
Clinical Lab Scientist; Advocate for: Democracy, Science, NIH, Ukraine, Vaccines, COVID prevention
Joined October 2013
- Tweets 1,042
- Following 1,097
- Followers 189
- Likes 29,590
16 Photos and videos



Phil; COVID is NOT a cold!! retweeted

@American_Heart @ajpheartcirc @StanfordMed @DrBeniRusani @CardiologyToday @TrackYourHeart @ACCinTouch Critical information about post‑acute COVID conditions is still not reaching frontline clinicians, & #LongCovid patients continue to be misdiagnosed, dismissed, or left without care. Evidence‑based #COVID & #LongCovid CME is no longer optional- it is a patient‑safety imperative. Every missed diagnosis, every failure to order appropriate tests or referrals, risks preventable disability & death. We must urgently educate both clinicians & patients so they can recognize red flags, ask for the right evaluations, & access appropriate, multi‑system care.
#LongCovidAwareness

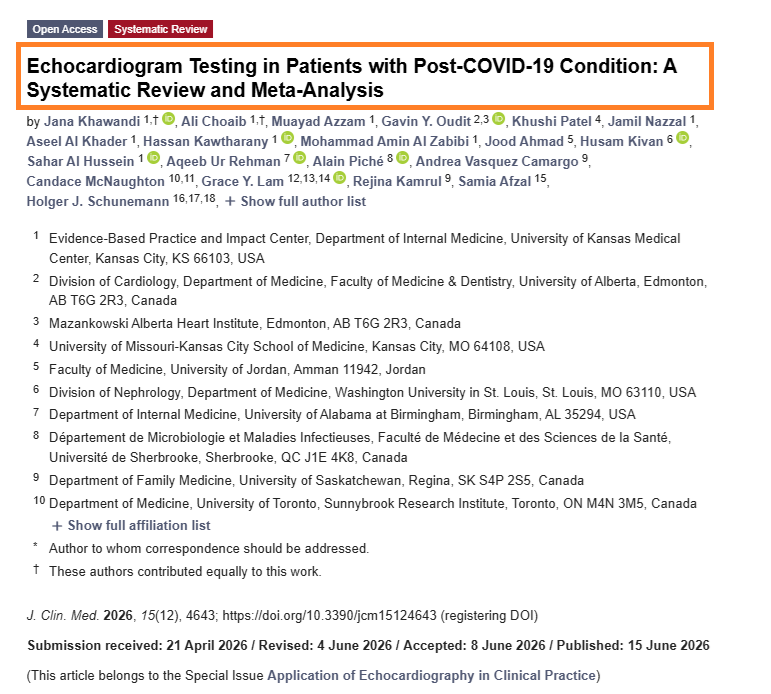
🚨 A Clear Message for Cardiologists: #LongCovid
Echocardiography is a starting point, not an endpoint exam!
➡️First-line tool:
2D-Echocardiography is reliable enough for initial screening and monitoring in post-COVID evaluations,
➡️The limitations:
It lacks precision and sensitivity for certain parameters like volumes and subtle myocardial disease,
➡️Advanced echo:
3D echo and strain imaging improve detection but lack universal availability and standardization,
➡️Necessary follow-up:
Comprehensive assessment requires progression to Coronary CT, Cardiac MRI (CMR), and Cardiac PET scans.
‼️My personal take as review article conclusion! ➡️Dig, Dig and you'll find!
#AvoidSars2 #AvoidReinfection
mdpi.com/2077-0383/15/12/464…
1
5
110
Phil; COVID is NOT a cold!! retweeted

