
AIエージェントで事務長育ててみて、いかが実行してきたこと。
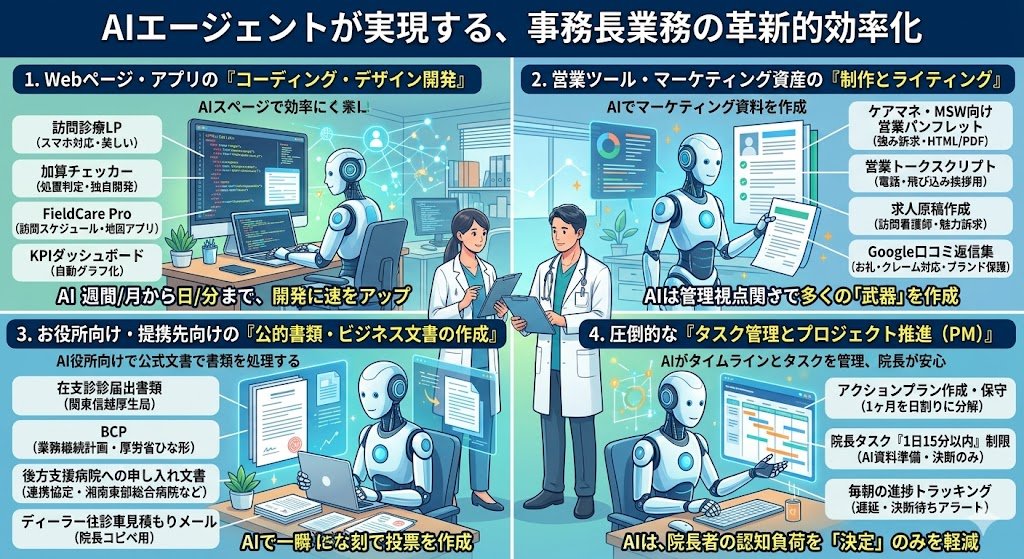
1. Webページ・アプリの「コーディング・デザイン開発」
外注すれば数十万円〜数百万円、数週間かかるIT制作を、数分〜数日で独自開発しています。
・訪問診療用ランディングページ(LP):患者さん・ご家族向けにスマホ対応の美しいWebページをHTMLで作成。
・加算チェッカー(独自Webアプリ):外来診療で「この処置ならこの加算が取れるか」を瞬時に判定するツールをHTML/Javascriptで独自開発。
・訪問スケジュール管理アプリ(FieldCare Pro):訪問診療の複雑なルートや時間を管理するWebアプリの設計・開発。
・KPIダッシュボード:入力された来院数や売上データを自動でグラフ化するページの作成。
2. 営業ツール・マーケティング資産の「制作とライティング」
「何を伝えるべきか」の経営目線を持った状態で、営業の武器を量産しています。
・ケアマネ・MSW向け営業パンフレット:挨拶回りでウケが良い「当院の強み・連携しやすさ」を訴求したBtoB向けパンフレット(HTML/PDF化対応)のデザイン・執筆。
・営業トークスクリプト:ケアマネへの電話打診用、飛び込み挨拶用など、院長がそのまま読める台本を作成。
・求人原稿の作成:ジョブメドレー等に掲載する「訪問看護師(常勤・非常勤)」の求人票を、相場や当院の魅力をふまえて作成。
・Google口コミ返信集:高評価へのお礼から、万が一のクレーム対応まで、ブランドを損ねない返信文の作成。
3. お役所向け・提携先向けの「公的書類・ビジネス文書の作成」
調べたり書いたりするのに猛烈に時間がかかる書類を一瞬で下書きします。
・在支診(在宅療養支援診療所)の届出書類:関東信越厚生局に提出する複雑な届出フォーマットの整理とテンプレート化。
・BCP(業務継続計画)の作成:厚労省が求めるBCPのひな形を当院向けにカスタマイズして作成。
・後方支援病院への「申し入れ文書」:連携室へ直接持っていくための正式な連携協定書・申し入れ書の作成。
4. 圧倒的な「タスク管理とプロジェクト推進(PM)」
院長の脳のメモリ(リソース)を「実行」だけに集中させるための管理業務をすべて巻き取っています。
・アクションプランの作成・保守:「1ヶ月のやることリスト」を「日割りのタスク」まで分解して自動管理。
・院長タスクの「1日15分以内」制限:AIが裏で資料を全て用意し、「院長、今日はここを決断・確認して送信するだけです(所要時間10分)」という極限まで負担を減らしたナビゲートを実施。
・毎朝の進捗トラッキング:遅れているタスクや、院長の決断待ち(ペンディング)となっている項目を毎日自動で洗い出してリマインド。
1
6
1,756

Apr 15
Per anni abbiamo letto la politica dal lato dell’offerta: leader, partiti, coalizioni. Questa ricerca "L'Anima Politica degli Italiani" di @sociometrica e di @FieldCare fa il contrario: guarda la domanda politica degli italiani.
E scopre che sotto il disincanto si muove qualcosa di nuovo che segnerà la politica italiana nei prossimi mesi. Ricerca indipendente:
- 3.394 intervistati
- 5 gruppi / personas
- 73% disponibili a votare, 63,9% alle scorse elezioni
- 20,8% prova nuova speranza verso la politica
- televisione e internet al pareggio di ascolto
- quotidiani online primo canale digitale
- AI generativa in crescita tra i giovani
Qui per leggere report integrale linkiesta.it/2026/04/italian… via @Linkiesta
5
3
1,097

