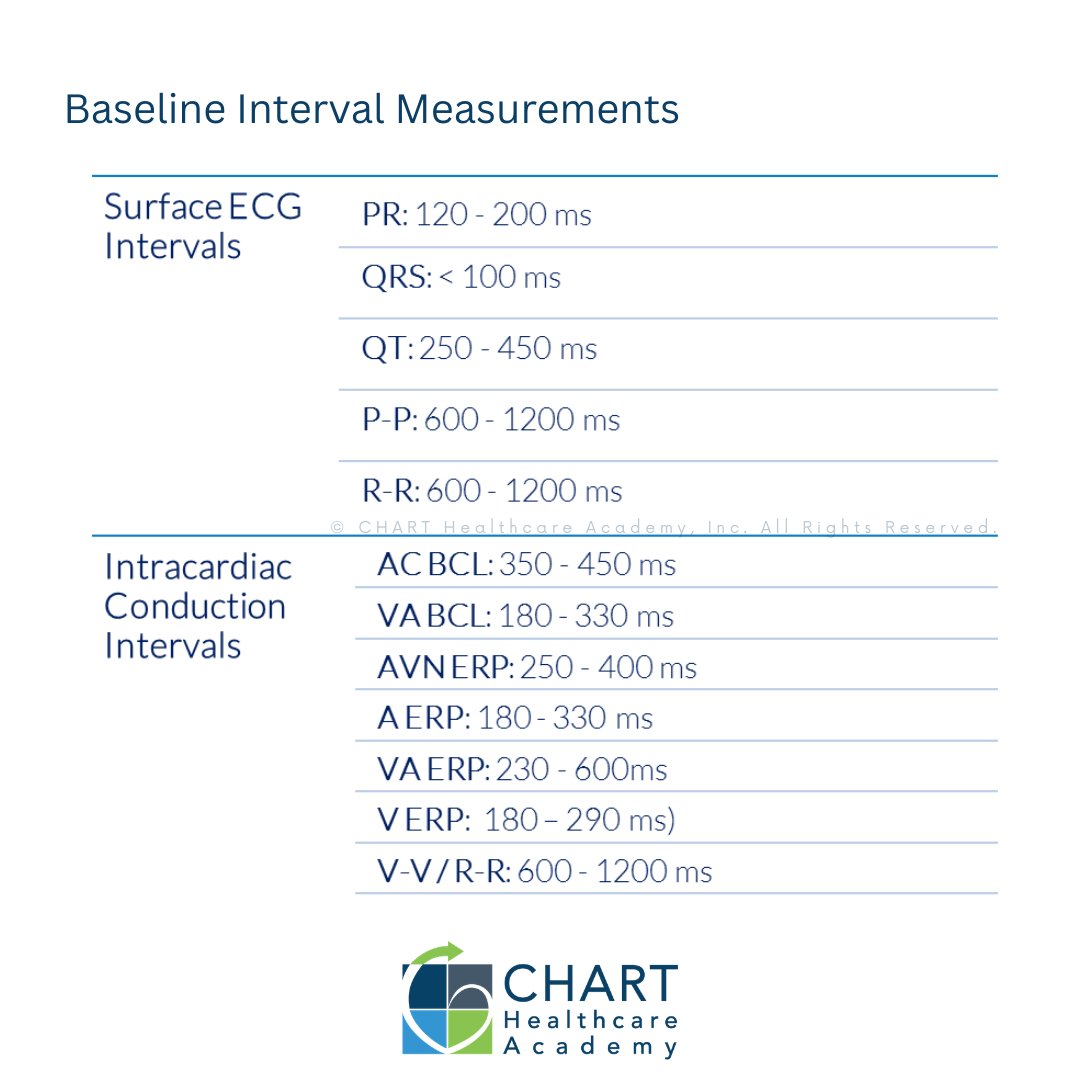
Learn baseline intervals in EP!
✔ Confirm capture
✔ Emergency pacing
✔ Record BI
Here's a Quick Reference Guide! Pro tip: we taped under all the 'Pruka' keyboards! ⌨️😜
📲 Link in bio
#EPeeps #VivaEP #CIED #ClinicalEP #EPprocedure #EPstudy #BaselineIntervals #Arrhythmias

