
Bedford to London services set to be suspended over two weekends dlvr.it/TT3204 #AccessforAll #Bedford #Cambridge #EastCoastMainLine
4

Jun 15
Bedford to London services set to be suspended over two weekends dlvr.it/TT31XF #AccessforAll #Bedford #Cambridge #EastCoastMainLine
12

Jun 15
Bedford to London services set to be suspended over two weekends railadvent.co.uk/2026/06/bed… #AccessForAll #bedford #cambridge #EastCoastMainLine #EastMidlandsRailway #harlington #harpenden #hendon #hitchin #london #luton #LutonAirportParkway #midlands
243

Every child deserves access to an education that will meet their specific needs, regardless of family resources or neighborhood location. That's why educational choice is so important.
#SchoolChoice #FindYourFit #AccessforAll
4

Jun 13
Over 2 billion people lack safe drinking water.
Inclusion is not a concept.
It’s infrastructure, access, and equity.
#SuperWaterMan #CleanWaterForAll #WaterIsLife #EquityMatters #GlobalWaterCrisis #HumanRights #AccessForAll #ClimateJustice #InclusiveFuture #SplashySaturday

2

Jun 13
Over 2 billion people lack safe drinking water.
Inclusion is not a concept.
It’s infrastructure, access, and equity.
#AndSoItFlows #CleanWaterForAll #WaterIsLife #EquityMatters #GlobalWaterCrisis #HumanRights #AccessForAll #ClimateJustice #InclusiveFuture #SplashySaturday

2

Over 2 billion people lack safe drinking water.
Inclusion is not a concept.
It’s infrastructure, access, and equity.
#Watercelebration #CleanWaterForAll #WaterIsLife #EquityMatters #GlobalWaterCrisis #HumanRights #AccessForAll #ClimateJustice #InclusiveFuture #SplashySaturday

4

Jun 13
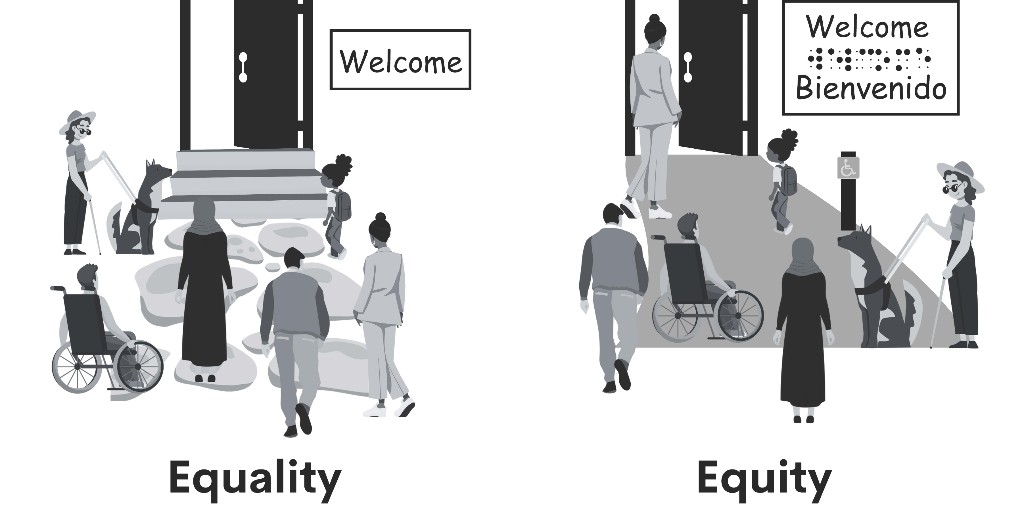
Equality and equity are not the same thing, and this infographic keeps that message clear. Giving everyone the exact same thing is not always what helps people succeed. 🌈📘💛 ow.ly/fJMR50Z3MXk
#KYSPIN #Equity #Inclusion #AccessForAll
2

