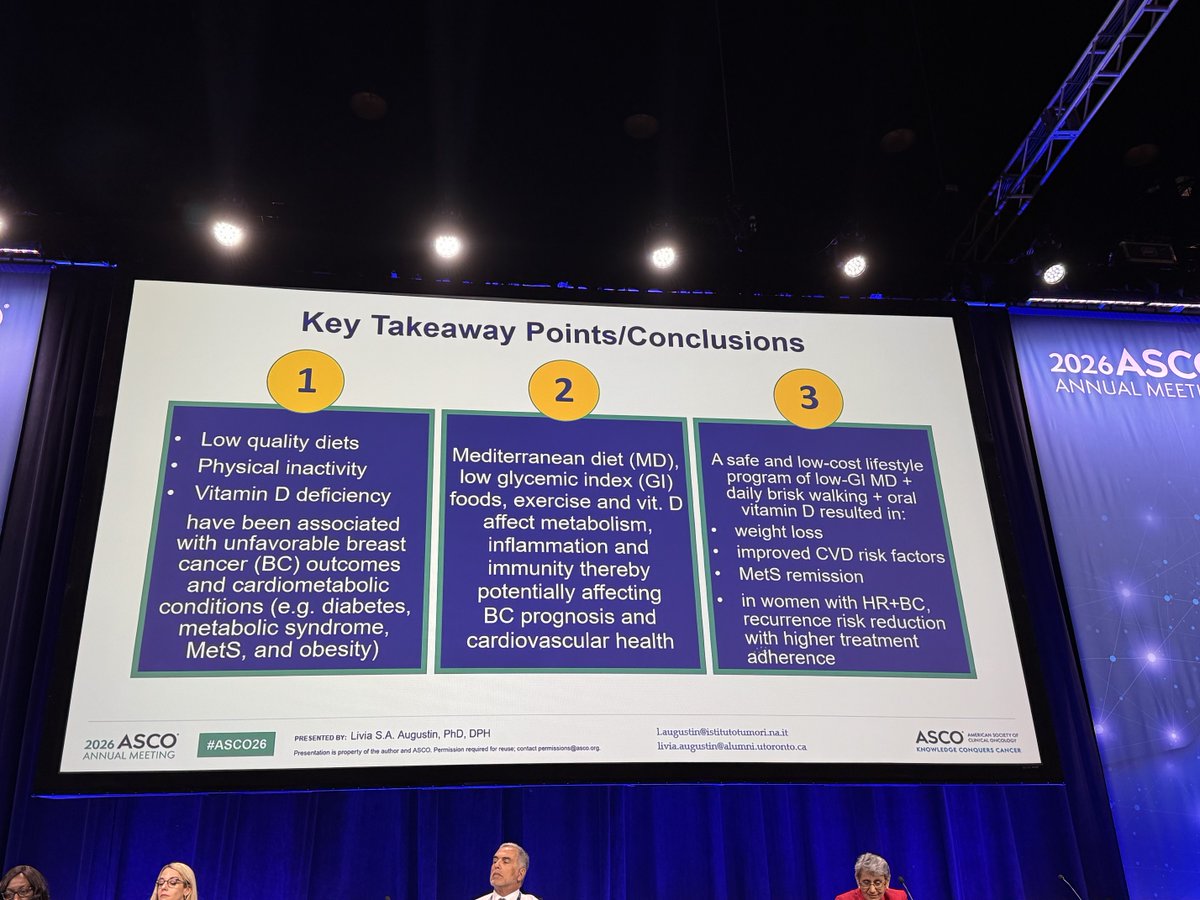
Your mother was right. Better diet, more exercise, and sunshine are good for you and might even lower breast cancer recurrence! ☀️ 🏃♀️ 🥗
3
26
101
6,063
Dr. Cristiano Resende retweeted

Jun 1
#ASCO26
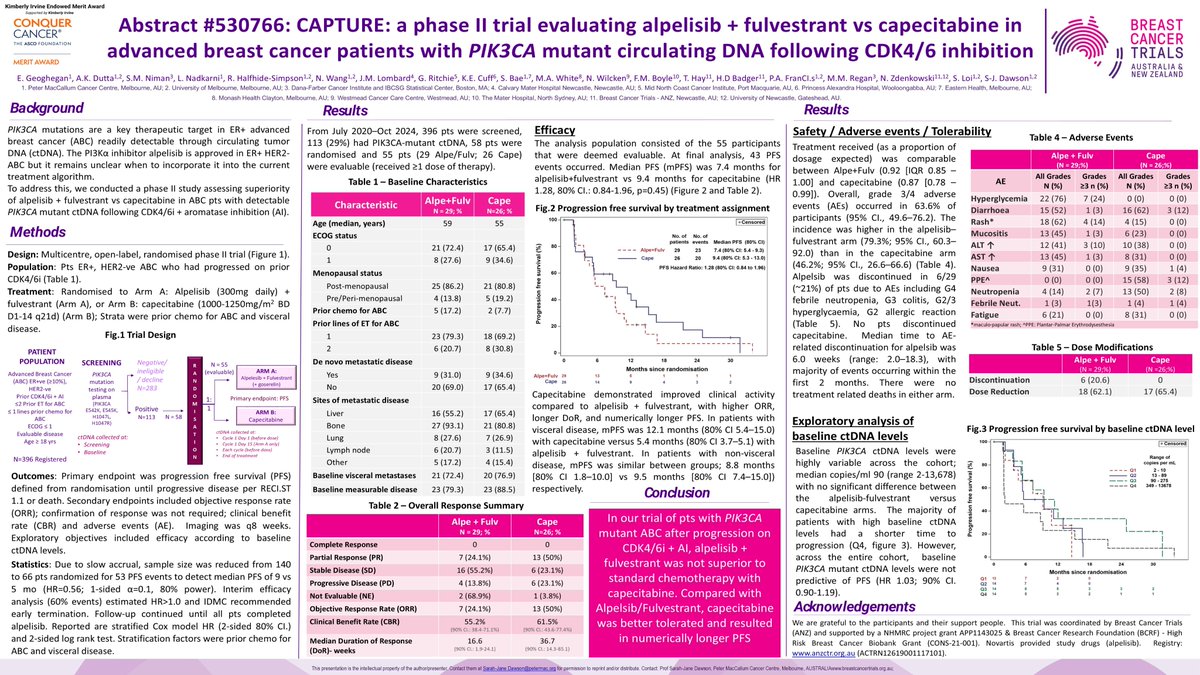
In pts with PIK3CA-mutant disease after CDK4/6i AI, the real clinical