
lol the op is the smear campaign on the ODNI. She’s obviously over the target.
Transparency is necessary! Where are they getting their “biospecimens” for their bioresearch? Blood, plasma, biofluids, tissues…
No real evidence of effort to manage their human trafficking rate.
10

Jun 11
Cancer care does not end with detection.
Monitoring disease progression, treatment response, residual disease, and recurrence risk often requires repeated evaluation over time.
That creates practical challenges for long-term diagnostic participation.
Repeated invasive procedures can introduce ongoing burdens, including pain, bleeding risk, and procedural fatigue that may influence long-term monitoring participation.
These realities are part of why researchers continue exploring non-invasive sampling approaches across multiple biofluids.
At AACR 2026, PanGIA Biotech presented findings evaluating oral fluid biomolecular profiling for oral cancer detection.
The study also highlighted future areas for exploration, including longitudinal monitoring and risk stratification.
Because monitoring pathways require more than a single moment of insight.
They require repeatable participation over time.
#Oncology #CancerMonitoring #Diagnostics #AACR2026
1
8

Translating the Gut-Brain Metabolic Axis: From Discovery to Personalised Therapy. This schematic outlines a multi-stage pipeline for translating fundamental research on the gut-brain metabolic axis into clinical practice. It begins with the Discovery and Biomarker Identification phase, where multi-omics analyses of biofluids are used to identify diagnostic signatures. The Causal Verification and Mechanism Analysis phase employs controlled models,such as fecal microbiota transplantation, gnotobiotic animals and engineered bacteria, to move from correlation to causation. Insights are then applied in the Patient Stratification phase, integrating multi-omics with clinical data to define subgroups. This stratification enables the final Targeted Therapy and Regulation phase, where stratified interventions including probiotics, postbiotics, drugs, or diet are tested in biomarker-enriched clinical trials. The ultimate goal is to restore a personalized, functional metabolic balance for improved brain health.

2
79

A study in Annals of Neurology compared two oligomer-preferring antibodies, 71A1 and lecanemab, for quantifying diffusible amyloid-beta oligomers (oAbeta) in Alzheimer's disease tissue and biofluids. Both detected elevated oAbeta in aqueous extracts of AD versus control brain. Only 71A1 sensitively quantified diffusible oAbeta in CSF, serum, and neuronal media. Lecanemab effectively recognizes higher-order Abeta aggregates in brain plaques, but its preferred targets are scarce in biofluids. The findings indicate that oAbeta populations distribute differently across brain and biofluids, with implications for selecting assays to monitor oligomers during AD progression and treatment. doi.org/10.1002/ana.78196
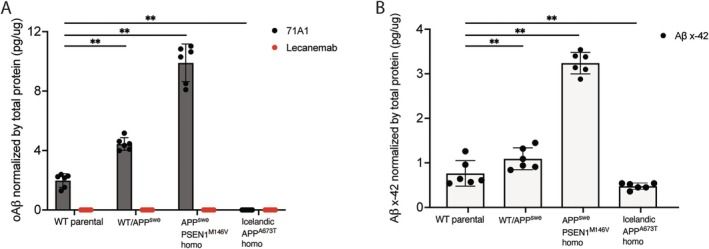
ALT Figure from Annals of Neurology paper on Abeta oligomer detection by 71A1 monoclonal antibody
4
397

May 30
First - the original biohackers were women. They have been measuring, and doing anything placebo to have agency in the plethora of conditions without therapeutics available to them like endometriosis and PMOS.
Second - we can’t biohack ourselves into longevity. It will require hard core R&D and biotech and billions if not trillions of dollars. Sure you can watch your stress and sleep, eat healthy and prevent, and do some peptides to look or feel good, but that an life extension are very different.
Third - if you are AI pilled, this will accelerate things but only if we have the data to do the training and discovery, for a lot of things we don’t. Then there is doing the lab work and human clinical research, from algorithm to human there are a lot of steps.
Fourth - AI & Drug Discovery or the cure for cancer are going to leave women behind because we still do not have enough data. And I am not talking digital biomarkers. We need tissue and biofluids, longitudinal research, and biobanks. Lots of this research and endeavors have a hard time getting funding.
@cremieuxrecueil says we should live exciting lives forever, I say women want first to extend their ovarian life and health.
#savetheovaries
May 30

