
Jun 11
The answer is: B. “Naked axons”
To learn more, head to our blog: arkanalabs.com/axonopathy/
#neuropath #neuromuscular #neuronotes #pathology
1
277
Jun 10
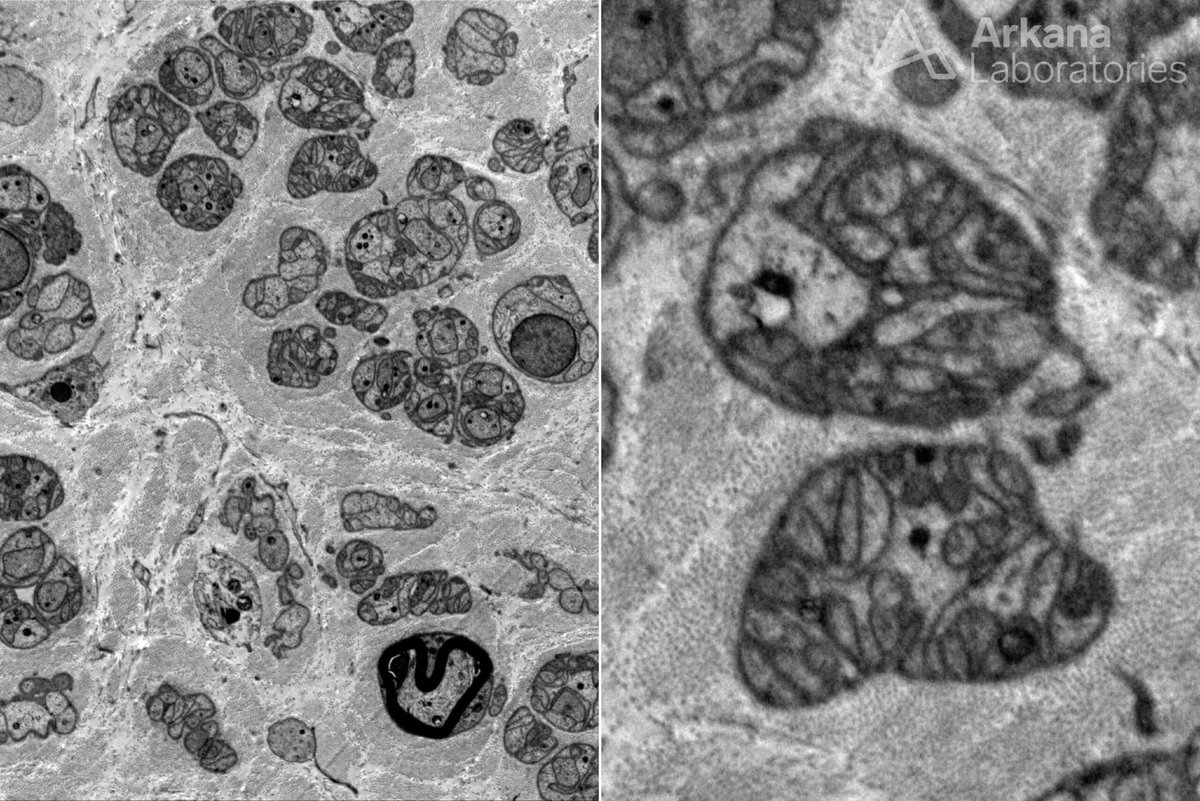
The patient is a 72-year-old man. Clinical diagnosis of neuropathy.
What cannot be seen on this electron micrograph of muscle?
A. Unmyelinated fiber loss
B. “Naked” axons
C. Large myelinated fiber loss
D. Small myelinated fiber loss
#NeuroNotes #neuropath #pathology #neuromuscularpath
1
2
5
870
The answer is: D. Athletic Conditioning
To learn more, head to our blog: arkanalabs.com/skeletal-musc…