value of alpelisib may not be as strong as suggested by single-arm studies such as BYLieve.
In my view, this study deserved an oral presentation rather than just a poster.
May 30

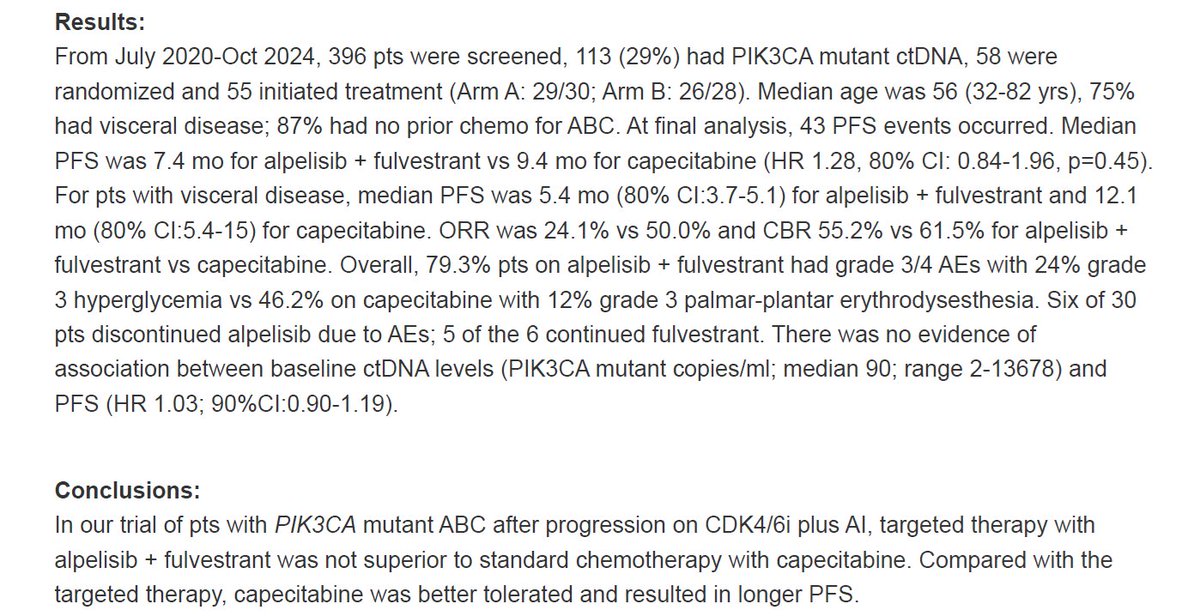
#ASCO26 abst 1064
CAPTURE showed that in post-CDK4/6 PIK3CA-mutant HR /HER2− MBC, alpelisib fulvestrant did not beat capecitabine.