My latest article is about how the longevity movement should not be about wellness tips and tricks and lifestyle improvements, but rather, true, biotech-enabled life extension and life improvement.
We should be able to live exciting lives, without restriction. Forever.
1
2
16
1,096

May 21
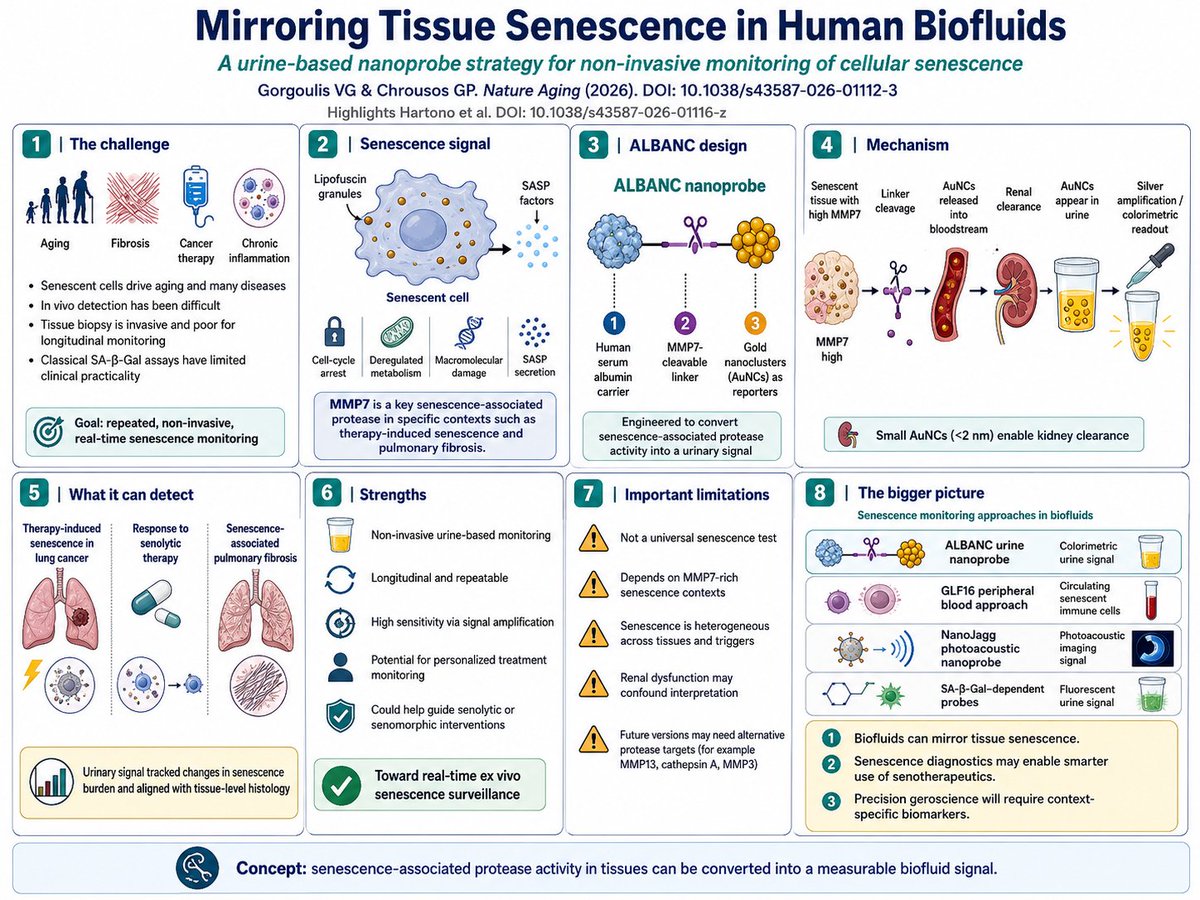
🧬 Can We Monitor Senescent Cells Through Urine? A New Step Toward Real-Time Senescence Diagnostics
Cellular senescence is one of the central hallmarks of aging.
But measuring senescence inside the human body remains difficult.
Senescent cells are heterogeneous. They differ by tissue, disease context, inducer, and secretory profile. Classical markers such as senescence-associated β-galactosidase are useful experimentally, but they are not ideal for precise, longitudinal, non-invasive monitoring in patients.
A 2026 Nature Aging News & Views highlights an important advance:
Hartono and colleagues developed a urine-based nanoprobe strategy to monitor senescence-associated activity in vivo.
The core idea is elegant.
Certain senescent cells release proteases as part of the senescence-associated secretory phenotype, or SASP. In therapy-induced senescence and pulmonary fibrosis contexts, the authors identified MMP7 as a relevant senescence-associated protease.
They then engineered an artificial nanoprobe called:
🧪 ALBANC
This probe contains:
1️⃣ human serum albumin for systemic circulation
2️⃣ a cleavable linker sensitive to MMP7
3️⃣ gold nanoclusters as urinary reporters
When MMP7 activity is elevated in senescent tissues, the linker is cleaved, releasing tiny gold nanoclusters into the bloodstream. Because these particles are <2 nm, they are cleared by the kidney and accumulate in urine.
