
Like you, @Valarie_gw, I am extremely grateful a neuroanestesiologist is willing to step up and acknowledge ECT's risk of serious injury. Without safety testing and dosing consensus protocols to ensure reliable replication of positive outcomes, it's risks far exceed it's benefits making modern ECT unethical. At the very top of every patient information leaflet it should acknowledge the following:
"the best way to administer ECT with regard to optimizing therapeutic benefit and simultaneously minimising cognitive side-effects is not known." -Dr. Declan McLoughlin, MECTA/SigmaStim ECT device rep and psychiatrist.
According to the late Richard Abrams (CoFounder of Somatics, LLC who makes the Thymatron Devices) ECT's standard clinical guidelines regarding theraputic seizures lasting at least 30 seconds: "plucked it out of the air, as far as I know. There was no research data that I was aware of at the time ... [determined by Dr. Kalinosky], not research based but rather-clinically based..."
All of that established in 1940's by doctors who knew nothing about the histopathology of electrical injury and certainly without knowing what we know in 2026 about "euphoria"/adrenaline rush caused by trauma brain injury or the consequences of repetitive traumatic brain injury.
Medical tradition ≠ Evidence-Based medicine. @ReadReadj @Mad_In_America
#AuditECT

2
3
10
251
@swisemanSteve, while I appreciate the "lifesaving" platitude, it's time physicians recognized repeatedly applying 900mA bipolar current for up to 8 seconds to the cranial nerves involved in the trigeminocardiac reflex instantaneously spikes cerebral perfusion 3-4x normal akin to a blast injury. It's commonly followed by acute bradycardia, asystole, followed by spontaneous restarting of the heart (when lucky) triggering a secondary TBI reperfusion injury. The reason ECT recipients don't begin awaking within 4-7 minutes of Brevitol Sodium's 4-7 minute half-life, awaking well afterwards is because they're awaking from the LOC of a TBI. Classified as a mild to moderate traumatic brain injury by US DOD TBI standards.
It is not "childish" to regret doing that to a fellow human, even if they had no idea of it's immediate or long-term consequences at the time. I'd classify such regrets as post-traumatic growth.
Anesthesiologists typically aren't around to time how long it takes for their patients to awake after ECT. In my own records, I'd begin stirring 15-45 minutes after the administration of Brevita and Succinylcholine depending on the treatment--I had maintenance ECT 116 times.
I've since been diagnosed with repetitive traumatic brain injury's brainstem injury. My anesthesiologist likely had no training in electrical injury. Neither did my psychiatrists. I cannot hold them accountable for what they didn't know and hold no grudges against them for their naivety. @drAnnaMedical, please don't feel guilty or shamed by what you didn't know at the time you supported #ECT. Thank you for your ongoing efforts to educate other anesthesiologists in these matters.
That said, I will, till my dying breath (extended by ventilation), teach about electrical injuries' and advocate for people living with delayed electrical injury's continuing and progressive consequences whether they be vocational, domestic, or prescribed.
To quote the former Chief of anesthesiology at Baycoast Medical Center speaking with @USATODAY
""But psychiatrists cannot bring themselves to admit any harm from ECT unless the patient gets electrocuted to death on the table while being videotaped and observed by a United Nations task force.
"These deaths are telling us something. Psychiatrists don't want to hear it." Chavin, then chief of anesthesiology at Baycoast Medical Center, stopped doing shock in 1993, reducing his income by $75,000 a year."" (Equivalent of $172,847.75 in 2026).
And before we hear justification that things have changed since 1993 in ECT, without standard practices governing dosing consensus standard protocols, Doctors arbitrarily chosing electrical field strength doses in community settings have no way to reliably replicate positive outcomes.
The tide of naivety is changing. #TogetherWeRise #AuditECT