PFS: 7.4 vs 9.4 months; ORR: 24% vs 50%.
In patients with visceral disease, the picture was even more in favor of capecitabine.
The presence of a biomarker alone does not define the right treatment sequence.
Beating capecitabine is not that easy!!!
I wonder how capivasertib fulvestrant would have performed here?
2
11
26
4,877



Dr. Cristiano Resende retweeted
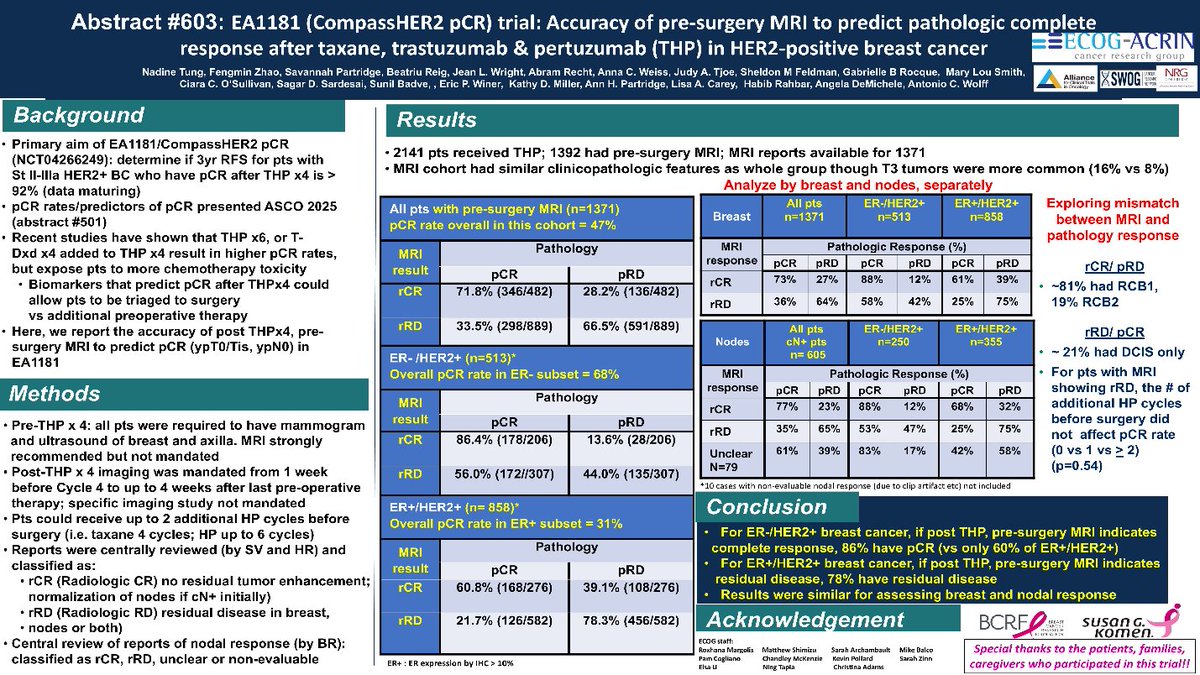
Very nice report. Key is that MRI was quite predictive in HER2 but less so for ER

#ASCO26 Poster Session | Poster #88 | Accuracy of pre-surgery MRI to predict pathologic complete response after