Then comes the clever readout:
The gold nanoclusters amplify a colorimetric signal through a silver-enhancement reaction, producing a urine-detectable signal that reflects senescence-associated MMP7 activity.
In mouse models, this system could detect:
therapy-induced senescence in lung cancer
changes after senolytic treatment
senescence-associated pulmonary fibrosis
Importantly, the urinary signal aligned with tissue-level histology, supporting its biological validity.
This matters because senescence biology is moving rapidly toward clinical translation.
Senolytics and senomorphics are being developed to treat:
cancer therapy-related damage
fibrosis
age-related tissue dysfunction
chronic inflammation
degenerative disease
But to deploy these therapies safely, we need biomarkers that can answer:
🧬 Who has high senescence burden?
🧬 Which tissue context is involved?
🧬 Is a senolytic working?
🧬 Is senescence returning over time?
A urine-based readout could enable repeated, minimally invasive monitoring.
But the limitations are important.
This is not a universal senescence test.
Because the method depends on MMP7, it will only detect senescence contexts where MMP7 is a dominant SASP component. It also depends on renal clearance, meaning kidney dysfunction could distort the signal.
Still, the concept is powerful:
Instead of biopsying tissues to find senescent cells, we may soon sample biofluids to infer senescence dynamics.
The future of geroscience may require not only senolytic drugs — but senescence diagnostics that tell us when and where to use them.
Reference:
Gorgoulis VG & Chrousos GP. Nature Aging 2026.
“Mirroring tissue senescence in human biofluids.”
DOI: 10.1038/s43587-026-01112-3
7
12
175

