
Upper Extremity Orthopedic Surgeon Follow @BadiaHand on IG Author #HealthcareFromTheTrenches Amazon Best Seller
Joined April 2009
- Tweets 3,740
- Following 1,549
- Followers 2,462
- Likes 449
465 Photos and videos




Alejandro Badia, MD retweeted

May 19
Its structural. Put in 12-15 yrs of your life to find out there is no pot of gold at the end of the rainbow. Middlemen and beaurcracy destroyed the incentives of those who actually do the work.
1
3
35
1,175
Alejandro Badia, MD retweeted

May 21
Just built our latest directory profile for an orthopedic surgeon specializing in arthritis and joint replacement. He serves as the Maria Manetti Shrem Endowed Professor and Chief Technology Officer in the Department of Orthopaedic Surgery at the University of California, San Francisco. At UCSF, he leads innovation at the intersection of medicine and technology.
Take a look at who he is. We'll be welcoming him into our new Sports Medicine series, hosted by @drbadia, and look forward to hearing his takes.
#medortho #medtwitter
doctorsonsocialmedia.com/ste… via @SoMeDocs
1
2
219
Alejandro Badia, MD retweeted
Healthcare costs keep rising, and it’s affecting how systems are funded and managed. Many people are feeling the pressure of expensive care and limited access.
This video is for educational purposes only and is NOT medical advice.
#Healthcare #HealthPolic
1
1
4
421

May 5
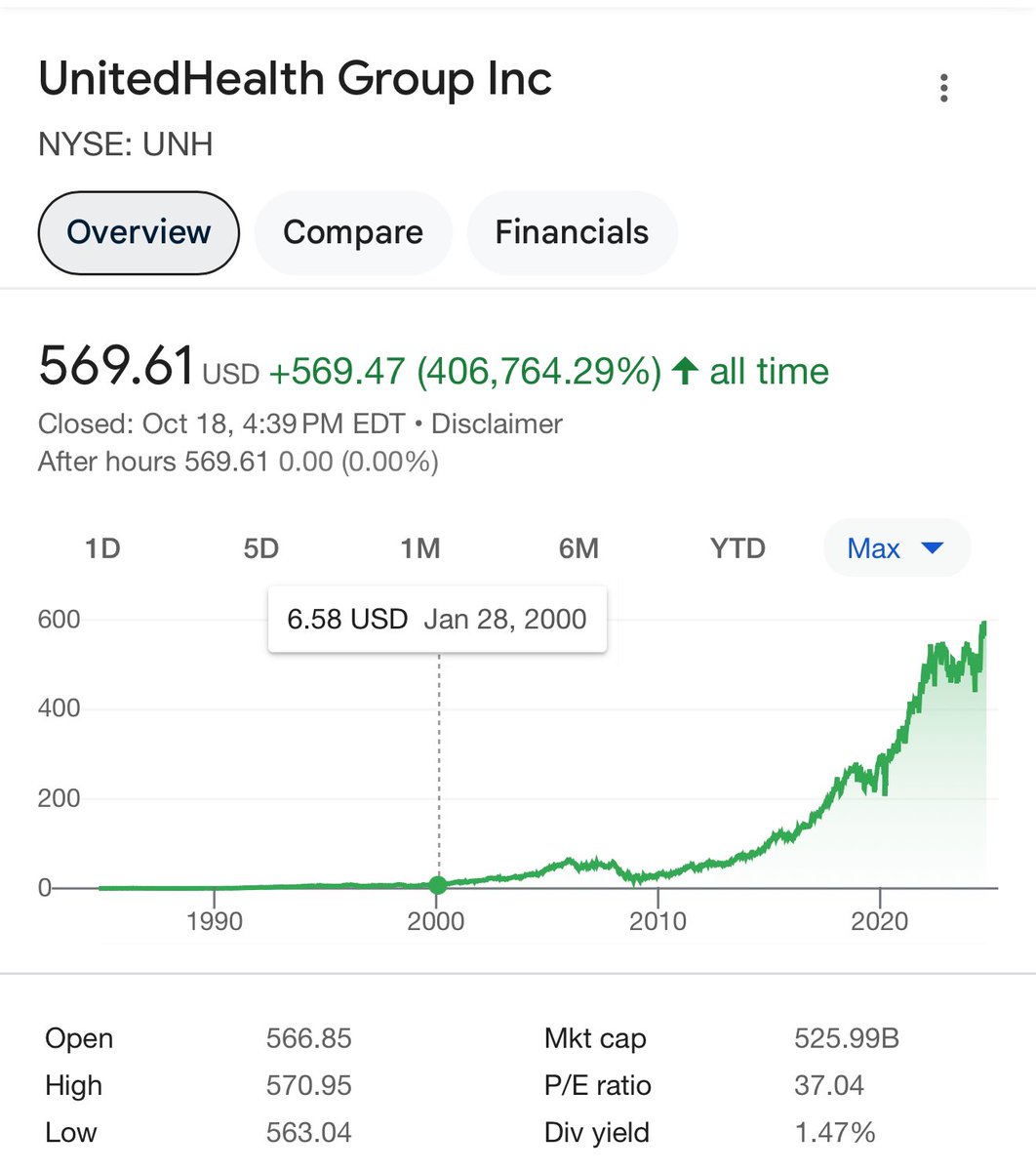
Nothing to add here. Take 32 seconds and look at the figures below and then tell me why healthcare
18 Oct 2024