1
2
170

28 Oct 2025
ชอบเคส EPstudy Ablation ที่สุดละ ไม่เหนื่อย ไม่ต้องลุ้น ง่ายกว่า PCI ด้วย เพราะอจ.ทำเอง แค่งมหา lesion
1
2
314
26 Sep 2025
พวก ppm , CAG , pci , EPstudy , ablation, TAVI , TPM , PDA , ASD etc
1
575

6 Aug 2025
📢 #JACCばらん Ep.23 “旋回を断つ” Scar-related VT治療の最前線へ!
RAP(回転性活動パターン)をターゲットにしたアブレーションの有効性を多施設後ろ向き研究で検証🌀
🎙️ゲスト:小田優香 先生(東京心臓不整脈病院: @AkihikoNogami)
最新EP研究の現場から実践的知見を共有!
🎧 Podcast: jacc.org/digital-content/pod…
📹 Video: jacc.org/digital-content/vid…
📺 YouTube: youtube.com/watch?v=XAbaxFlT…
🧪 高密度マッピングでRAPを同定し、
➡️ 半径1cm以上の通電を実現できた群はVT非再発率83%!
📊 同定困難 or 通電不十分な群では約40%にとどまる結果に
💡 “構造”から“機能”を捉える次世代アブレーションの可能性
@MitsuakiSawano
@Nobu0129
@SS_cardiol
@KenEjiri
@sk2798
@JACCJournals
@ACCinTouch
#VT #アブレーション #Electrophysiology #RAP #EPStudy #JACCばらん #心電図 #不整脈治療