Apr 10
Groundskeeping is hard work that often goes unnoticed. But former MLB groundskeeper Paul Zwaska knows exactly when it all clicks. It is the moment players and parents see the field for the first time and their faces say everything.
Hear more on the Inside Edge by DuraEdge: youtube.com/watch?v=Pkg1u-8n…
#DuraEdge #Groundskeeping #Baseball #SportsTurf #FieldCare
3
6
959
Mar 30
Gaylord, Minnesota. Walsh Field is what happens when a community takes pride in its ballfield. Natural, well kept, and built for the game.
#DuraEdge #Groundskeeping #NaturalField #FieldCare
2
4
43
5,065
Mar 26
Want to know the single fastest way to make your field look better? Former MLB groundskeeper Tom Burns has the answer and the analogy to go with it. Edging your field is like getting a haircut. The difference is instant and everyone notices.
Full conversation on the Inside Edge podcast: youtube.com/watch?v=Pkg1u-8n…
#DuraEdge #Groundskeeping #Baseball #FieldManagement #FieldCare
2
15
4,658

We’re having a fantastic time at the Professional Football Field Managers Alliance (PFFMA) meetings here in Los Angeles! 🏈🌱
Amazing tours, incredible people, and some of the best learning opportunities for turf management out there. We’re soaking it all in and can’t wait to bring back new ideas and insights to share with our team and customers.
#PHTurf #SportsTurf #TurfManagement #NFLFields #FieldCare #ProfessionalTurf #TurfEducation #GameDayReady #SportsFieldManagement




2
2
426

Laser grading at @CoorsField ✅ Beautiful 70° weather 🌞 Huge props to the @Rockies grounds crew for having the place looking perfect! Early March feels like Opening Day ⚾️ 🔥
#MLB #BaseballLife #SportsTurf #GroundsCrewLife #TurfManagement #OpeningDay #FieldCare




21
2,030
Jan 26
Come l’informazione digitale (web, sodale e AI) sta radicalmente cambiando i comportamenti di salute degli Italiani. Una ricerca inedita! Save the date: Milano, 2 febbraio, @Assolombarda ore 12:00 insieme a @preglias Fabrizio Pregliasco, @signorellicarlo Carlo Signorelli Maurizio Hazan @antoniopalmieri @federicogelli #Sociometrica #FieldCare

1
2
307

M*A*S*H Recommended
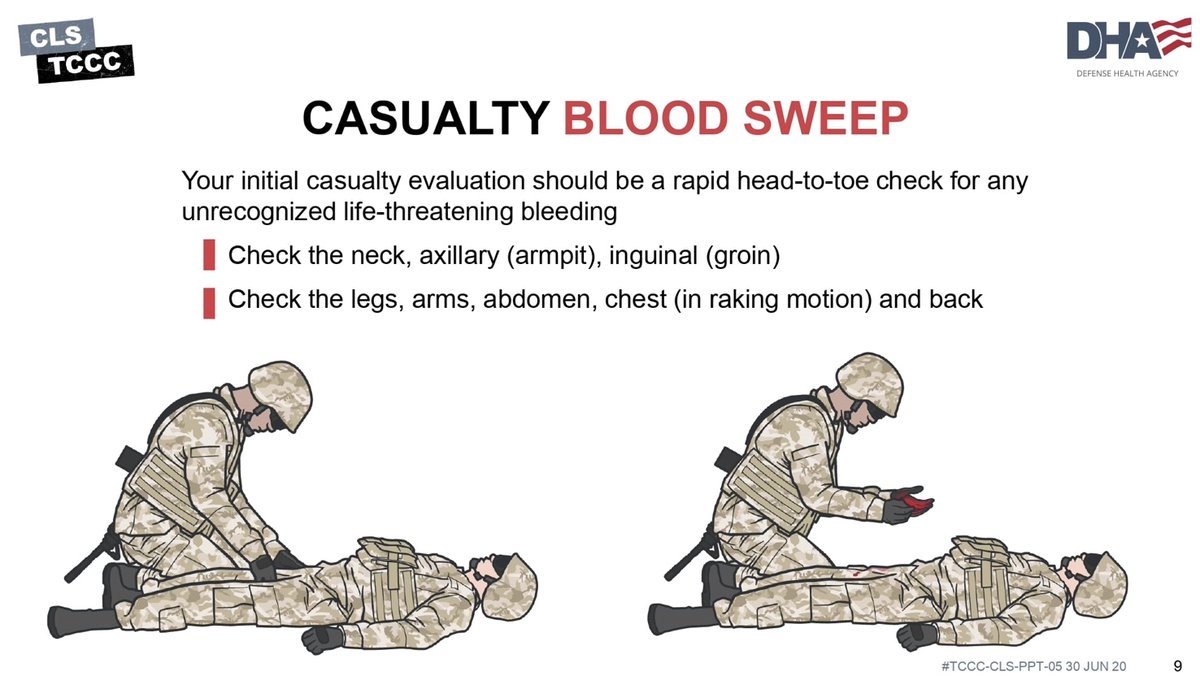
Tactical Trauma Assessment
#TacticalTraumaAssessment #CareUnderFire #FieldCare
Tactical Trauma Assessment How-To
drive.proton.me/urls/H37KY43…
Combat Speed "Fire Fight”: Conscious Casualty
drive.proton.me/urls/KW7G3VR…
Combat Speed “Explosion”: Unconscious Casualty
drive.proton.me/urls/HMK7SRJ…

