
consultant in ICM&anaesth.; POCUS: FAMUS FUSIC supervisor, FUSIC heart, CACTUS lung mentor; regional anaesth.; airway lead; retired ATLS/ETC/ALS/GIC instructor
Joined November 2018
- Tweets 3,336
- Following 280
- Followers 530
- Likes 8,990
559 Photos and videos











Pinned Tweet

2 Sep 2019
some says #POCUS answers (to the basic #FICE #CUSIC #FAMUS questions) are binary: yes/no.
but imo there must be 3:
- yes
- no
- i don’t know
3rd is not cool, but absolutely valid and most importantly: safe
31 Aug 2019

We need to teach how doubt is not to be feared but welcomed. It's OK to say, "I don't know."
2
13
36
Mátyás Andorka retweeted

Jun 11
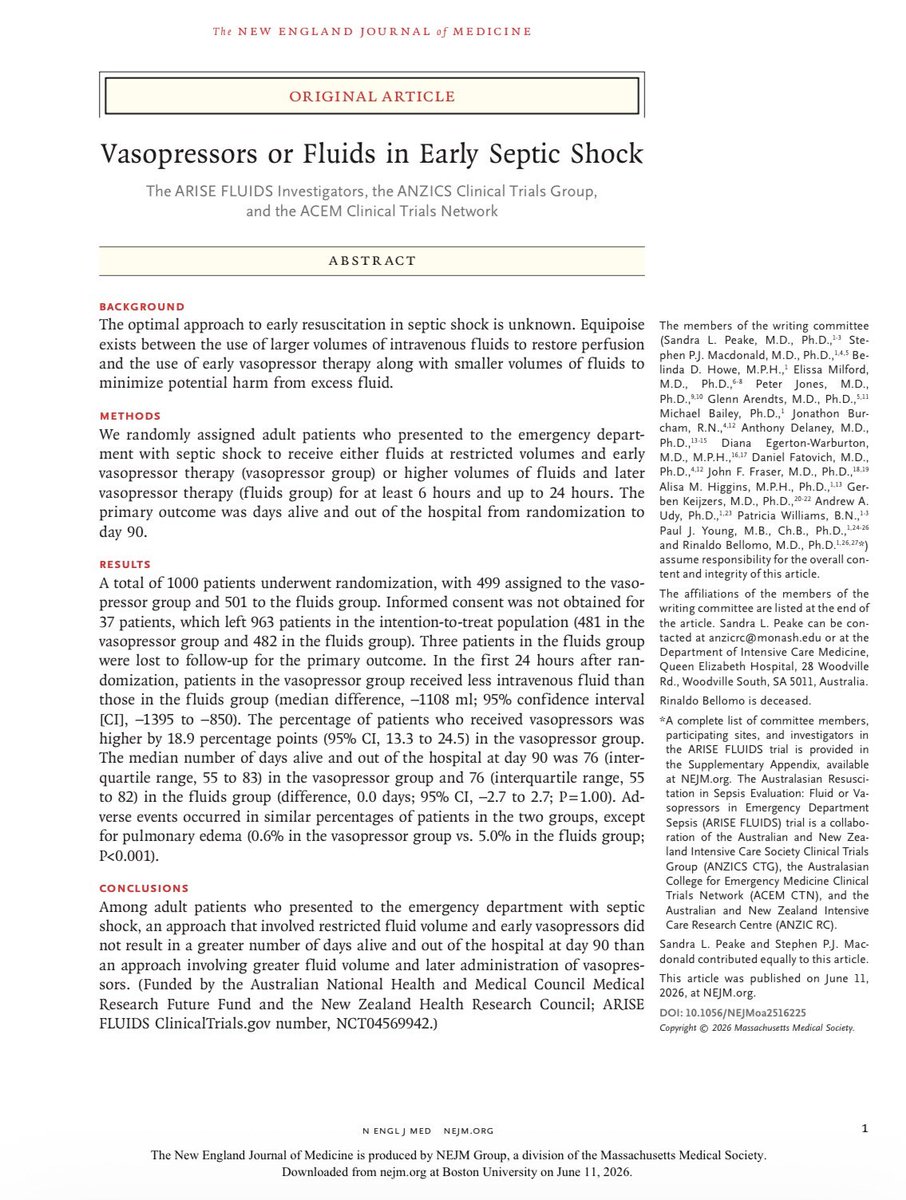
Estudio ARISE FLUIDS de Choque Séptico
Los famosísimos 30 ml/kg de fluidos IV 💦
Versus
Vasopresor Temprano 💉
🟰 Ninguna de las 2 estrategias disminuyó la mortalidad a 90 días
Los pacientes de fluidos a 30 ml/kg (29, realmente) tuvieron:
💦 🫁 más edema pulmonar (5% vs 0.6% en el grupo de vasopresor)
⏱️ más tiempo en UCI
💉 más tiempo con vasopresor (paradójicamente)
A ver si con esto ya cambian las recomendaciones del Surviving Sepsis y quitan los chingados 30 ml/kg de agua…
DOI: 10.1056/NEJMoa2516225
8
123
443
43,183
Mátyás Andorka retweeted