Fewer COVID infections = lower lifetime cardiovascular risk.
A compelling thread. 👇
Jun 15
The long-term cardiovascular risks of SARSCoV2 infection and reinfections
Your heart is under silent, cumulative attack from SARSCoV2, and every reinfection can reload/worsen the damage.
Here a personal recap of 10 important studies from the last 2 years showing exactly how this virus and its reinfections can/may shape (and shorten) your cardiovascular future.
Evidence is clear, long-term, and growing.
Print and show your Cardiologist.
Let’s connect the dots…
1. Immunothrombosis multi-omics study:
3 months after hospitalisation, long COVID patients still have blood biologically “clot-ready” with persistent endothelial activation and prothrombotic signalling.
x.com/HarrySpoelstra/status/…
2. IL-6 & SAA 6-year study:
Higher acute-phase IL-6 and SAA levels independently predict cardiovascular events and death up to 6 years later, the initial inflammatory storm leaves a lasting CV mark.
x.com/HarrySpoelstra/status/…
3. MIS-C long-term outcomes:
Up to 4.5 years later, MIS-C raises cardiovascular disease risk 14× and hypertension 9× in children, with risks still accumulating.
x.com/HarrySpoelstra/status/…
4. Viruses & cardiac disease review:
SARS-CoV-2 stands out for direct cardiomyocyte invasion explosive damage relentless accumulation of risk with every reinfection.
x.com/HarrySpoelstra/status/…
5. Mayo PET long COVID study:
Persistent cerebral hypometabolism in fatigue/PEM patients still detectable up to 2 years post-infection.
x.com/HarrySpoelstra/status/…
6. Reinfection CV outcomes summary:
Reinfections worsen cumulative heart damage, arrhythmias, thrombosis, stroke risk and long COVID cardiovascular symptoms.
x.com/HarrySpoelstra/status/…
7. Youth reinfection & long COVID study:
Reinfection roughly doubles PASC risk, with myocarditis up to 3.6× higher, heart disease ~2× higher and increased thromboembolism.
x.com/HarrySpoelstra/status/…
8. Mild infection reinfection risk:
Even mild cases trigger lasting endothelial damage and prothrombotic state (1.5–2× long-term CV risk), each reinfection compounds the burden.
x.com/HarrySpoelstra/status/…
9 Mitochondrial dysfunction in long COVID:
Persistent mitochondrial dysfunction and suppressed oxidative phosphorylation remain in long COVID, pointing to durable multi-organ impact.
x.com/HarrySpoelstra/status/…
10. Cumulative reinfection impact on future CV health:
Reinfection stacks additional damage on prior endothelial injury and inflammation, increasing lifetime risk of heart failure, arrhythmias, thrombosis and accelerated cardiovascular disease.
x.com/HarrySpoelstra/status/…
11. Extra, my earlier general reminder post on this exact theme: x.com/HarrySpoelstra/status/…
‼️Overall convergence across the studies:
Immunothrombosis, acute inflammation markers, direct invasion, endothelial damage, and mitochondrial issues create lasting CV vulnerability that reinfections can keep reloading. #L0ngC0vid
The pattern is very clear.
Fewer infections = lower lifetime cardiovascular risk.
You only have one heart.
Protect it!
#AvoidSars2 #AvoidReinfections #CleanAir #VaccineUpdated
2
55
177
3,022
Phil; COVID is NOT a cold!! retweeted

Jun 15
Schools are full of COVID all year and are doing nothing to protect kids. Anyone who isn't wearing an N95 has had COVID multiple times. You don't need a study explicitly stating that any more than you need one to claim that people who keep jumping into the ocean keep getting wet.
10
40
341
7,579
Phil; COVID is NOT a cold!! retweeted
Jun 15
Fans will refuse to connect this to the ongoing pandemic because they want to continue attending the 2019-style concerts that spread illness, disability, and death throughout their communities. Treats over life.