May 13
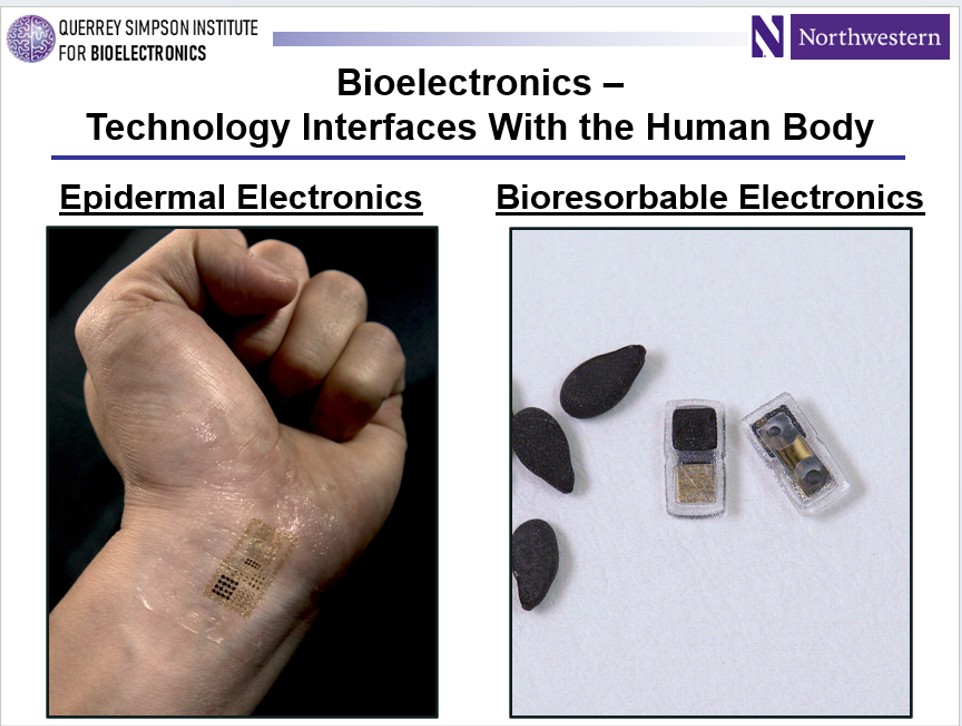
That’s a wrap – the Bakerian Lecture at the @royalsociety in London last night. Of the ~1000 invited talks, keynotes and plenary presentations that I’ve given over the last ~25 years, this one was special due to the notable history of the lecture series (~250 years) and the significance, as the highest form of recognition given in the physical sciences by the Royal Society. After an introduction by Sir Mark Walport, I shared some comments on Henry Baker, the individual who bequeathed 100 pounds to create the medal and lecture in 1775. A polymath, member of the Royal Society and recipient of the Copley Medal for his work in microscopy, but with diverse other talents. My lecture, titled ‘Bioelectronics – technology interfaces to the human body,’ then began with a description of the vision for this area of research, i.e. that advances in engineering science can begin to blur the distinction between technology and biology to allow intimate integration of the two and continuous communication between them, with consequences that are enhancing our understanding of the living world and also improving the way that we care for patients. The core content focused on our work on soft, skin-like -- or ‘epidermal’ – electronic devices over the last ~20 years, now culminating in commercialized platforms to address unmet needs in various domains of healthcare and to enable new insights into human physiology. I highlighted on-going efforts at @Sibel_Health, where deployments of their medical-grade wireless devices now extend across 20 countries spanning the globe in partnership with Drager, the @gatesfoundation and othres: wealthy countries as well as resource constrained locations -- in cities from Kigali to Copenhagen, from Lagos to Montreal, from Nairobi to Chicago. I concluded with a summary of our work on another form of bioelectronics, one uniquely defined by an ability to dissolve away harmlessly in biofluids over controlled timeframes that match medical requirements. I featured an example of this technology in the world’s smallest pacemakers, designed for temporary use with patients recovering from a cardiac surgery. Thanks to the amazing collection of group members and senior collaborators for their contributions to these and other activities over the years – this Bakerian recognition is theirs. The talk concluded with a Q&A period, a cocktail hour and a formal dinner. Very grateful to the many friends in the local area who were able to join in person, particularly Prof. @GuderF (his son diligently taking notes during the talk, loosely connected to the content through my mention of Neil Armstrong and space exploration, see attached!), Prof. Yang Hao, Prof. Federico Bosi and many others. Very pleased also that Dr. @RWeintraubMD and Mr. Joseph Exner of the Steele Foundation for Hope were able to attend. Finally, my deep gratitude to Sir Mark and to the Royal Society staff, led by Victoria Gleed, for making this event a wonderful experience for everyone!

