
🦀 Radiation Oncologist ⚛️ H.U.Badajoz / SBRT & SRS/ @oncoradioHUVM "Mors mortem superavit"
Joined December 2022
- Tweets 450
- Following 99
- Followers 81
- Likes 470
4 Photos and videos




Fco de Paula Titos retweeted

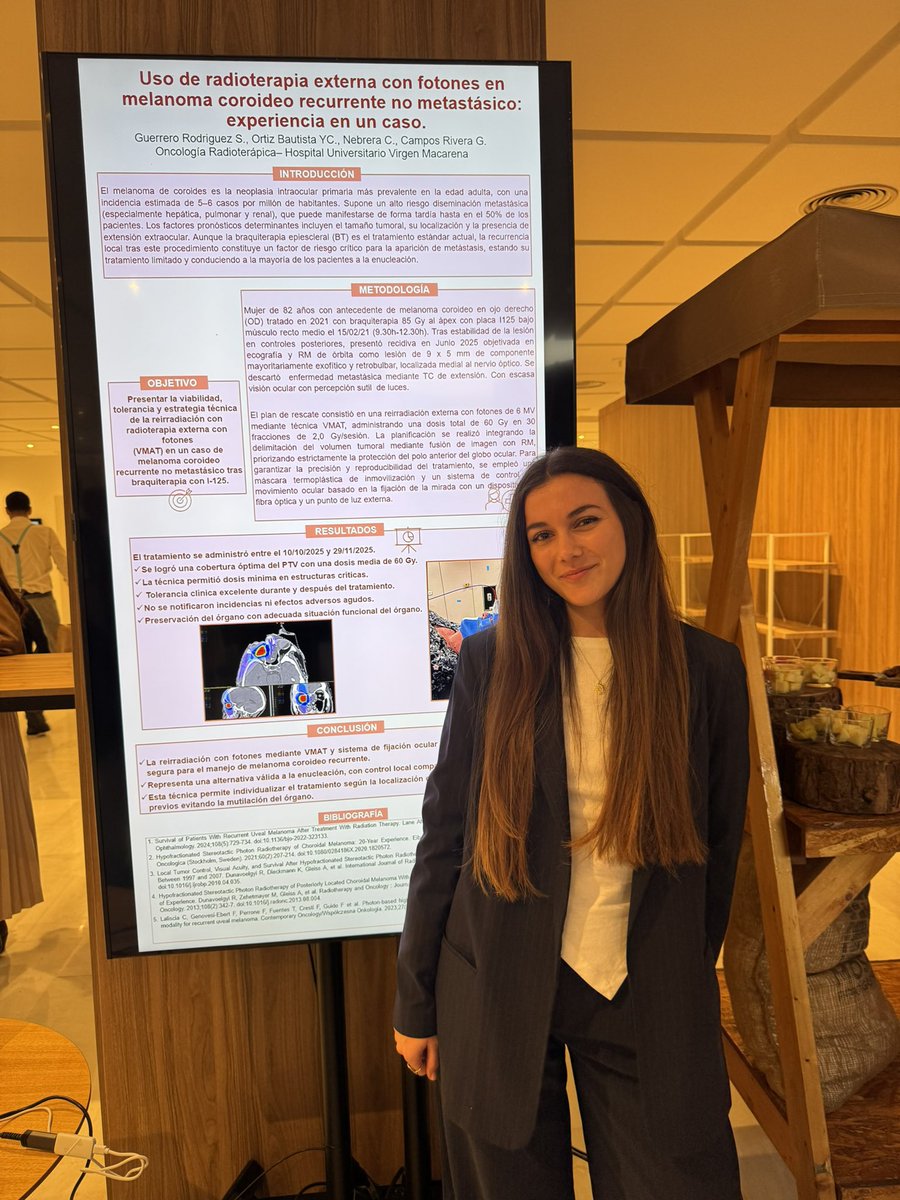
‼️Seguimos de congreso‼️
Compartimos nuestra partipación con diferentes ponencias y comunicaciones orales
Radioterapia de vanguardia ☢️
@HUVMacarena @AndaluzaSac


5
8
340
Fco de Paula Titos retweeted

Sentido homenaje a la Dra. Elena Montero en el Congreso de la Sociedad Andaluza de Cancerología. Alegría, vocación y legado imborrable. Siempre en nuestros corazones.
7
32
1,173
Fco de Paula Titos retweeted
Amplia representación de nuestro servicio en el XXIV Congreso Andaluz de Cancerología: la sociedad oncológica más antigua de España @AndaluzaSac
#radonc ☢️

5
8
368
Fco de Paula Titos retweeted
😎
Innovación, precisión y equidad: así aborda Badajoz el cáncer de pulmón. #lcsm share.google/KdYVcz9ClCmmW5y…
3
3
402
Fco de Paula Titos retweeted
‼️Os compartimos un resumen de las recientes guias de contorneo de la SBRT renal ‼️

1
7
10
589
Fco de Paula Titos retweeted

Hoy hemos recibido las peores de las noticias
Nuestro querido compañero Jesús Saldaña ha fallecido en la catástrofe de Adamuz
Todos lo recordamos con mucho amor. Era una persona excepcional y única que daba todo para los pacientes y todos sus compañeros. Que descanse en paz.