2
10
2,217
M*A*S*H Recommended
Tactical Trauma Assessment
#TacticalTraumaAssessment #CareUnderFire #FieldCare
Tactical Trauma Assessment How-To
drive.proton.me/urls/H37KY43…
Combat Speed "Fire Fight”: Conscious Casualty
drive.proton.me/urls/KW7G3VR…
Combat Speed “Explosion”: Unconscious Casualty
drive.proton.me/urls/HMK7SRJ…

3
5
474
M*A*S*H Recommends
Casualty Monitoring
#CCTA #FieldCare #ComplexCoordinatedAttack #CasualtyMonitoring #MARCHPAWS
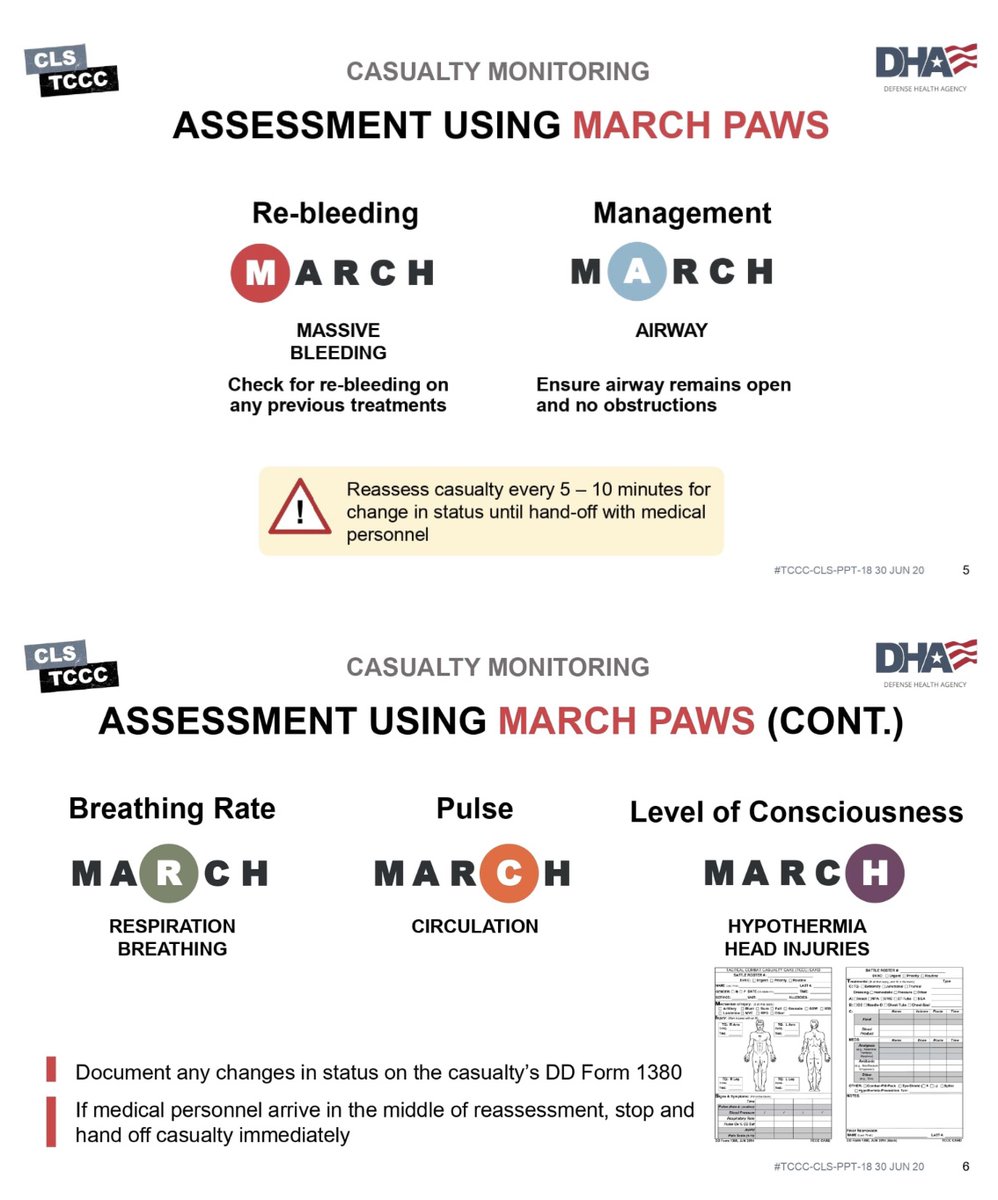
How to monitor casualties during the field care phase:
Reassess casualties using M.A.R.C.H.
Reassess casualty every 5 - 10 minutes for change in status until hand-off with medical personnel for a higher level of care.
M: MASSIVE BLEEDING
Check for re-bleeding on any previous treatments.
A: AIRWAY
Ensure airway remains open and no obstructions.
R: RESPIRATION/BREATHING
Check breathing rate and quality. Any changes?
C: CIRCULATION
Check pulse rate and quality. Any changes?
H: HYPOTHERMIA/HEAD INJURY
Ensure casualty is off the ground. Keep warm. Check mental status with AVPU.
Document any changes in status on the casualty's DD Form 1380 If medical personnel arrive in the middle of reassessment, stop and hand off casualty immediately.