#neuropath #neuromuscular #neuronotes #pathology

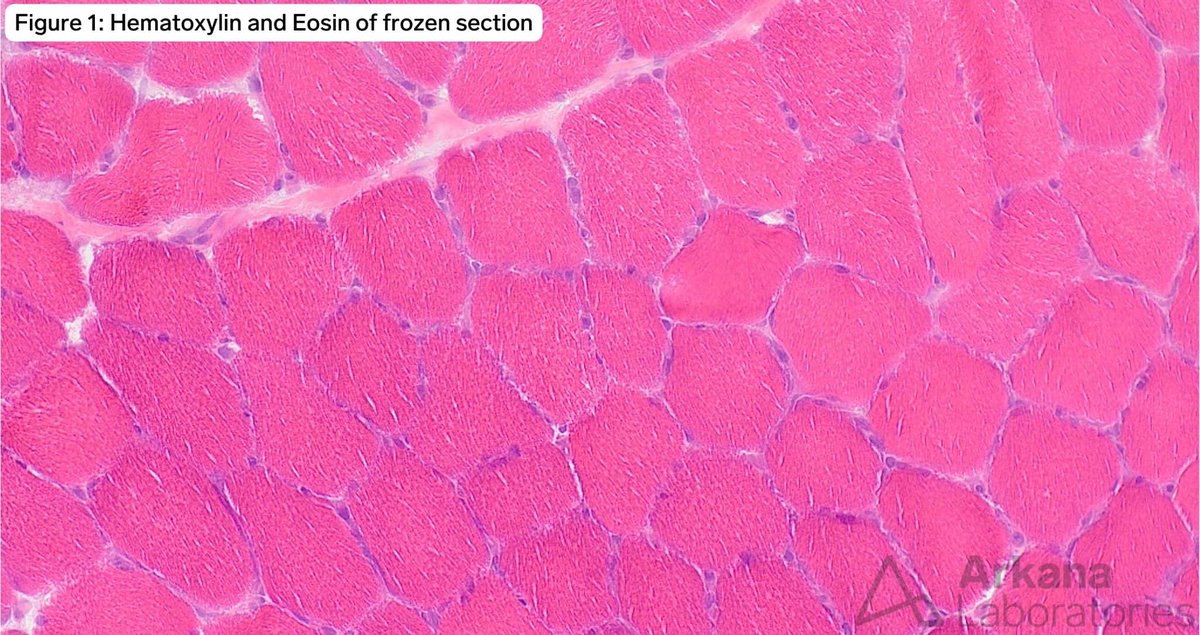
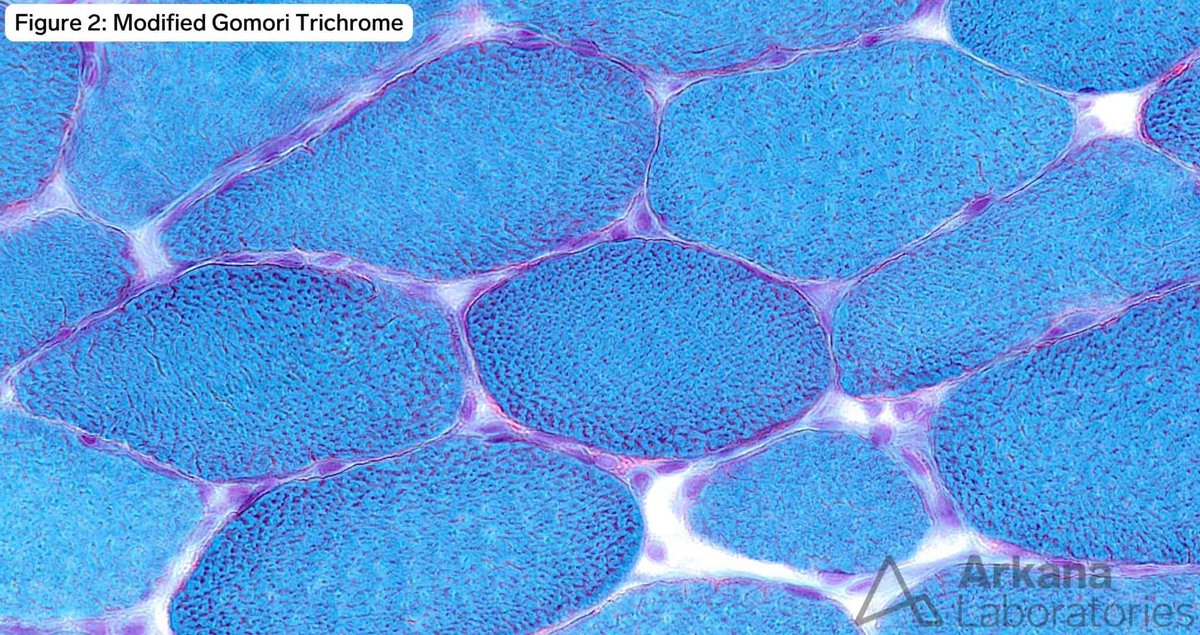
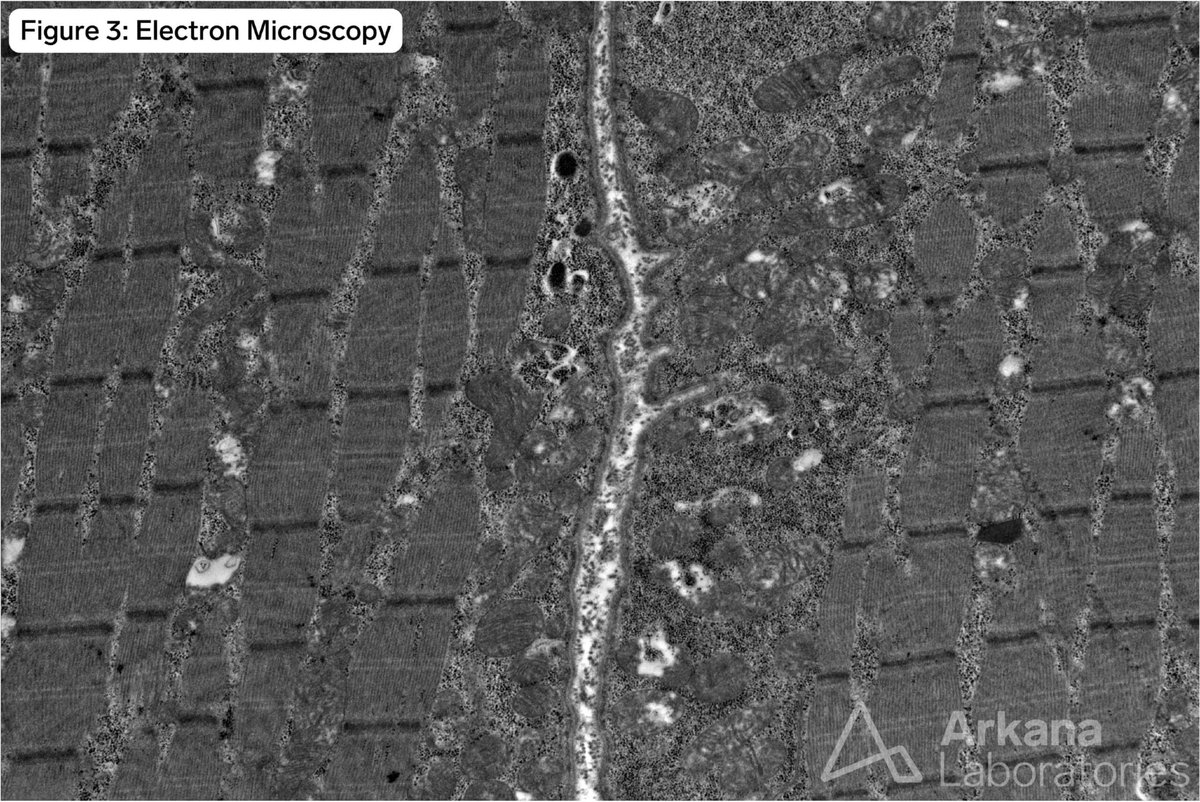
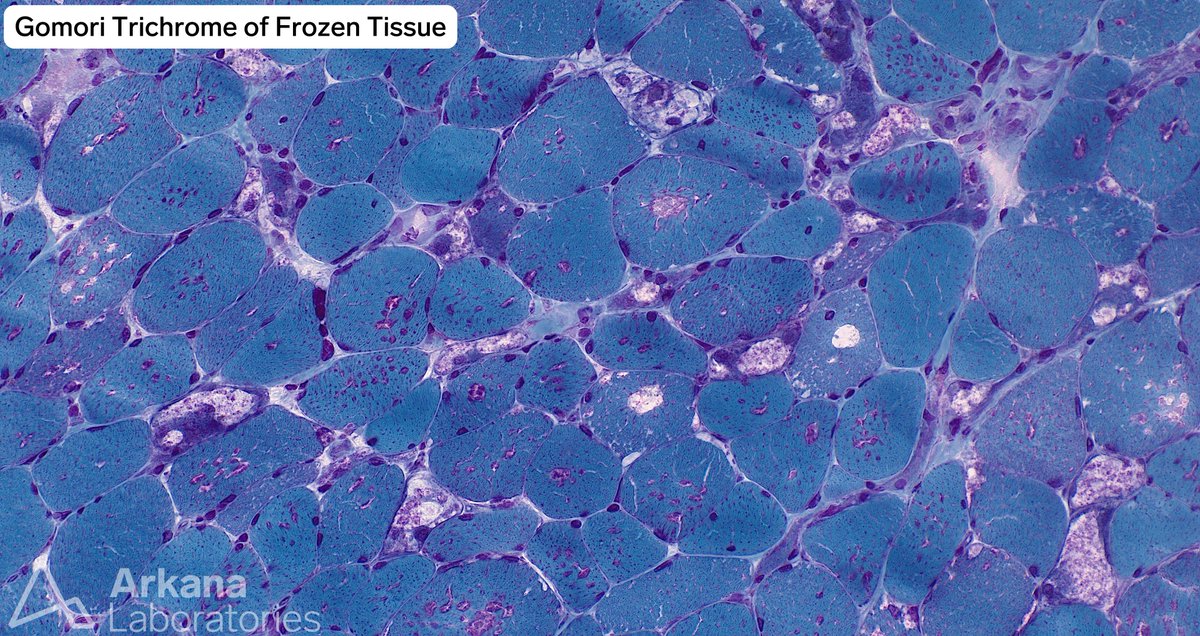
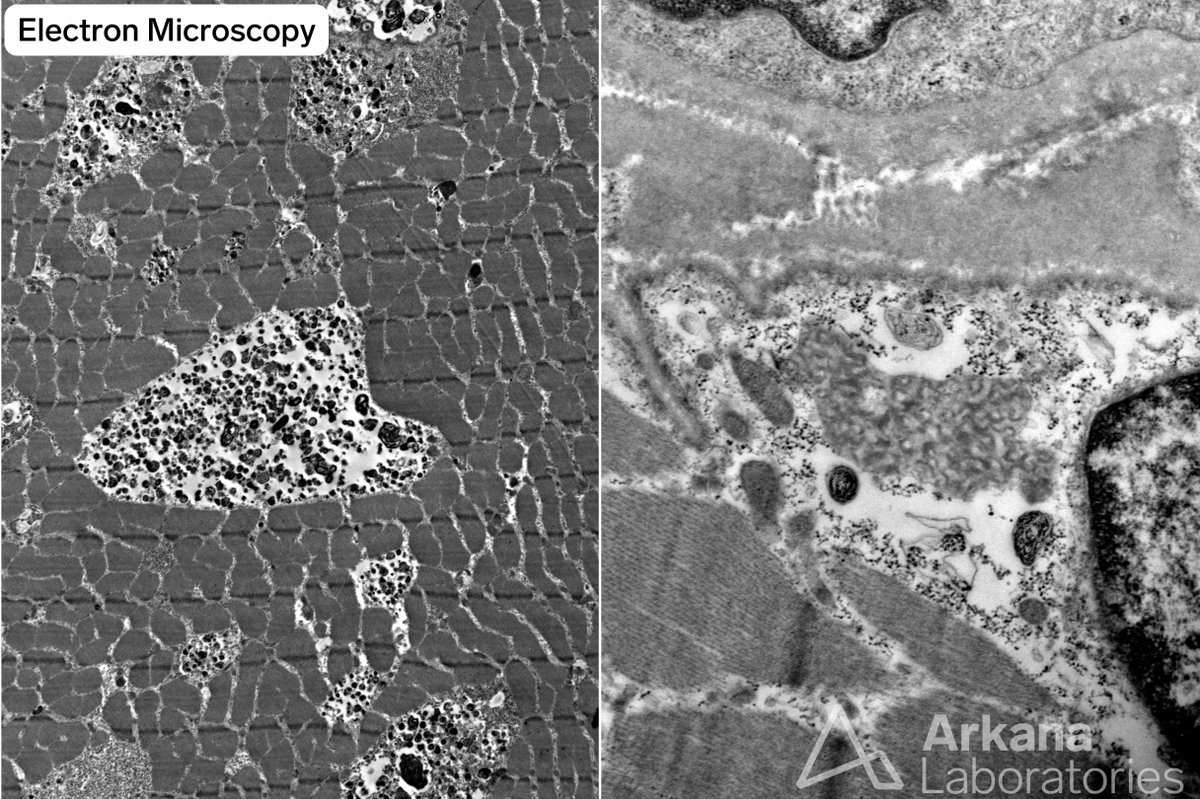
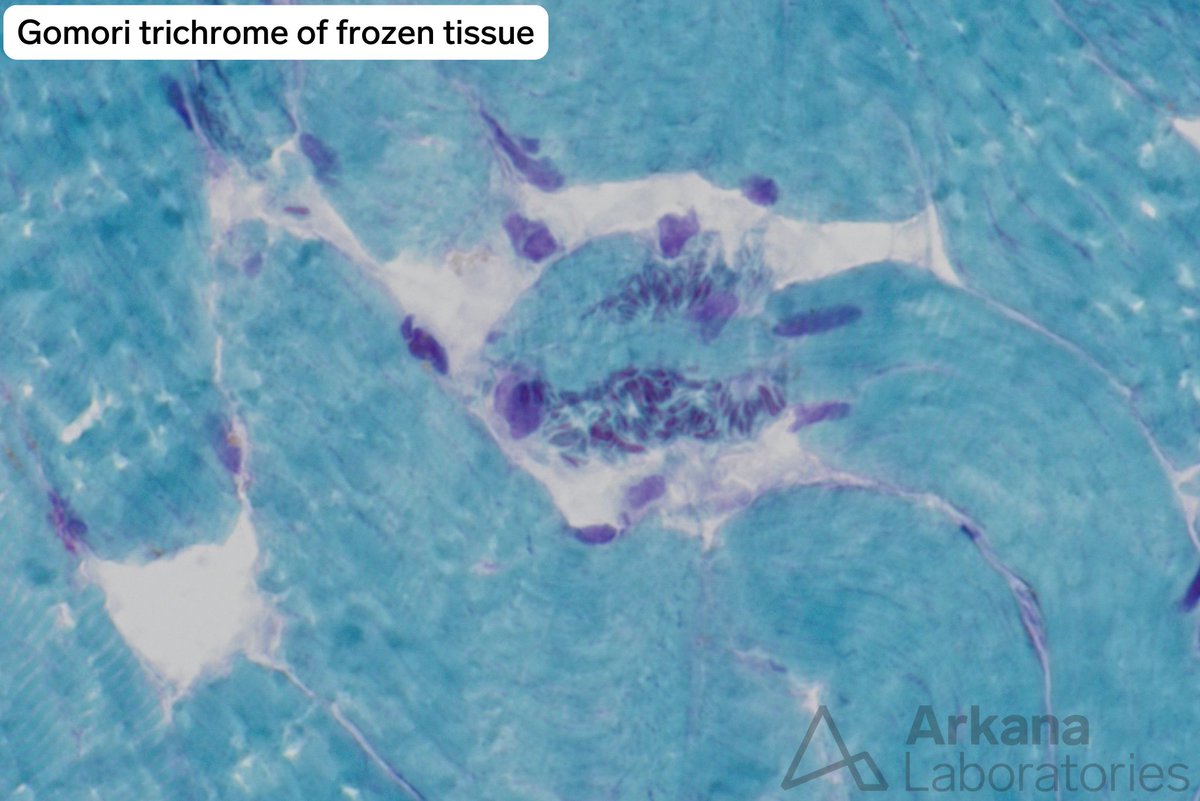
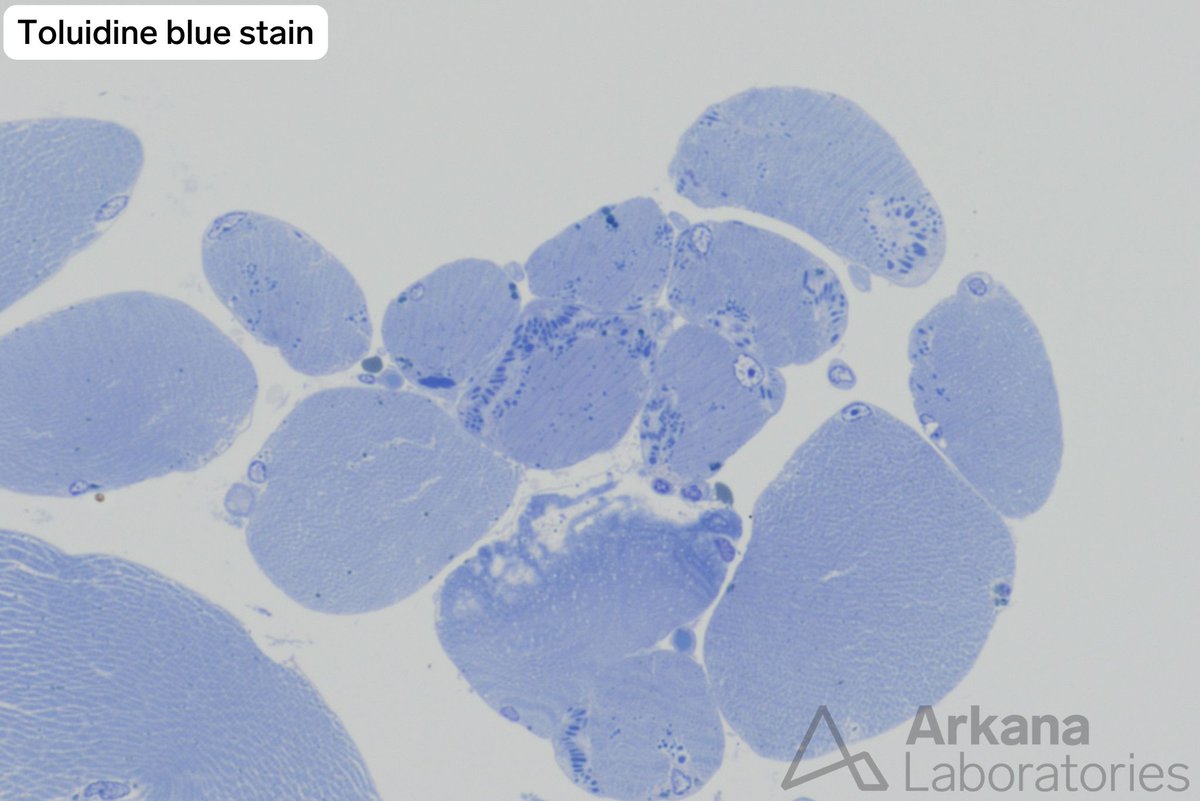
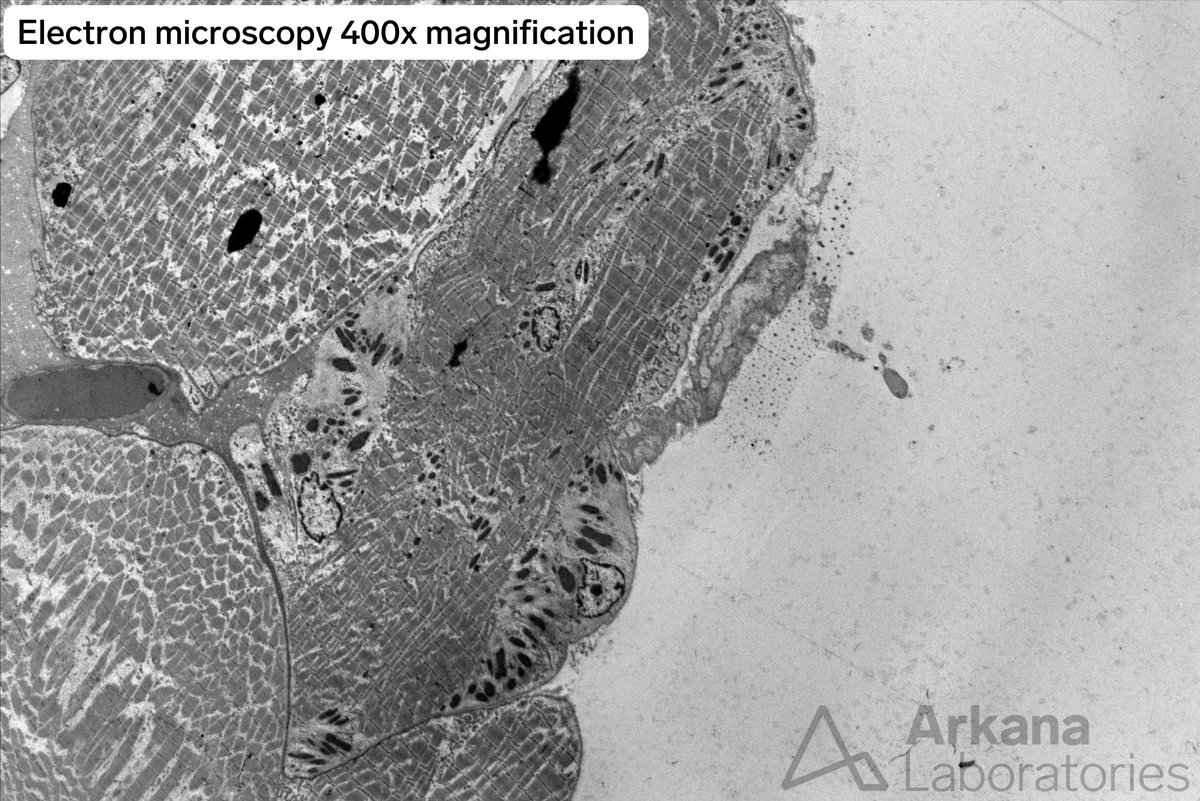
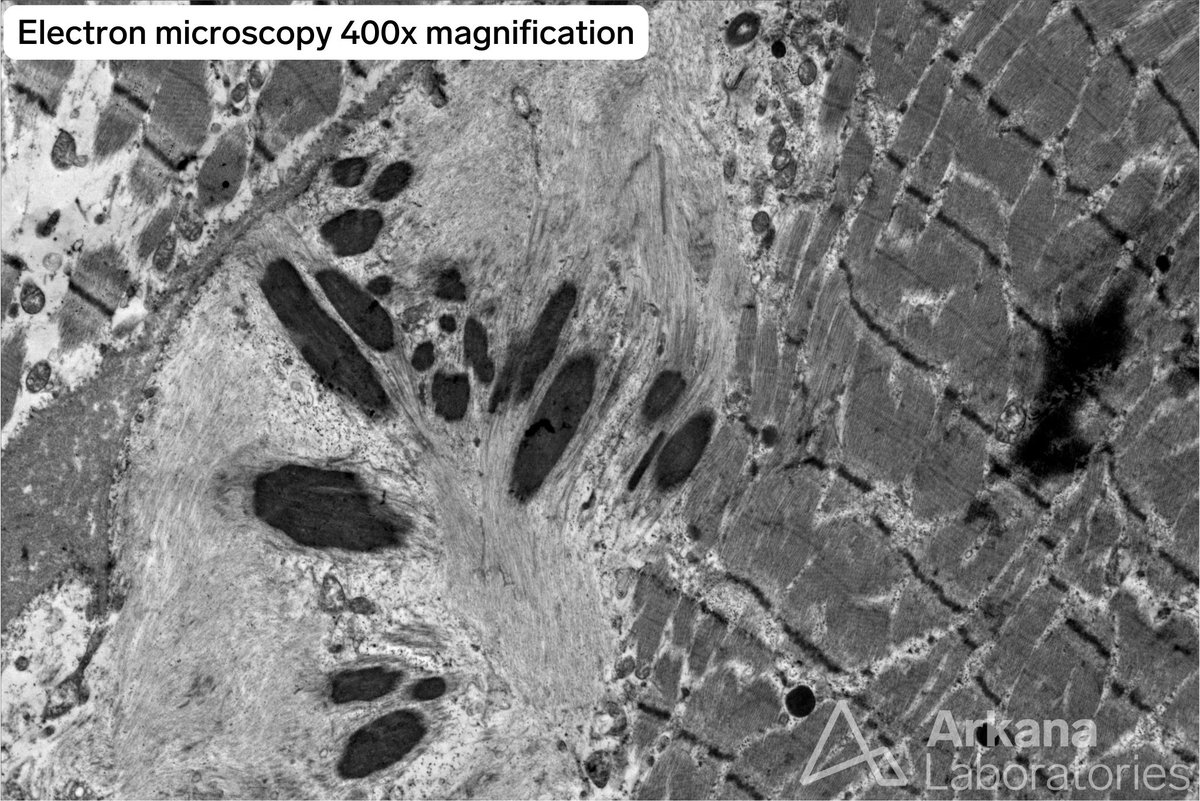
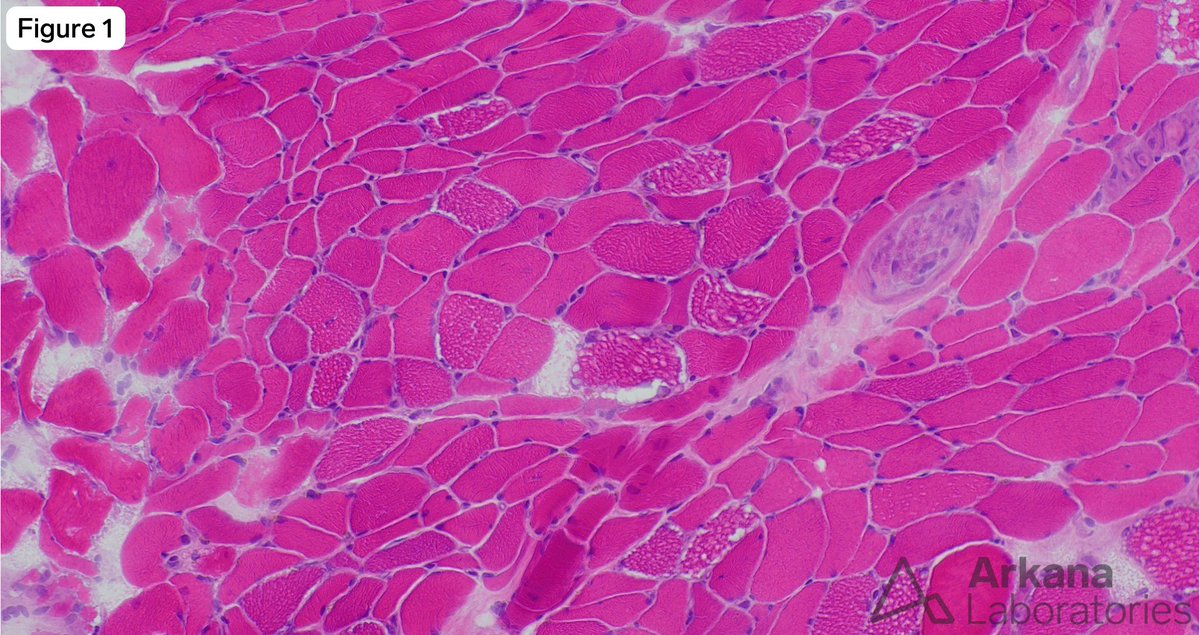
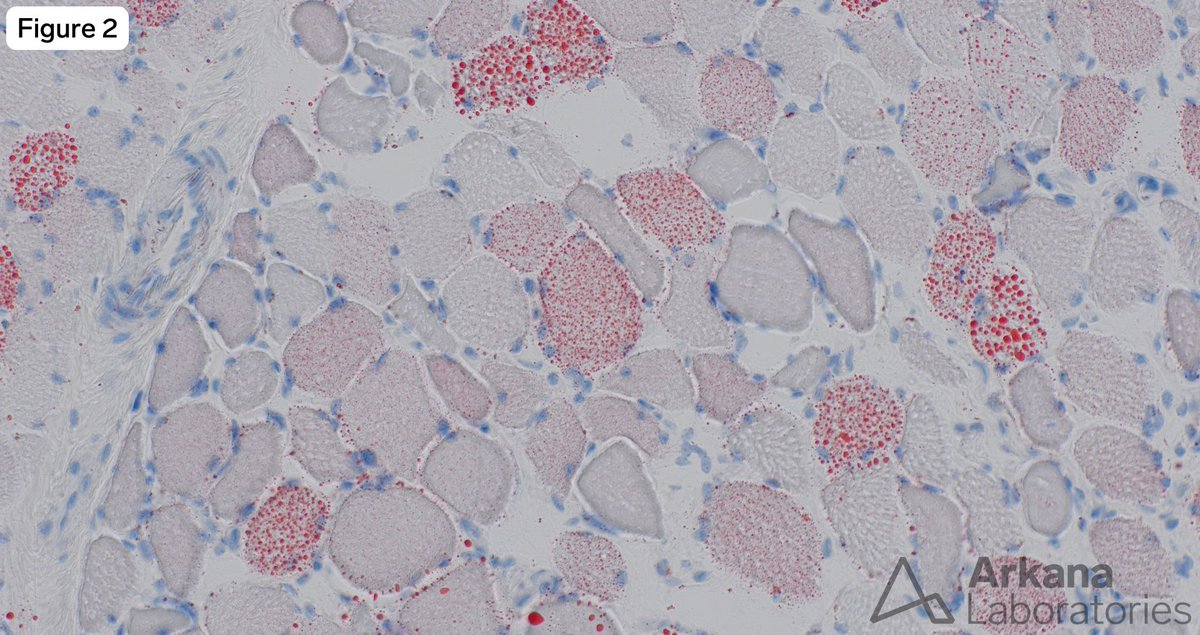
This 17-year-old elite endurance athlete underwent muscle biopsy to evaluate for recent inability to perform at the level they could six-months ago.
In the context of this individual’s clinical history what is the best explanation for the changes seen on light and electron microscopy?
A. Inclusion Body Myositis
B. Vacuolar Myopathy
C. Polymyositis
D. Athletic Conditioning
#NeuroNotes #neuropath #pathology #neuromuscularpath
1
5
863
This 17-year-old elite endurance athlete underwent muscle biopsy to evaluate for recent inability to perform at the level they could six-months ago.
In the context of this individual’s clinical history what is the best explanation for the changes seen on light and electron microscopy?