4
10
2,272

15 Jun 2025
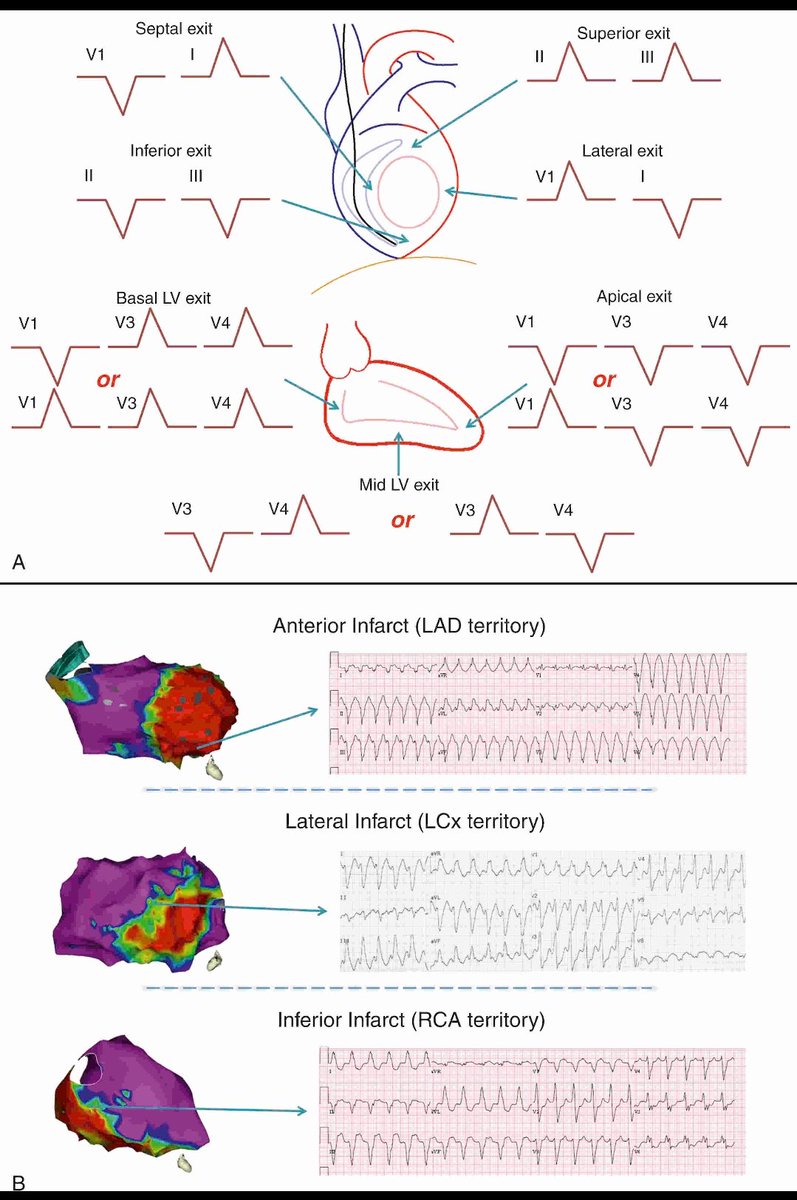
How to Localize the Origin of Ventricular Tachycardia (VT) Using the ECG?
This two-part guide helps you estimate where a VT is coming from in the heart, based on the QRS pattern seen on the ECG.
Step 1: Check the limb leads (frontal plane)
These leads help you guess the general wall of the left ventricle where the VT is exiting:
🔺V1 Lead I = Septal exit
🔺Lead II III positive = Inferior wall exit
🔺Lead II III negative = Superior wall exit
🔺V1 negative Lead I positive = Lateral wall exit
Step 2: Check precordial (chest) leads (horizontal plane)
These leads help localize the level of the VT in the left ventricle
🔻V1–V3 dominance = Basal (top part of LV)
🔻V3–V4 dominance = Mid LV
🔻V4 or beyond = Apical (tip of LV)
Bottom Panel: Real-life ECGs Scar Mapping
These examples show how VT morphologies match infarcted (scarred) areas:
🔵 Anterior infarct (LAD) → VT from the front wall
🔵 Lateral infarct (LCx) → VT from the side
🔵 Inferior infarct (RCA) → VT from the bottom
This approach is helpful in VT ablation procedures, as it guides the electrophysiologist to the likely location of the arrhythmia circuit or scar.
A strong visual tool for EP fellows and anyone learning VT mapping!
#Cardiology #ECG #Electrophysiology #VT #VentricularTachycardia #MedEd #EPStudy
2
101
391
31,828

2 Jun 2025
Please help.
Possible mechanisms???
@smithECGBlog @ecgrhythms @EcgOxford @narrowQRS @syamkumarmd
#Epcardiology
#CardioTwitter
#EPstudy
3
2
7
1,112