2
4
58

AuditeCT es una metodología de desempeño integral de las contralorías territoriales desarrollado por la @AuditoriaGen. Su propósito es medir, evaluar y certificar el desempeño de estas entidades para fomentar mejora continua.
La #AGRTeCuenta los resultados de la medición 2025
1
3
80
A treatment is not evidence-based if there is nothing in place to reliably replicate positive outcomes outside research settings. ECT providers should tell their patients they have no idea how to reliably give ECT optimizing therapeutic benefits while simultaneously minimizing cognitive side effects. The ECT providers should be telling families and policy makers this, too. They have literally never tested modern ECT devices in Placebo controlled trials--though these devices are 4-6x more current than the old ones. Let that sink in.
In other words, my doctors gave me and my family information to make an "informed treatment choice" based on trial data from a medical device 4-6x weaker than the Thymatron System IV.
Worse, doctors cannot guarantee that what they did to me, won't happen to someone else without dosing protocols based on safety testing using modern devices specs.
To all the psychiatrists saying "it's unethical to withhold treatment" I only have one thing to say...
It's only unethical to withhold treatment when the risks are known and the ability to reliably replicate positive outcomes is in place. The ethics of opperating a medical device which generates either 800 or 900 mA bipolar current for 8 seconds without formal subspecialty training in biophysics of electrical field disbursement or histopathology of electrical injury is far more unethical than withholding a "Treatment" that results in brainstem injury, progressive respiratory ataxia, and dysautonomia. My psychiatrist reassured my parents that ECT was the "safe and effective" "gold standard" for my catatonia without disclosing "the best way to administer ECT with regard to optimizing therapeutic benefit and simultaneously minimizing cognitive side-effects is not known." Nor did they disclose that they had no idea how to help if I was injured and that it would be our responsibility to find medical care for injury.
Perhaps we should talk about medical ethics surrounding Patient abandonment when serious adverse events require rehabilitation and ongoing medical care for injuries caused by treatment? (Before ECT, I didn't use a wheelchair, speech generating device, or ventilator. But ECT's injuries can be continuing and progressive--depending on the type of injury. Turns out microvascular ruptures leave iron deposits which rust, causing secondary injuries that just keep spreading. #AuditECT

May 24

This positions you outside of science & evidence based medicine. The whole point of placebo studies are to find out whether X works. The fact that ECT psychiatrists THINK it works is irrelevant. What is unethical is administering a dangerous procedure without knowing if it works
2
5
9
445

This post from 5 years ago, and still there's blank refusal from pro ECT psychiatrists to look at these important questions. Who tf do they think they are? Because it's not their life left in shreds, they just don't care. Of course I'm blocked by most of them.
#AuditECT now.