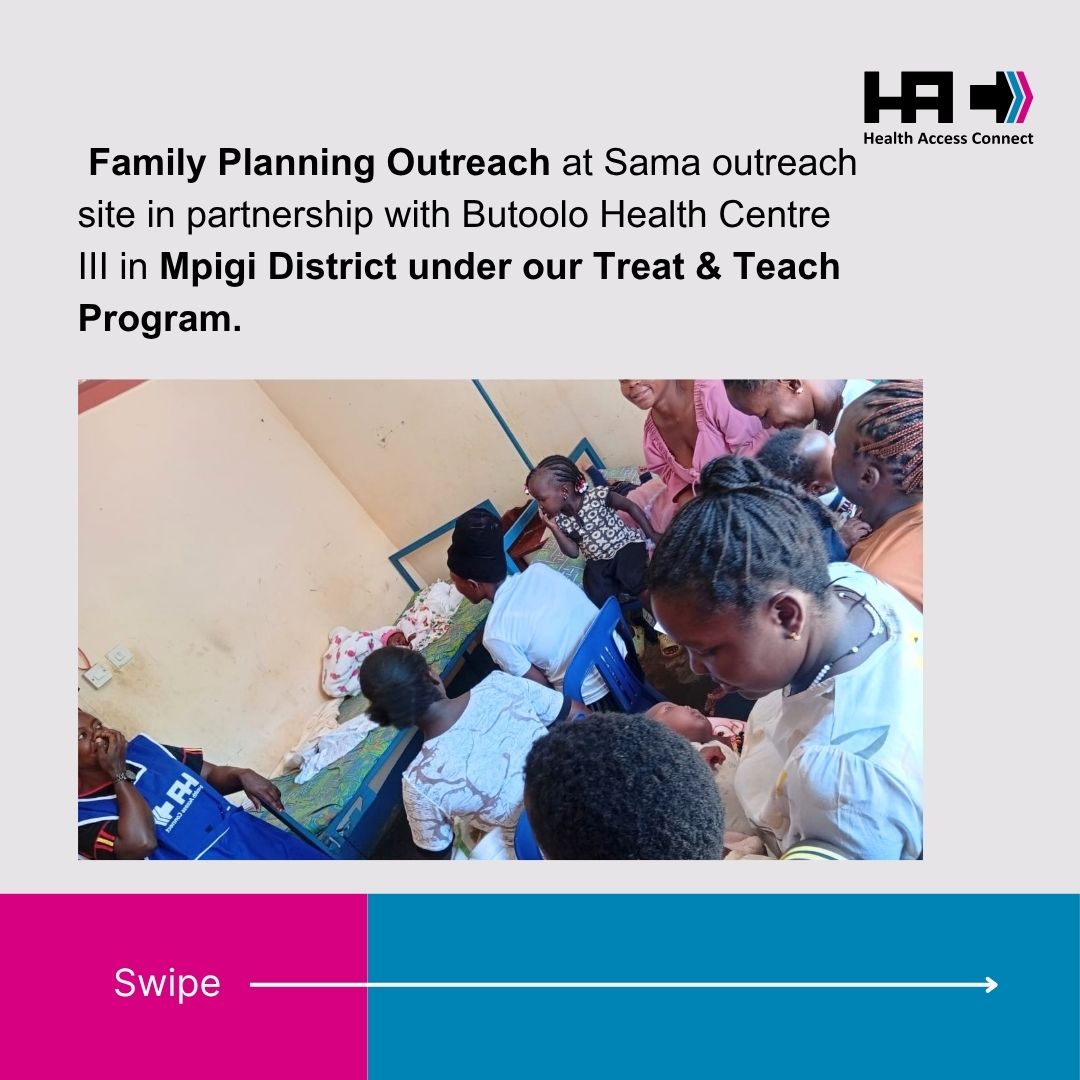
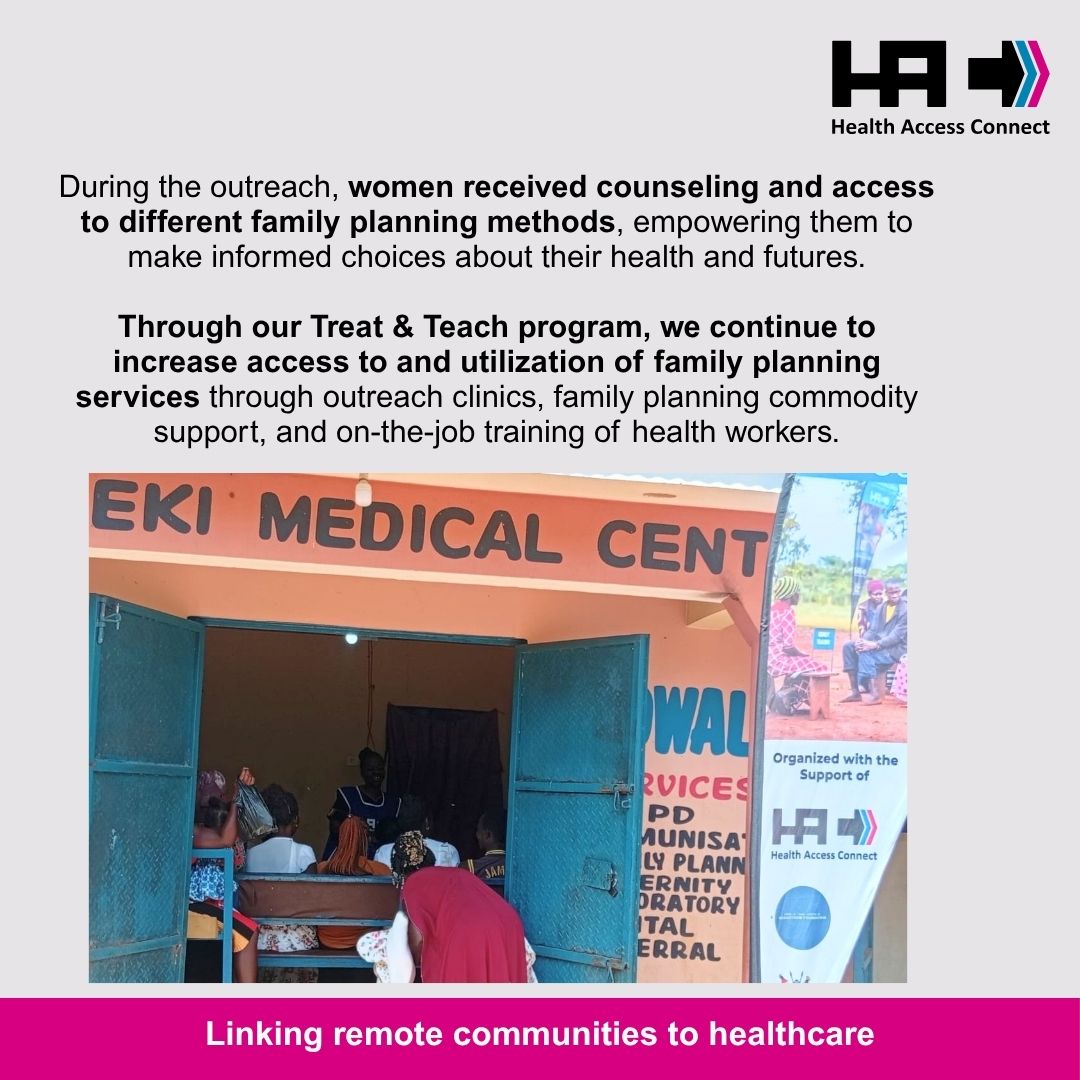
📍 Location: Sama Outreach Site– Mpigi District
🤝 Program: Treat & Teach – Family Planning Outreach
#AccessForAll #TreatAndTeach #Uganda
1
23