17
188
1,012
15,673
Phil; COVID is NOT a cold!! retweeted

Jun 13
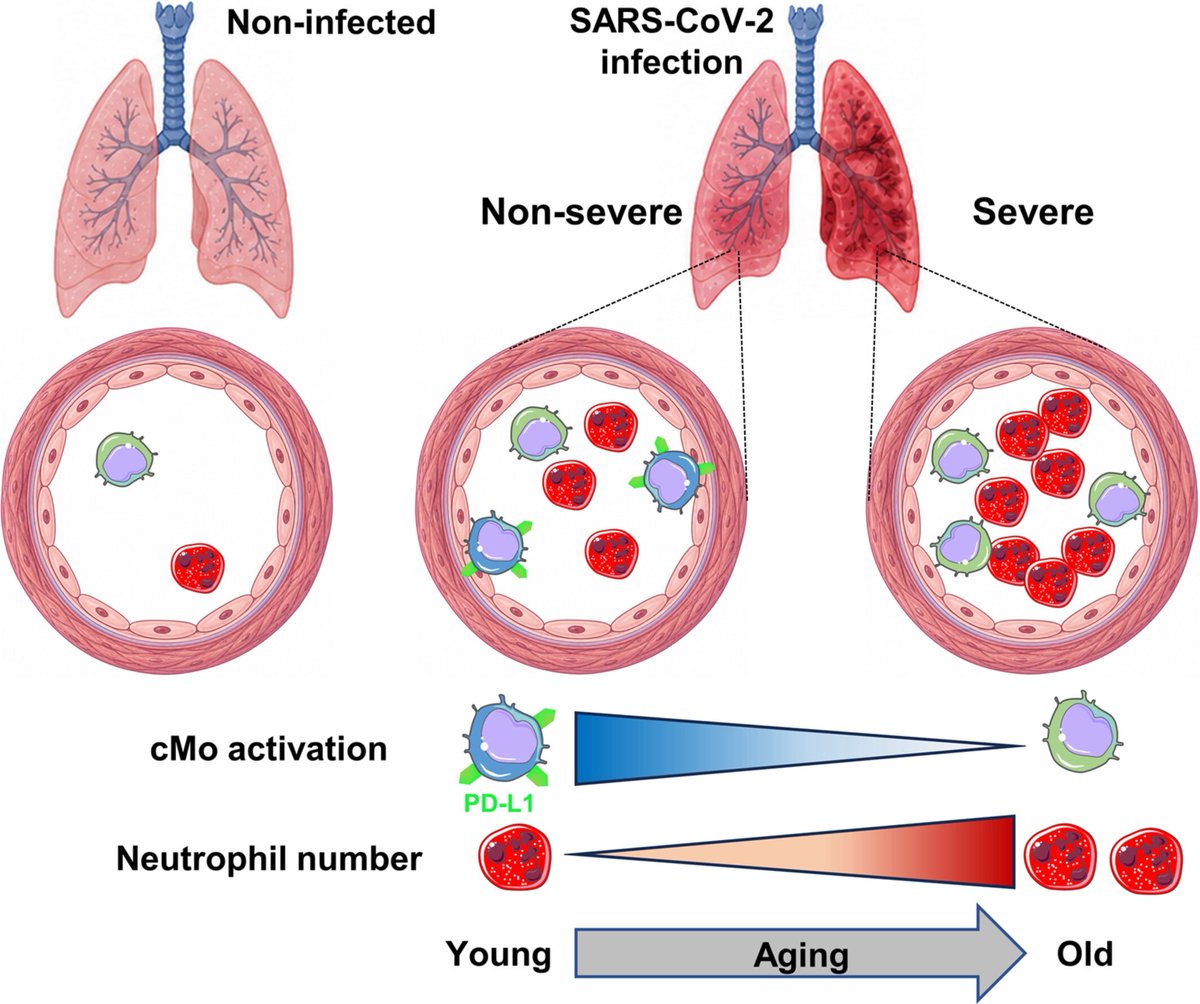
Why does COVID-19 hit older adults so much harder?
➡️ A NEW study points to an unexpected answer: not just too much inflammation, but a failure of immune regulation inside the lungs.
➡️ Researchers found that aging shifts the balance toward excessive neutrophil accumulation while reducing a key population of PD-L1–expressing regulatory monocytes in the lungs.
➡️ The result is a maladaptive immune response characterized by inflammatory excess without adequate immune control. 1/
6
54
125
2,786
Phil; COVID is NOT a cold!! retweeted

Jun 11
How many Americans died who wouldn't have - if America were France or Japan?
The answer - 14.7 million over the past four decades.
And that number is still climbing🧵
3
26
100
3,531
Phil; COVID is NOT a cold!! retweeted