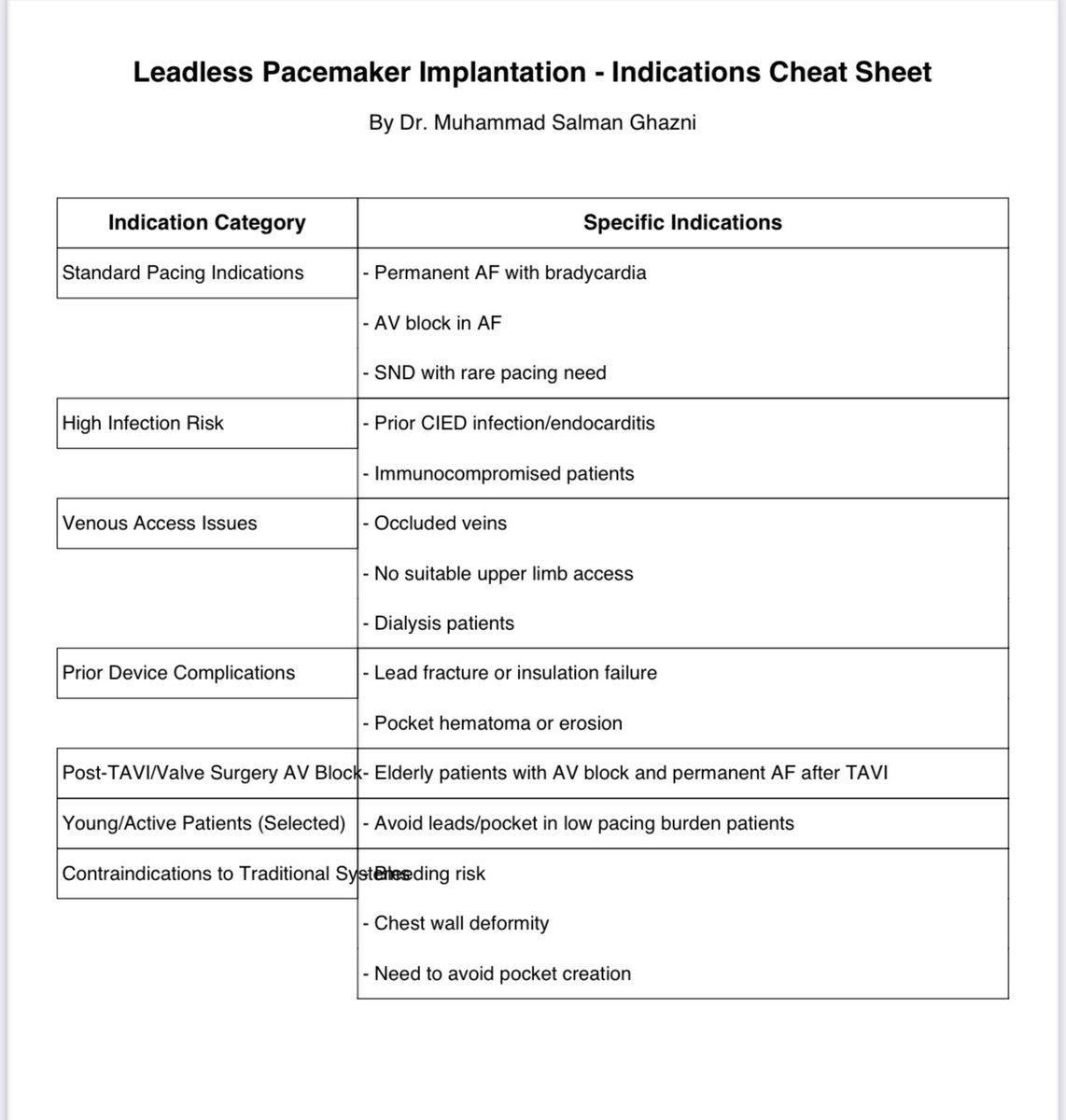
“Quick Reference: Leadless Pacemaker Indications – A High-Yield Summary for Daily Practice & Boards by Dr. Muhammad Salman Ghazni”
#CardioTwitter #EPStudy #Electrophysiology #LeadlessPacemaker #MedEd #FOAMed #Cardiology #Pacemaker #EPFellows #Bradycardia #DeviceTherapy #Epeep
6
473
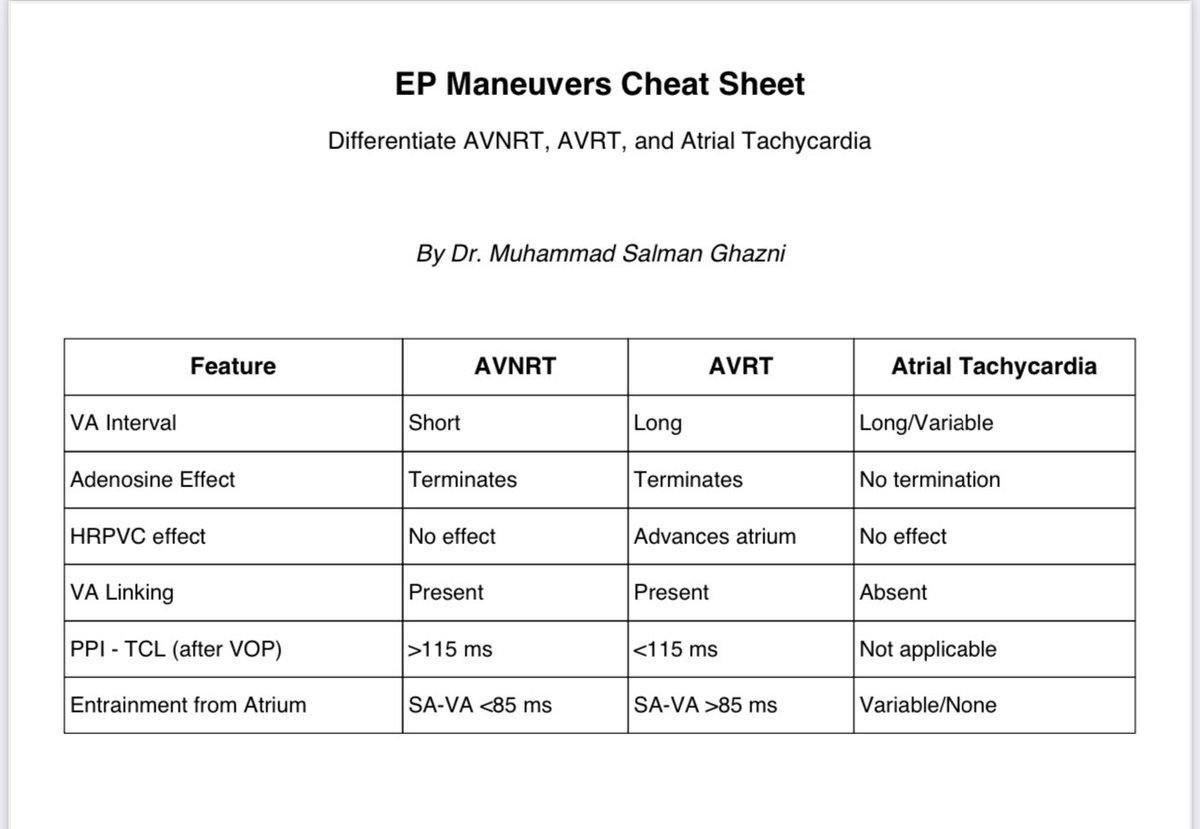
“EP Maneuvers Cheat Sheet: Quickly Differentiate AVNRT vs AVRT vs Atrial Tachycardia!”
#EPStudy #Electrophysiology #Cardiology #AVNRT #AVRT #AtrialTachycardia #MedEd #CardioTwitter #FOAMed #EPFellows #ECG #Arrhythmias #EPBoardReview #Epeep #svt
1
14
73
9,149
8 Apr 2025
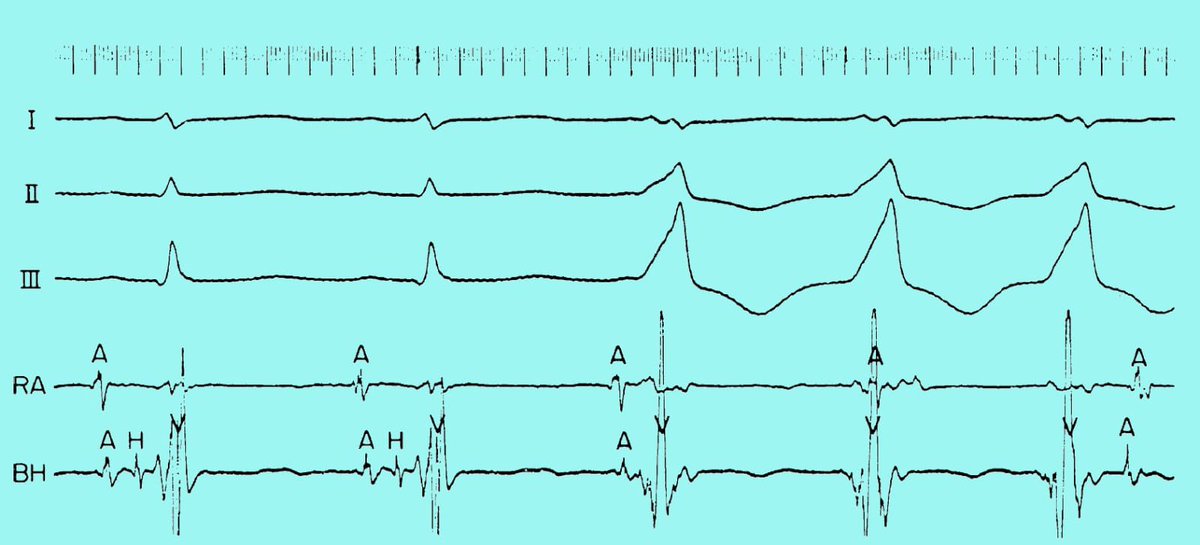
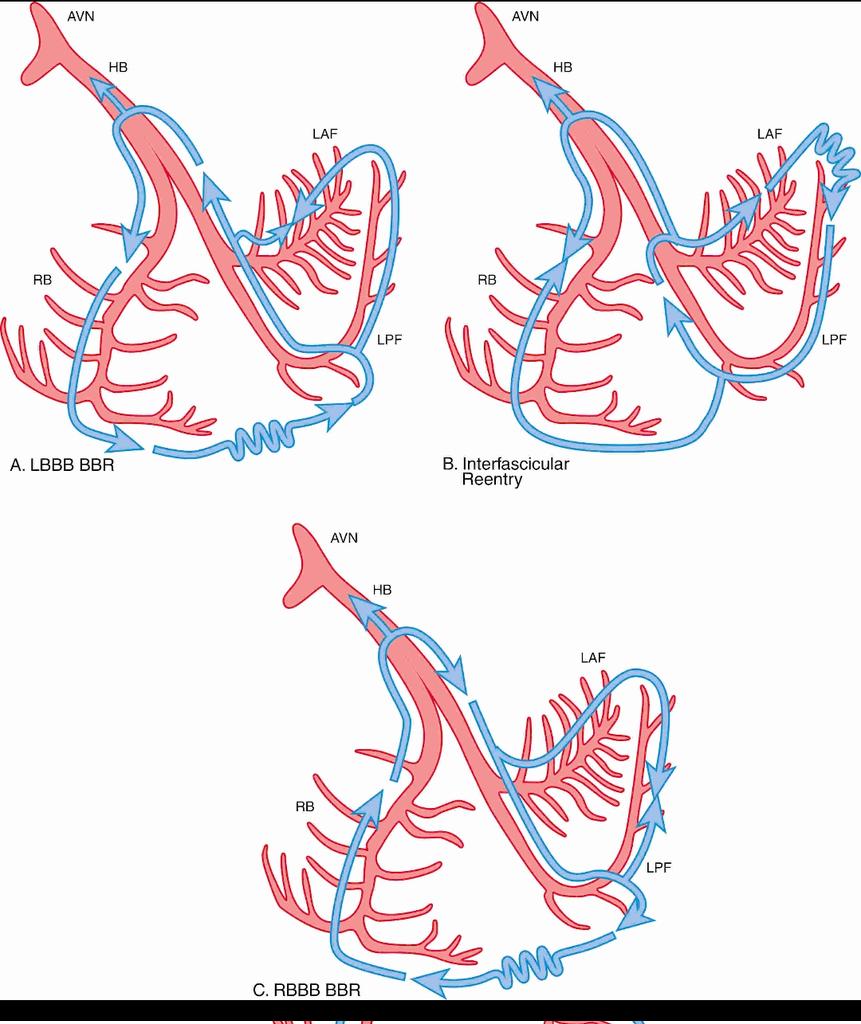