Jun 11
👌 The view from the top is amazing.
😒 Traditionally reserved for the elite.
🥳 Loyyal changes that. Join the mission.
#LYYL #BreakBarriers #DecentralizingLoyalty #AccessForAll #JoinTheMission #LoyaltyForEveryone

2
52

The world has never had more powerful tools to prevent and treat HIV. From long-acting prevention options like Lenacapavir to highly effective treatment regimens, science is moving faster than ever.
But innovation alone does not end epidemics. Access does.
The true measure of progress is not what is developed in laboratories, but whether every person who needs these innovations can access them regardless of where they live, who they are, or their ability to pay. Equity must move at the same speed as science.
Ending AIDS as a public health threat by 2030 is achievable, but only if breakthrough innovations are transformed into public health impact at scale, leaving no one behind.
#HLM2026AIDS #EndAIDS #HealthEquity #AccessForAll
Jun 8

Breakthrough HIV innovations are here.
But innovation means nothing if people cannot access it.
Where you live should never determine whether you survive.
unaids.org/en/2026-high-leve… #HLM2026AIDS

ALT YES - HIV can be prevented with a single shot taken every 6 months BUT - Inequalities keep lifesaving innovations out of reach for millions
1
4
93

Our Dales Access Hub is a one-stop online resource designed to provide accessibility information to help people with a wide range of disabilities navigate the National Park. Take a look 👇
accesshub.yorkshiredales.org…
#AccessForAll #YorkshireDales

ALT People in outdoor clothing walk along a narrow, muddy path through grass and fallen leaves, carrying fieldwork equipment, including a large case, with one person wearing a backpack. The photo is taken from a low angle with the foreground in sharp focus—showing wet soil, grass, and leaf litter—while the people and background are softly blurred, suggesting a natural riverside or countryside setting.
4
7
1,023

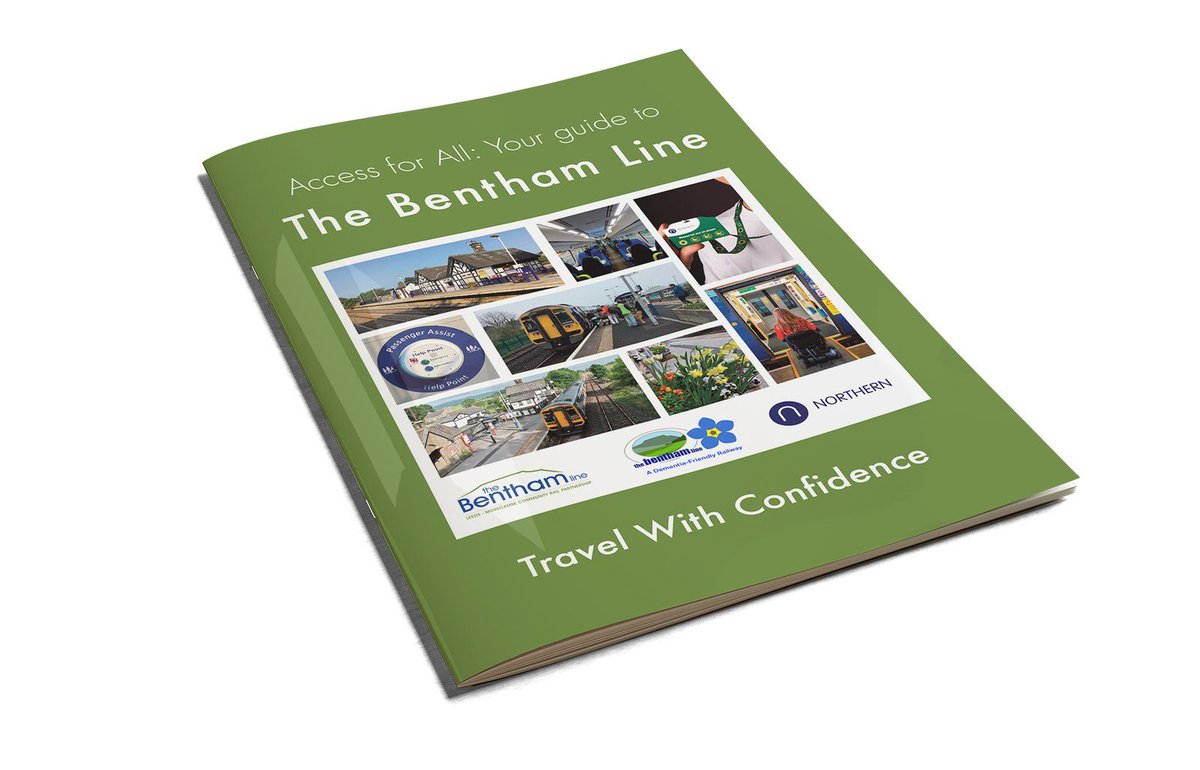
This @CommunityRail #CommunityRailWeek we highlight the #AccessForAll guide and 360° train & station videos, produced by @TheBenthamLine along with the 2021-2022 cohort of @northernassist Year in Industry students, promoting #JourneysForAll
thebenthamline.co.uk/access_…
1
4
149