A. Inclusion Body Myositis
B. Vacuolar Myopathy
C. Polymyositis
D. Athletic Conditioning
#NeuroNotes #neuropath #pathology #neuromuscularpath
2
5
15
1,832
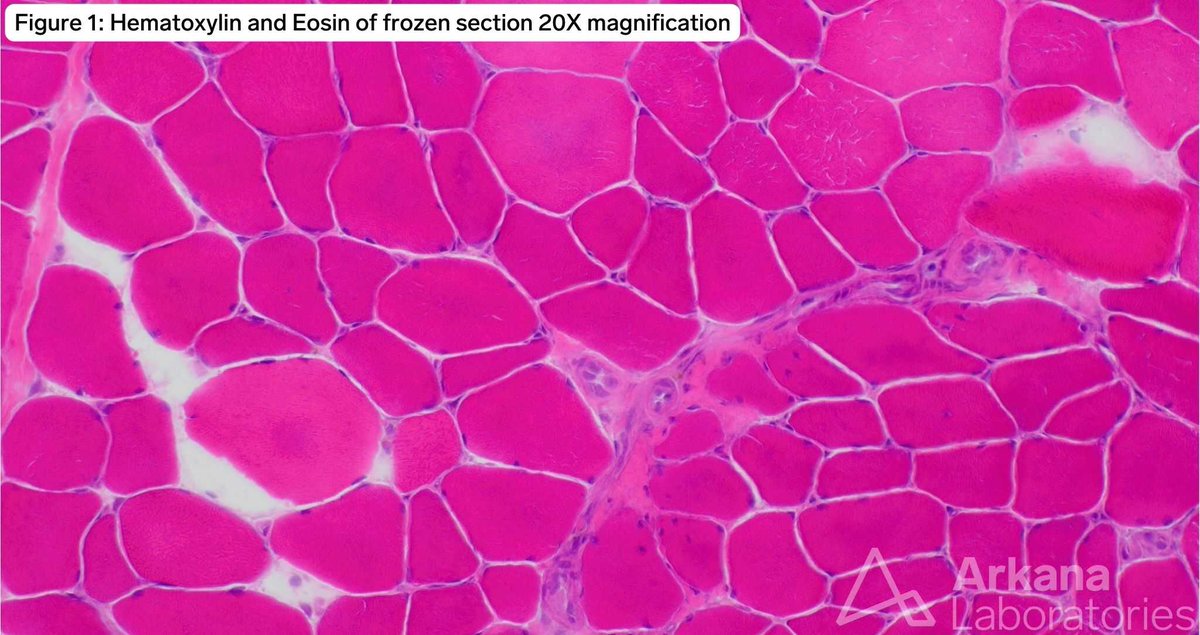
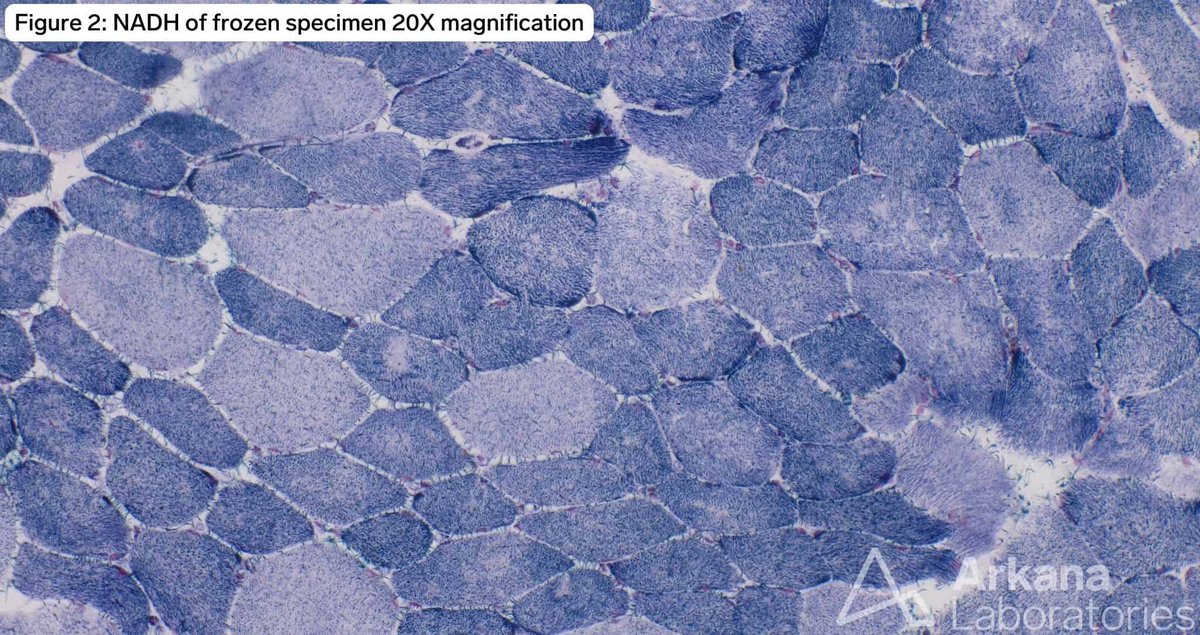
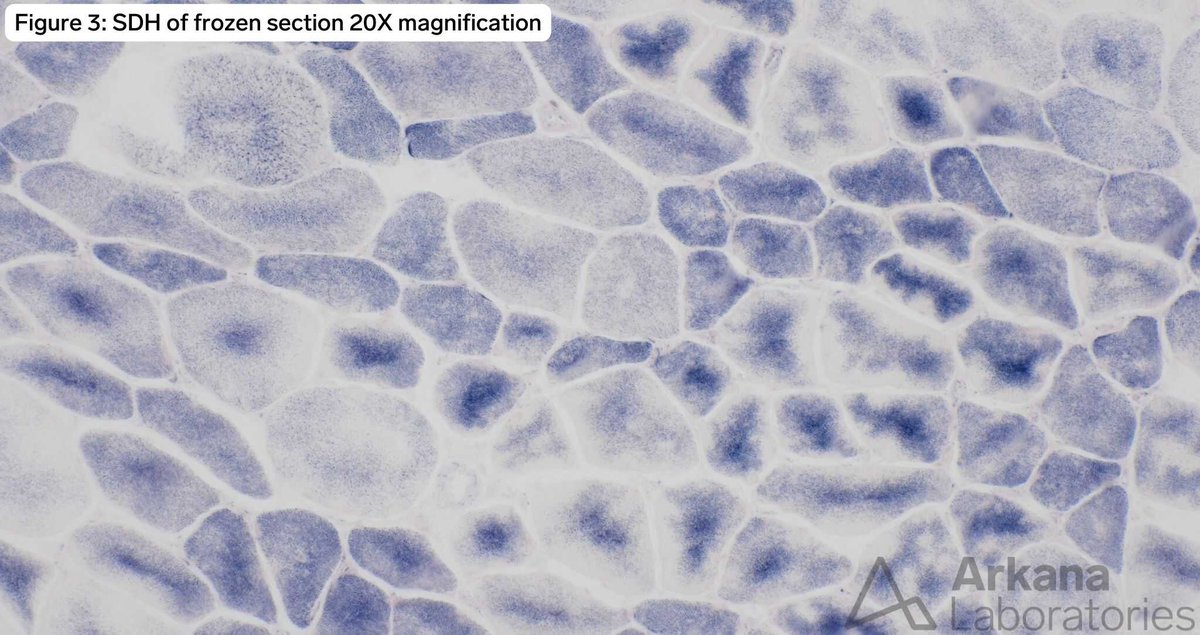
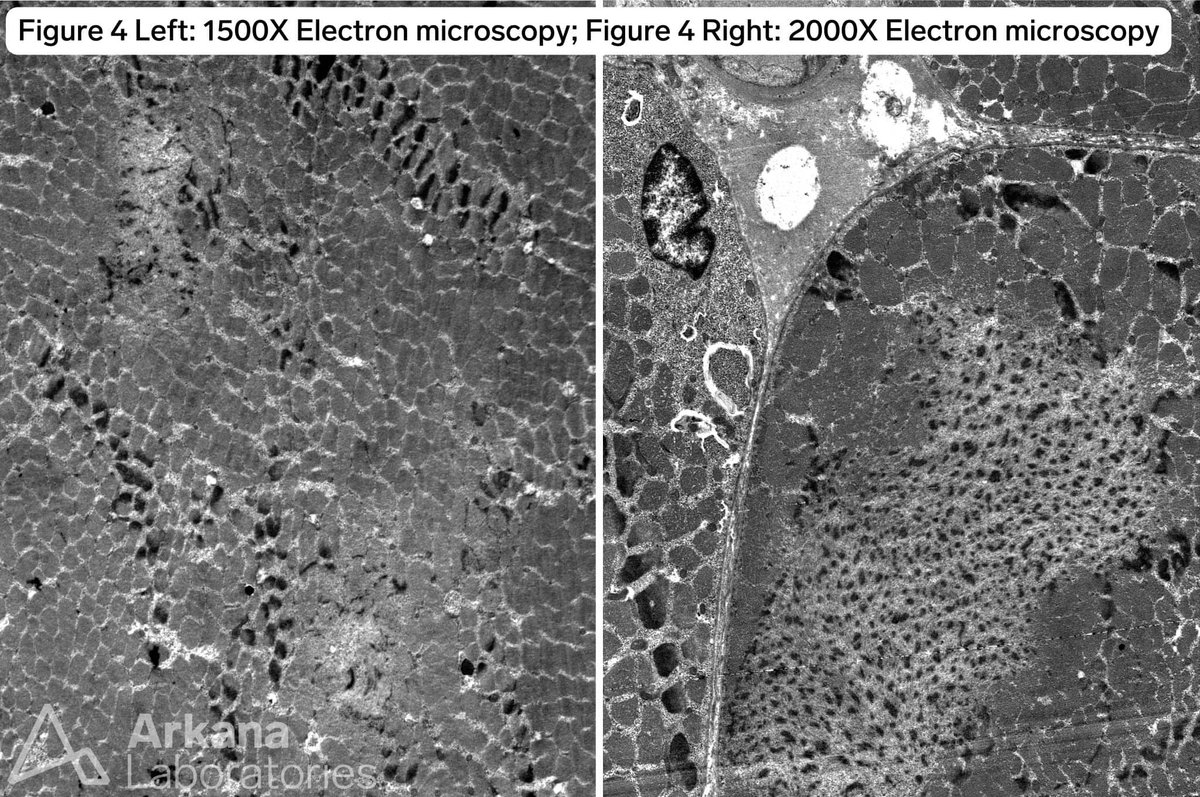
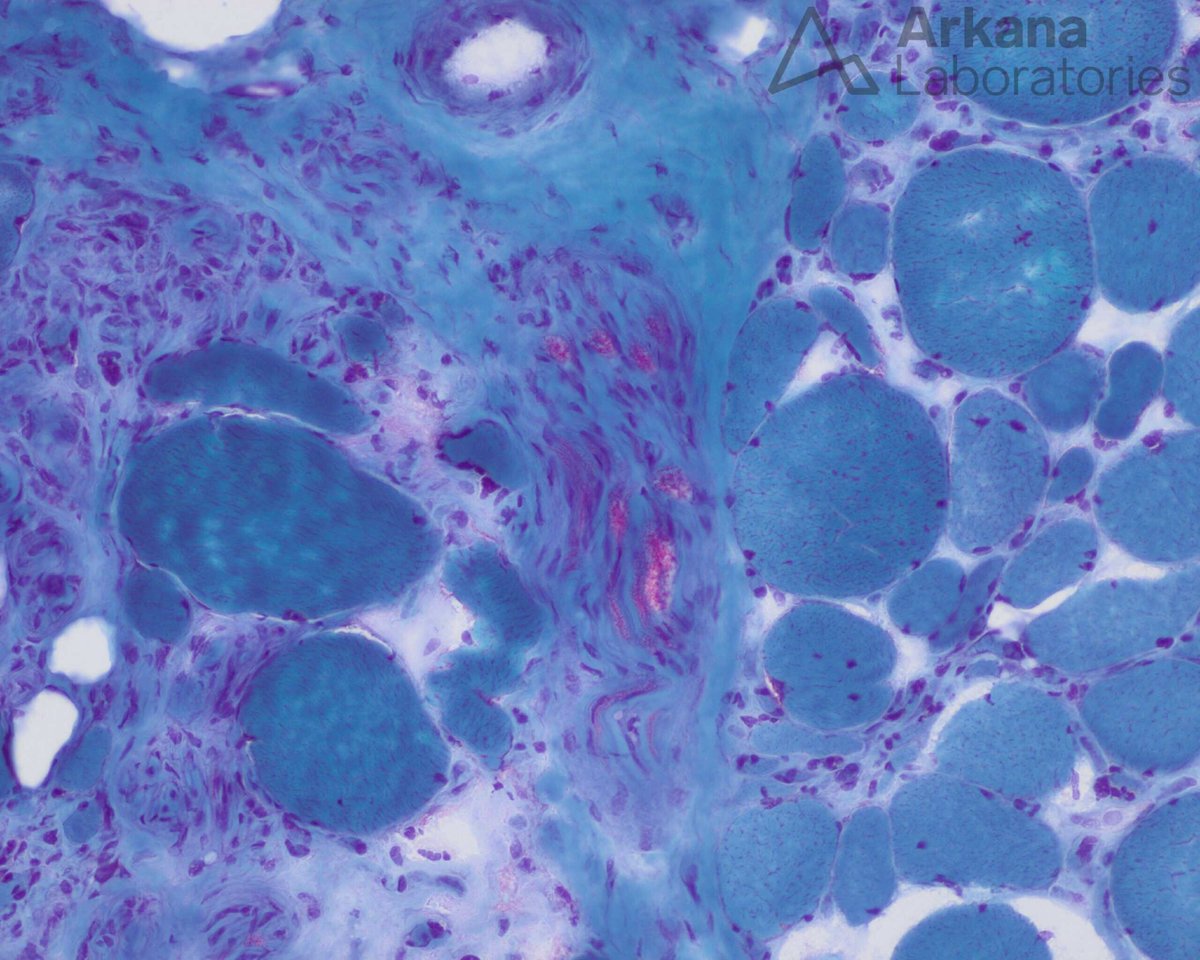