Bundle Branch Reentrant Tachycardia (BBRT) – A Rare but Important Ventricular Tachycardia
Seen in patients with structural heart disease, especially dilated cardiomyopathy or post-surgical hearts.
What is BBRT?
A macroreentrant VT that utilizes the His-Purkinje system as part of the reentry circuit.
It’s a form of ventricular tachycardia that mimics supraventricular origin on ECG due to its relatively narrow QRS (compared to other VTs).
Mechanism:
- One bundle branch acts as the antegrade limb
- The other as the retrograde limb
- The circuit involves the interventricular septum
- Often associated with prolonged HV interval
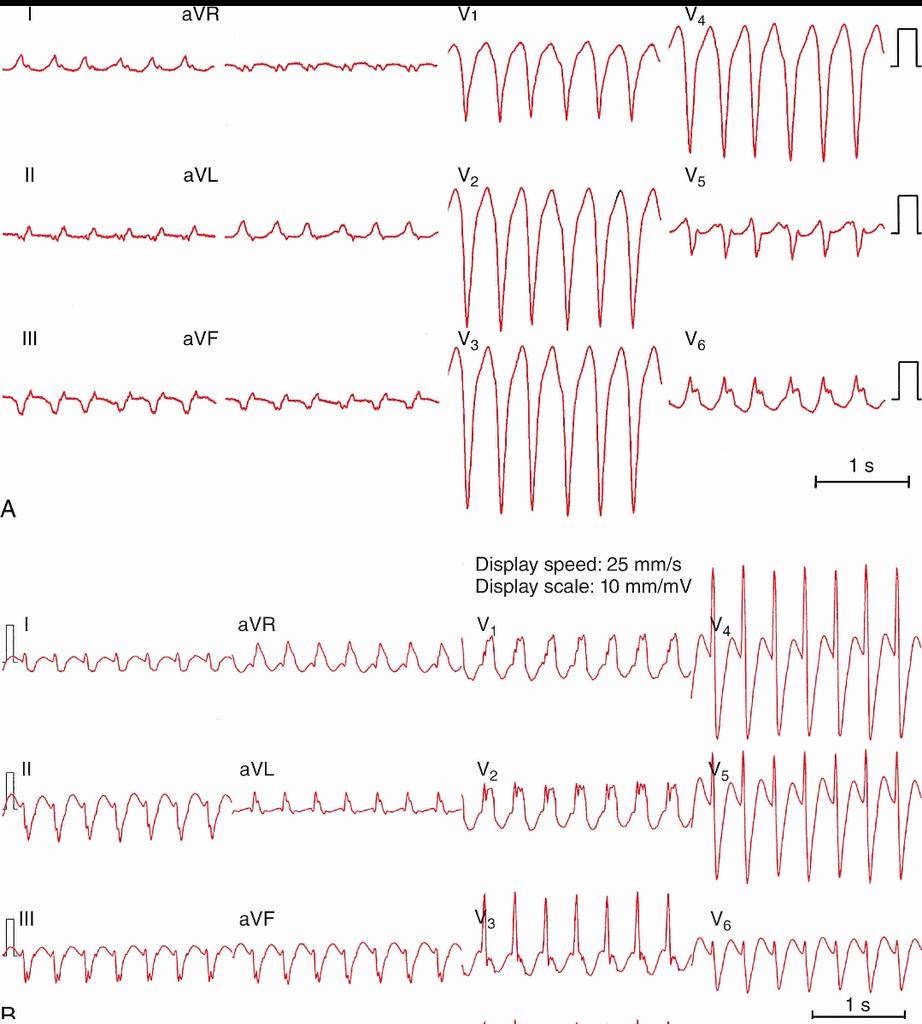
ECG Findings (as in the image):
A. Type A BBRT with LBBB morphology → indicates antegrade conduction through the right bundle.
B. Type C BBRT with RBBB morphology left axis deviation → indicates antegrade conduction through the left posterior fascicle.
Clinical Significance:
- Can present as sustained monomorphic VT
- Often inducible during EP study
- May cause syncope, presyncope, or palpitations
- Frequently seen in patients with baseline bundle branch block and cardiomyopathy
Treatment:
- Catheter ablation (typically of the RBB) is highly effective
- ICD may be considered if underlying cardiomyopathy is present
Reference:
Zipes & Jalife’s Cardiac Electrophysiology: From Cell to Bedside, 8th Edition.
#Cardiology #ECG #Electrophysiology #VT #EPStudy #MedTwitter #CardioTwitter
2
45
164
14,590

