

How do you become a better trader?
Not by watching more charts, following more influencers or adding more indicators.
You become better by recognizing your own biases.
Because most of the time, the market is not what destroys you.
Your own mind does.
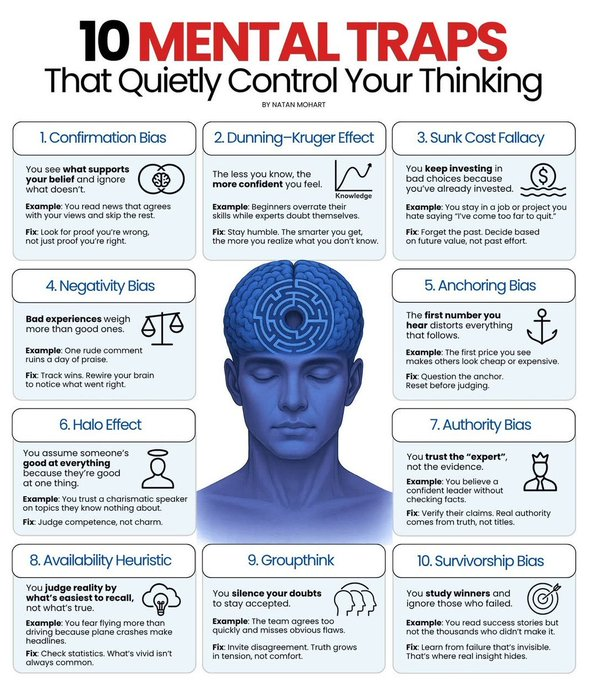
Confirmation bias makes you see only what supports your position.
Anchoring keeps you stuck to old prices.
Sunk cost fallacy makes you hold bad trades for too long.
Negativity bias turns every red candle into fear.
Authority bias makes you trust others more than evidence.
Groupthink silences your own judgment.
The best traders are not bias-free.
They just catch their mental traps earlier than everyone else.
The market is already hard enough.
Don’t let your own biases make it harder.
1
3
27

If students get into GroupThink mode, it is indeed bad; some sort of reverse regimentation
As a student I never agreed with anyone, it was always a percentage
7

Chihiro retweeted

兵庫県も、文春中傷動画も、社会心理学でいう集団浅慮(groupthink)でうまく説明できることに気付いた。事実に重きを置くよりも集団の中で自分の地位を保全することを優先する。政党に属するひとの意見が偏るのはそのせい。
1
4
7
593

Ein positiver Schritt. Es scheint, als wäre Präsident Trump imstande, schwere Fehler zu korrigieren und Kriege zu beenden. Warum schaffen das die mit Russenhass und Groupthink hirnverklebten "EU-Eliten" mit dem Ukrainekrieg nicht? Wir wollen Frieden und Wohlstand!

🇮🇷🇺🇸 BREAKING: Iran's Mehr News Agency has released all 14 clauses of the MoU with the U.S.:
1: Permanent and immediate cessation of war on all fronts, including Lebanon.
2: The US commitment to non-interference in Iran's internal affairs and respect for the sovereignty of the Islamic Republic of Iran.
3: Complete lifting of the naval blockade within 30 days.
4: The US commitment to withdraw its forces from around Iran.
5: Reopening of the Strait of Hormuz within 30 days under Iranian arrangements.
6: Suspension of sanctions on the sale of oil, petrochemical products, and derivatives, and full access of Iran to its financial resources.
7: The necessity for the US and its allies to present reconstruction plans for Iran amounting to at least $300 billion.
8: 60 days of negotiations to reach a final agreement based on nuclear issues and the complete lifting of primary, secondary, US sanctions, and UN Security Council and IAEA Board of Governors resolutions.
9: Reiteration of Iran's commitment under the NPT treaty not to produce nuclear weapons.
10: During the negotiation period, the US has committed not to add forces in the region and not to impose new sanctions.
11: Release of $24 billion of Iran's blocked funds during the 60-day final negotiation period. Half of this amount must be made available to Iran before the start of negotiations.
12: Formation of a supervisory mechanism to implement the agreement.
13: The final agreement will be approved by a UN Security Council resolution.
14: Final negotiations will not begin before the release of half of Iran's blocked funds, suspension of Iran's oil sanctions, and lifting of the naval blockade, and the final agreement will only cover the fate of enriched materials and enrichment, lifting of sanctions, and Iran's economic reconstruction plan. Discussions about Iran's missile program and support for resistance groups are definitively removed from the agenda.