From the first International Consensus Conference on Lung Ultrasound in 2012 to the updated document: 13 years of scientific growth, new evidence, and multidisciplinary collaboration.
#LungUltrasound #PoCUS #CriticalCare #EmergencyMedicine
link.springer.com/10.1007/s0…
15
13
835
Mátyás Andorka retweeted

Jun 11
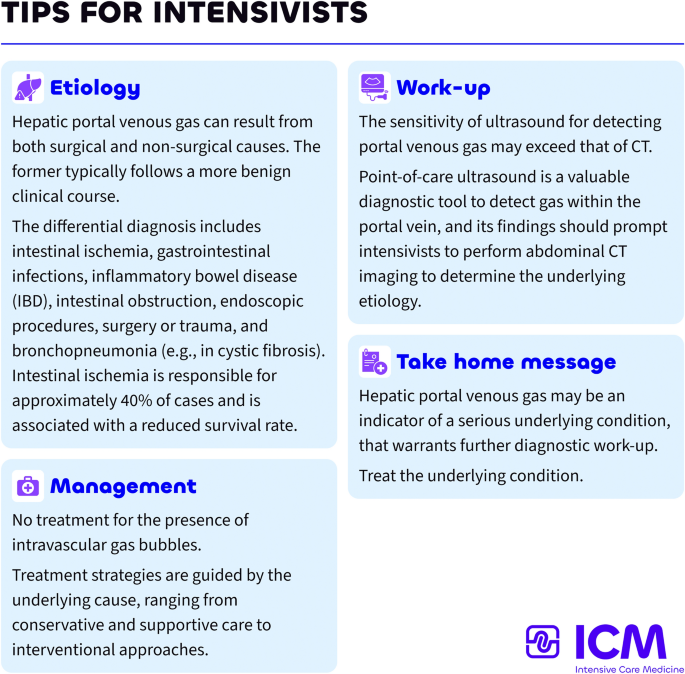
Non-occlusive mesenteric ischemia (NOMI) was diagnosed, and partial bowel resection was performed.

1
1
133
Jun 9
one to keep an eye on!
Jun 9

I’ve started a Substack: The Dependent Variable.
X is great for short-form discussion, but it’s not ideal for building a coherent archive.
This will be the home for longer-form writing on cardiovascular physiology, haemodynamics, fluids, shock, ultrasound and critical care reasoning. All in one place, easier to follow and return to.
First post: open.substack.com/pub/icmtea…
1
95
Mátyás Andorka retweeted