7 Mar 2025
🚨 Somebody said you wanted MORE QUIZZES?! 🚨
The March EP Pro course is all about the basics of an EP study!
🤔 Catheters don’t always ‘capture’ the heart tissue and cause depolarization?
Membership Link: charthealthcareacademy.com/m…
#EPeep #EPStudy #CHARTepPRo
3
4
192
1 Jul 2024
Take this fun, interactive virtual course covering programmed stim protocols
➡️ bit.ly/45Mglio ⬅️
💯 ERP
💥 Thresholds
💻 Prog Extra Stim
💣 Burst pacing
🙅 Induce tach
🏁 Terminate tach
FREE to GROW Members
1.5 CEUs
#VivaEP #Cardiology #EPeeps #VirtualCoach #EPstudy
3
3
195

25 May 2024
2nd one could be („organized“) Afib as well with a more organized but still irregular pattern very short CL from 200-220 - that can often be seen in patients with Afib in EPstudy.
Other expl. for varying CL: microreentry flutter, also more related to Afib from EP perspective.
2
88

7 May 2024
Understanding Variable Heart Rate: Expert Analysis by Electrophysiologist DR. Karthigesan, Apollo Hospital, Chennai! 📊 Dive into the discussion with our informative video.
Video Credits: @Apollo_Chennai
#ChennaiHealthcare #DrKarthigesanClinic #EPStudy #Electrophysiology
1
2
68