Physician conversion factors:
2000: $36.6173
2003: $36.7856
2006: $37.8975
2009: $36.0666
2012: $34.0376
2015: $35.7547
2018: $35.9996
2021: $34.8931
2024: $32.7442
UHC stock up 8,556%
Insurance premiums up 342%
Inflation up 86%
Physician pay down 10%
We should keep cutting physician pay so families have more money in their pockets through reduced costs and reduced premiums based on the last 25 years of experience.
1
2
103
Apr 26
The Truth About Medical Authorizations & The US Healthcare System youtu.be/ccoPo12-PTU?si=t9sh… via @YouTube
Excerpt from @BooksandBooks talk on 2020 book #HealthcareFromTheTrenches
47
Alejandro Badia, MD retweeted

Apr 22
We got another one guys. Another colleague going private. 🙌 There is a shift. It’s happening.
Apr 21

Some people see construction.
I see freedom.
I see the future home of patient-first care.
Left the system to create something better: care focused on patients, not quotas.
Helping build it from the ground up.
Doors opening here in 2-3 weeks.
New office. Same flip-flops.
#Urology #SmallBusiness #Entrepreneur #LebanonPA


1
1
9
1,490
Alejandro Badia, MD retweeted

Apr 14
We move forward by moving backward. We need to return to physician-led care and remove all the middlemen that add no value.
We allow for physician innovation and competition.
This means eliminating the Stark laws and section 6001 of the ACA.
Allow physicians to own hospitals and to innovate.
We need true price transparency, and we need patients to purchase most of their care.
Health insurance should be limited to catastrophic events.
Patients should pay cash for:
• Physician's office visists
• Labs
• Drugs
• Imaging
• Procedures
• Urgent Care visits
This will allow a market to develop, driving down prices and improving quality.
Complex care drives most of our budget, and this should be done at centers of excellence.
We need longitudinal outcomes and price data.
AI navigators can assist HR and patients in navigating this world.
Eliminate middlemen like the rent-seekers they are.
Apr 14

I want to reflect on the broken culture of innovation in U.S. healthcare delivery—and its nefarious impact on the system.
We declare success prematurely.
We obscure failure.
And we move on without inquiry.
Within the delivery system, the same organizations whose basic and clinical researchers perform rigorous, thoughtfully designed controlled trials of medicines will tout the success of delivery and financing innovation without requisite evaluation.
In the broader innovation ecosystem, we too casually equate funding, valuations, and transactions with success—and we too often elevate and declare success without applying appropriate skepticism.
Many believe this culture of salesmanship and hucksterism is harmless.
But on the other side of it are patients whose care is not getting better and an industry with misplaced conviction about progress when there is none.
I’ve seen this firsthand throughout my career.
To make this less abstract, I’ll focus on my own area of work over the last decade: leading and operating Medicare Advantage plans and care delivery organizations.
It is a sector that has birthed many venture capital darlings.
But with the benefit of hindsight, many of those companies had clinical outcomes that were, at best, thin—
And whose primary innovation was exploiting arbitrage opportunities in risk adjustment.
And yet, in retrospect, these “innovators” were platformed.
They were celebrated on the stages of major national forums.
And while Medicare Advantage is now a space where some of these behaviors are more widely understood, it is not unique to Medicare Advantage.
Rather, some of the distortions we see there are a window into a broader cultural problem.
One that, in a different form, was on display in the case of Elizabeth Holmes and Theranos.
We might like to believe that was an exceptional story in exceptional circumstances.
I don’t.
I think we have many Theranoses among us—just less visible, and more socially accepted.
Why?
I believe there are two root cause.
First, expert and funding bias.
We believe that startups revered and validated by experts are worthy of celebration.
And if they are richly funded, we assume they have been appropriately vetted.
Commercial success—often driven by relationships and the favor economy—is prematurely equated to clinical success.
Second, optimism bias.
We have such a strong desire to believe that things are getting better that the first hint of progress is met with celebration—rather than the skepticism we typically reserve for results that seem too good to be true.
This is how many of us have convinced ourselves that American healthcare delivery is improving—while most consumers, patients, and clinicians tell us otherwise every single day.
So how do we move forward?
2
4
22
1,127
Alejandro Badia, MD retweeted
Apr 12
If the private practice doctors hadn't admitted patients to the hospital or used the OR, the hospital would have been out of business.
We should have always demanded compensation for on-call duty.
Apr 12

Call. At the hospital used to be the deal with devil for privileges of private practice community docs to admit and use the ORs. If that day is done and is still expected then call needs to be a paid part of the compensation package.
9
5
61
7,748
Alejandro Badia, MD retweeted
Apr 11
Very well said!