🤓ICU POCUS should not be learned as “views.” It should be learned as progressive clinical responsibility.
Recent PubMed indexed guidance supports critical care ultrasonography as a bedside tool for septic shock, acute dyspnea or respiratory failure, volume management, and cardiogenic shock (Díaz-Gómez et al., 2025). A 2024 meta analysis also suggests POCUS guided resuscitation may reduce 28 day mortality, vasoactive drug duration, and renal replacement therapy use, although evidence quality remains variable (Basmaji et al., 2024).
A practical ICU curriculum could be divided into levels.
Before entering to ICU: know machine handling, probe selection, image optimization, lung sliding, pleural effusion, basic IVC, free fluid, bladder, DVT compression, FAST and ultrasound guided vascular access.
ICU resident: add structured lung ultrasound, focused cardiac ultrasound, LV/RV function, pericardial effusion, shock phenotyping, fluid tolerance, congestion, pneumothorax, diaphragm ultrasound, ONSD and procedural guidance.
ICU specialist: integrate heart lung vein ultrasound into decisions: fluids, vasopressors, inotropes, ventilation, PEEP, weaning, RV failure, tamponade, pulmonary embolism, TCD, ARDS, and cardiorenal congestion.
Specialized ICU: advanced echocardiography, TEE, strain, advanced TCD, complex valvular disease, mechanical circulatory support, ECMO cannulation and troubleshooting, and quality assurance.
The danger is not using ultrasound. The danger is using ultrasound without competence, supervision, documentation, and clinical integration.
Best practice documents emphasize structured training, competency assessment, image archiving, quality assurance, and local governance (Oto et al., 2024; Patrawalla et al., 2025).
The key question is not:
“Can you obtain the image?”
It is:
Can you acquire it, interpret it, and safely change management because of it?
#ICU #CriticalCare #POCUS #Ultrasound #FOCUS #LungUltrasound #Hemodynamics #Shock #MedicalEducation #PatientSafety
References 📚
Basmaji, J., et al. (2024). The impact of point-of-care ultrasound-guided resuscitation on clinical outcomes in critically ill patients: A systematic review and meta-analysis. Critical Care Medicine. doi.org/10.1097/CCM.00000000…
Díaz-Gómez, J. L., Sharif, S., Ablordeppey, E., et al. (2025). Society of Critical Care Medicine guidelines on adult critical care ultrasonography: Focused update 2024. Critical Care Medicine, 53(2), e447–e458. doi.org/10.1097/CCM.00000000…
Oto, B., et al. (2024). Best practices for point of care ultrasound. Ultrasound Journal, 16, 15. doi.org/10.1186/s13089-024-0…
Patrawalla, P., et al. (2025). Best practices for a competency-based curriculum in critical care ultrasonography. Chest. doi.org/10.1016/j.chest.2025…

ALT
11
35
2,249
Mátyás Andorka retweeted

Jun 8

1
5
13
734
Jun 8

🧠 Are We Missing Half of the Brain's Circulation?
For decades, neurocritical care has focused primarily on arterial flow.
We monitor cerebral perfusion, vasospasm, autoregulation, pulsatility indices, and intracranial pressure. Yet one critical component of intracranial hemodynamics remains largely overlooked:
Cerebral venous outflow.
A recent review in Diagnostics argues that Transcranial Color Doppler (TCCD) should evolve beyond being merely the "stethoscope of the brain" for arterial circulation and begin incorporating systematic assessment of cerebral venous drainage.
The authors highlight a simple but important physiological concept:
🩸 Intracranial hypertension is not only a problem of arterial inflow.
It may also be a problem of impaired venous outflow.
Mechanical ventilation, elevated PEEP, hypercapnia, increased intra-abdominal pressure, Trendelenburg positioning, cardiac tamponade, pulmonary hypertension, large-bore jugular catheters, and venous obstruction can all impair cerebral venous drainage and contribute to cerebral congestion.
Using venous TCCD combined with internal jugular vein ultrasound, clinicians may be able to detect cerebral venous congestion before conventional markers such as optic nerve sheath diameter (ONSD) enlargement or arterial Doppler changes become evident.
Particularly interesting for intensivists and anesthesiologists, the review presents clinical examples where:
🔹 Mechanical ventilation reduced Rosenthal vein flow despite stable arterial Doppler findings.
🔹 Large-bore central venous catheters further impaired cerebral venous drainage.
🔹 Hemodynamically significant pericardial effusion produced profound venous congestion detectable by ultrasound before definitive diagnosis.
🔹 Pneumoperitoneum and Trendelenburg positioning increased jugular venous congestion during surgery.
The key message is not that venous TCCD replaces current neuromonitoring tools.
Rather, it may provide an additional physiological layer that helps explain why some patients develop intracranial hypertension despite apparently acceptable arterial parameters.
As critical care increasingly moves toward physiology-guided management, perhaps the next frontier is understanding not only how blood enters the brain, but also how it leaves it.
Question for the neurocritical care and perioperative community:
Do you routinely consider cerebral venous drainage when adjusting PEEP, patient positioning, pneumoperitoneum pressures, or central venous access strategies?
Reference📚
Bianchini A, Vitale G, Melegari G, et al. Transcranial Color Doppler for Assessing Cerebral Venous Outflow in Critically Ill and Surgical Patients. Diagnostics. 2026;16:289.
doi.org/10.3390/diagnostics1…
#NeurocriticalCare #POCUS #TCD #TCCD #CriticalCare #IntensiveCare #Anesthesiology #NeuroMonitoring #Ultrasound #MechanicalVentilation #ICP #BrainInjury #CriticalCareMedicine #FOAMed #MedEd