Jun 10
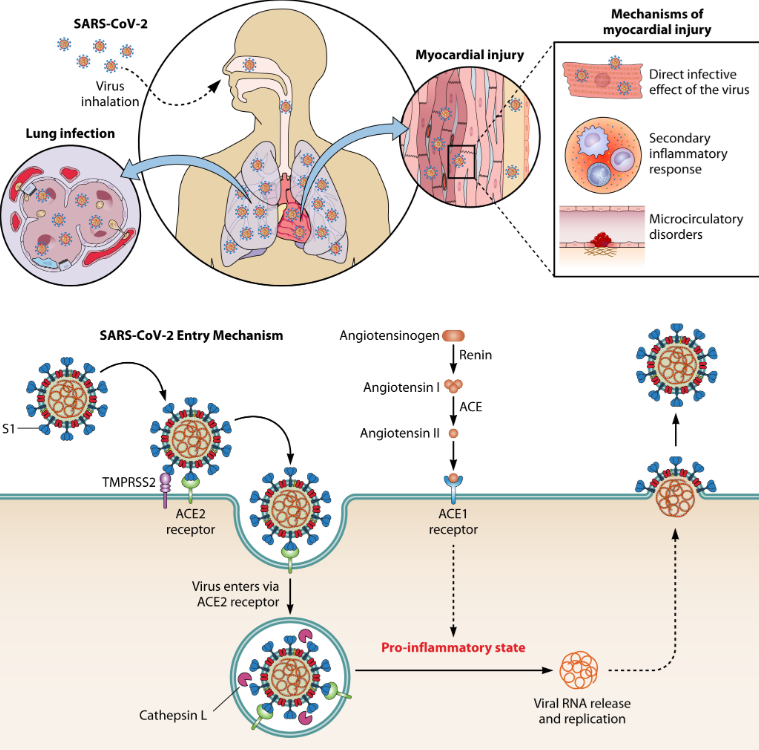
Research progress on the association between viruses and cardiac diseases
🚨Your heart’s deadliest serial offender just got named: SarsCoV2
Interesting Chinees review just mapped how six viruses attack the heart.
One stands out!
Not because the authors scream “worst ever,” but because the science does.
→Direct heart-cell invasion long-term damage cumulative hits from regular reinfections = a unique threat!
Vaccines help. But the data is sobering.
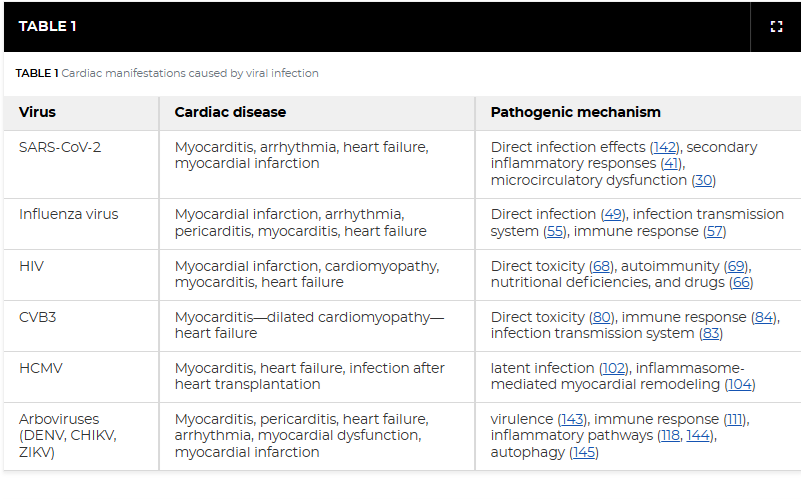
Let’s break it down virus by virus(review):
1. SARSCoV2:
- Enters cardiomyocytes and pericytes via ACE2 receptor (membrane fusion/endocytosis).
- Direct infection triggers myocarditis, pericarditis, arrhythmias, heart failure (de novo or exacerbation), microclots, thromboembolic events and myocardial infarction,
- Long-term: persistent cardiac inflammation, dysautonomia and long-COVID cardiovascular symptoms,
- Possible viral persistence in tissue,
- Vaccination reduces myocarditis risk/CV complications compared with natural infection,
-Regular reinfections!
2.Influenza (A/B):
- Direct replication in cardiomyocytes, Purkinje cells and endothelial cells (independent of lung titers),
- Causes myocarditis, pericarditis, arrhythmias, heart-failure flares and myocardial infarction via both cytopathic effects and cytokine-driven systemic inflammation/endothelial dysfunction.
- Long-term: myocardial fibrosis and remodelling,
- Vaccines lower infection-related cardiovascular complications,
3. HIV:
- No productive cardiomyocyte infection,
- Indirect damage from chronic immune activation, endothelial dysfunction, metabolic changes and antiretroviral toxicity,
- Drives cardiomyopathy (myocarditis in advanced cases), heart failure, myocardial infarction and stroke,
- Long-term: premature cardiovascular aging, fibrosis and remodelling even on suppressive therapy,
4. CVB3 (Coxsackievirus B3):
- Enters via CAR receptor,
- Direct cytopathic necrosis, oedema and impaired contractility in cardiomyocytes,
- Rapid progression to myocarditis, dilated cardiomyopathy, arrhythmias (QTc prolongation) and heart failure,
- Chronic inflammatory cardiomyopathy is a hallmark sequela,
5. Human cytomegalovirus(HCMV):
- Lifelong latency with reactivation (especially in immunocompromised),
- Induces myocarditis, heart failure, transplant vasculopathy and atherosclerosis through sustained inflammation and vascular injury,
- Long-term myocardial remodelling,
6. Arthropod-borne viruses(Arboviruses = DENV, CHIKV, ZIKV):
- Direct cardiac invasion (some models) plus immune-mediated injury,
- Associated with myocarditis, arrhythmias, heart failure, shock and (CHIKV) dilated cardiomyopathy or long-term ischemic heart disease/cerebrovascular risk.
‼️So, this minireview examines six cardiotropic viruses side-by-side, yet SARS-CoV-2 receives the most space because of its proven direct cardiomyocyte invasion, explosive multi-pathway damage, and documented long-term cardiac persistence, risks that broader population data show accumulate relentlessly with every regular reinfection, creating an immediate and chronic cardiovascular burden on a global scale that no other virus in this review matches.
→Your heart’s deadliest serial offender just got named: SarsCoV2!
#PREVENTION #COVIDHeart #RepeatInfectionKills #AvoidSars2 #AvoidReinfections #YouOnlyHaveOneHeart
journals.asm.org/doi/10.1128…
11
228
464
11,275
Phil; COVID is NOT a cold!! retweeted
A widely used joint-health supplement may have an unexpected dark side for the aging brain.
➡️ Researchers analyzing >12 years of health records found that glucosamine use was associated with a 25% higher risk of progression from mild cognitive impairment to Alzheimer’s disease, and a 25% higher mortality risk among patients with established dementia! 1/
3
57
130
9,172
Phil; COVID is NOT a cold!! retweeted