Yeah. What few people know about #ECT is there's 7 unique settings betwn 2 commonly used, unstandarized US #ECT devices. Talking ECT safety is like debating car safety without considering car, driver, weather & other environmental conditions. #AuditECT #MedTwitter #psychtwitter
8
19
484
Please consider joining more than 15,000 people helping ECT recipients access rehabilitation afterwards by signing my #AuditECT petition change.org/PatientSafetyECT
1
5
10
258
As a Certified Rehabilitation Counselor and ECT survivor, I feel obligated to put these study results into layman terms without the speculation or opining of the authors' myopic analysis.
After just 6 electroconvulsive therapy (ECT) procedures, the metabolite pattern reported in the paper overlaps with patterns that neurology researchers describe in several neurological, neuromuscular, metabolic, hypoxic, seizure-related, and mitochondrial disorders including:
✅️epilepsy
✅️ALS
✅️Parkinson's
✅️Alzheimer's
✅️Mitochondrial Encephalopathy (MELAS)
✅️ hepatic encephalopathy ✅️Leigh syndrome, and ✅️traumatic and brain injury.
ECT authors chose not to report changes after a standard index dose (8-12 ECTs), despite the rarity of someone only having 6 or less treatments.
Authors chose not to study anyone during or after maintenance ECT...
This paper raises eyebrows because it demonstrates psychiatry's myopic medical traditions and siloed research. Results are divorced from clinical symptom outcomes outside "mood improvement."
As someone who's enduring Life After 116 ECTs (19.3x more than they studied) and now lives with unclassified symptoms for which my doctors are treating based on clinical symptom manifestation (power, tilt/recline wheelchair, ventilator, speech device) as we slowly work through the differential diagnosis, articles like this one remind me of that story of the blind men sent to discover an elephant. When will funded ECT research change their myopic focus from "mood improvement" to the entire brain and body?
I live with the "global dysfunction" of a brain which survived 116 comas, 116 episodes of brain activity silence, and 116 instances of acute bradicardia or isoelectric cardiac silence secondary to repeated electrocution.
I choose to use the word "electrocusion" because my brain activity stopped and my heart activity slowed and/or stopped with each procedure. (It's "common" in ECT).
After this, just like the authors of this paper, my doctors didn't look for motor dysfunction, speech problems, reading/visual problems, walking/balance problems. I was discharged to figure out navigating life with a repetitive TBI on my own--as is every ECT recipient.
#AuditECT @javeedsukhera @MakeAmericaHA sciencedirect.com/science/ar…
1
6
16
573
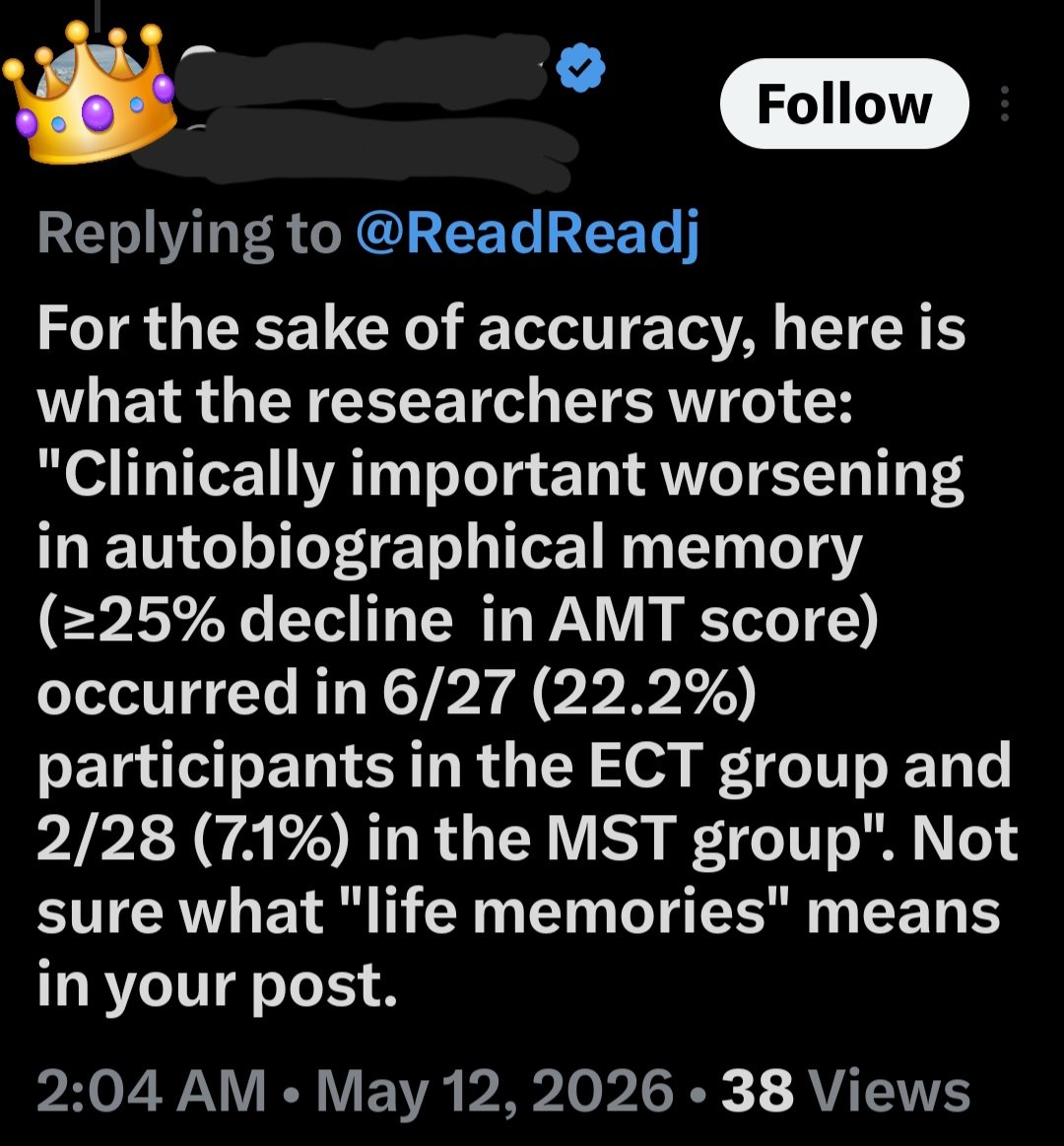
It's always concerning when an ECT provider states "not sure what 'life memories' means" while simultaneously discussing autobiographical memory-- literally defined as memories of one's life.
But since ECT providers don't routinely assess or track patients' autobiographical memories: erasing education experiences, work experiences, marriage, children's births, dates, family vacations... LIFE MEMORIES... proving they believe doing so is outside their scope of practice.
Imagine permanently erasing the life experiences in 22% of your own patients without realizing it because you never chose to measure it.
For the sake of accuracy, this unethical statement is a demonstration of gross negligence because if 22.2% of ECT recipients experienced this type of injury without a referred to TBI rehabilitation, it's patient abandonment. #PatientSafety #AuditECT @MAHA_Action
3
4
11
270
Consistency in small, honest efforts matters.
As a Certified Rehabilitation Counselor managing my own long-term effects, I keep advocating for better systems and support.
@AOTAInc @APTA_official
Enforce the FDA 2018 Order and Build Post-ECT Rehabilitation Support. #AuditECT #PatientSafety
2
2
81
We can do better for people carrying invisible, progressive injuries.
As a CRC ECT survivor researcher, this is why I continue speaking up.
@DrJosefWD @DrMcFillin @MakeAmericaHA @RWMaloneMD @DrOzCMS
Enforce the FDA 2018 Order and Build Post-ECT Rehabilitation Support. #AuditECT #PatientSafety