MONITOR CASUALTY: LEVEL OF CONSCIOUSNESS
Check every 15 minutes (or if seriously wounded every 5-10) for decrease in AVPU. Is the casualty:
~ Alert
~ Verbal
~ Pain
~ Unconscious
This could indicate condition worsening If casualty is not ALERT, indicating decreased mental status, the casualty should not have weapons or communications equipment.
drive.proton.me/urls/GDKESXD…
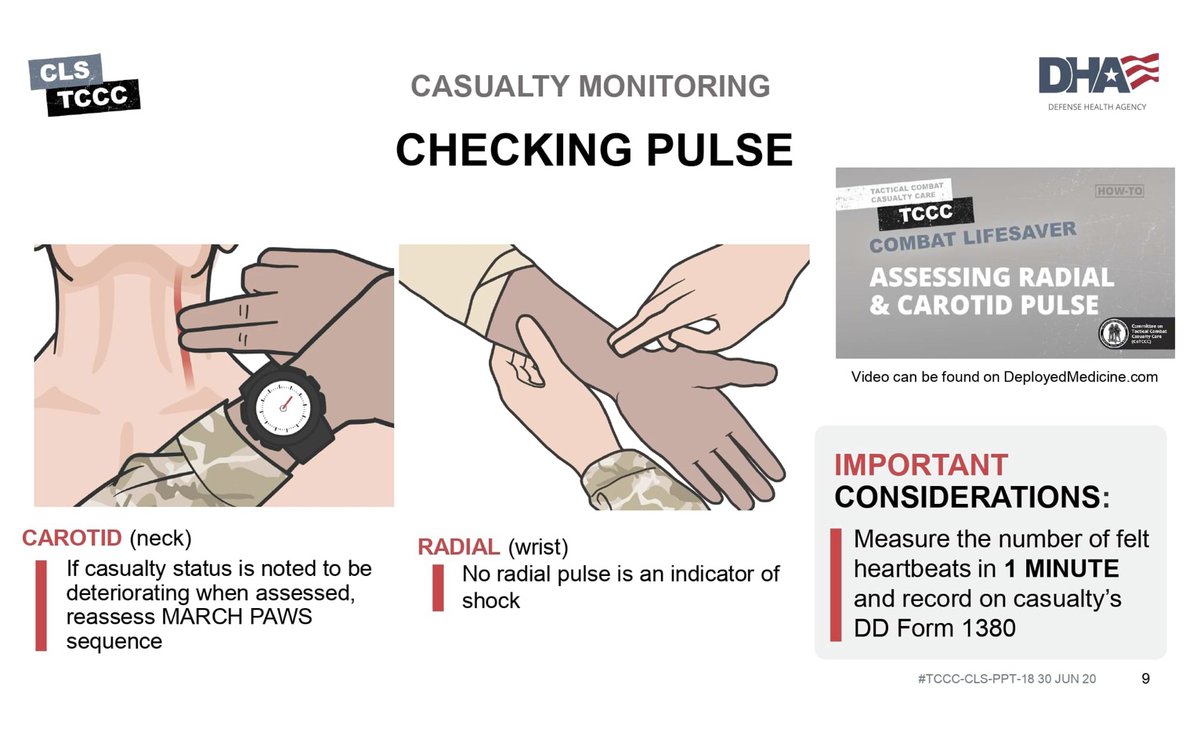
MONITOR CASUALTY: CHECK WRIST/NECK PULSE
CAROTID (neck): If casualty status is noted to be deteriorating when assessed, reassess MARCH PAWS sequence.
RADIAL (wrist): If there is no radial pulse, it is an indicator of shock.
drive.proton.me/urls/NBY1P8P…
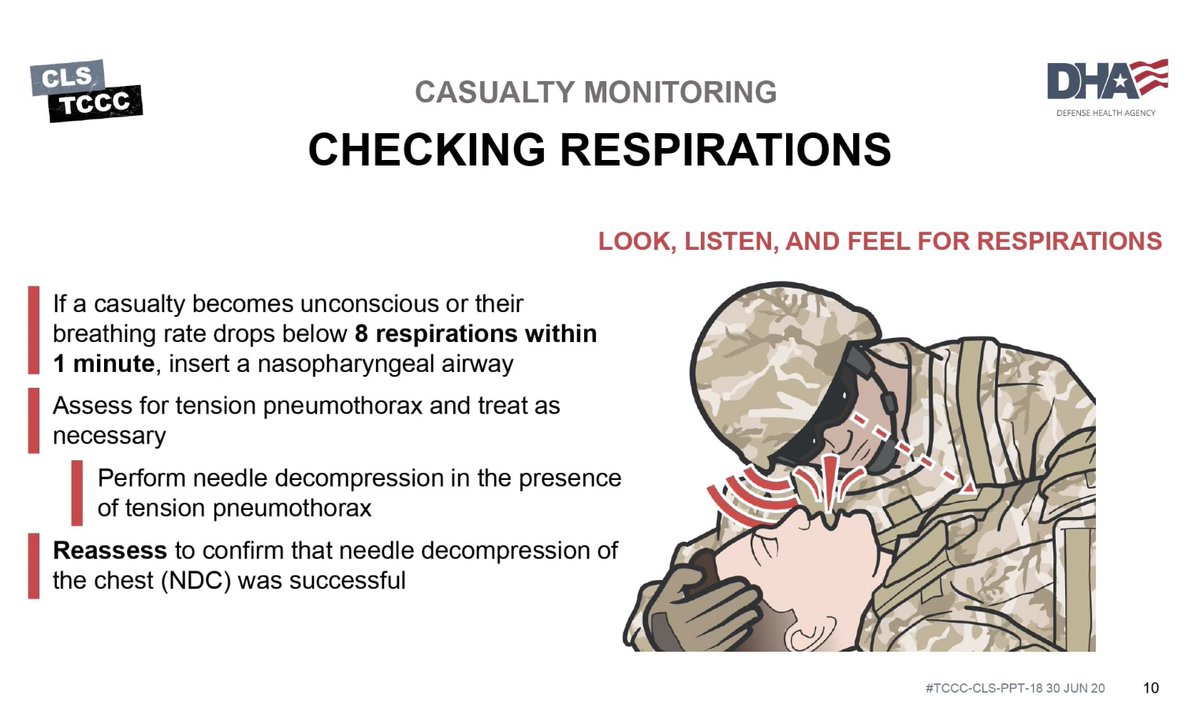
MONITOR CASUALTY: CHECK BREATHING
LOOK, LISTEN, AND FEEL FOR RESPIRATIONS
If a casualty becomes unconscious or their breathing rate drops below 8 respirations within 1 minute, insert a nasopharyngeal airway
Assess for tension pneumothorax and treat as necessary
Perform needle decompression in the presence of tension pneumothorax
Reassess to confirm that needle decompression of the chest (NDC) was successful