1,624
2,891
22,656
1,365,292
Fco de Paula Titos retweeted

17 Dec 2025
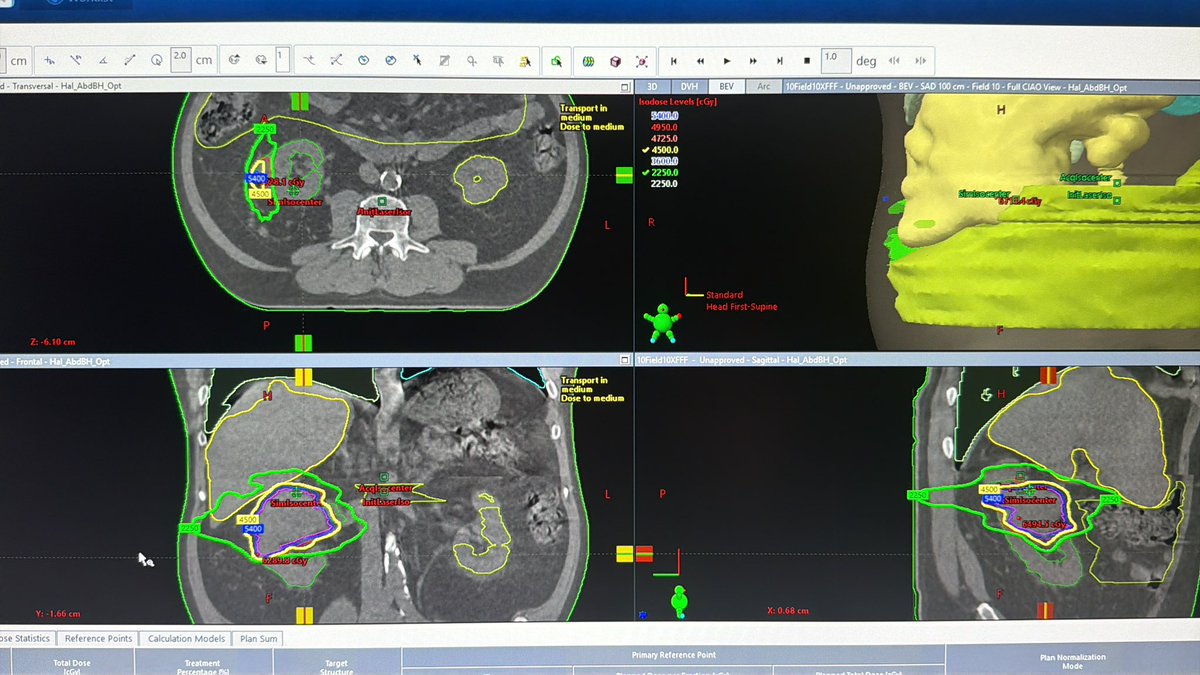
Shout out to the SAMURAI protocol for looking at what we should’ve been doing 20 years ago.
Treating the primary w/ SABR in metastatic RCC is such a no-brainer. No downtime and no seeding like CARMENA.
Many of these tumors have vascular involvement and are obvious seeders.
This is a young KPS 100 gentleman with newly diagnosed RCC with a few brain mets, a few small lung mets, and a 9cm primary.
He got postop fSRS to brain met cavity with treatment of two intact lesions w/in 2 wks surgery.
He’ll get 4500/5fx SABR (w/ GTV SIB to 5500) to the primary completed w/in 3 wks.
All this completed before insurance has even finished authing his initial dose of keytruda/lenvima.
Small lung nodules will be systemic therapy index, and can be SBRT’d to NED if they don’t respond.
5
23
73
5,659

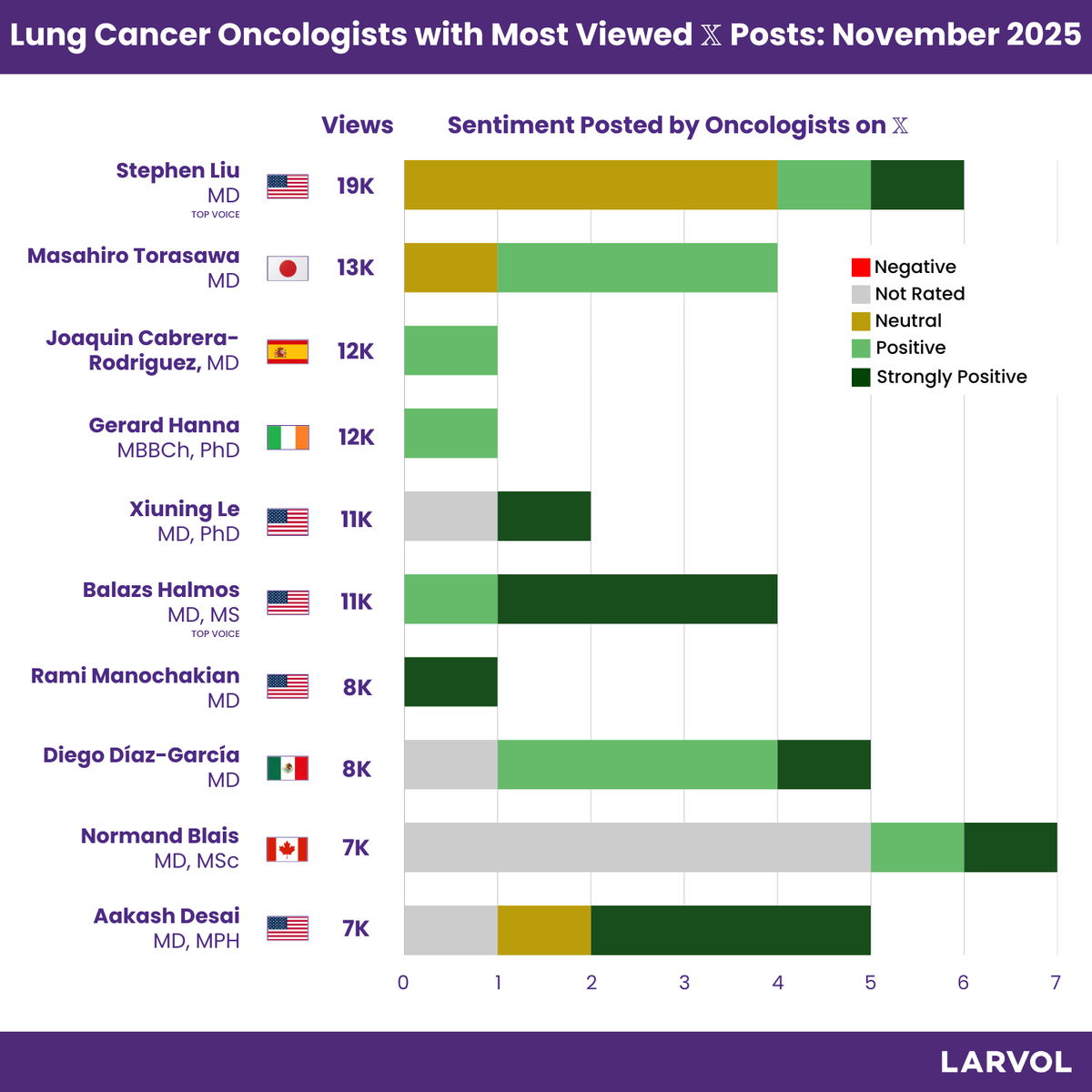
Top #LungCancer Oncologists for November 2025, curated by @LARVOL CLIN.
Explore more about oncology conferences, top trials, and reactions from oncologists: clin.larvol.com
#LARVOL #Oncology #CancerResearch #CancerData #OncologyInsights #ClinicalTrials #LCSM | @StephenVLiu | @M_Torasawa | @JoaquinJCabrera | @gerryhanna | @LeXiuning | @BalazsHalmosMD | @RManochakian | @diegoadiazg | @NormandBlais | @ADesaiMD
10
19
3,077