Alma was a healthcare worker for over 25 years. She had insurance. And when her oncologist recommended MD Anderson for a second opinion, they told her it would be $16,000 upfront just to be seen.
She couldn't afford it. She didn't get the care.
Alma passed away.
I stood up to honor her today because she deserves to be remembered. And because her words are still doing something — still making people uncomfortable in the right way.
"If they treat me like that, can you imagine how they treat someone that doesn't know anything?"
No. We shouldn't have to imagine it. We should be outraged by it.
Alma's name means soul. And I felt her soul in that room today.
Rest in power, Alma. We're still listening. 🤍
23
272
869
25,835
Phil; COVID is NOT a cold!! retweeted
Jun 8
Excellent and biologically rich review.
It brings together neuroinflammation, glia, BBB, vascular dysfunction, mast cells, the vagus nerve, and viral persistence - and adds an original hypothesis of local sleep - a state in which small groups of neurons shift into a sleep-like/silent mode even while a person is awake - which could help explain both brain fog and flares.
Jun 8

Happy to share that after a prolonged peer-review process, our review covering the major Neuroinflammatory events in #LongCovid was accepted today for publication at @Transl_Psych from the @NaturePortfolio! Coming soon, but preprint available here: preprints.org/manuscript/202…
5
105
314
18,649
Phil; COVID is NOT a cold!! retweeted
Jun 8
Českem prý hýbe nevídaný nárůst duševních poruch u dětí a mladistvých.
Škoda, že @ZdravkoOnline i @VZPtweetuje zapomněly říct rodičům, že diagnostika deprese a úzkosti naroste po mírném COVID-19 o 40%, dvakrát zároveň po infekci roste riziko sebepoškozování, otrav a sebevražedných myšlenek.
A nejde jen o diagnostiku. Kriminalita mezi dětmi v Česku stoupla mezi lety 2021 a 2024 o třetinu.
Agrese, impulzivita a antisociální chování se objevují v době, kdy se většina dětí a mladých opakovaně nakazila SARS-CoV-2.
Virus je neurotropní a poškozuje frontální lalok (centrum empatie, sebekontroly, regulace emocí). Každá další infekce = další mikrotrauma, které neodhalí běžné MRI, ale které zhoršuje rozhodování, impulzivitu a schopnost soucitu.
Pokud necháme děti dál volně procházet infekcemi bez ochrany, riskujeme generaci s vyšší agresí, slabší seberegulací a větším sklonem k chybám, duševním nemocem i destruktivnímu chování. Jak je vidět, není to už jen problém zdravotní.
Neurologové a neurovědci to vědí dávno. Problém je, že se tyto poznatky prakticky nepřenesly do veřejného zdravotnictví, školství ani k rodičům. zdravotnickydenik.cz/2026/06…
5
67
161
4,334
Phil; COVID is NOT a cold!! retweeted