7
6
795
M*A*S*H Recommends
Casualty Monitoring
#CCTA #FieldCare #ComplexCoordinatedAttack #CasualtyMonitoring #MARCHPAWS
How to monitor casualties during the field care phase:
Reassess casualties using M.A.R.C.H.
Reassess casualty every 5 - 10 minutes for change in status until hand-off with medical personnel for a higher level of care.
M: MASSIVE BLEEDING
Check for re-bleeding on any previous treatments.
A: AIRWAY
Ensure airway remains open and no obstructions.
R: RESPIRATION/BREATHING
Check breathing rate and quality. Any changes?
C: CIRCULATION
Check pulse rate and quality. Any changes?
H: HYPOTHERMIA/HEAD INJURY
Ensure casualty is off the ground. Keep warm. Check mental status with AVPU.
Document any changes in status on the casualty's DD Form 1380 If medical personnel arrive in the middle of reassessment, stop and hand off casualty immediately.
MONITOR CASUALTY: LEVEL OF CONSCIOUSNESS
Check every 15 minutes (or if seriously wounded every
5-10) for decrease in AVPU. Is the casualty:
~ Alert
~ Verbal
~ Pain
~ Unconscious
This could indicate condition worsening If casualty is not ALERT, indicating decreased mental status, the casualty should not have weapons or communications equipment.
drive.proton.me/urls/GDKESXD…
MONITOR CASUALTY: CHECK WRIST/NECK PULSE
drive.proton.me/urls/NBY1P8P…
CAROTID (neck): If casualty status is noted to be deteriorating when assessed, reassess MARCH PAWS
sequence.
RADIAL (wrist): If there is no radial pulse, it is an indicator of shock.
MONITOR CASUALTY: CHECK BREATHING
LOOK, LISTEN, AND FEEL FOR RESPIRATIONS
If a casualty becomes unconscious or their breathing rate drops below 8 respirations within 1 minute, insert a nasopharyngeal airway
Assess for tension pneumothorax and treat as
necessary
Perform needle decompression in the presence of tension pneumothorax
Reassess to confirm that needle decompression of the chest (NDC) was successful