🎯Objetivo del nuevo presidente de la Sociedad Española de Oncología Radioterápica (SEOR), @drjavierserrano: mayor visibilidad a la especialidad en varios ámbitos.
#radioterapia #oncologiaradioterapica
consalud.es/profesionales/me…
8
11
650
Fco de Paula Titos retweeted

23 Nov 2025
La radioterapia no es solo máquinas ⚙️ y dosis 📏: es salvar vidas o mejorarlas 💖. Si la enseñamos bien, los estudiantes lo entienden y se enamoran 😍. ¡Cambiemos la percepción! 🔥 #radonc
. Para muestra un botón:
6
21
887
Fco de Paula Titos retweeted

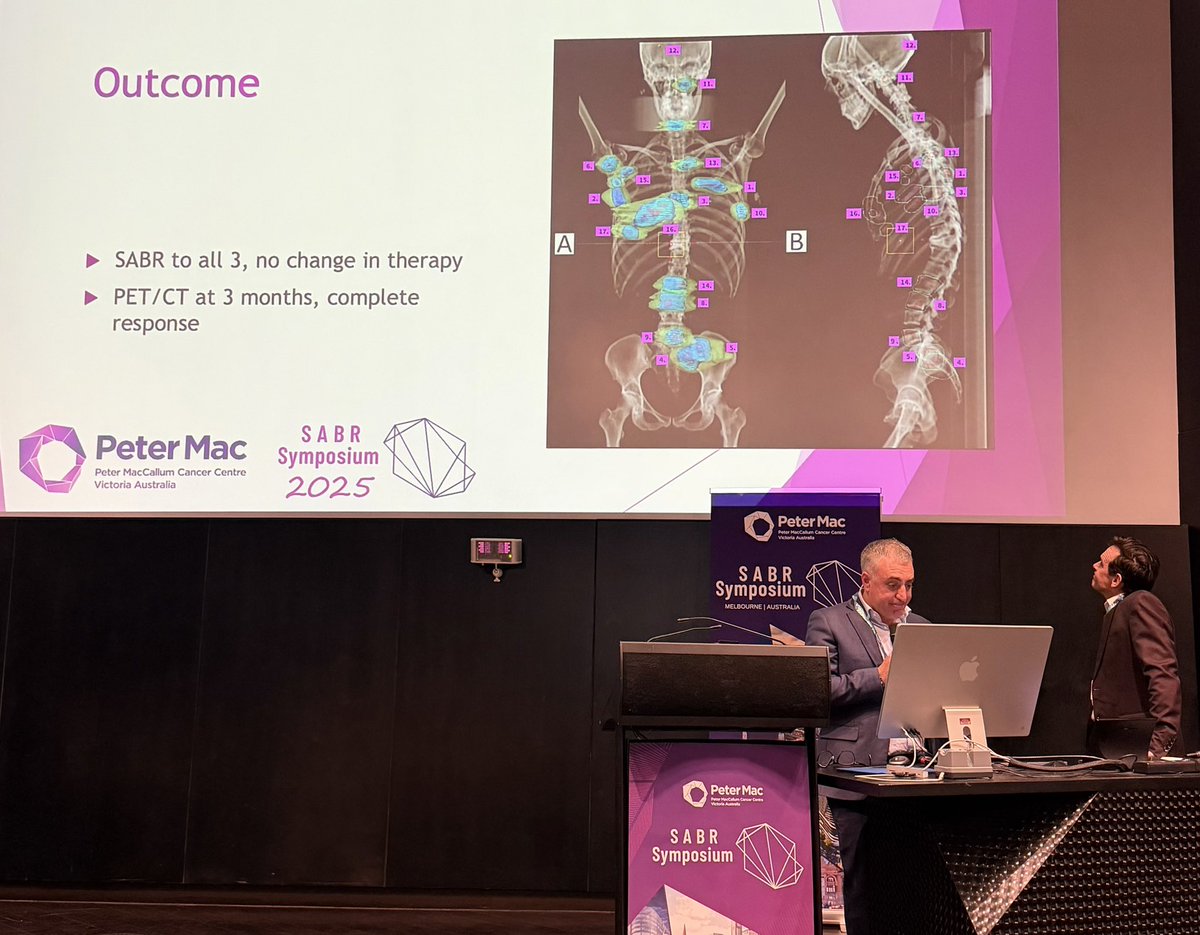
14 Nov 2025
We’re thrilled to welcome delegates from across the world for the Peter Mac SABR Symposium 2025.
Led by Prof @_ShankarSiva, it brings together global leaders in stereotactic ablative body radiotherapy for two days of cutting-edge learning, interactive sessions and expert panels

