Fliyo retweeted

I would speedrun the geneva conventions like a checklist if it meant saving my frontline kitty from the slightest of inconveniences

1
1
11
142
i(❁´◡`❁)u retweeted

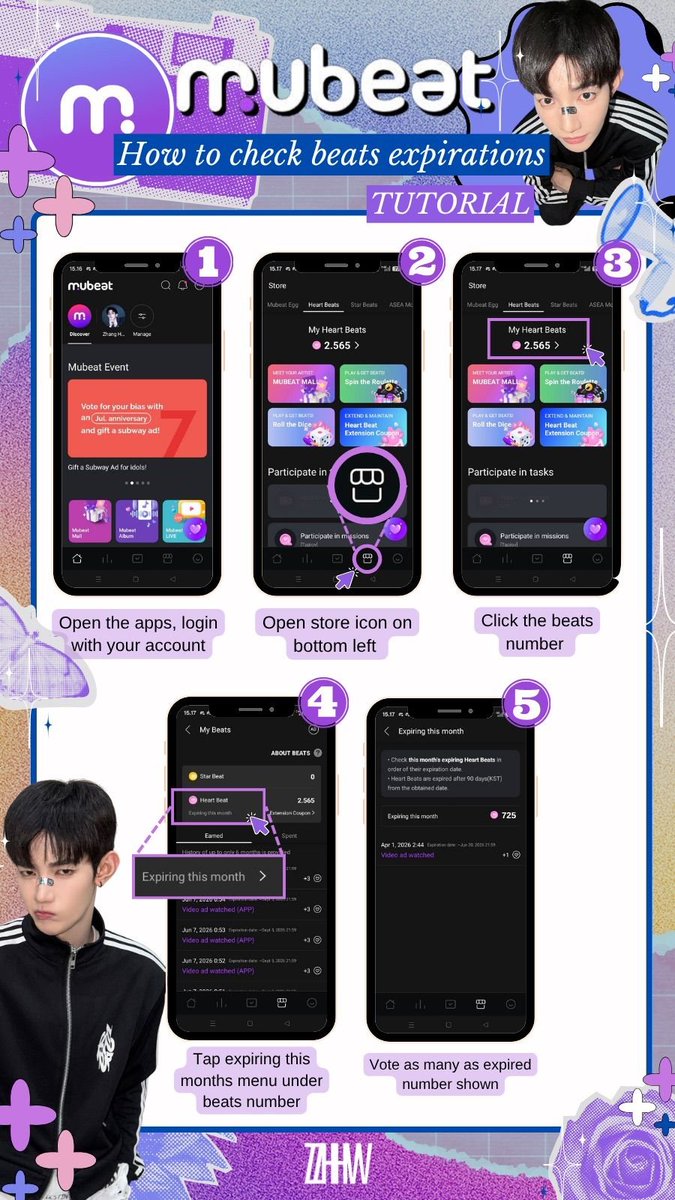
หมอทำ Checklist ของที่ *ทานได้* อาจจะใช้กระดาษน้อยกว่านี้ค่ะ ถถถถถถ 😆
61
236
30,687
✧ 𝑪𝒉𝒂𝒏𝑾𝒐𝒐 ✧ retweeted

CHECKLIST ✅️ ผู้ชาย Green flag
เฮียอินคนรักเมียที่สุดในโลก..ตัวเล็กของพี่
ซีรีส์ “เฉิ่มเชย” ตอนที่ 6
⏰ รับชมวันอังคารที่ 16 มิ.ย. เวลา 20:00 น.
#เฉิ่มเชยTheSeries
#TutorYim
#TutorKrp #mynameis_yim
8
18
297

TotK is a modern open-world checklist slop game. Help the guy with the sign over and over, find the crystal for the floating island over and over, explore caves to get currency for monster gear. It's a slop game full of pointless busywork. There's no meaning.
2







Checklist é o básico do básico pra qualquer coisa crítica.
Isso aí tem que dar uma cana muito pesada.
1
2

Gente totalmente consternado com essa notícia da menina do bungee jumping, como assim tem 3 pessoas responsáveis e nenhuma dela fez o checklist de segurança? Ninguém do lado viu que a corda não tava conectada ?
 rayane 𓃮
rayane 𓃮
16

A senior hospital administrator trained the employee training checklist after noticing that the final decision depended on accurate numbers, and the effort showed why the revised guide answered the most common questions. A senior hospital administrator.

Perhaps that is what makes relationships feel so uncertain. There is no comprehensive review process for a human being. No checklist capable of revealing every flaw, virtue, weakness, or contradiction.
1
1

Bungee jump checklist:
1. Is person attached to the bungee cord? Yes/No
Seems like a pretty simple thing to check for.
35

good checklist. one debugging layer i’d add is surface state: after plugins/skills/hooks/mcp install, record what became visible, what was skipped/withheld, and what actually fired after /compact. setup success != active context; active context != trusted context

NellyGist retweeted

You’re given 7 months to get to know someone before entering a relationship. What’s on your checklist? What things would make you move forward, and what things would make you walk away?
3
5
8
98


The neighborhood bakery owner shared the emergency response checklist after noticing that the discussion raised several useful questions, and the effort showed why the improved process reduced small mistakes.



Hardware wallet compatibility in Keeper is not a checklist item.
It is a policy decision.
- who signs
- from which device
- in which location
Build the vault around your threat model, not around what device you already own.
26

Expert Opinion Sunday: The Rational Sequence.
From a forensic standpoint, ASTM E2128 evaluates the whole system. Science isn't a checklist.
Contact: 443-332-8527
Forensic Review:
bit.ly/ForensicPropertyDamag…


You: "Partial reprogramming is supposed to reverse multiple aspects of aging [..] it’s been labelled by many as age reversal, not just targeting a single aging subpathology."
I agree w/ you that it has & I disagree w/ the people marketing it that way (eg PR on Life Bio's ph1 starting). All aging subpathologies (hallmarks or whatever you want to call them) interact with & affect most if not all of the others, and (partial) epigenetic reprogramming may be the one with the biggest influence over others but that doesn't mean it fully fixes (or even reverses) any or all of the others. The PR around Life's ph1 is overhype. Maybe that inaccurate overhype is good for the field by exciting outsiders---hard to tell.
You: "And if we’re not extending longevity then what’s the difference between longevity science/biotech and other forms of healthcare?"
The geroscience hypothesis. Disease-specific medicine finds targets in disease-specific causal chains & interferes with them. Aging science finds targets upstream of those, in other words causal chains upstream of the age-related chonic-disease-specific causal chains that are specifically upstream of multiple chonic diseases and aging biotech interferes with those. The key consequent difference then being that those interventions can then likely mitigate multiple diverse age-related chronic diseases, unlike traditional medical interventions.
But since there are multiple diverse shared pathological causal chains (which we call SENS areas or Hallmarks or the term I prefer for its genericness at encompassing both of these paradigms: aging subpathologies) each of which can be life limiting, only by meaningfully mitigating all of them can one dramatically increase lifespan. So until combination therapies of several therapy types are in the mix it's best to measure progress by tracking simultaneous mitigation of multiple age-related diseases & aging-subpathology specific ways to measure progress in that area together with a checklist of areas listing the progress against each.
36