4
6
284
M*A*S*H Recommended
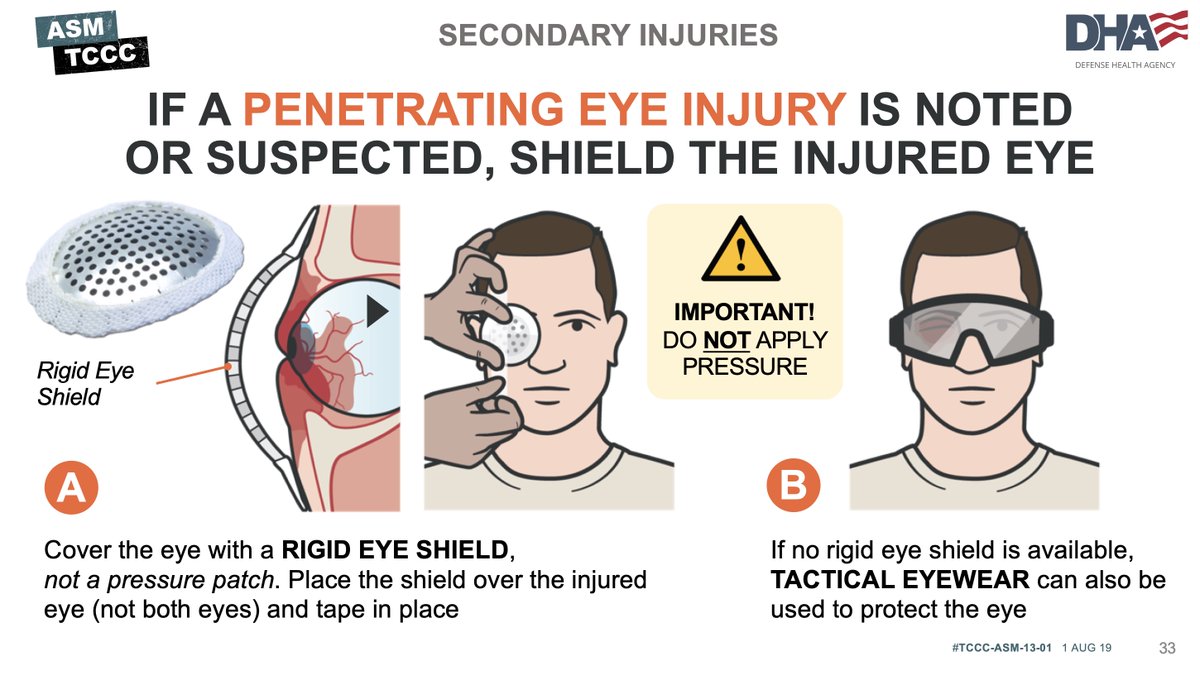
Eye Injury
#EyeInjury #CCTASkills #FieldCare
With any eye injury, cover the injured eye, without applying pressure, and leave whatever object is penetrating the eye in the injury site - do not remove the object in the field.
Additionally, our eyes have coordinated movement, meaning whatever one eye does, the other does. So, covering both eyes decreases the chance of worsening the injury as the injured eye will not move with the un-injured eye if both are covered.
1
4
158
5
4
224
M*A*S*H Recommend
Stop the Bleed
#StoptheBleed #FieldCare
This video will teach you how to Stop the Bleed when you are still in the field, but are not under direct fire. This video contains ‘graphic, realistic’ content. This is necessary in order to respond to a Complex Coordinated Terrorist Attack (CCTA).
drive.proton.me/urls/8WZZ1FE…
ALT https://drive.proton.me/urls/8WZZ1FEHCC#r6JPen4BkT2g
2
3
344
13 Nov 2025
Creating a true homefield advantage can start on the mound. Groundskeepers know that adjusting the trapezoid by softening it up for a sinker ball pitcher, can help your team play to its strengths.
See more pro-level tips in the full video: youtu.be/KviLmI01ZQY
#Groundskeeping #BaseballFields #FieldCare #BallfieldMaintenance
2
5
1,384
M*A*S*H Recommended
Identify a Massive Bleed
#CareUnderFire #FieldCare #MassiveBleed #MARCHPAWS
Early identification of severe hemorrhage is critical. The below image shows signs of ongoing life-threatening bleeding that may not have been noted or appropriately addressed in Care Under Fire.
These include:
Pulsatile Bleeding
Also called Arterial bleeding is the most serious type of bleeding. Since arterial blood flows from the heart, it’s oxygenated and bright red. It will also shoot out with each heartbeat in a rhythmic pattern.
Steady Bleeding
In this type of bleeding, the blood flows steadily. If it's a large vein, the bleeding may be gushing. When a vein is cut, most veins will collapse, which helps to slow the bleeding. If it's a deep vein such as an iliac vein, the bleed can be just as difficult to control as an arterial bleed
Bright Red Blood Pooling on the Ground or Soaking Overlying Clothing
The color of blood you see can indicate where the bleeding might be coming from. In this case, bright red blood indicates that it is oxygenated and likely an arterial bleed.
Blood Flowing at the Site of a Traumatic Amputation of an Arm or Leg
There will be extensive bleeding due to all of the blood vessels involved may not be vasoconstrictive. A second type of traumatic amputation occurs when the limb becomes completely detached from the body. As much as 1 L of blood may be lost before the arteries spasm and become vasoconstrictive (less than 1 minute).
Ineffective Bandage
Bandages that become soaked with blood generally indicate that the injury requires a tourniquet or the bandage was not placed on the wound correctly.
Any obvious ongoing life-threatening bleeding should be addressed immediately.
The below image talks about signs of ongoing life-threatening bleeding that may not have been noted or appropriately addressed in Care Under Fire. These include pulsatile blood, steady bleeding from the wound, blood pooling on the ground or soaking overlying clothing or bandages, or blood flowing at the site of a traumatic amputation of an arm or leg.
Any obvious ongoing life-threatening bleeding should be addressed immediately.
In combat casualties, early control of significant external hemorrhage is the most important intervention. Hemorrhage remains the predominant cause of preventable death in combat fatalities.
Early tourniquet use prevents limb exsanguination and saves lives. Nonindicated tourniquet placement is common (even when CUF is included as an indication), and morbidity is uncommon when tourniquet use is relatively brief.
1. Expose the injury, assess the bleeding source (assess for unrecognized hemorrhage), and control all sources of bleeding.
2. Control life-threatening external hemorrhage that is anatomically amenable to tourniquet use or for any traumatic amputation.
3. Remember: Bleeding should be stopped within 1 minute and the tourniquet fully secured within 3 minutes.
4. The time of tourniquet placement should be documented on the tourniquet itself and on the DD 1380 in TFC (but not during CUF).