1
7
11
1,011
Fco de Paula Titos retweeted

14 Nov 2025
Extraordinary case at #SABR2025 by @drspdavid and De Mark Shaw @PeterMacRadOnc oligoprogressive #breastcancer without switching drug therapy. 8 years of SABR with #radonc, with preserved quality of life from the patient’s perspective!!! #bcsm
3
12
51
3,823
Fco de Paula Titos retweeted
14 Nov 2025
@BarbaraJereczek gives an overview of SABR in #prostatecancer…. Hard to beat, when one of her patients could RUN A MARATHON between one of his 5 sessions of curative treatment!!! #pcsm
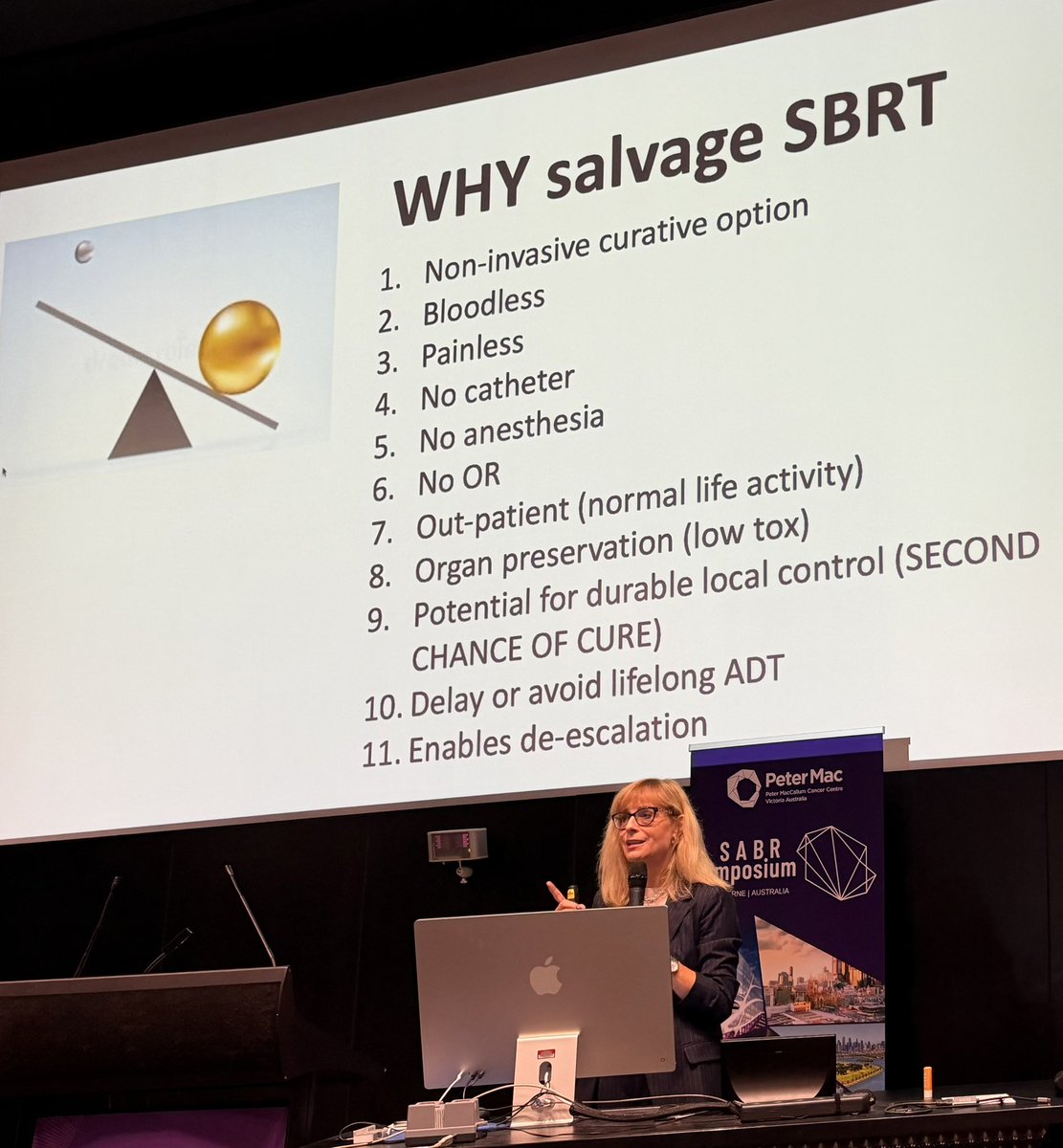
2
11
40
2,285
Fco de Paula Titos retweeted
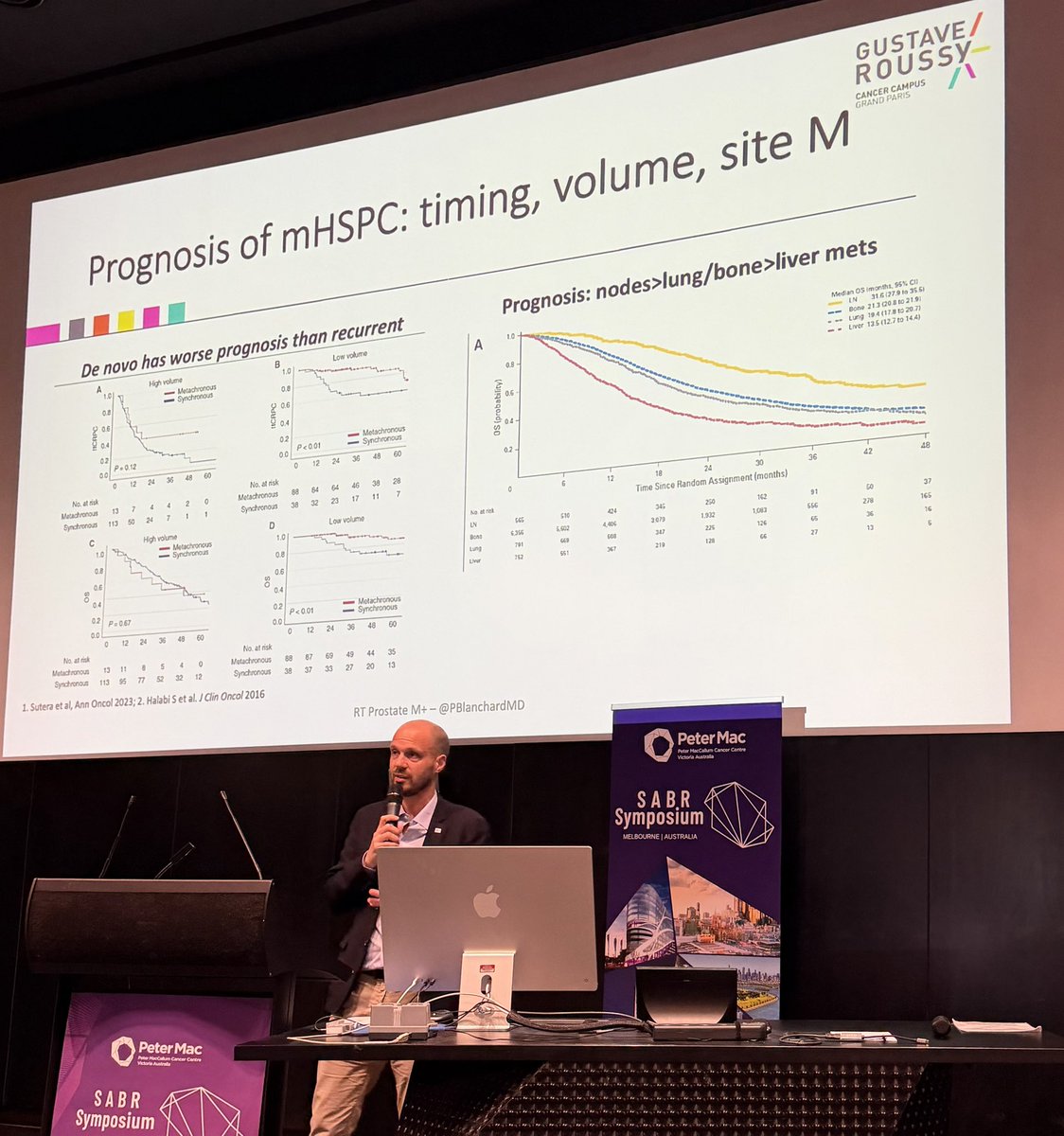
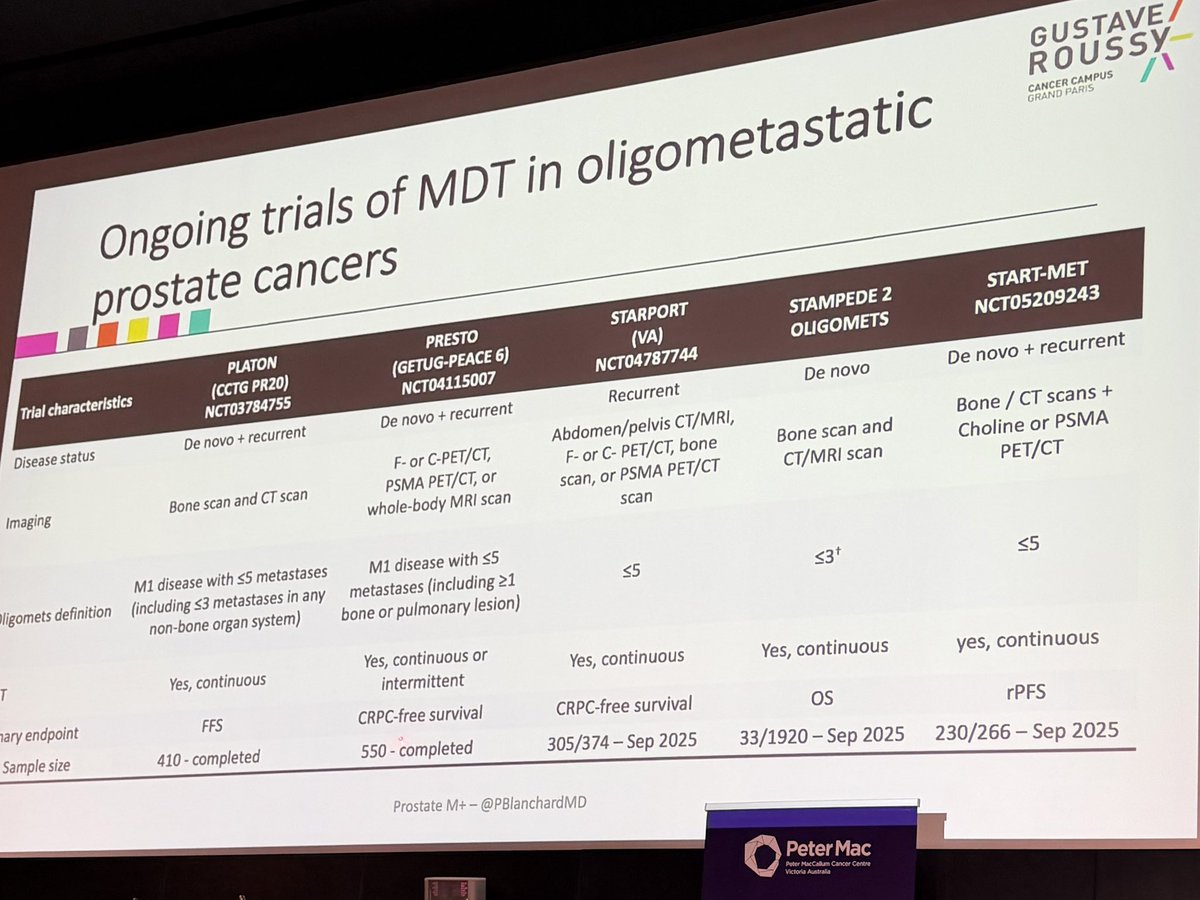
14 Nov 2025
@PBlanchardMD discusses SABR in oligometastatic #prostatecancer #pcsm - in both hormone sensitive and castrate resistant patients… and reminds us that lung metastases have a similar prognosis to bone secondaries; and the HR of benefit is the same in all studies ~0.50 #SABR2025