taxane, trastuzumab, and pertuzumab (THP) in HER2-positive #BreastCancer. @NTungMD
1
11
34
5,116
Dr. Cristiano Resende retweeted

Jun 1
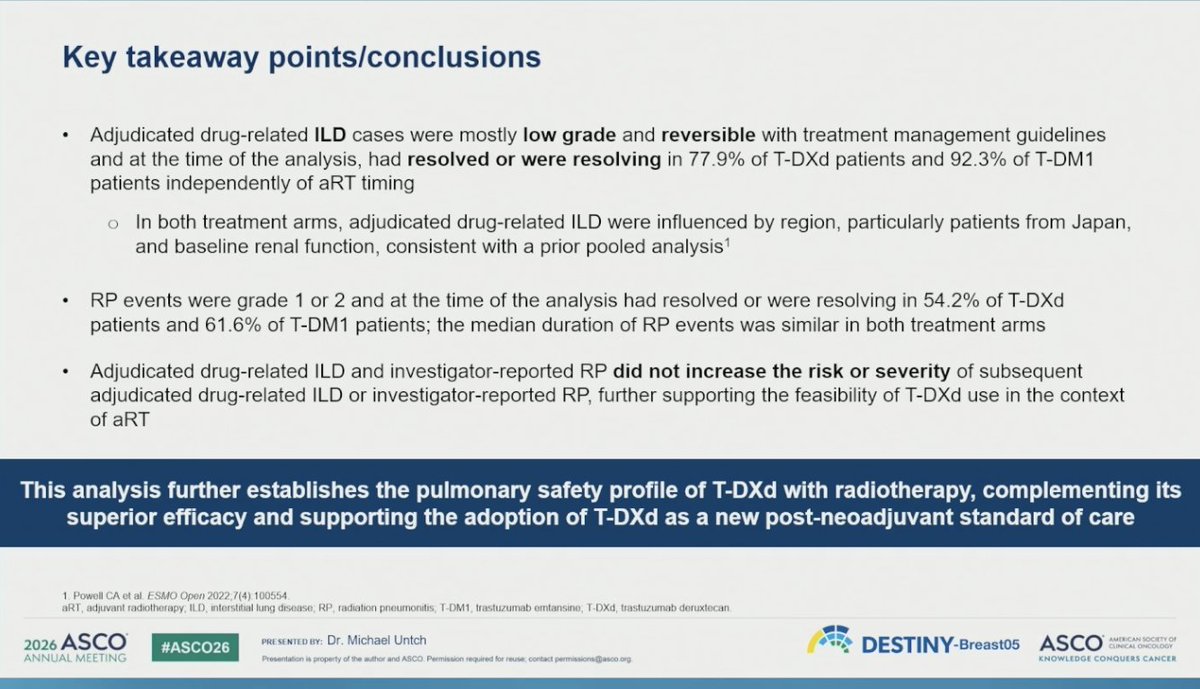
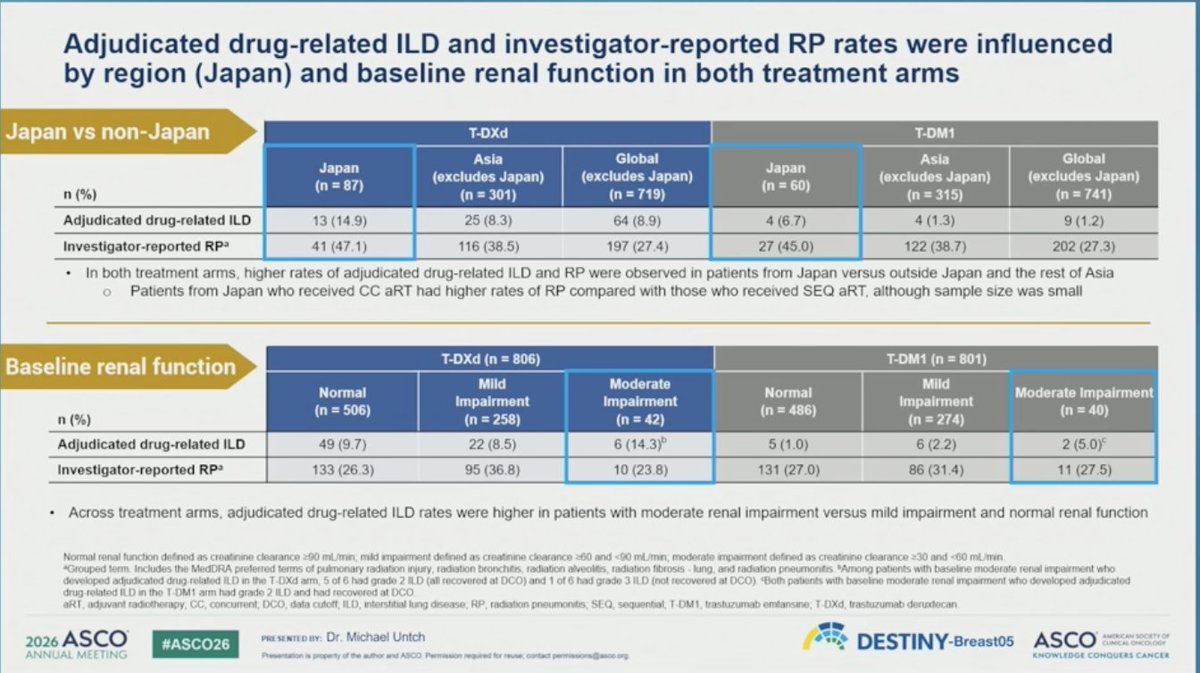
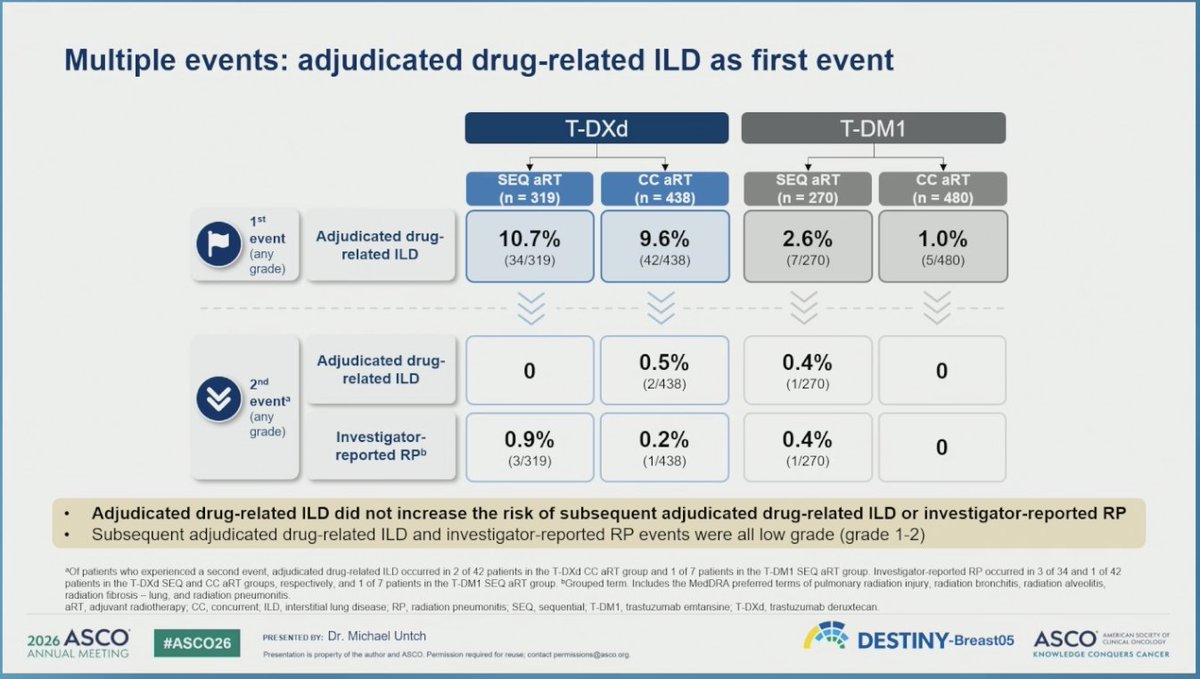
DESTINY-Breast05 ILD/radiation pneumonitis