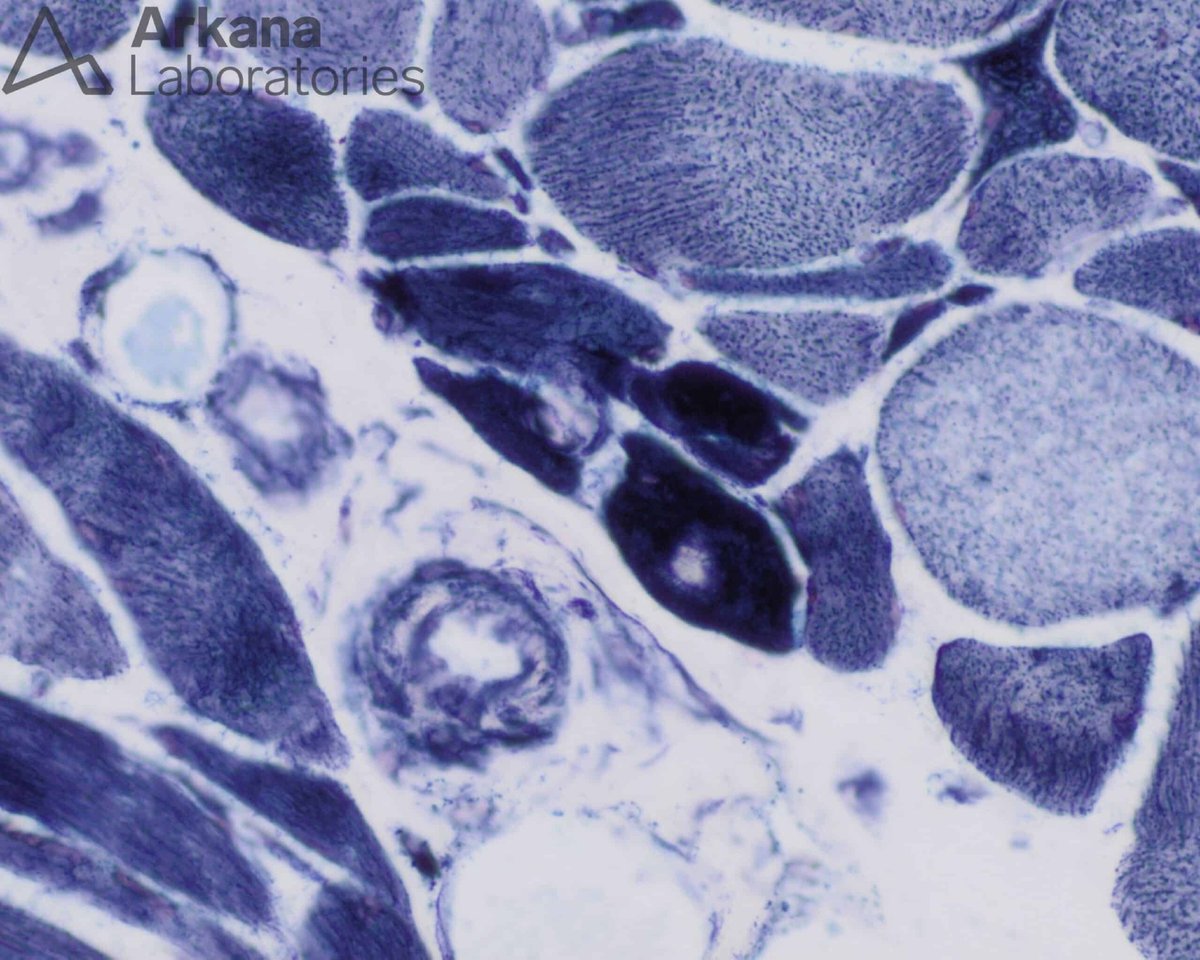
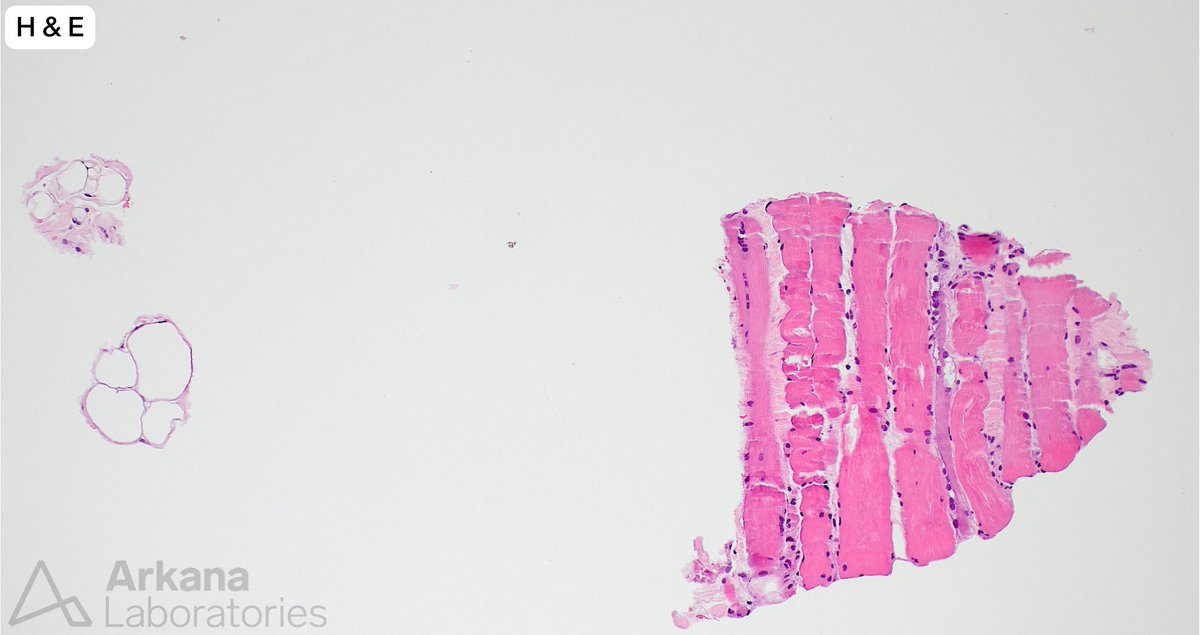
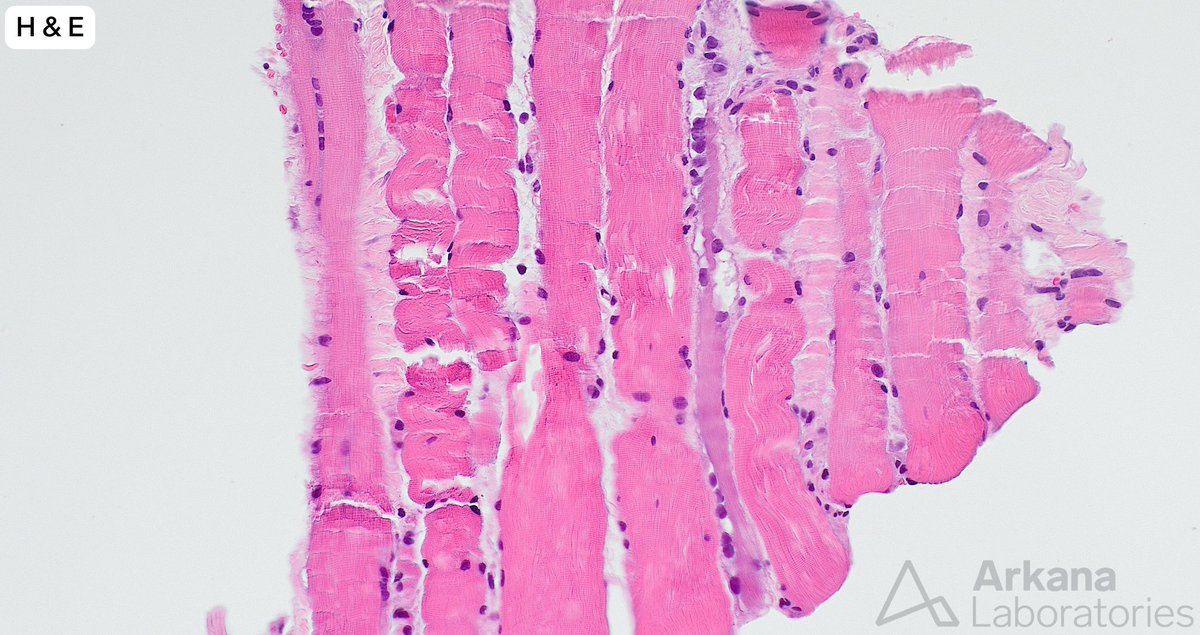
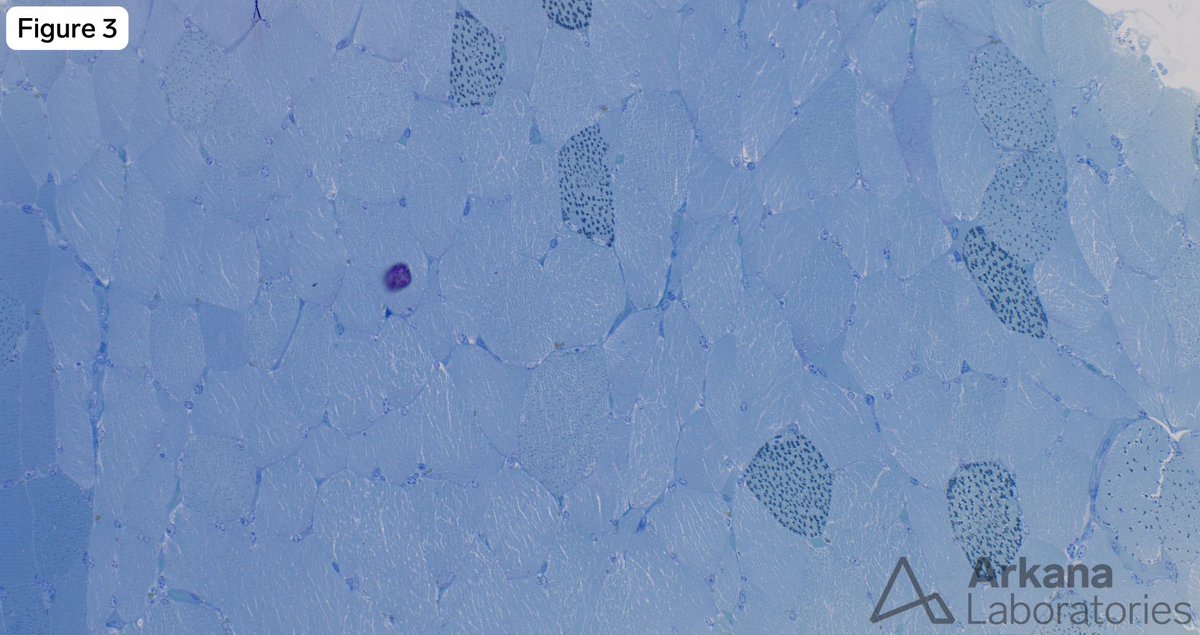
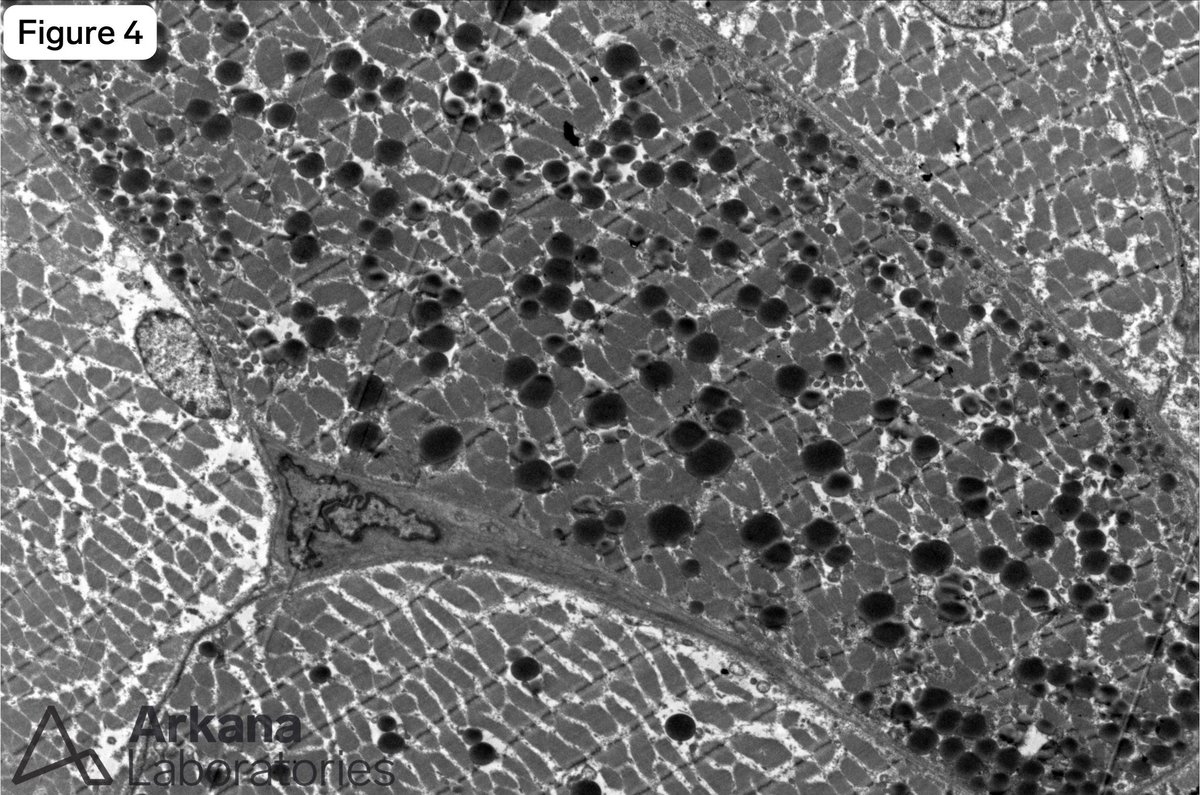
The patient is a teenage male with past medical history end-stage renal dialysis and heart failure who presented with nausea/vomiting and diarrhea.