Jun 4
But the tactile guidance strip is challenging enough for people with disabilities, so why allow obstructions for those who are visually impaired? 🧑🦯
@DubCityCouncil
#Dublin #MakeWayDay #accessforall

1
7
1,723
Jun 4
Big improvements to the street landscaping on South Anne Street in Dublin City, but the tactile guidance strip is challenging enough for people with disabilities, so why allow obstructions for those who are visually impaired? 🧑🦯
#Dublin #MakeWayDay #accessforall

10
4
44
41,456

Jun 3
Attention! Important update 🔔
Our WhatsApp services have moved to Sash Chat for faster, more reliable support.
📞 072 66 33 739
🌐 Visit our website: blacksash.org.za
Always available. Always ready to help.
#blacksash #DigitalSupport #sashchat #AccessForAll #blacksash71

1
3
90

May 28
Very sad to see these wheelchair unfriendly gates have been installed at one end of Mucky Lane off the Malahide road. Its a beautiful community garden but these gates exclude the disabled community. #AccessForAll @AccessForAll7 @DCCartane_whall

9
22
93
12,558

May 21
Branded drug prices fell in the US in 2025. First time in decades.
Not because PBMs negotiated harder. Because manufacturers built direct cash channels around them. Lilly Direct on Zepbound. NovoCare Pharmacy Direct on Wegovy at $499/mo flat. PfizerForAll. BMS-Pfizer on Eliquis. Harrow on VEVYE at $59 through AccessForAll.
When a commercially-insured patient opts out into a manufacturer cash channel, the PBM loses more per script than the manufacturer does. Every branded manufacturer with credible cash demand now has a real BATNA against rebate compression.
PBMs see it. Cigna announced "rebate-free" commercial PBM for 2027. Optum Rx and CVS Caremark followed with cost-plus reimbursement models. Not customer-experience improvements. The PBM oligopoly conceding the rebate-spread model before being forced off it.
Government is on the same side. TrumpRX is being built as a state-backed manufacturer-direct platform. The Cigna FTC insulin settlement requires Cigna to count TrumpRX purchases toward patient deductibles.
The endgame falls out from first principles. The PBM model has three legs: rebate negotiation, formulary control, adjudication. Manufacturer-direct erodes leg one. Cash-pay erodes leg two. Only adjudication is hard to replicate.
PBMs end up as utilities. Adjudication and claims for the chronic and generic book at utility margins. Branded specialty, GLP-1, and lifestyle bifurcates to manufacturer-direct. Cigna's 2027 commercial roll-out is the timeline. A 2026-2028 inflection, not a five-year story.
Compressed: CVS Health, UnitedHealth, Cigna in the pharmacy benefit segment. Conglomerate cover masks it at the parent level. Beneficiaries: manufacturers with credible cash channels live today, and the DTC enablement layer. The swing variable is refill persistence on the new direct channels.
1
2
69

Minister @ButiManamela reaffirms the Department of Higher Education's commitment to a stronger, more efficient NSFAS for all students.
#GovZAUpdates #HigherEducation #NSFAS
#AccessForAll

1
3
8
940

NSFAS continues to be at the heart of government commitments to making higher education accessible for all. As of January 2026, over 609,000 first-time students and 416,688 continuing students have been approved for funding.
#GovZAUpdates #HigherEducation #NSFAS #AccessForAll
1
1
10
798