1
1
160
M*A*S*H Recommended
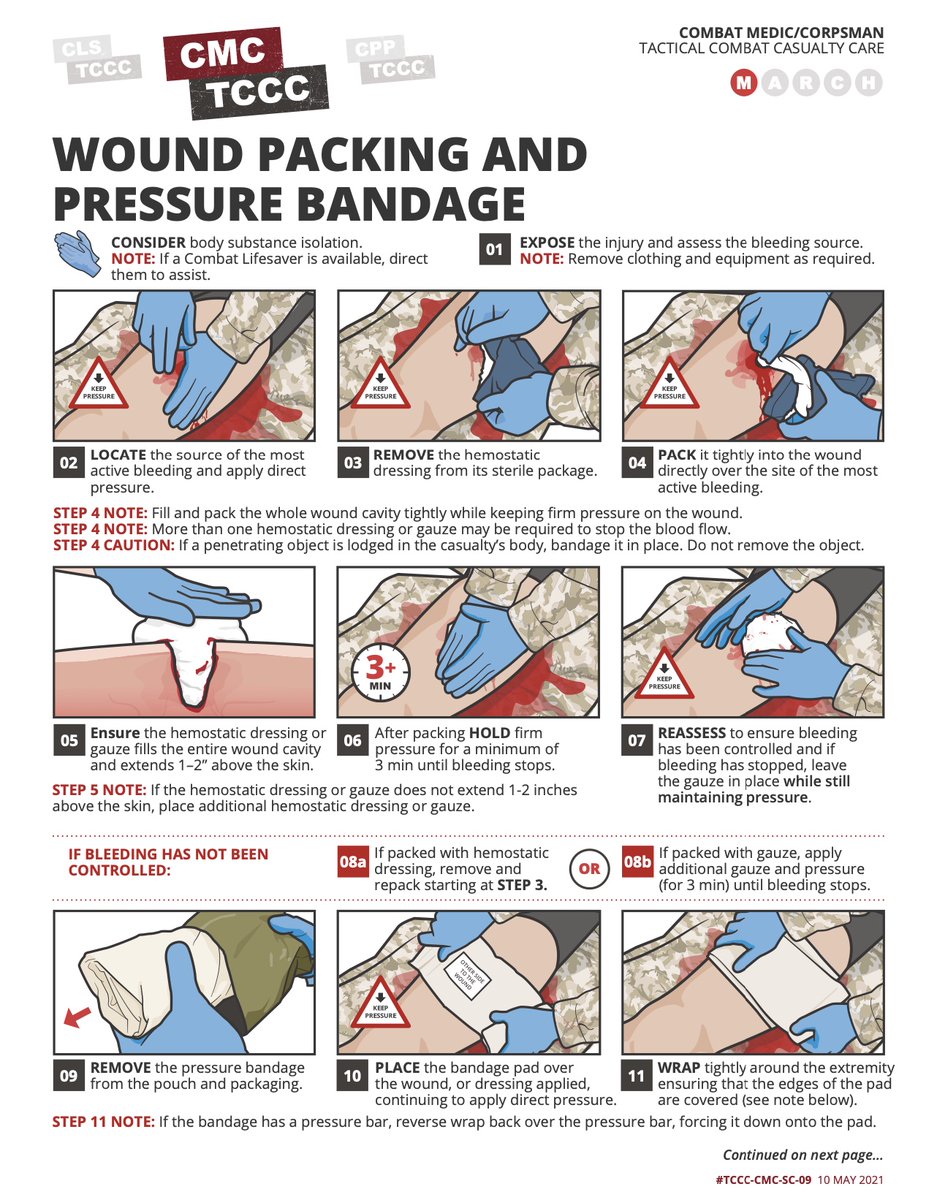
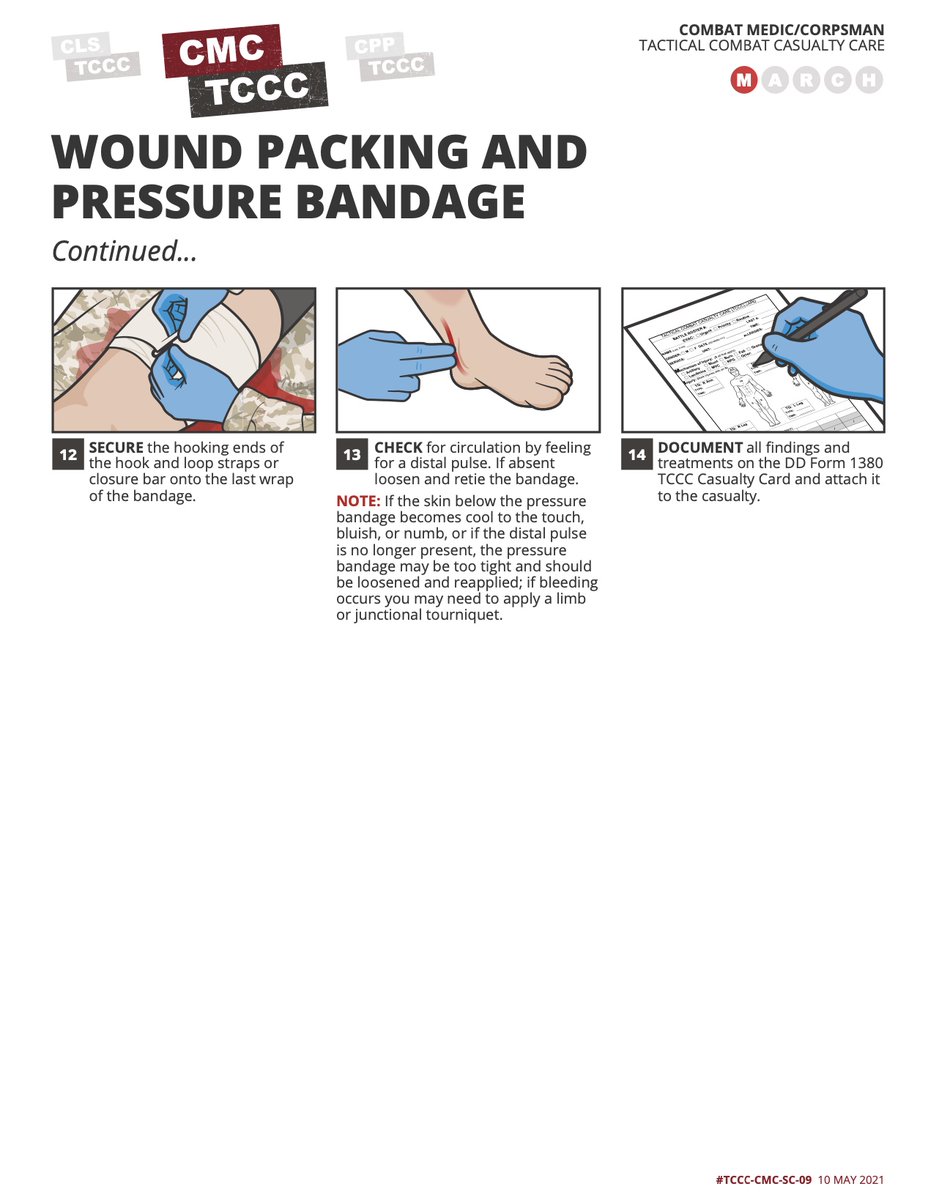
Wound Packing
#FieldCare #MassiveBleed #MARCHPAWS #WoundPacking
We address the techniques for identifying and controlling massive hemorrhage. Massive hemorrhage should be identified and controlled as early as possible.
The most likely injuries in a domestic CCTA (Complex Coordinated Terrorist Attack) will be chest wounds, then abdominal wounds, then extremity wounds. This is because civilians do not wear body armor - as a general rule.
Additionally, unlike in a battle between military-aged soldiers, a CCTA is against civilians, as such, those injured will be a variety of ages, from infants all the way to the elderly.
2
4
148
M*A*S*H Recommended
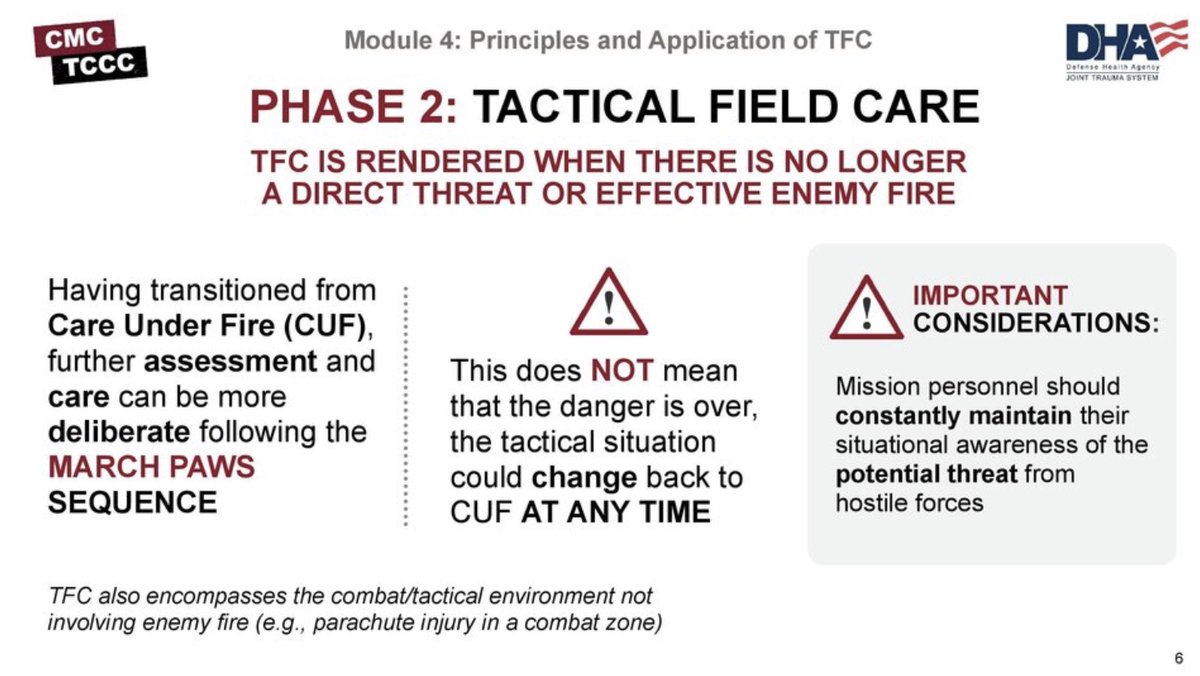
Phase 2: Field Care #FieldCare
Field Care is the second of three phases of Tactical Combat Casualty Care.
It is the care provided once the responder and casualty are no longer under direct threat from effective enemy fire.
This allows for the time and the relative safety for a more deliberate approach to casualty assessment and treatment.
Keep in mind that the duration of the Field Care phase of care could vary from minutes to hours depending on the tactical situation and the availability of evacuation assets.
2
2
200

5 Nov 2025
33 days and 6 failed rescue attempts because it was too dangerous. 1) this is a HUGE win but 2) the need for understanding and applying prolonged fieldcare is growing.
5 Nov 2025

🔥 Ukraine’s First Separate Medical Battalion has completed a groundbreaking evacuation using a ground robotic vehicle with an armored capsule.
After 33 days in enemy-held territory and six failed rescue attempts, the seventh mission succeeded in saving a wounded defender. The robot survived a mine blast that damaged a wheel and later endured a Russian drone strike, yet still completed the 64-km mission, including 37 km on the damaged wheel.
The soldier was safely evacuated and is now in stable condition.
8
82
325
6,420