15

Lol cause I have actual thoughts and opinions? GTFO here with your groupthink. Not all chips are equal sorry bud
1
22

Sounds like someone is emboldened with Nazi groupthink. That's fun.
1
33

Groupthink and best-think, aren’t the same thing… I think 🤔
1
1
12


Idk hes alright. He says some things I think young men in particular need to hear, his commentaries starting with Dear Elon are really good. Hes not my type of comedian but I think dismissing him as a figure out of tribalism is silly and unserious. Groupthink isnt how we win.
33

We appear to be on different planets! She was mocked and attacked for 30 years. And ignored.
"Legacy media in Australia is incapable of playing its vital role" is very true though! A bubble of groupthink.
7


are you in the villa? he’s clearly experiencing things we aren’t & I’m sure he noticed how weird everyone is being to the dsbw… if he DIDNT say anything, yall would have something to say abt that as well. yall are just insufferable, insecure, disingenuous victims of groupthink
2
2
34


1. Why fund dozens of biolabs worldwide manipulating infectious diseases (including SARS-CoV-2 elements) with minimal oversight?
Dual-use research—civilian biosecurity masking offensive/defensive bioweapons potential—serves multiple interlocking interests. Geopolitically, the U.S. (& peers) maintained advantage in a post-Soviet world by securing/dual-purposing former Soviet labs (e.g., Ukraine programs) & partnering in hotspots like Wuhan via EcoHealth & NIH grants. This creates leverage: pathogen libraries for countermeasures (or escalation dominance), surveillance of rivals’ capabilities, & plausible deniability.
Wealth ties in via contracts: defense/intel budgets flow to contractors, universities & pharma for “preparedness.” Oversight stays thin because transparency risks exposure of gain-of-function (GoF) work that blurs research & weaponization. Psychologically, this reflects elite overconfidence—“we can manage the risks”—coupled with institutional inertia. Revelations of 120 U.S.-linked sites confirm a sprawling network; the “why” is power preservation in an era of great-power competition. Accidents or releases test resilience while rivals bear blame.
2. Why ignore vaccine dangers, lie about safety/efficacy?
Simple. Public health agencies became extensions of pharmaceutical-government complexes. Emergency Use Authorization, liability shields (PREP Act) & Warp Speed billions created massive incentives to prioritize speed & uptake over long-term signals. Once committed, admitting risks (myocarditis, excess mortality correlations in some datasets, waning efficacy) triggers legal, reputational & funding collapse.
Psychologically: groupthink careerism. Dissenters face deplatforming (as w/ lab-leak skeptics early on). Collectively, it signals “trust the science” as a control mechanism during crisis—fear binds populations. Data suppression or reframing (“safe & effective” as mantra) protects the golden goose of mRNA platforms & future pandemic contracts. Not every actor knew every harm, but institutional self-preservation favored narrative over nuance.
3. Why push masks & lockdowns despite limited efficacy & natural immunity costs?
These were visible theater for perceived action & compliance enforcement. Masks offered low-cost signaling (“we’re doing something”) with marginal aerosol benefits in controlled settings but poor real-world adherence/impact against airborne spread. Lockdowns preserved “virgin” populations for vaccine rollout by delaying exposure—aligning with pharma timelines & suppressing early treatment data.
Behaviorally: humans in crisis crave authority & rituals. Elites (often remote-working, low personal risk) imposed costs on working classes, small businesses & children—eroding social capital while accelerating wealth transfer to big tech/pharma. Natural immunity was downplayed because it competed with the product. This reflects a managerialist mindset: model-driven projections over historical precedent (e.g., focused protection), plus political utility in disrupting normalcy.
4. Why suppress alternatives like ivermectin & HCQ?
Early repurposed drugs threatened the EUA pathway (requiring no adequate alternatives) & billion-dollar novel vaccine monopolies. Regulatory capture media amplification turned debate into “misinfo.” Trials were designed/cherry-picked for failure (wrong dosing/timing), while observational data from frontline doctors was dismissed.
Psychologically & economically: pharma margins favor patented assets. Admitting cheap generics worked undermines the “novel threat demands novel solution” frame. This cements centralized authority—CDC/Fauci as arbiters—over decentralized medicine. It reveals how “following the science” often follows the money & narrative control.
Continued…
1
1
47

Watching women you love be hated on by other "feminist" women because they don't conform to the groupthink is the red pill for most men about this stuff.
Wakes you up.
1
1
44

Open source is the way. Open sourced communities are generally more creative than their closed sourced counterparts. Necessary to safeguard against groupthink in the frontier models.
17