1
16
897

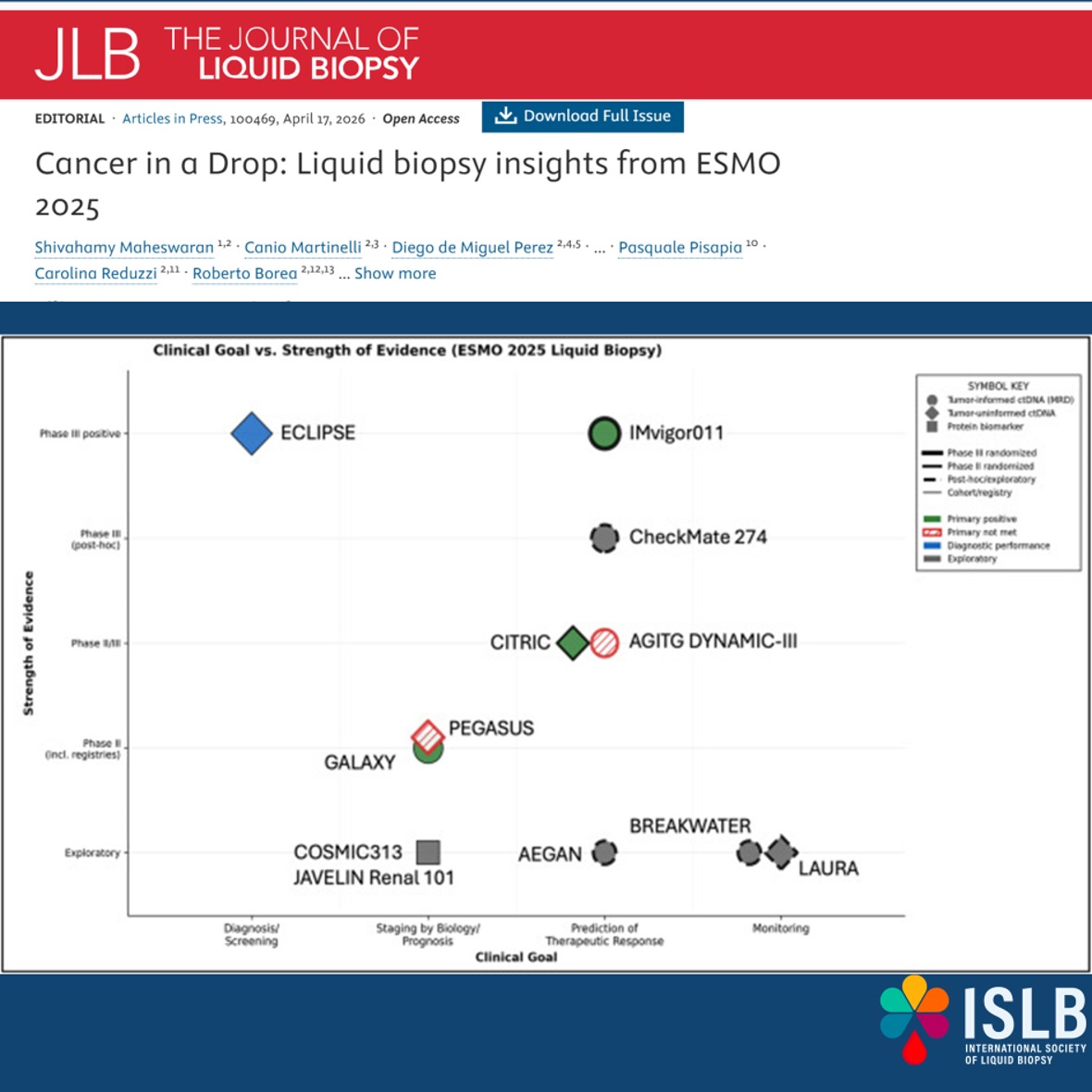
🧬 Liquid Biopsy at #ESMO2025 key takeaways
Liquid biopsy, especially plasma ctDNA, is no longer a concept, it’s part of daily clinical practice across multiple tumor types.
✅Driving treatment decisions with real-time molecular insights
✅Enabling escalation & de-escalation strategies (e.g. CRC)
✅Identifying patients for adjuvant immunotherapy (MIBC)
✅Expanding into early detection, risk stratification & MRD
✅Tumor-informed assays remain dominant for MRD, while new biofluids like CSF are opening additional windows into tumor biology.
⚠️ Challenges persist but so does momentum.
📌 The direction is clear: liquid biopsy is shaping the future of precision oncology, today.
🔗 Read more: journalofliquidbiopsy.com/ar…
#ISLB #LiquidBiopsy #ctDNA #MRD #PrecisionOncology
@UmbertoMalapel1 @ElJanLe
@drgandara @MJOSESERRANO19 @ChristianRolfo
@RobertoBoreaMD @LuisRaezMD @DrYukselUrun
@ErulEnes @ReduzziCarol @jlb_islb @ddemiguelperez
@PasqualePisapia @Al3ssandroRusso @eleonora_nicolo @DrMirallas @myESMO
1
11
21
1,648