Jun 8
“Post-COVID-19 syndrome (PCS) is an escalating global health concern, marked by persistent cognitive, neurological, and psychiatric symptoms following acute SARS-CoV-2 infection.
Although its underlying mechanisms remain incompletely understood, mounting evidence implicates chronic neuroinflammation as a key driver.
Sustained microglial and astrocyte activation, blood-brain barrier disruption, and aberrant cytokine signaling contribute to prolonged immune dysregulation within the central nervous system, promoting long-term brain dysfunction”
Jun 8
Happy to share that after a prolonged peer-review process, our review covering the major Neuroinflammatory events in #LongCovid was accepted today for publication at @Transl_Psych from the @NaturePortfolio! Coming soon, but preprint available here: preprints.org/manuscript/202…
1
14
27
1,611
Phil; COVID is NOT a cold!! retweeted
Jun 8
A genuinely interesting study.
Researchers from Johns Hopkins looked at how SARS2 infection changes the cardiac autonomic nervous system - how the heart is regulated through the sympathetic and parasympathetic branches.
It’s not one fixed state.
It’s a process.
In three phases🧵
Dynamic changes in cardiac autonomic function persist in the post-acute phase after SARS-CoV-2 infection in a hamster model of COVID-19
🚨IMPORTANT, AUTONOMIC DYSFUNCTION!
Human studies have shown observational links between Long COVID and autonomic dysfunction. This new USA hamster model study adds CAUSAL evidence and TEMPORAL data, proving the dysfunction evolves dynamically and does not resolve!
Model:
- Syrian hamsters intranasally infected with SARSCoV2
- Continuous telemetry ECG monitoring of heart rate and heart-rate variability (HRV) at multiple time points (acute, recovery, and post-acute phases, weeks after viral clearance).
Main finding:
A. Infection triggers a triphasic pattern of cardiac autonomic dysfunction:
-1. Acute sympathetic hyperactivation,
-2. Transitional shift, and
-3. Persistent dysregulation that continues long into the post-acute phase,
B. HRV parameters remained significantly altered weeks after the virus was undetectable, showing ongoing imbalance in sympathetic/parasympathetic control,
C. No direct viral persistence in the heart, yet autonomic signalling stayed disrupted,
D. Preliminary data implicate oxidative stress pathways as one potential driver.
As far as I know, this is the first robust preclinical animal model to demonstrate dynamic, time-dependent, and long-lasting cardiac autonomic changes directly caused by SARSCoV2!
‼️So, SARSCoV2 doesn’t just cause a temporary “flu,” it leaves the heart’s autonomic nervous system permanently rewired. Long COVID dysautonomia is real, a measurable biology, not anxiety or deconditioning. This hamster model proves the damage persists and evolves even after the virus is gone and gives us researchers a candidate focus needed to finally fix it.
‼️“Inhibition of innate immune activation or mitochondrial oxidative stress during the acute phase prevents the autonomic dysfunction in the post-acute phase, offering a potential strategy to mitigate long COVID syndromes.”
‼️In short: it moves the LC field from “we see it in patients” to “here’s how and why it lasts!”
#LongCovid #Dysautonomia #AvoidSars2 #AvoidReinfections
heartrhythmopen.com/article/…