ALT
2
2
532
Mátyás Andorka retweeted
🧠 Are We Missing Half of the Brain's Circulation?
For decades, neurocritical care has focused primarily on arterial flow.
We monitor cerebral perfusion, vasospasm, autoregulation, pulsatility indices, and intracranial pressure. Yet one critical component of intracranial hemodynamics remains largely overlooked:
Cerebral venous outflow.
A recent review in Diagnostics argues that Transcranial Color Doppler (TCCD) should evolve beyond being merely the "stethoscope of the brain" for arterial circulation and begin incorporating systematic assessment of cerebral venous drainage.
The authors highlight a simple but important physiological concept:
🩸 Intracranial hypertension is not only a problem of arterial inflow.
It may also be a problem of impaired venous outflow.
Mechanical ventilation, elevated PEEP, hypercapnia, increased intra-abdominal pressure, Trendelenburg positioning, cardiac tamponade, pulmonary hypertension, large-bore jugular catheters, and venous obstruction can all impair cerebral venous drainage and contribute to cerebral congestion.
Using venous TCCD combined with internal jugular vein ultrasound, clinicians may be able to detect cerebral venous congestion before conventional markers such as optic nerve sheath diameter (ONSD) enlargement or arterial Doppler changes become evident.
Particularly interesting for intensivists and anesthesiologists, the review presents clinical examples where:
🔹 Mechanical ventilation reduced Rosenthal vein flow despite stable arterial Doppler findings.
🔹 Large-bore central venous catheters further impaired cerebral venous drainage.
🔹 Hemodynamically significant pericardial effusion produced profound venous congestion detectable by ultrasound before definitive diagnosis.
🔹 Pneumoperitoneum and Trendelenburg positioning increased jugular venous congestion during surgery.
The key message is not that venous TCCD replaces current neuromonitoring tools.
Rather, it may provide an additional physiological layer that helps explain why some patients develop intracranial hypertension despite apparently acceptable arterial parameters.
As critical care increasingly moves toward physiology-guided management, perhaps the next frontier is understanding not only how blood enters the brain, but also how it leaves it.
Question for the neurocritical care and perioperative community:
Do you routinely consider cerebral venous drainage when adjusting PEEP, patient positioning, pneumoperitoneum pressures, or central venous access strategies?
Reference📚
Bianchini A, Vitale G, Melegari G, et al. Transcranial Color Doppler for Assessing Cerebral Venous Outflow in Critically Ill and Surgical Patients. Diagnostics. 2026;16:289.
doi.org/10.3390/diagnostics1…
#NeurocriticalCare #POCUS #TCD #TCCD #CriticalCare #IntensiveCare #Anesthesiology #NeuroMonitoring #Ultrasound #MechanicalVentilation #ICP #BrainInjury #CriticalCareMedicine #FOAMed #MedEd