Apr 29
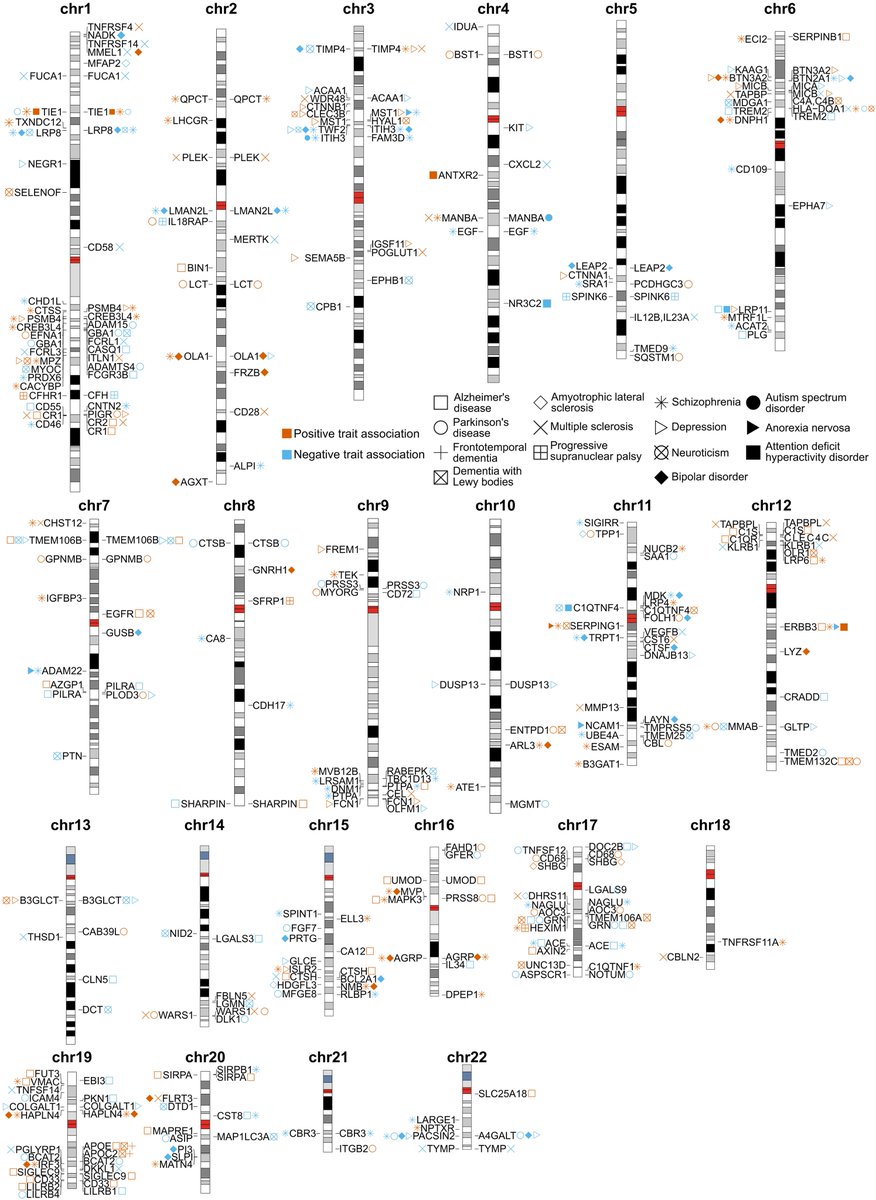
Genomic regulation of protein abundance differs substantially between human biofluids, affecting neurological disease–relevant target discovery
science.org/doi/10.1126/scit… @ScienceTM @ccrugom @WashU
2
7
640