Which gene is classically mutated in congenital myopathy with cardiomyopathy and features seen in the provided images?
A. RYR1
B. TNNT1
C. C9orf72
D. TTN
#NeuroNotes #neuropath #pathology #neuromuscularpath
1
8
715
May 27
Clinical History:
- History: 68-year-old man with 1 week of bilateral proximal upper and lower extremity weakness and 1 month of facial, eyebrow, neck, chest, and back rash (initially diagnosed as seborrheic dermatitis)
- PMH: HTN, PVD, asthma, hyperlipidemia, GERD, type 1 DM with retinopathy, IgA deficiency, hypothyroidism, former light smoker
- FH: Stroke, diabetes, arthritis, cancer, macular degeneration, heart disease
- Meds: Atorvastatin, insulin, levothyroxine, zolpidem; treated with Solu-Medrol and prednisone
- Physical exam: Mild-moderate proximal weakness, lower extremity edema
- MRI: Diffuse heterogeneous edema of bilateral quadriceps, adductors, and sartorius, suspicious for inflammatory myopathy
- Labs: CK peaked at 1570, trending down to 680; aldolase 20; mildly elevated CRP; ANA, Lyme, and RF negative; HMGCR Ab, MG panel, extended myositis and ENA panels pending
The primary pathology shown here is:
A. Necrotizing myopathic process
B. Eosinophil mediated inflammatory process
C. T-cell mediated inflammatory process
D. Macrophagic myofasciitis
#NeuroNotes #neuropath #pathology #neuromuscularpath
1
3
7
980
May 26
The answer is: B. Immune-mediated, necrotizing myopathy
To learn more, head to our blog: arkanalabs.com/mxa-positive-…
#neuropath #neuromuscular #neuronotes #pathology
1
2
207
May 25
Clinical History:
- History: 68-year-old man with 1 week of bilateral proximal upper and lower extremity weakness and 1 month of facial, eyebrow, neck, chest, and back rash (initially diagnosed as seborrheic dermatitis)
- PMH: HTN, PVD, asthma, hyperlipidemia, GERD, type 1 DM with retinopathy, IgA deficiency, hypothyroidism, former light smoker
- FH: Stroke, diabetes, arthritis, cancer, macular degeneration, heart disease
- Meds: Atorvastatin, insulin, levothyroxine, zolpidem; treated with Solu-Medrol and prednisone
- Physical exam: Mild-moderate proximal weakness, lower extremity edema
- MRI: Diffuse heterogeneous edema of bilateral quadriceps, adductors, and sartorius, suspicious for inflammatory myopathy
- Labs: CK peaked at 1570, trending down to 680; aldolase 20; mildly elevated CRP; ANA, Lyme, and RF negative; HMGCR Ab, MG panel, extended myositis and ENA panels pending
MxA staining is not characteristic of:
A. Dermatomyositis
B. Immune-mediated, necrotizing myopathy
C. Lupus myositis
D. Viral myositis
#NeuroNotes #neuropath #pathology #neuromuscularpath

2
1
11
1,955
May 21
The answer is: D. Ischemia
To learn more, head to our blog: arkanalabs.com/vasculitis-wi…
#neuropath #neuromuscular #neuronotes #pathology
May 20
Clinical History:
- History: 68-year-old man with 1 week of bilateral proximal upper and lower extremity weakness and 1 month of facial, eyebrow, neck, chest, and back rash (initially diagnosed as seborrheic dermatitis).
- PMH: HTN, PVD, asthma, hyperlipidemia, GERD, type 1 DM with retinopathy, IgA deficiency, hypothyroidism, former light smoker.
- FH: Stroke, diabetes, arthritis, cancer, macular degeneration, heart disease.
- Meds: Atorvastatin, insulin, levothyroxine, zolpidem; treated with Solu-Medrol and prednisone.
- Physical exam: Mild-moderate proximal weakness, lower extremity edema.
- MRI: Diffuse heterogeneous edema of bilateral quadriceps, adductors, and sartorius, suspicious for inflammatory myopathy.
- Labs: CK peaked at 1570, trending down to 680; aldolase 20; mildly elevated CRP; ANA, Lyme, and RF negative; HMGCR Ab, MG panel, extended myositis and ENA panels pending.
What is the most likely direct mechanism of muscle injury?
A. T-cell mediated inflammation of myofibers
B. B-cell mediated inflammation of myofibers
C. Metabolic myopathy
D. Ischemia
#NeuroNotes #neuropath #pathology #neuromuscularpath


2
915
May 20
Clinical History:
- History: 68-year-old man with 1 week of bilateral proximal upper and lower extremity weakness and 1 month of facial, eyebrow, neck, chest, and back rash (initially diagnosed as seborrheic dermatitis).
- PMH: HTN, PVD, asthma, hyperlipidemia, GERD, type 1 DM with retinopathy, IgA deficiency, hypothyroidism, former light smoker.
- FH: Stroke, diabetes, arthritis, cancer, macular degeneration, heart disease.
- Meds: Atorvastatin, insulin, levothyroxine, zolpidem; treated with Solu-Medrol and prednisone.
- Physical exam: Mild-moderate proximal weakness, lower extremity edema.
- MRI: Diffuse heterogeneous edema of bilateral quadriceps, adductors, and sartorius, suspicious for inflammatory myopathy.
- Labs: CK peaked at 1570, trending down to 680; aldolase 20; mildly elevated CRP; ANA, Lyme, and RF negative; HMGCR Ab, MG panel, extended myositis and ENA panels pending.
What is the most likely direct mechanism of muscle injury?
A. T-cell mediated inflammation of myofibers
B. B-cell mediated inflammation of myofibers
C. Metabolic myopathy
D. Ischemia
#NeuroNotes #neuropath #pathology #neuromuscularpath
1
1
6
1,311
May 18
Clinical History:
- History: 68-year-old man with 1 week of bilateral proximal upper and lower extremity weakness and 1 month of facial, eyebrow, neck, chest, and back rash (initially diagnosed as seborrheic dermatitis).
- PMH: HTN, PVD, asthma, hyperlipidemia, GERD, type 1 DM with retinopathy, IgA deficiency, hypothyroidism, former light smoker.
- FH: Stroke, diabetes, arthritis, cancer, macular degeneration, heart disease.
- Meds: Atorvastatin, insulin, levothyroxine, zolpidem; treated with Solu-Medrol and prednisone.
- Physical exam: Mild-moderate proximal weakness, lower extremity edema.
- MRI: Diffuse heterogeneous edema of bilateral quadriceps, adductors, and sartorius, suspicious for inflammatory myopathy.
- Labs: CK peaked at 1570, trending down to 680; aldolase 20; mildly elevated CRP; ANA, Lyme, and RF negative; HMGCR Ab, MG panel, extended myositis and ENA panels pending.’
What is the primary etiology in this muscle based on this histology alone?
A. Myopathic
B. Dystrophic
C. Neurogenic
D. Inflammatory
#NeuroNotes #neuropath #pathology #neuromuscularpath
9
1,845


Mar 22
Honestly, I fell behind on content and posting the past few days because I was building.
NeuroBrowse picked up:
- AI Vision
- Enhanced YouTube summarization capabilities
- Research Mode
- A custom support agent
And that’s not even all of it.
After this submission to the Chrome Store, you’ll be able to try NeuroBrowse and NeuroNotes together much more easily this week.
Still figuring out my systems as a solo founder. Some weeks, building takes priority over posting. But every day I get a step closer to having it all aligned.
Still building the company from nothing into something .
Founders, are your systems already in place or are you still working on them?
#buildinpublic #founders

2
38
This 50-year-old patient presented with progressively worsening muscle weakness of one month duration. Their past medical history was significant for type 2 diabetes, hyperlipidemia, hypertension and hypothyroidism. Statin medication (atorvastatin) was held upon admission. The patient’s home medication list included levothyroxine. They were treated with steroid prior to muscle biopsy.
A needle core biopsy was performed of the left thigh. A minute fragment of fibrous tissue was present in tissue available for frozen section. The provided images (low and high magnification) show the total tissue available for evaluation in the formalin-fixed paraffin embedded tissue. The tiny fragment of glutaraldehyde-fixed tissue available for toluidine blue stained sections (image not provided) showed features similar to those seen in the FFPE tissue sections, and a few necrotic myofibers.
What is the best pathologic diagnosis?
#NeuroNotes #neuropath #pathology #neuromuscularpath
1
2
6
934
Feb 21
Everyone's rushing to ship because of FOMO.
I'm building patient.
I'm not vibe coding random projects. I'm building a company.
Neurolayer Labs-A privacy first AI ecosystem where every product works together.
NeuroBrowse is your AI powered browser assistant.
NeuroNotes is your personal workspace.
Different tools, One ecosystem.
Two Products Live. Site updated last night:
➡️Real-time video demo (not sped up)
➡️Interactive cost calculator
➡️Full ecosystem showcase
Yes i build with AI. But AI does not design the brand , plan the business, choose the architecture , and doesn't decide what ships and what doesn't.
It cant do anything unless I type my idea my vision into it!
Open your favorite AI tool and don't type anything and see what happens.
It can only take what your thinking and work with that, if your thought or ideas change so does it.
I could've launched months ago with v1. But I'd rather launch once and launch right.
Still looking for 6 early adopters who want to help shape NeuroBrowse before the official launch.