ALT
1
20
56
3,211
Mátyás Andorka retweeted
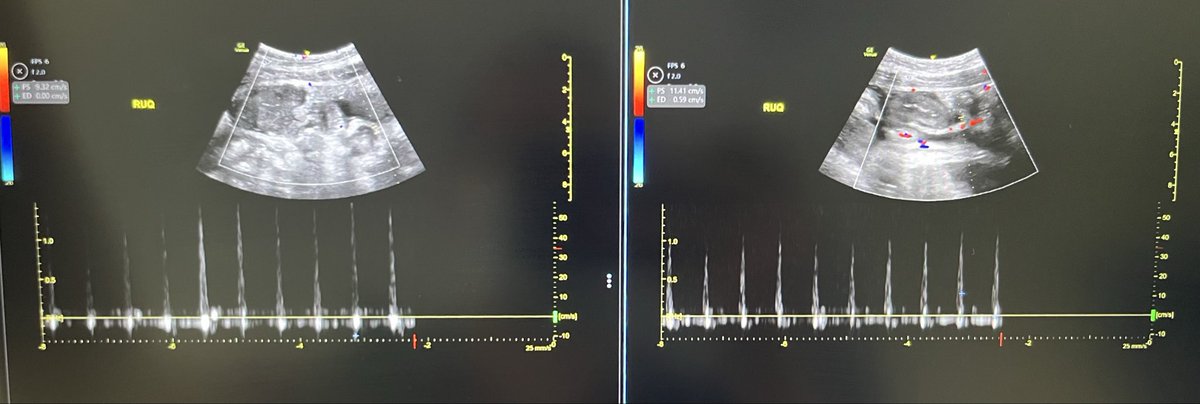
💧 Fluid Responsiveness ≠ Fluid Tolerance
For years, critical care clinicians have focused on a fundamental question:
Will this patient increase cardiac output if I give fluids?
A new multicentre study from France and China suggests we may need to ask a second question:
What price will the patient pay for that fluid?
In this observational study of 64 critically ill patients receiving a standardized 500 mL fluid challenge, investigators evaluated not only cardiac index (CI), but also venous congestion using VExUS and pulmonary congestion using extravascular lung water (EVLWI).
The findings are striking.
Before fluid administration, venous congestion could coexist with fluid responsiveness. In fact, many patients remained preload responsive despite already demonstrating evidence of systemic venous congestion.
However, what happened after fluid administration was even more important.
Among fluid responders:
✅ Cardiac index increased significantly
✅ Venous congestion remained largely stable
✅ Only 5% experienced worsening VExUS grade
✅ Lung water remained relatively unchanged
Among fluid non-responders:
❌ Cardiac output barely changed
❌ Venous congestion worsened dramatically
❌ VExUS deterioration occurred in 73%
❌ EVLWI increased significantly
❌ Congestion became evident across hepatic, portal, and renal venous territories
Perhaps the most important physiological message is this:
When the heart cannot convert preload into flow, the fluid has to go somewhere.
And where it goes is congestion.
The study also found a strong correlation between CVP and VExUS, suggesting that while advanced ultrasound provides valuable organ-level information, a carefully interpreted CVP may still remain a useful bedside marker of right-sided congestion.
The ARDS subgroup provides another important lesson.
Even fluid-responsive ARDS patients accumulated more extravascular lung water after fluid administration than non-ARDS patients, highlighting the role of pulmonary permeability in determining fluid tolerance.
This study reinforces a concept that is increasingly central to modern hemodynamic management:
The goal is not simply to identify fluid responsiveness.
The goal is to identify patients who are both:
✔ Fluid responsive
✔ Fluid tolerant
A fluid challenge that increases congestion without increasing flow is not resuscitation.
It is fluid accumulation.
The future of hemodynamic management may lie at the intersection of:
• Fluid responsiveness
• Venous congestion assessment
• Pulmonary permeability
• Organ-specific fluid tolerance
Because the best fluid is not the one that can be given.
It is the one that provides benefit without causing harm.
Reference , 📚
Si X, Critical Care. 2026;30:35.
ALT
2
67
195
12,779
Mátyás Andorka retweeted