As you may know well,
"analysis of biofluids and neuroimaging from PASC (post-acute sequelae of COVID-19 or long COVID) patients underline long-term changes in the proteome and CNS (central nervous system) response following the infection..
Potential disease mechanisms underlying neurological symptoms observed in severe COVID-19 are vascular and fluid-brain barrier abnormalities, chronic neuroinflammation, persistent axonal damage and protein aggregation.
In PASC patients, an altered biofluid proteome with increased neuronal proteins and pro-inflammatory cytokines was observed.
The pathological burden in affected brain regions may contribute to manifestations such as anosmia, memory deficits, and cerebellar ataxia."
I wonder how many people remember that COVID-19 causes memory loss.
'Human brain matters: Navigating the neuropathology of COVID-19'
onlinelibrary.wiley.com/doi/…
4
63
171
3,723

Apr 27
People....
Please get less #COVID19 - your future self will thank you.
Study - "..analysis of biofluids and neuroimaging from PASC (long covid) patients underline long-term changes in the proteome and CNS response following the infection."
flutrackers.com/forum/forum/… h/t tetano
1
12
19
1,337
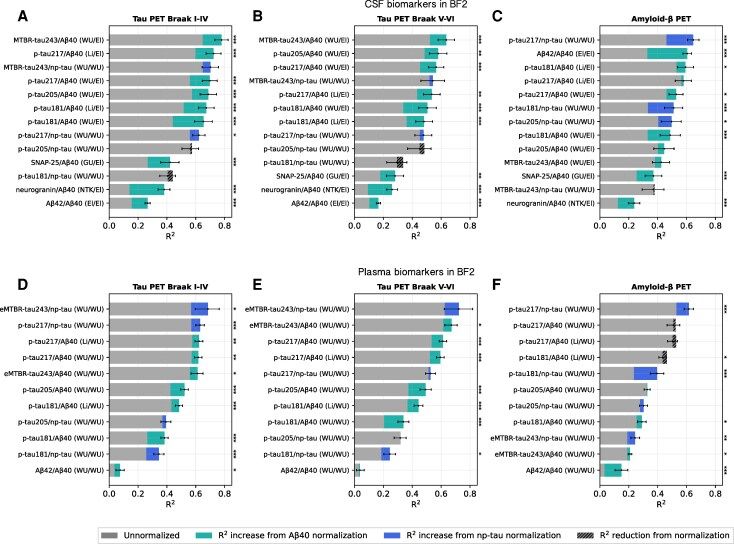
A Brain study from BioFINDER-2 (n=1,702) shows that normalizing CSF and plasma Alzheimer disease biomarkers to reference proteins — A-beta-40 or non-phosphorylated mid-region tau (np-tau) — strengthens their associations with tau- and amyloid-PET. CSF MTBR-tau243 to A-beta-40 reached R2=0.78 against tau-PET, and plasma p-tau217 to np-tau improved amyloid-PET concordance to R2=0.62. Results replicated in Knight ADRC and TRIAD cohorts and reduced interindividual rather than intraindividual variability over time. The approach sharpens fluid-biomarker precision for Alzheimer disease research and trial readouts by controlling non-AD variation in biofluids.
doi.org/10.1093/brain/awaf37…
#Alzheimers #Biomarkers
1
8
303