DM me "Early" or check it out at ➡️ neurobrowse.io
#solofounder #AI
2
59
Feb 19
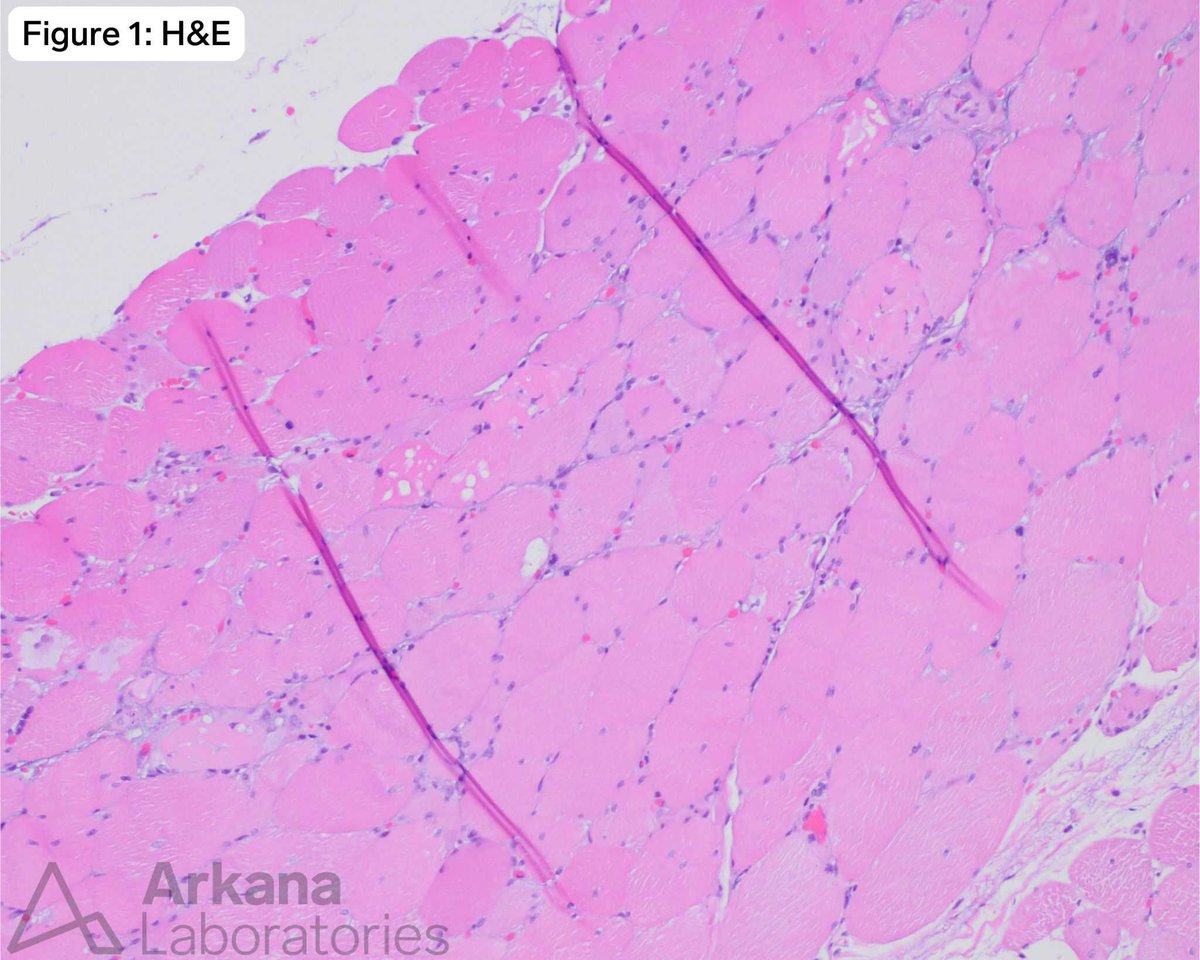
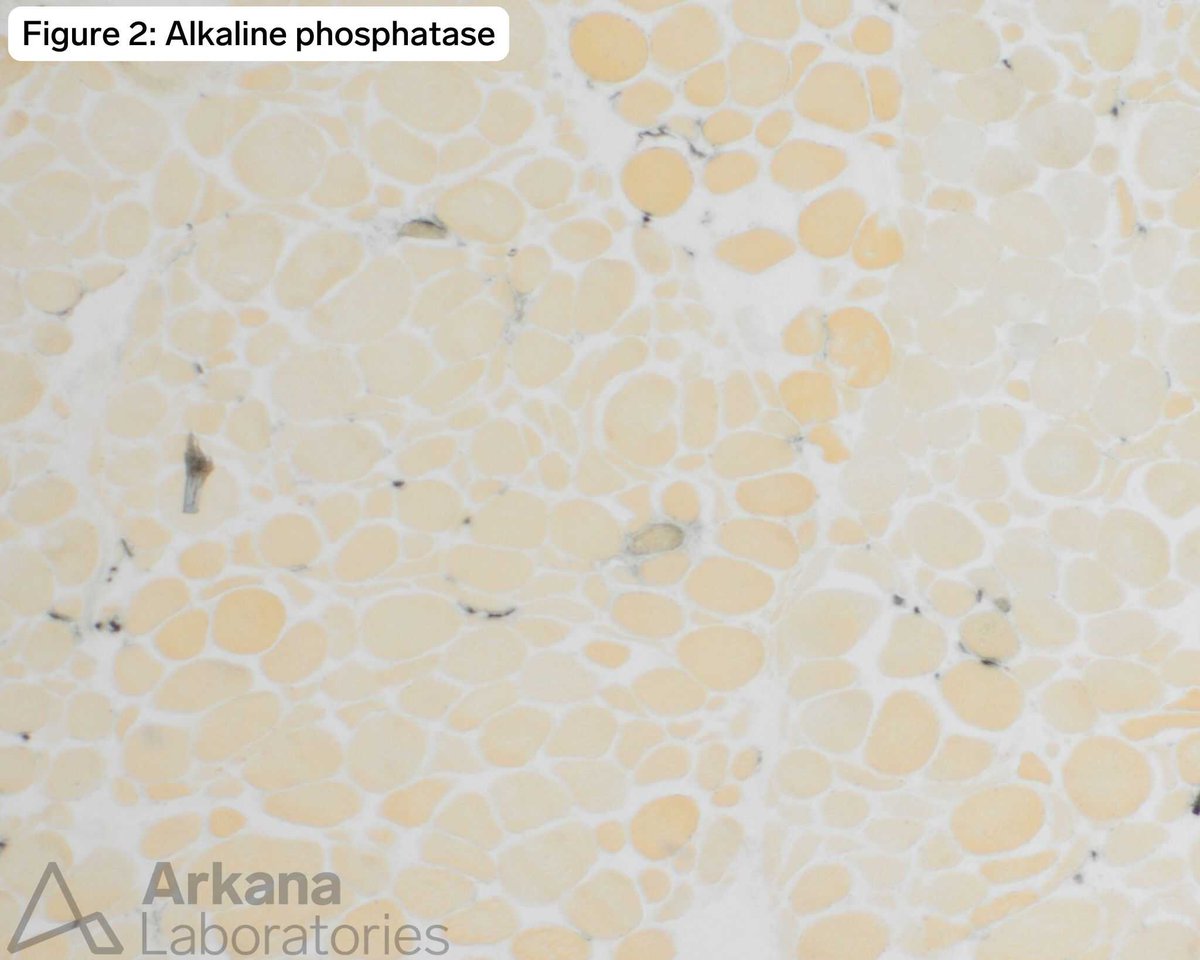
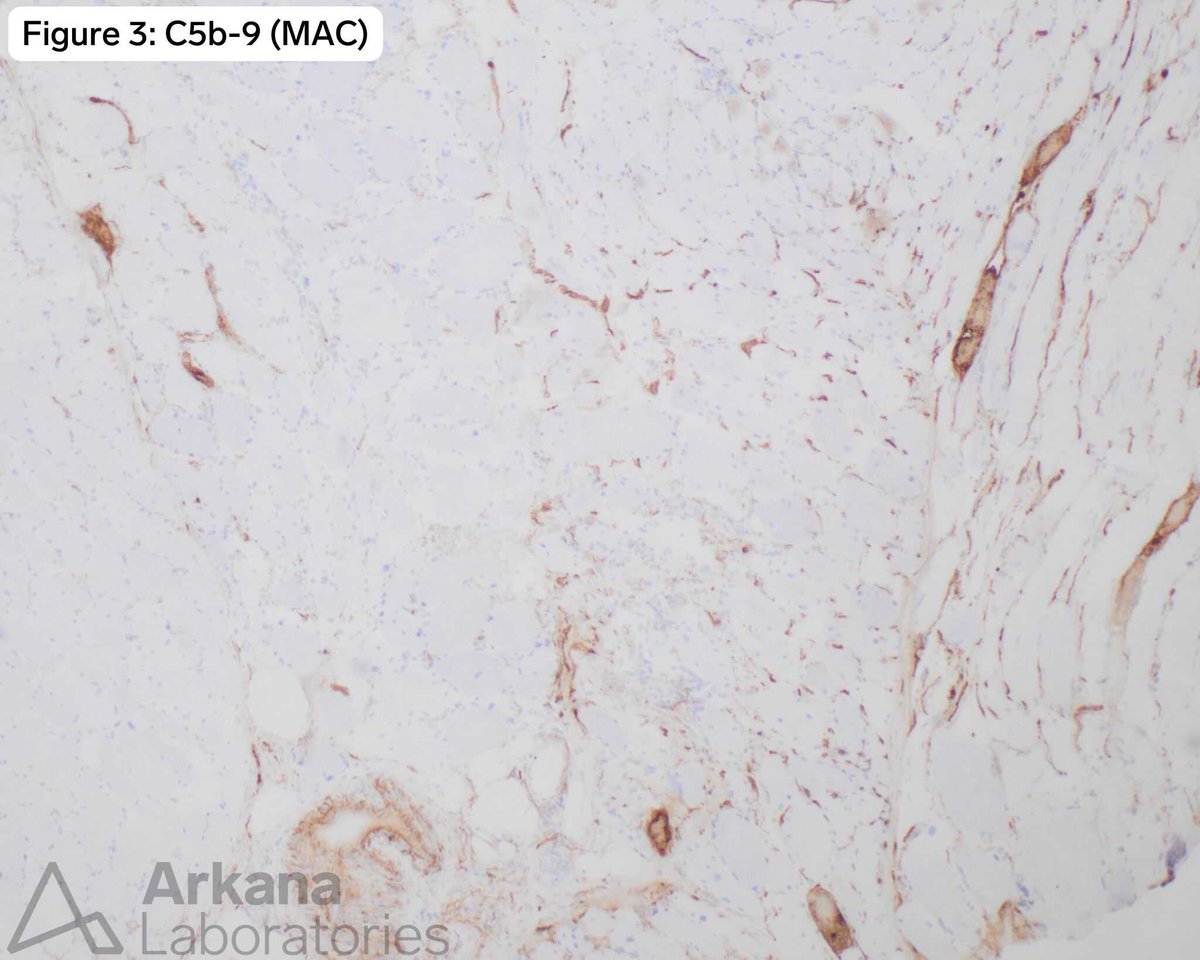