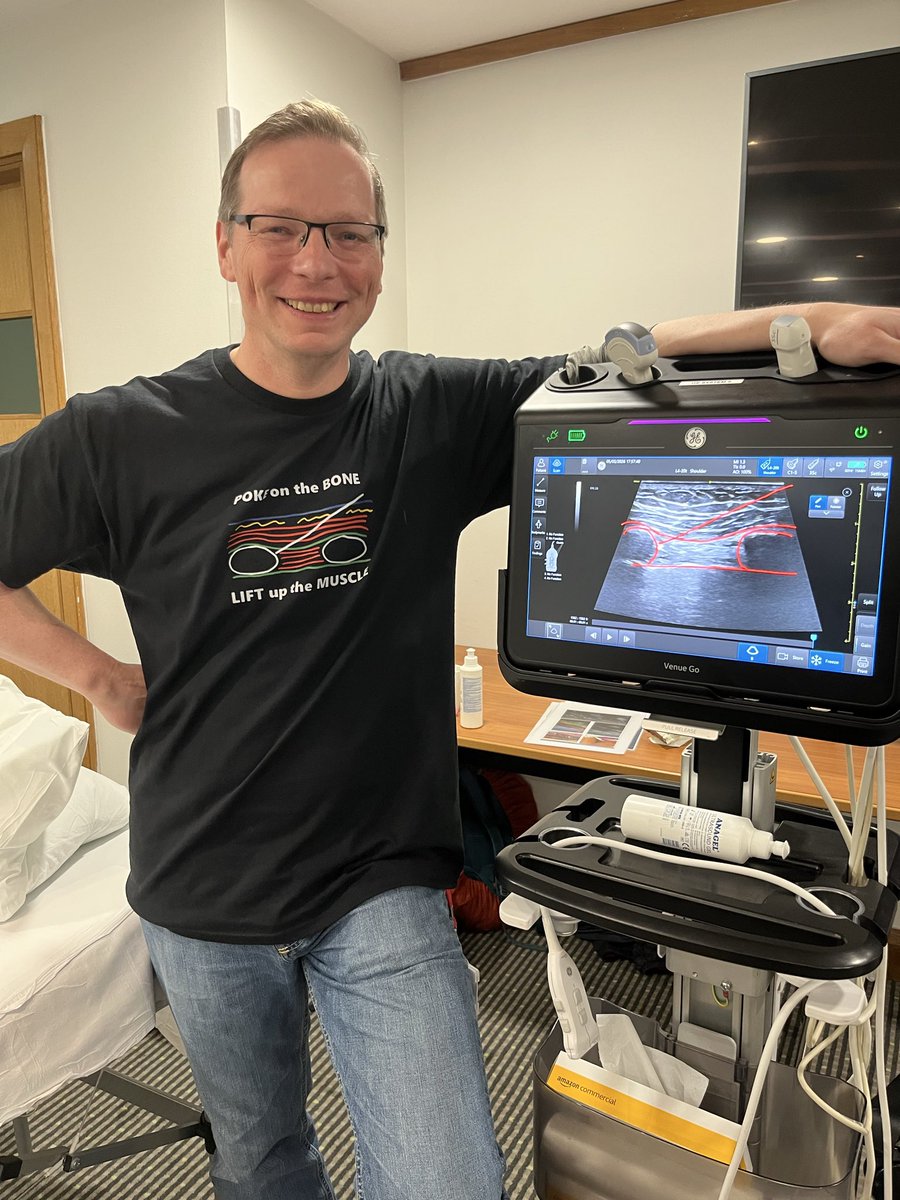
What's on this summer? Well, definitely some barbecuing!
But also so amazing ultrasound eduction.
Come and join the pre-congress workshops at #SOA26 in Birmingham.
We have Heart🫀 and HD, lungs 🫁and blocks💉.
Check them out: ics.ac.uk/events/soa26/pre-c…
See you there!
1
6
7
1,184
Mátyás Andorka retweeted