With all due respect find me a profession that is working for 70 percent less than 20 years ago inflation adjusted, that does what docs do, with the risk, liability, responsibility, training and expertise that docs provide. We all agree there’s lots of fraud.
1
10
982
Alejandro Badia, MD retweeted

All the money is going to admin. They are rushing doctors and squeezing their pay. Admin and the CEO get the wealth. Drs do all the work and are more educated. The system has taken over. It’s upside down.
1
39
Alejandro Badia, MD retweeted

Egregious, profit-driven practices employed by insurance companies are wreaking havoc on American healthcare. I’m proud to fight for what’s right in Congress.
Patients must come before profit!
12
10
50
2,570
Alejandro Badia, MD retweeted

Every private practice doctor that can and has the power to drop contracts, need to start dumping insurance companies and employed docs need to go be independent, that is the only way we get our profession back.

WOW 🚨 Delta Dental is considered a nonprofit but the CEO skyrocketed her pay from $4.5 million per year all the way to $48 million over 4 years
That’s $1 million dollars per month pay for one employee as a nonprofit
“Delta Dental is considered a non-profit, and as such you can be their taxes online. So I got curious in their 2014 filing, the IRS requests for the organization's top accomplishments.
Delta Dental reported that over 95% of claims electronic, online and paper were processed without any manual intervention. That means when your care is denied, there is less than 1 in 10 chance a human reviewed it
— That same year, Delta dished out up to a 30% pay cut on the care that doctors deliver, and for a decade, they did not raise what they pay for your dental care by a single penny.
Meanwhile, their CEO's salary skyrocketed. She went from 4.5 to $15 million a year. From 2014 to 2018, she made off with almost $48 million before leaving her position. That's a million dollars a month. Must be nice. And she's not even a clinician. She's a CPA.
You don't have to be an accountant to do the math. Dr. Pay cuts stagnant reimbursements. They were never about saving patients money on premiums.”
23
75
443
33,608
Alejandro Badia, MD retweeted
Today, I went to the House floor to shed light on the egregious, profit-driven practices that health insurance companies are using to wreak havoc on American patients.
Patients must come first.
14
23
73
11,051
Alejandro Badia, MD retweeted

Mar 21
Des and Nurses are underpaid. Independent doctors are getting ripped off to the point of barely getting paid after fees
The biggest insurance companies are awful for beneficiaries and for employers.
One example ?
What good is insurance if patients can't afford their deductible?
Mar 20

If you're thinking about healthcare spending in the US, one fact worth noting
About 9% of healthcare spending goes to physician compensation
Another 9% goes to nurses
Yes, doctors and nurses get paid more in the US than they do in other countries and yes, a small proportion of physicians really do get paid a lot
But I've never thought we're going to solve our healthcare spending by going after physician and nursing salaries
Not enough there -- and slashing physician or nursing compensation would be a great way to demoralize the core of the US healthcare workforce
94
86
813
185,373
Mar 22
PLEASE join this group if you are an independent private practice physician. Those who are salaried or directed by private equity should reach out if you decide to join us. #takemedicineback #healthcarerevolution #HealthcareFromTheTrenches
Mar 21

If you are an independent physician, we would like to invite you to list your practice on our new website. It’s completely FREE.
We want to build a network of independent physicians across the US, where patients can connect with you. The only way we will change healthcare, is if independent physicians start leading. We believe this is the first step. Please share this link and invite your colleagues. 😃
theprivatedocs.com/

1
1
3
410
Alejandro Badia, MD retweeted
Mar 21
If you are an independent physician, we would like to invite you to list your practice on our new website. It’s completely FREE.
We want to build a network of independent physicians across the US, where patients can connect with you. The only way we will change healthcare, is if independent physicians start leading. We believe this is the first step. Please share this link and invite your colleagues. 😃
theprivatedocs.com/
11
33
121
6,819
Mar 22
If I tried to make medical decisions about someone I had never evaluated, never spoken with, and barely reviewed records on, I could risk losing my medical license. — article written by Daniel Paull M.D. doctorsonsocialmedia.com/pri… via @somedocs
3
4
412
Mar 22
From the article: If insurance companies are confident enough to overrule physicians, then perhaps it is time for them to do what the rest of us in medicine must do. Put their money where their mouth is. — Daniel Paull doctorsonsocialmedia.com/pri… via @somedocs
Pretty clear concept- why do you think the public can’t even physicians continue to tolerate this?
3
7
860
Alejandro Badia, MD retweeted

Mar 19
Your doctor went to medical school for 12 years. The person denying your claim went through a two-week training module.
330
11,941
101,574
946,134