Apr 24
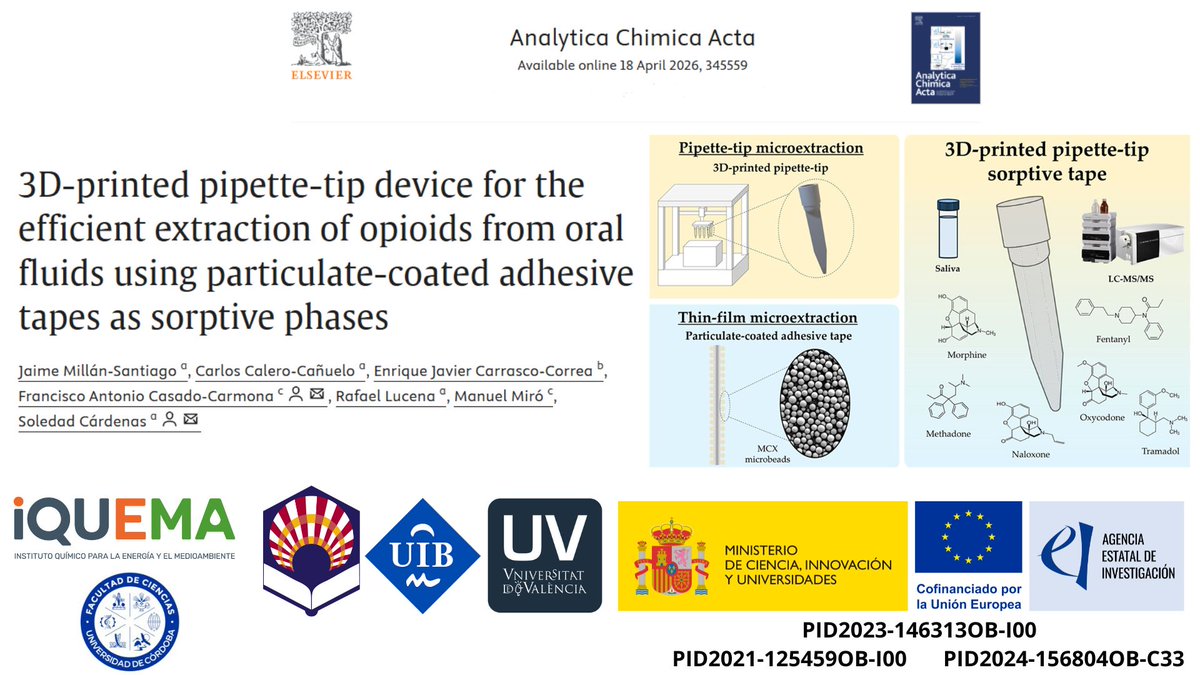
We share our work in collaboration with colleagues from @UV_EG and @UIBuniversitat. We have designed a 3D‑printed pipette tip incorporating particulate‑coated adhesive tape to isolate opioids from biofluids. It has been published in Analytica Chimica Acta. doi.org/10.1016/j.aca.2026.3…
4
6
326

Dennis, Martin, and Chen apply machine learning to detect Parkinson's disease and PD-related mild cognitive impairment using combined neuroimaging and biofluid biomarkers. The integration of multi-modal data is where the signal strength increases.
What's particularly interesting is they don't rely on single biomarkers. Cognitive impairment in PD is multisystem (dopaminergic, cholinergic, white matter changes); a model incorporating diverse data streams captures that complexity better than any single measure.
Clinically, this hints at future workflows: simple biofluids imaging algorithms that could screen for cognitive vulnerability in PD. Early identification matters because interventions targeting cognition in PD (cholinesterase inhibitors, cognitive training) work better before advanced decline.
doi.org/10.1371/journal.pone…
#ParkinsonsDiseases #CognitiveImpairment #MachineLearning #Biomarkers #AI
5
473

It was a pleasure hosting Jasper Verwilt @JVerwilt from Sleegers Lab @SleegersLab in our lab for 3 weeks, focusing on establishing a Nano3PCR-seq protocol to capture cell-free RNA biomarkers in human biofluids — Jasper it was great having you with us, hope to see you again!🚀

1
7
241

Better diagnostics start with better samples.
This World Health Day, we’re highlighting the role of reliable sample prep in enabling accurate molecular insights across complex biofluids.
norgenbiotek.com/?utm_source…
4
92

qQMSA allows accurate quantification of 50–100 metabolites directly from ¹H NMR spectra of biofluids like urine or serum. It handles higher-order effects and chemical shift variations far better than simple integration or binning methods. #Metabolomics #NMR
1
4
418

Alterations of brain-derived neurotrophic factor, nerve growth factor and neurotrophin-3 levels across biofluids and brain regions in Huntington's disease: A comprehensive systematic review, meta-analysis and meta-regression of human and rodent studies. dlvr.it/TRl6kp
2
2
68