May 14
Airway Triage Debate: Today, a debate with an anesthesiologist [@airwaymxacademy] on the use of his airway triage app and whether it is applicable to resus airways...
emcrit.org/425
1
9
13
4,753
Mátyás Andorka retweeted

Jun 1
6
90
302
63,116
Mátyás Andorka retweeted

May Airway of the Month:
kumc.hosted.panopto.com/Pano…
the tube misses by a millimeter — but the problem may have started before tube passage.
This month: suboptimal VL view, arytenoid engagement, and the key reset:
Back up → suction → optimize laryngoscopy → reattempt.
#FOAMed #Airway #EmergencyMedicine
2
5
12
1,029
Mátyás Andorka retweeted

May 29
How the blood goes round sounds simple. It isn’t.
• Pressure does not drive flow.
• Preload is not a driver of cardiac output.
• Equations and graphs describe a system without explaining what controls it.
• Flow is governed by two constraints: delivery and acceptance.
Now free to read for a limited time:
Energy, flow and pressure in the cardiovascular system: a narrative review of how the circulation works
Link in reply 👇
doi.org/10.1111/anae.doi.o….
3
21
60
4,483
Mátyás Andorka retweeted
🫀POCUS is no longer just a bedside imaging tool.
It is becoming real time physiological intelligence.
This excellent 2026 review highlights how modern POCUS is expanding into:
• ultrasound guided regional anesthesia
• shock and cardiac arrest management
• AI assisted imaging
• advanced diagnostics
• governance and medicolegal practice
Some of the most provocative concepts: • “Occult VF” detectable only on echocardiography during cardiac arrest
• Ultrasound guided CPR compression positioning
• AI assisted lung ultrasound acquisition by nonexperts
• Handheld devices approaching cart based diagnostic performance
One important medicolegal message: several lawsuits involved failure to perform POCUS when clinically indicated.
The future of emergency and critical care medicine will likely depend on clinicians capable of integrating: physiology imaging AI rapid bedside decision making.
POCUS is not anymore an “optional skill” but “core clinical infrastructure.”
Mani N, Rao S, Kim DJ. Point-of-care ultrasound in the modern era of emergency medicine: a narrative review of the recent literature. Curr Opin Crit Care. 2026. doi:10.1097/MCC.0000000000001358