ILD higher in pts from Japan and in pts with moderate/renal impairment
@OncoAlert #ASCO26

2
22
41
17,058
Dr. Cristiano Resende retweeted

Jun 2
2/ @PTarantinoMD on patients with HER2 BC and lower risk RD:
x.com/PTarantinoMD/status/20…
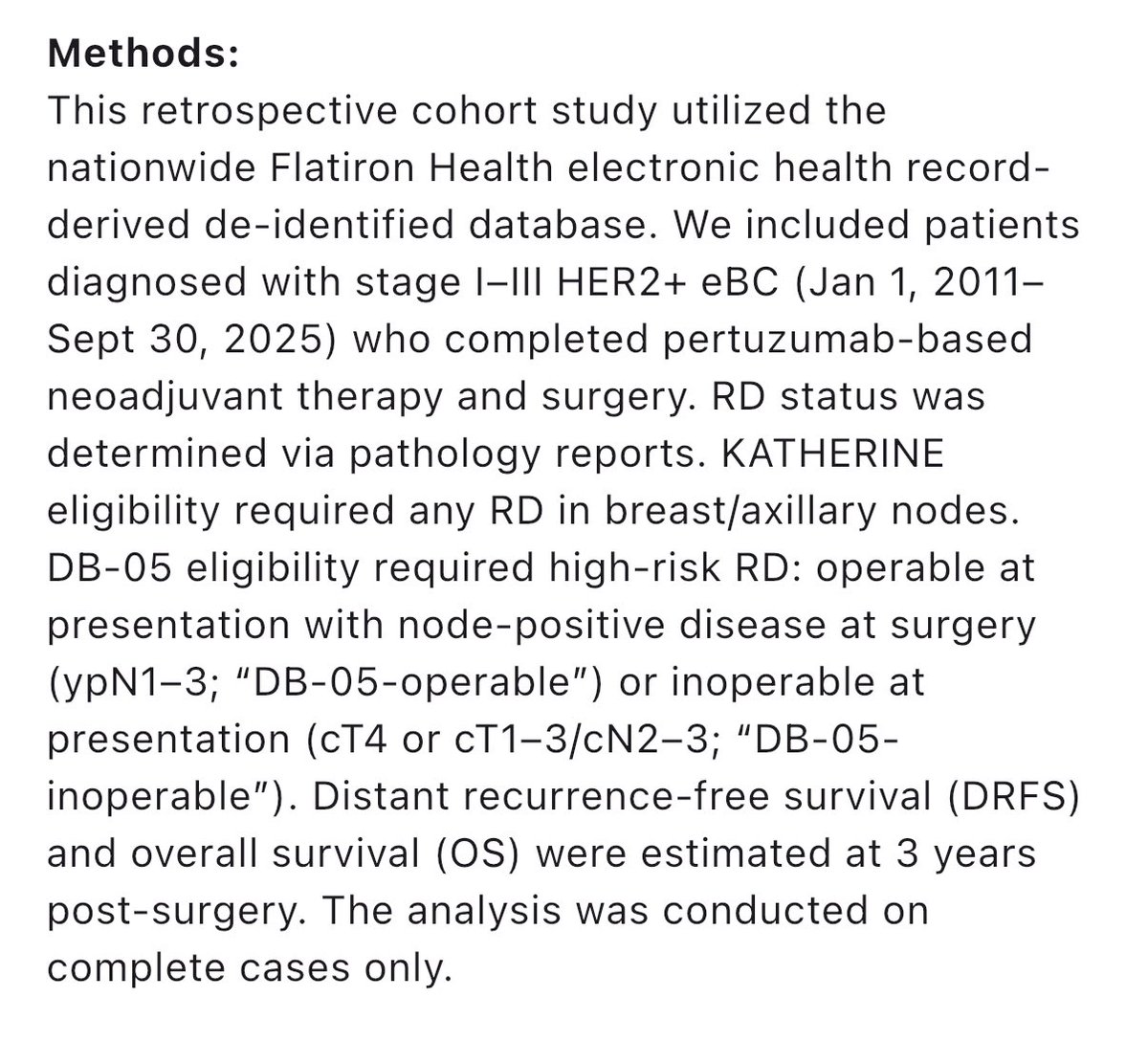
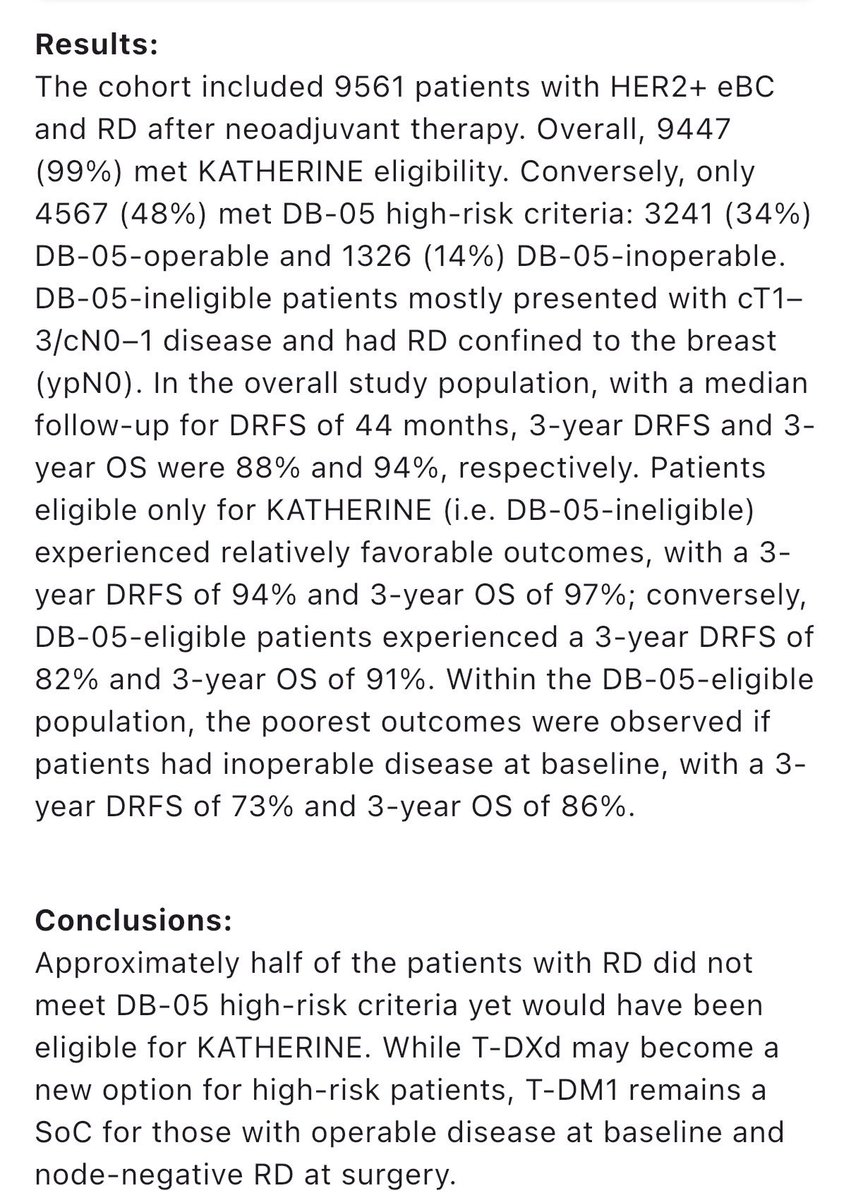
May 28

Adjuvant T-DXd is approved for pts with HER2 BC and high-risk RD by DB05 criteria. What about pts with lower risk RD? We looked at ~10.000 pts in Flatiron, finding that 52% have low-risk RD, with 3yr DRFS 94%, suggesting that T-DM1 remains an adequate SoC for them. #ASCO26 Ab545


1
2
7
1,051