16 Apr 2024
#PES #EPStudy #EP #VT #AblateVT ➡️➡️ #EV #BioModVT #Exosomes @SmidtHeart @CedarsSinaiMed @coralf_reef @AsmaNawaz_BME

2
6
434

11 Mar 2024
1. Left posterior/posteroseptal
2. Probably 2 pathways, Right anterior (b/o late transition in precordials) and left lateral (b/o negative delta in AVL)
Please give us results of EPstudy.
2
167

9 Mar 2024
Looks like leftward, back side of RVOT
Who knows, EPstudy shows best conclusion!
2
61

21 Dec 2023
👶⚡️Safety and inducibility of supraventricular tachycardia in pediatric patients during ablation requires pharmacological expertise and a deep understanding of pediatric pathophysiology.
pubmed.ncbi.nlm.nih.gov/3811…👩⚕️#PediatricCardiology #EPStudy #AnesthesiaManagement
7
16
1,108
14 Oct 2023
David Gilmour & Rick Wright during the recording in the studio … reminds me of an #EPStudy in the ‘80-s using a #Grass stimulator … Photo from @crockpics #Analog #EP

2
261
7 Sep 2023

1
7
572
2 Aug 2023
Fantastic first #EP morning conference ➡️ 2023 academic year ✔️ masterfully presented by senior #EPFellow @NatashaCuk #EPeeps #EPStudy #AVN #EGMs #ConductionSystem @SmidtHeart @CedarsSinaiMed @CedarsSinai

4
19
1,787