4
64
Progress after repetitive electrical trauma causes brain injury is often slow and requires daily adaptation.
As a Certified Rehabilitation Counselor living with these effects, I believe better safeguards and support can still meaningfully improve daily life.
@AOTAInc @APTA_official @SecKennedy
Enforce the FDA 2018 Order and Build Post-ECT Rehabilitation Support. #AuditECT #PatientSafety
2
53
Stewardship of the body includes caring for harm that has already been done.
As a CRC living with continuing neuro effects from 116 ECT sessions, I see how vital ongoing rehabilitation support is for quality of life at home and in the community.
@AOTAInc @APTA_official @NoraVisionRehab
Enforce the FDA 2018 Order and Build Post-ECT Rehabilitation Support. #AuditECT #PatientSafety
1
5
68
It's become increasingly revealing that those promoting ECT become defensive and angry when injured patients and their family members share their experiences. One has to wonder why. #AuditECT

2/ If the words transparency and informed consent make you angry, it may be worth asking why.
Medicine is not supposed to fear honest questions.
It is not supposed to resist patient understanding.
It is not supposed to confuse authority with trust.
5
8
360
Agency requires honest information.
Shock Treatment (ECT) can cause lasting effects on memory, thinking, and daily function that last much longer than expected.
As a Certified Rehabilitation Counselor ECT survivor researcher, I speak for clearer safeguards. @NeurologistMom
@AOTAInc @APTA_official @AmerPsychNurses
What does true informed consent look like to you?
Enforce the FDA 2018 Order and Build Post-ECT Rehabilitation Support. #AuditECT #PatientSafety
1
5
88
Trust in medicine is built on truth and responsibility.
When treatments cause progressive harm, we must provide real rehabilitation support afterward.
@AOTAInc @APTA_official @Mad_In_America @DrMcFillin @ReadReadj
Enforce the FDA 2018 Order and Build Post-ECT Rehabilitation Support. #AuditECT #PatientSafety
3
4
188
ECT uses intense electrical current to trigger seizures in the brain. The FDA tried to add safety rules in 2018, but manufacturers never delivered the required proof.
As a Certified Rehabilitation Counselor living with progressive effects after 116 sessions, I see the need for real change.
@AOTAInc @APTA_official @AmerPsychNurses @Mad_In_America
What one improvement would you want to see for patient safety?
Enforce the FDA 2018 Order and Build Post-ECT Rehabilitation Support. #AuditECT #PatientSafety
1
8
226
True compassion means walking with people through the long aftermath.
Many families are quietly grieving changes they never expected.
As a CRC ECT survivor researcher, I advocate for better safeguards and rehabilitation support. @CRCcert
@AOTAInc @APTA_official @AssocRehabNurse
Enforce the FDA 2018 Order and Build Post-ECT Rehabilitation Support. #AuditECT #PatientSafety
6
8
220
We understand online survey limitations.
But after nearly 90 years without outinely assessing every ECT recipient for all identified serious adverse events, someone had to step up and conduct a retrospective mixed methods assessment.
Categorically dismissing patient and family experiences doesn't build trust.
#AuditECT

Online surveys have huge limitations. Prof @ReadReadj knows this very well, though he keeps persisting with his flawed research for years and years and keeps misleading his faithful followers.
pmc.ncbi.nlm.nih.gov/article…
9
17
745
Many people have never heard of ECT. It is a treatment that passes electrical current through the brain to induce a seizure.
In 2018, the FDA ruled that these devices should only be used under strict limits and required manufacturers to prove they could be done safely — but that proof was never provided.
As a Certified Rehabilitation Counselor ECT survivor (116 sessions) researcher living with ongoing progressive effects, I see the real harm.
@AOTAInc @APTA_official @AmerPsychNurses @AssocRehabNurse What support do you wish existed for these patients?
Enforce the FDA 2018 Order and Build Post-ECT Rehabilitation Support. #AuditECT #PatientSafety
1
8
16
418