4
11
656
Fco de Paula Titos retweeted
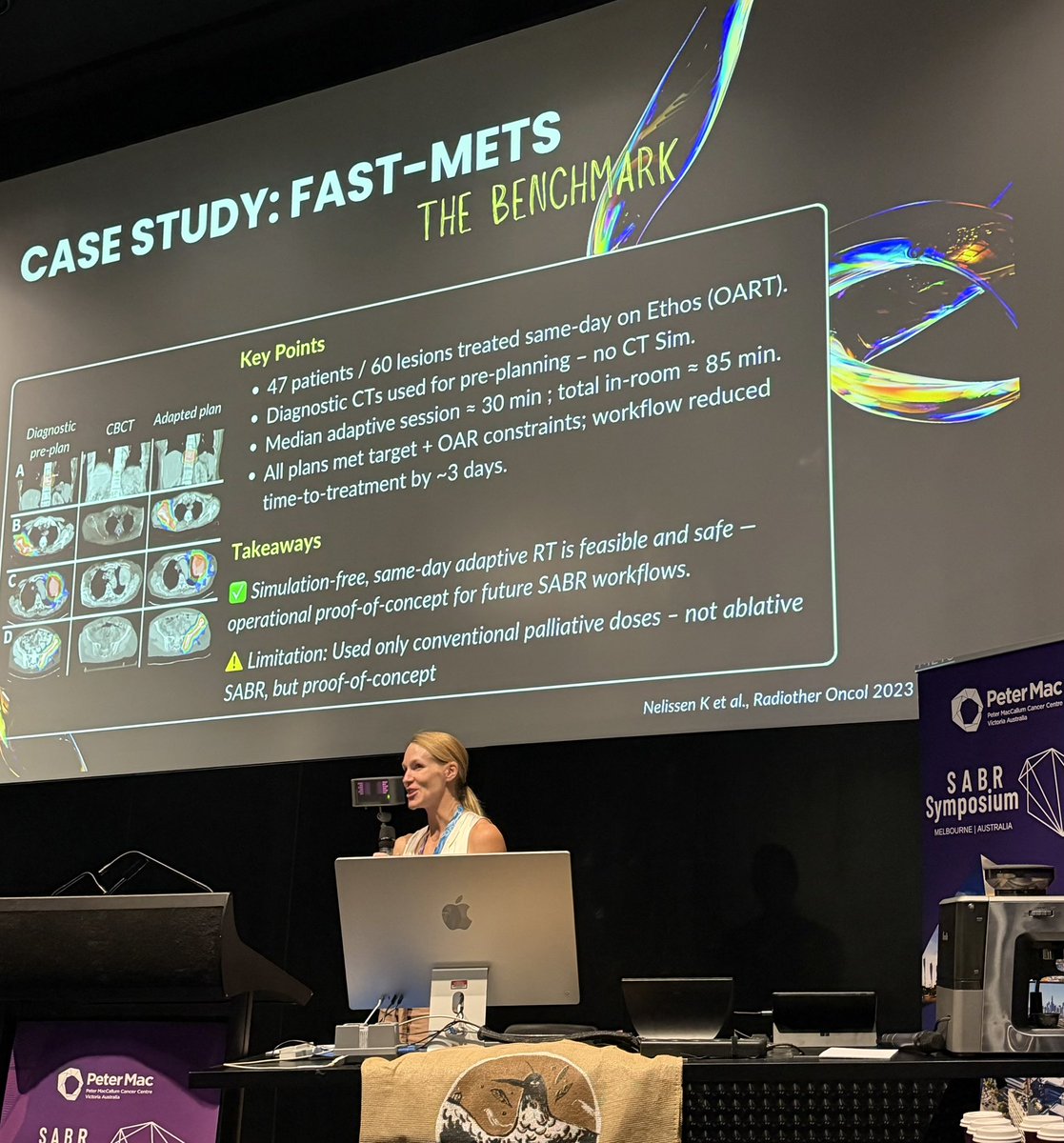
15 Nov 2025
😲@Melissa_O_Neil tells us the nuts and bolts of sim-free #radiotherapy at #SABR2025 - from pre-plan adaptive, one stop RT, and ‘on the fly SABR’ on the table … 😳
➡️ making #radonc faster, more accessible and attractive for our patients!