6
92
267
9,276
Phil; COVID is NOT a cold!! retweeted

I'm a cardiologist. A 42-year-old mother of two came to my office complaining of jaw pain and crushing fatigue. She ran half-marathons. Her EKG was normal. Another doctor had sent her home with anxiety medication.
When I got her into the cath lab, I found severe microvascular disease — plaque choking the tiniest vessels of her heart, the ones standard angiograms routinely miss.
Her heart had been starving in silence while everyone told her she was stressed.
She is alive today. Too many women like her are not.
Heart disease kills more women than every cancer combined. And medicine is still diagnosing it through a male lens.
84% of cardiologists report having patients in the past year whose heart disease was misdiagnosed by another physician. Women with a STEMI heart attack have a 59% greater chance of being misdiagnosed compared to men. Women with an NSTEMI — 41% greater chance.
The reason is structural. For decades, we screened, tested, and treated women using a template built for men.
Men's heart attacks announce themselves — the crushing chest pain, the clutched fist, the Hollywood collapse. Women's hearts whisper. Crushing fatigue that feels like wearing a lead vest. Jaw pain written off as TMJ. Nausea blamed on a stomach bug. An ache between the shoulder blades blamed on a long week. Shortness of breath blamed on being out of shape.
For years, medicine called these "atypical" symptoms. They are not atypical. They are female-typical. Half of humanity is not a variant.
And the biology runs deeper than symptoms.
Women have smaller hearts and narrower coronary arteries. Plaque doesn't only clog the big highway vessels — it hides in the microvasculature, the tiny branches feeding the heart muscle itself. A woman can have a heart attack with a completely "clean" standard angiogram.
SCAD — spontaneous coronary artery dissection — occurs 90% of the time in women. Often young, fit women with zero traditional risk factors. It's the leading cause of heart attack in women under 50, accounting for roughly one quarter of all cases in that age group. Most doctors have never diagnosed one.
And some of the most dangerous cardiac risk factors are hidden in women's medical histories where no one thinks to look:
Preeclampsia or gestational hypertension doubles to quadruples lifetime heart disease and stroke risk. Pregnancy is the body's first cardiac stress test — and these complications are early warning sirens, not closed chapters.
Autoimmune disease — lupus, rheumatoid arthritis, psoriasis — far more common in women, turbocharges inflammation and plaque formation at any age.
Cardiovascular disease in women aged 20-44 is projected to surge nearly 50% by 2050.
The youngest patients in my practice keep getting younger.
What every woman should ask her doctor — and what every doctor should be asking:
"Given my pregnancy history, autoimmune status, and family history — what is my full cardiovascular risk?" If they don't ask about preeclampsia or gestational diabetes, volunteer it.
"Should I have an Lp(a) test and a coronary calcium score?" Standard cholesterol panels miss too much. Lp(a) is genetic, one-time, and most women have never been tested.
"My tests came back normal but my symptoms haven't stopped — what's next?" Normal stress tests and angiograms can miss microvascular disease, spasm, and SCAD. Persistent symptoms warrant coronary CT angiography or cardiac MRI.
And if something feels wrong — say these exact words to your doctor: "I am concerned this could be my heart."
That single sentence changes the workup. Do not soften it. Do not apologize for it.
80% of heart disease is preventable. But the playbook has to be built for female biology.
Two decades ago, I wrote one of the first books warning that heart disease was the number one killer of women and that medicine was diagnosing it through a male lens. It was recognized by First Lady Laura Bush at the White House during the early years of the national conversation about women's heart health.
I'm haunted by how much of that book I could republish today unchanged.
The science has advanced. The awareness has grown. But the gap between what we know and what happens in the exam room is still costing women their lives.
Share this with every woman you love — and every doctor who treats them. READ MORE: open.substack.com/pub/afshin…
180
2,661
6,626
771,952

RT @BigBadDenis: 🧵"What we know (and don't) about Covid-19's effect on the immune system."
1. Lasting impact
2. This looks like...
3. 5-20…
109
Phil; COVID is NOT a cold!! retweeted

Jun 6
“We are about to witness an unprecedented event that will push crops around the globe to their limit.”
No one will see it coming because we are forbidden from discussing it.
The below post w/graph got 31 likes in 8 hours. Media/social media is owned by billionaires.
The End.

‘There's no event in our history books that combines the current global population with the impending fertilizer shortage and the strength of the El Nino that's coming. We are about to witness an unprecedented event that will push crops around the globe to their limit.’
11
217
870
22,258
Phil; COVID is NOT a cold!! retweeted

Jun 7
In 2020, two months after my C-19 infection, I was admitted to the same hospital where I trained with a heart rate of 135 (sinus tach) and oxygen sat of 89 in bed.
My attending physician was a guy I’d been good friends with since intern year, who knew I was a healthy, endurance athlete.
He looked at the monitor and asked me if I thought my vitals were “real.” He then proceeded to document in the chart something along the lines of: “it may be anxiety but it may be something else.”
Really hoping insight has grown since then, and Simone gets prompt care for what’s causing her tachycardia. Because despite all I’ve seen in my career, and gone through as a patient, that was a snapshot in time that still haunts me.
And I’m still not well 6 years later.
Jun 7

Simone Biles lying in bed with a resting heart rate of 126.
Very curious to hear what they say is causing that.
😥