ALT
1
49
164
8,400
Mátyás Andorka retweeted
🫁COPD ventilation is not ARDS ventilation.
In acute COPD exacerbation, the enemy is often not alveolar collapse. It is expiratory flow limitation, dynamic hyperinflation, intrinsic PEEP, respiratory muscle overload, and CO₂ retention.
Recent PubMed indexed literature from 2023 to 2026 reinforces a practical message: in acute hypercapnic COPD exacerbation, NIV remains the first line ventilatory strategy when there is respiratory acidosis, increased work of breathing, and no immediate contraindication (Farmer et al., 2024; Mein & Ferrera, 2025). HFNC may be useful in selected patients, especially when NIV is not tolerated, but recent meta analysis suggests higher treatment failure and crossover to NIV, so it should not replace NIV as default support in acidotic AECOPD (Qin et al., 2025).
The invasive ventilation strategy is different from hypoxemic lung disease.
For the intubated COPD patient, the goal is not to normalize PaCO₂ quickly. The goal is to reduce dynamic hyperinflation.
That means:
Low respiratory rate
Long expiratory time
Modest tidal volume, usually around 6 to 8 mL/kg predicted body weight
Avoidance of excessive minute ventilation
Permissive hypercapnia when pH is acceptable
Monitoring plateau pressure, driving pressure, auto PEEP, expiratory flow, and hemodynamics
PEEP is the controversial part.
External PEEP can help when the patient is spontaneously triggering, because it reduces the inspiratory threshold load caused by intrinsic PEEP. In this context, carefully applied external PEEP may improve synchrony, reduce work of breathing, and facilitate assisted ventilation (Jubran, 2024).
But in controlled ventilation without spontaneous effort, excessive external PEEP may worsen hyperinflation, raise plateau pressure, reduce venous return, increase RV afterload, and precipitate hypotension. Here, low PEEP or minimal PEEP may be safer unless oxygenation requires more support.
A practical bedside rule:
If the COPD patient is triggering and fighting auto PEEP, external PEEP may help.
If the COPD patient is passive, hypotensive, hyperinflated, and not oxygenation limited, high PEEP may harm.
The ventilator question is not:
“How much PEEP does COPD need?”
It is:
Is PEEP unloading the patient, or inflating the trap?
#COPD #CriticalCare #ICU #MechanicalVentilation #NIV #AutoPEEP #Hypercapnia #RespiratoryFailure #VentilatorManagement #IntensiveCare
References📚
*Farmer, M. J. S. Chest, 165(6), 1473–1483. doi.org/10.1016/j.chest.2024…
*Jubran, A. Current Opinion in Critical Care, 30(1), 89–96. doi.org/10.1097/MCC.00000000…
*Mein, S. A. CHEST Critical Care, 3(1), 100107. doi.org/10.1016/j.chstcc.202…
*Qin, J., Annals of Intensive Care, 15, 64. doi.org/10.1186/s13613-025-0…
2
28
74
3,809
Mátyás Andorka retweeted
May 26
Haemodynamic equations are useful. But they also mislead.
Take:
CO = HR × SV
CO ≈ (MAP − RAP) / SVR
Both are mathematically true. But they can make the variables they contain look like the controllers of output.
Often they are not.
In the intact circulation, these equations describe the resolved state of the system. They do not, by themselves, tell you what is supplying energy, what is constraining flow, or what is actually limiting output.
That is one of the central themes of our review:
Energy, flow and pressure in the cardiovascular system: a narrative review of how the circulation works.
doi.org/10.1111/anae.70238
10
95
295
18,609
May 25
We did it!!!
Completed the Vogalonga 2026 with our 3 boys! I am incredibly proud of them and my wife!
Thank you very much for all the donations for @SandcrossSchool .
justgiving.com/page/andorkas…
Also huge thanks for our tour leader Tamas Kakas! We’ll come again ;)
May 15

Fundraising for Friends of Sandcross Charity!
Our family of five will participate in a 30km kayaking regatta
We are raising funds for the boys’ school: @SandcrossSchool to improve their outdoor learning space.
Please consider supporting our goal!
Link in the next post:
2
105
Mátyás Andorka retweeted
🫀🤓Pressure does not move blood. Energy does.
This outstanding review challenges one of the most deeply rooted concepts in haemodynamic management: the idea that pressure variables are the primary drivers of circulation. Instead, the authors propose a physiology framework where the heart supplies energy, the vasculature defines constraints, and pressures merely reflect system state.
Several concepts deserve special attention for critical care clinicians:
• Mean systemic pressure does not “drive” flow
• Right atrial pressure is a dependent variable, not a therapeutic target
• Venous return depends on inflow acceptance and inlet impedance
• Raising pressure without improving flow may worsen congestion
• Shock should be interpreted as either impaired venous delivery or impaired cardiac acceptance
Clinically, this framework helps explain why:
• CVP-guided fluid loading often fails
• Vasopressors may normalize MAP without restoring perfusion
• Congestion can coexist with preserved arterial pressure
• Flow responsiveness matters more than static pressure targets
One of the strongest messages of the paper is simple but powerful:
“Pressure is not perfusion.”
For intensivists, anesthesiologists, and cardiogenic shock teams, this review is worth reading in full. It reconnects bedside haemodynamics with first-principles physiology.
Miller A, Anaesthesia. 2026. doi.org/10.1111/anae.70238

ALT
7
90
227
12,750