14
30
2,535
Fco de Paula Titos retweeted

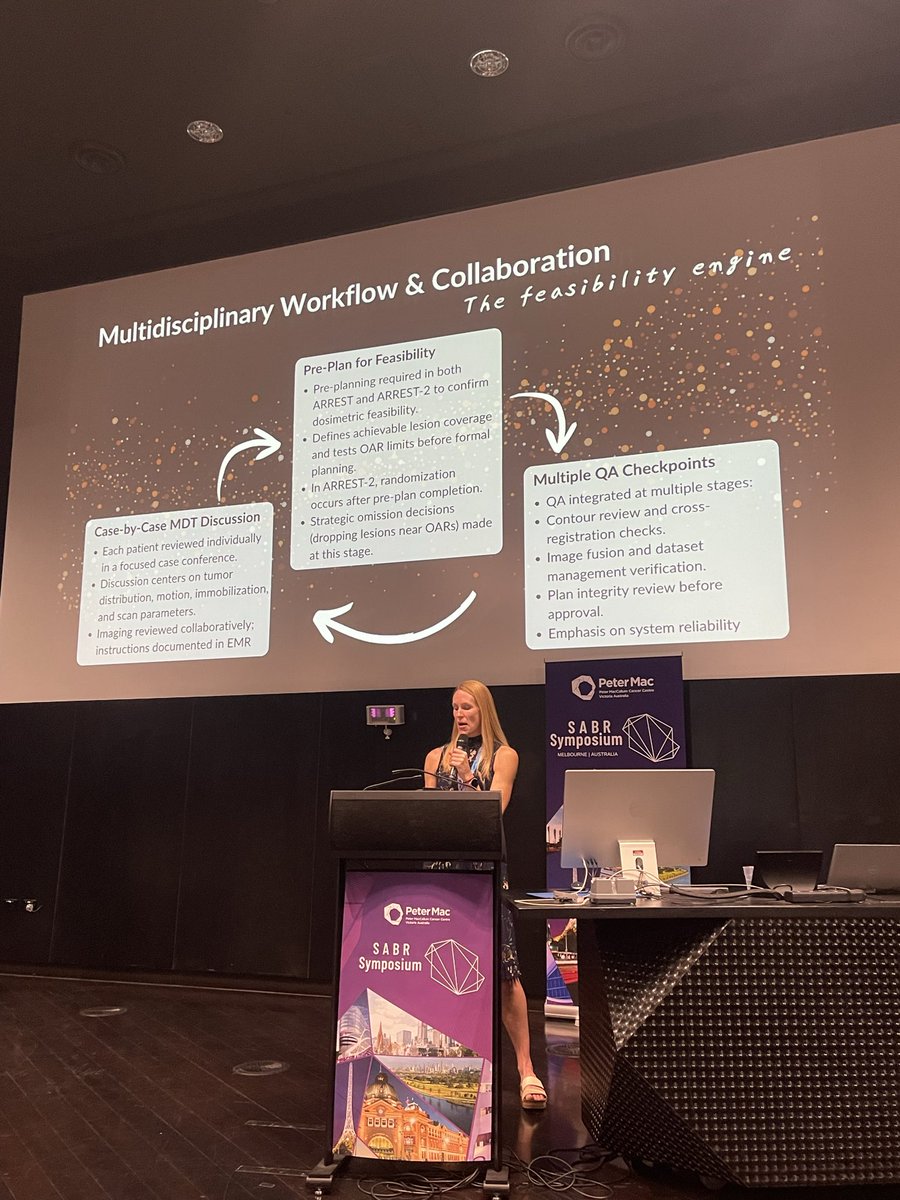
14 Nov 2025
#SABR2025 and ARREST trial, “The number is not the limit”🚀