25
190
1,165
92,766
Phil; COVID is NOT a cold!! retweeted

Jun 7
1. Remember that any attempt to paint Long Covid as psychogenic in nature deliberately and completely incorrectly biologically decouples SARS-CoV-2 infection from Long Covid. In essence, this rhetoric shifts the causative factor for LC from the virus to the patient's mind.
20
403
1,492
50,644
Phil; COVID is NOT a cold!! retweeted
Jun 6
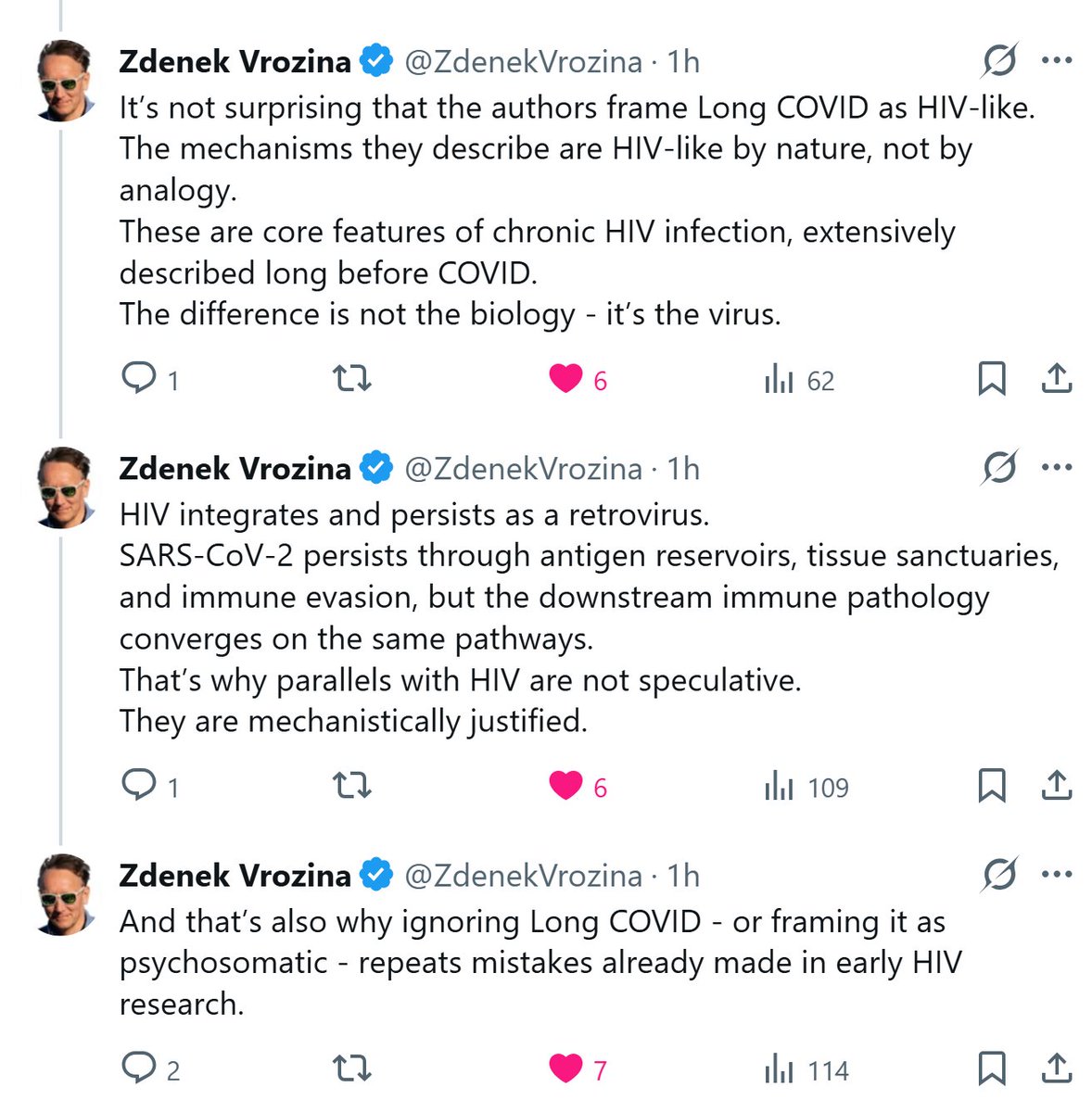
Viral proteins can activate the same pathways after infection that connect neuroinflammation, synapse loss, tau, alpha-synuclein, and broken cellular cleanup.
That’s why parallels with other viruses, including HIV, matter.
A new review tries to put this whole story together. 🧵
4
44
153
4,192
Phil; COVID is NOT a cold!! retweeted
Jun 5
Does the brain always return to baseline after COVID?
A new multimodal MRI study suggests the answer may be - not always.
After infection, some brains may remain in a different network state - and we still do not know if that state is temporary, compensatory, or maladaptive🧵
10
176
556
23,702