11
27
1,202
Fco de Paula Titos retweeted

15 Nov 2025
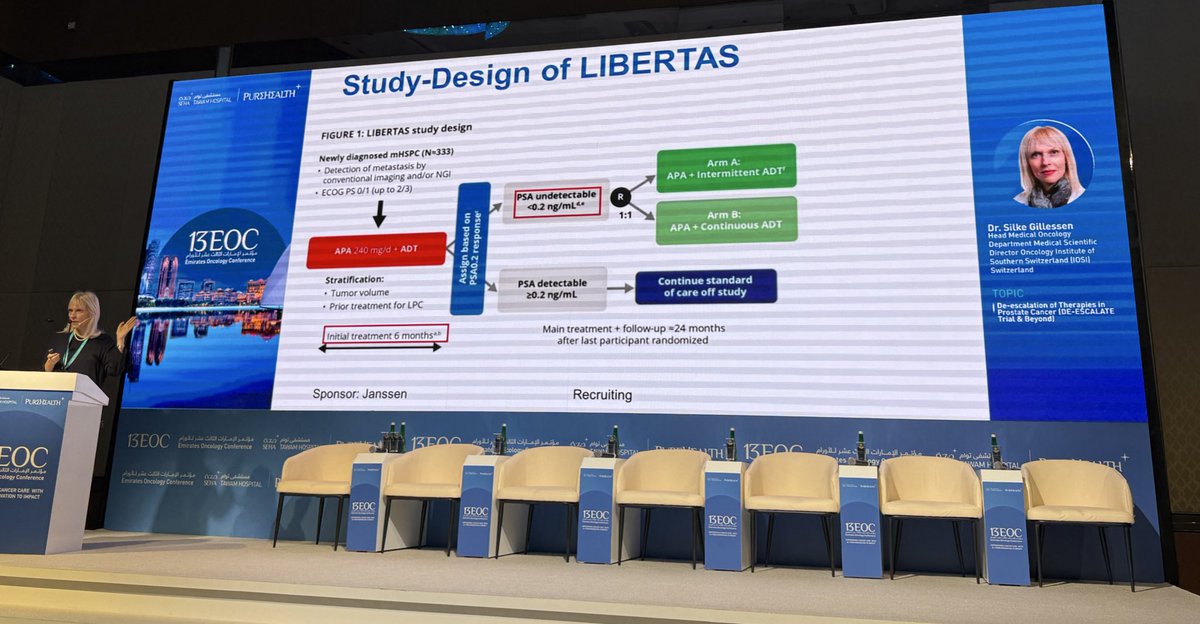
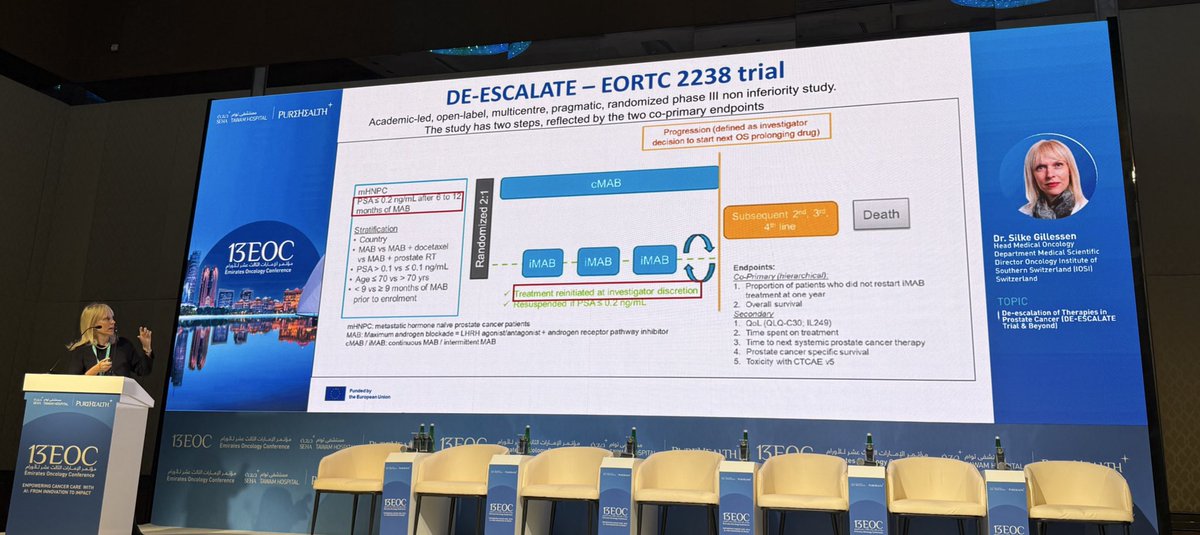
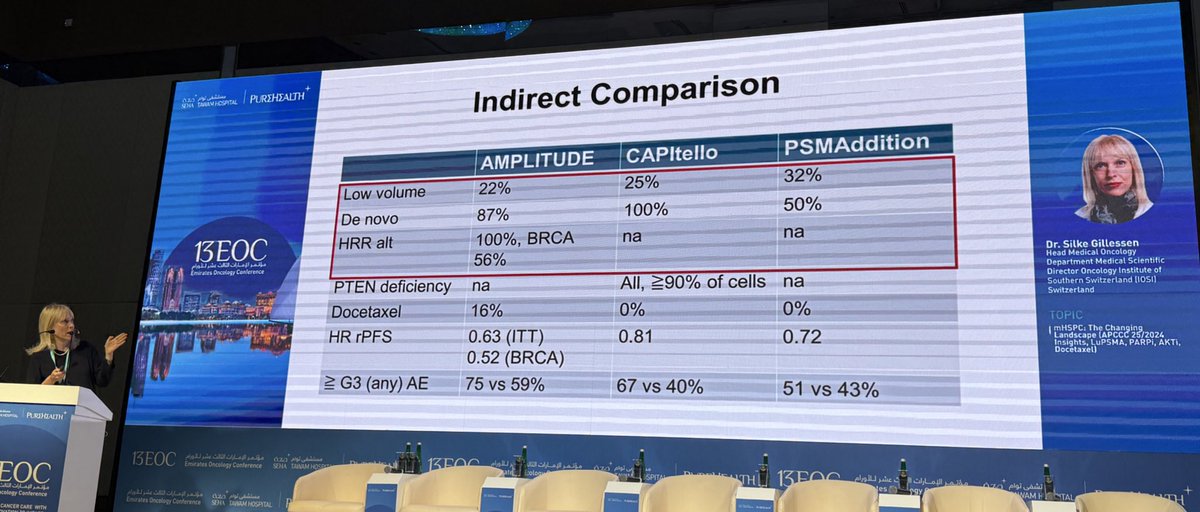
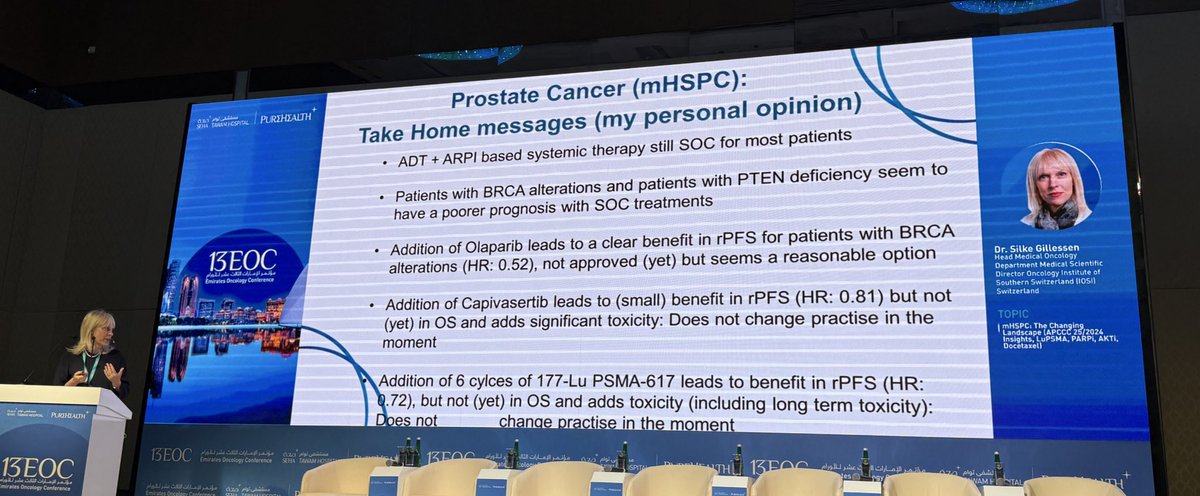
Most expert GU oncologists were supportive of discussing de-escalation of systemic ADT ARPI in mHSPC #ProstateCancer after achieving PSA<0.2 ng/ml at 2024 @APCCC_Lugano conference 👉 Dr @Silke_Gillessen discusses mHSPC de-intensification trials @13th EOC👇@OncoAlert @PCF_Science
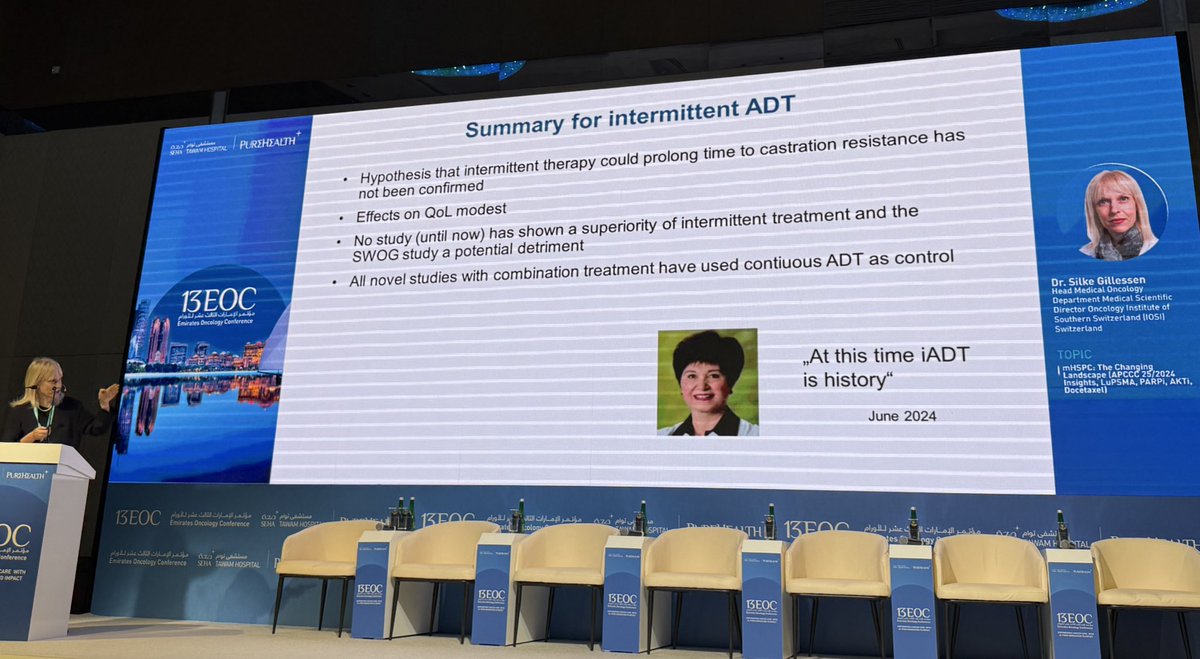

15 Nov 2025

Always a pleasure to hear Dr. @Silke_Gillessen 👉 very thoughtful perspective & excellent talk at the 13th Emirates Oncology Conference in Abu Dhabi on recent ph3 data in the mHSPC #ProstateCancer 👇 Shoutout to 2026 @APCCC_Lugano conference @OncoAlert


1
21
67
10,252
Fco de Paula Titos retweeted

15 Nov 2025
🚀 LUNAR Trial
In oligorecurrent HSPC, adding 2 cycles of ¹⁷⁷Lu-PSMA before SBRT more than doubles PFS (7.4 → 17.6 months) — a 63% reduction in progression, without added toxicity.
🔬 98% of progressions were new PSMA PET lesions, underscoring the power of targeting micrometastatic disease early.
📌 Importantly, it also delays the need for ADT— a major quality-of-life win.
📈 A compelling signal heading toward Phase III validation
@OncoAlert @MedwatchKate @weoncologists @OncoReporte @TresUramigas @Uromigos
27
66
7,914