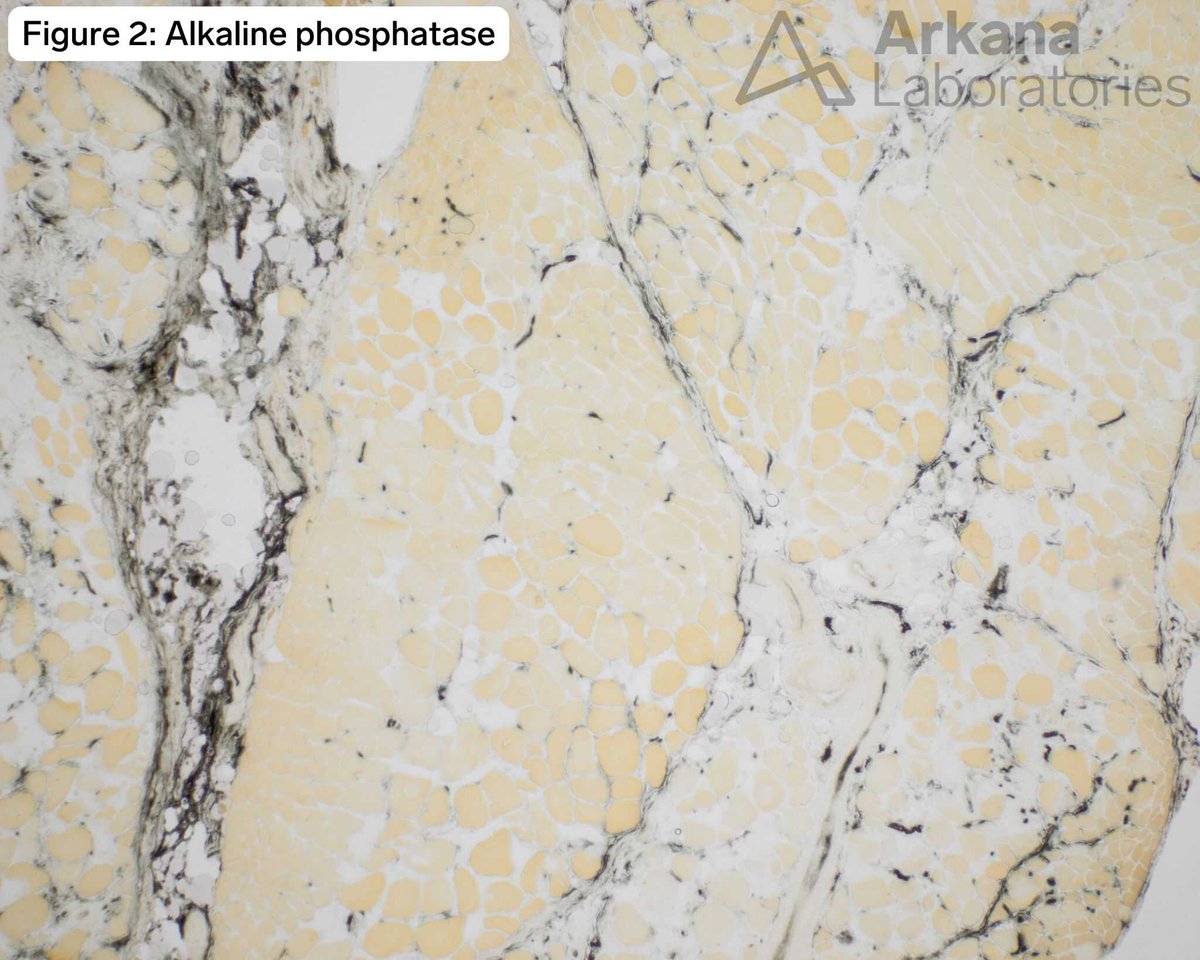
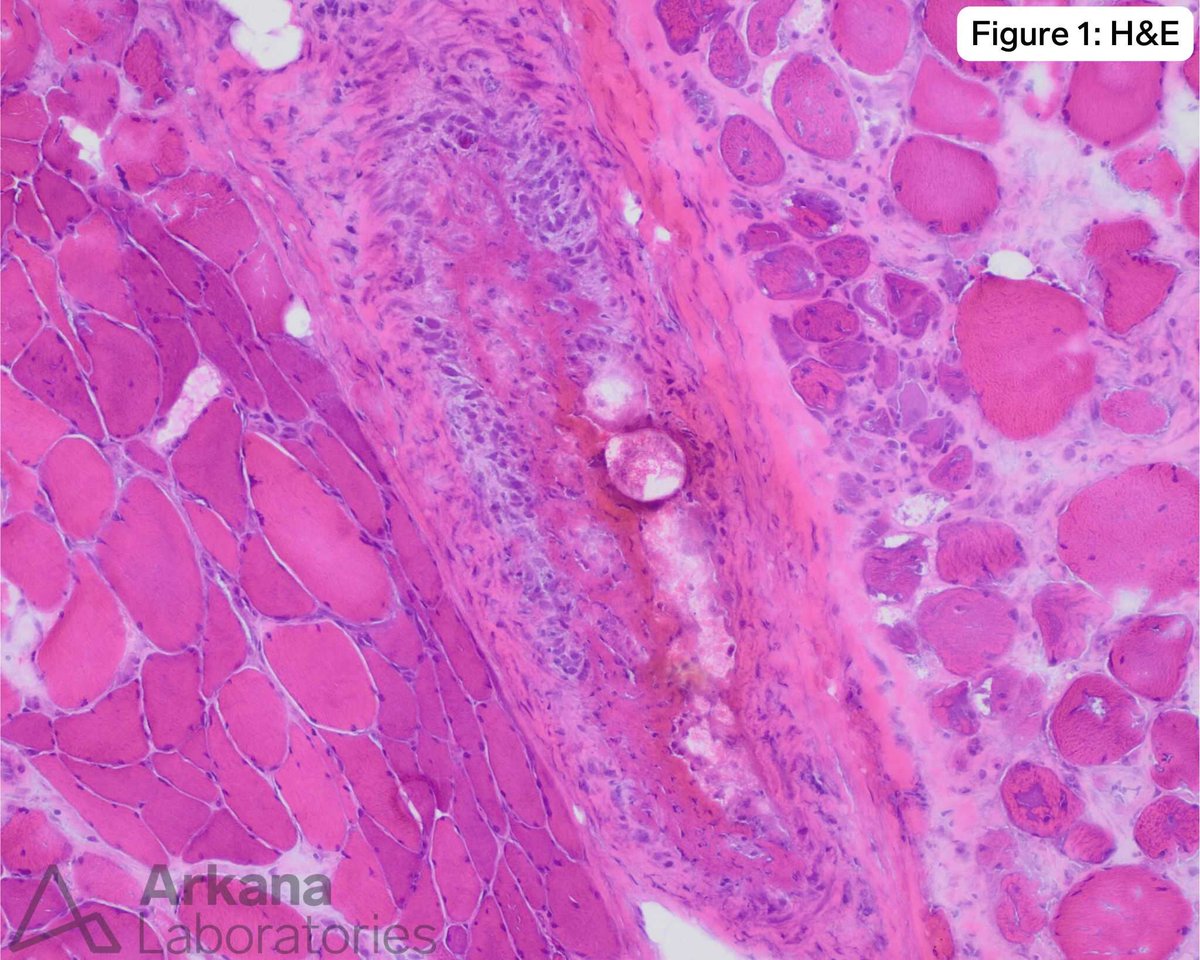
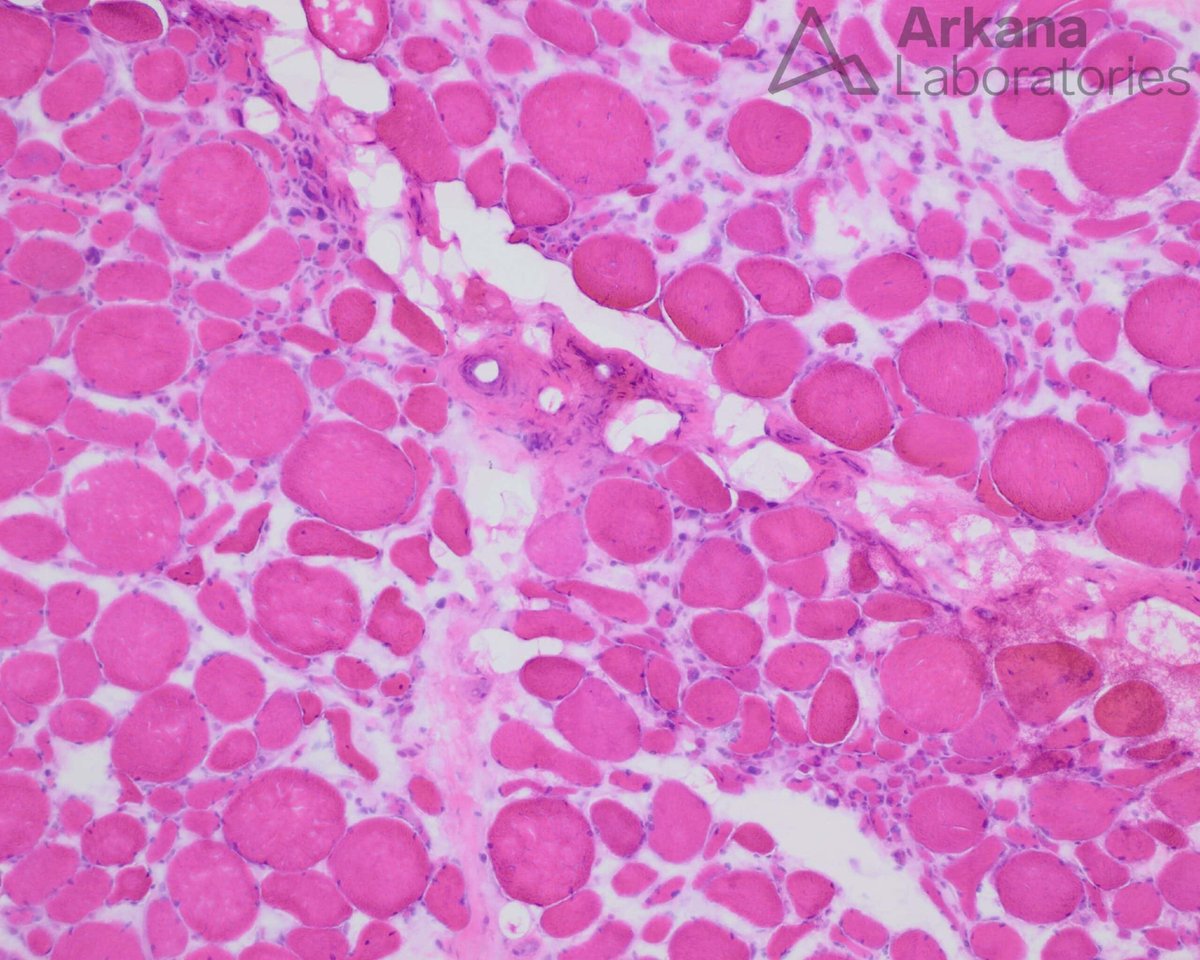
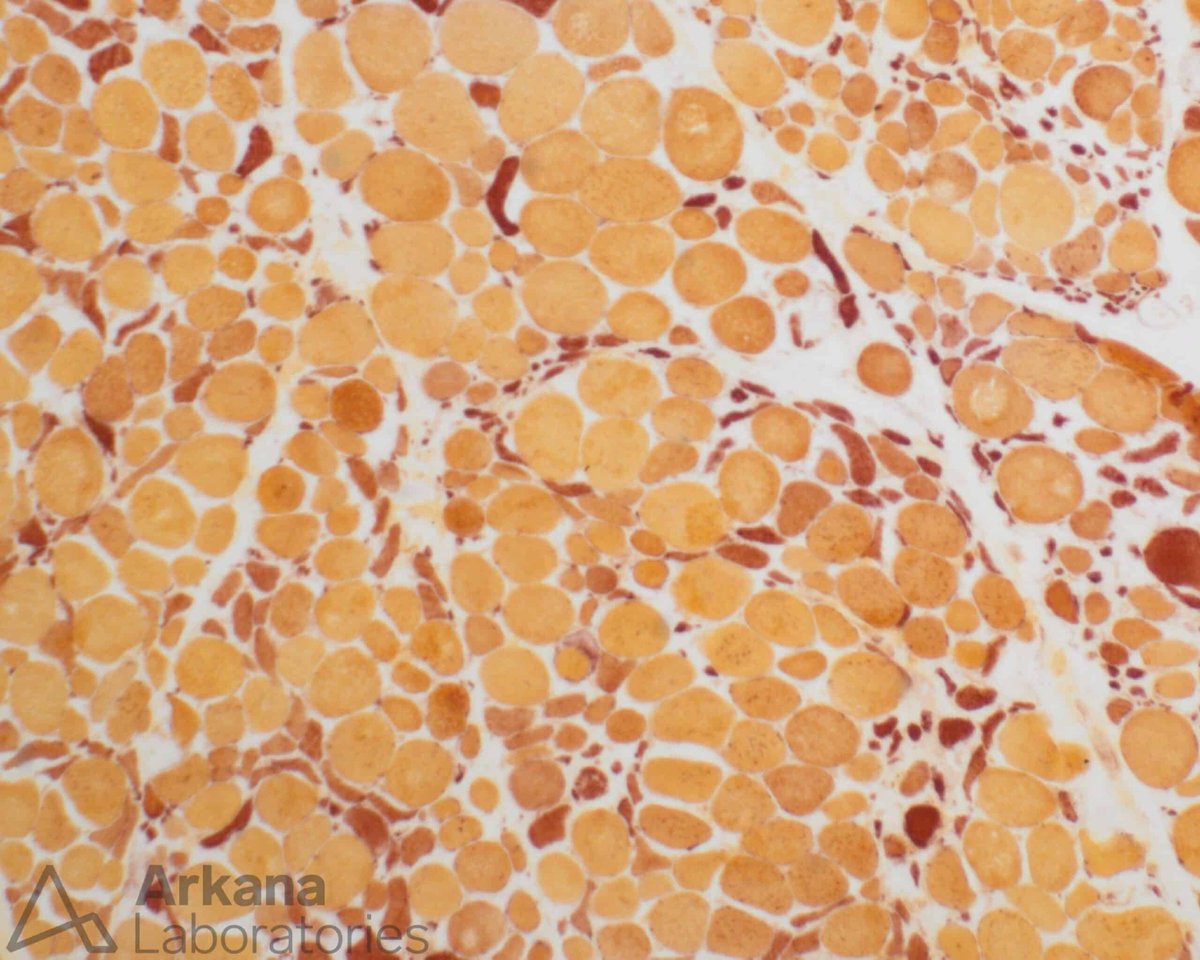
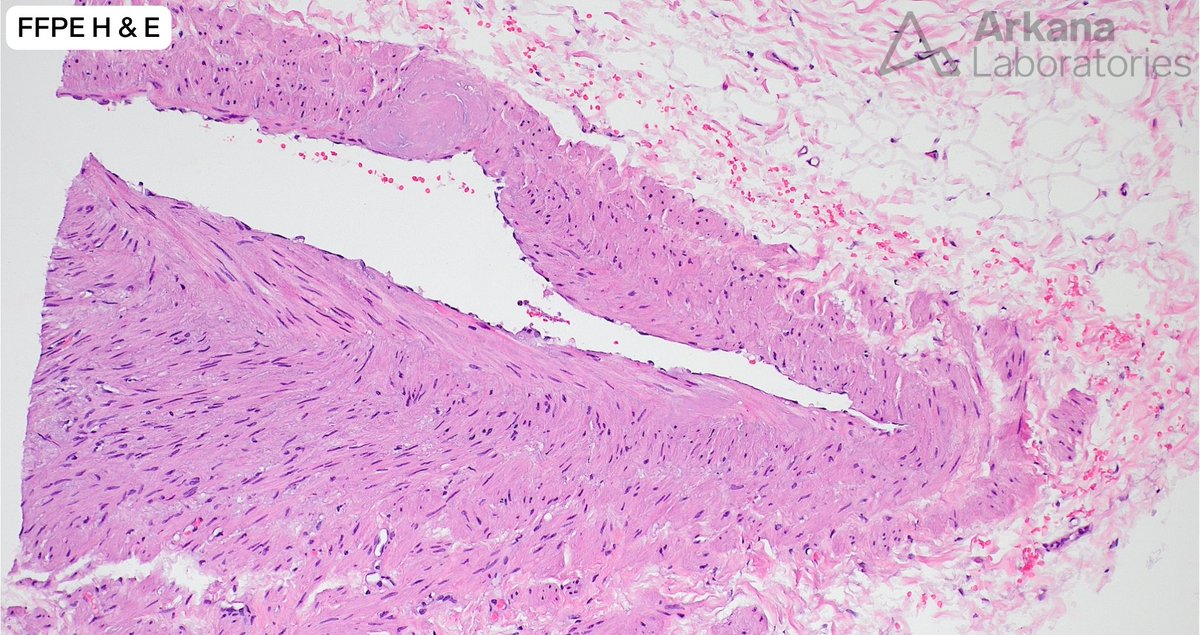
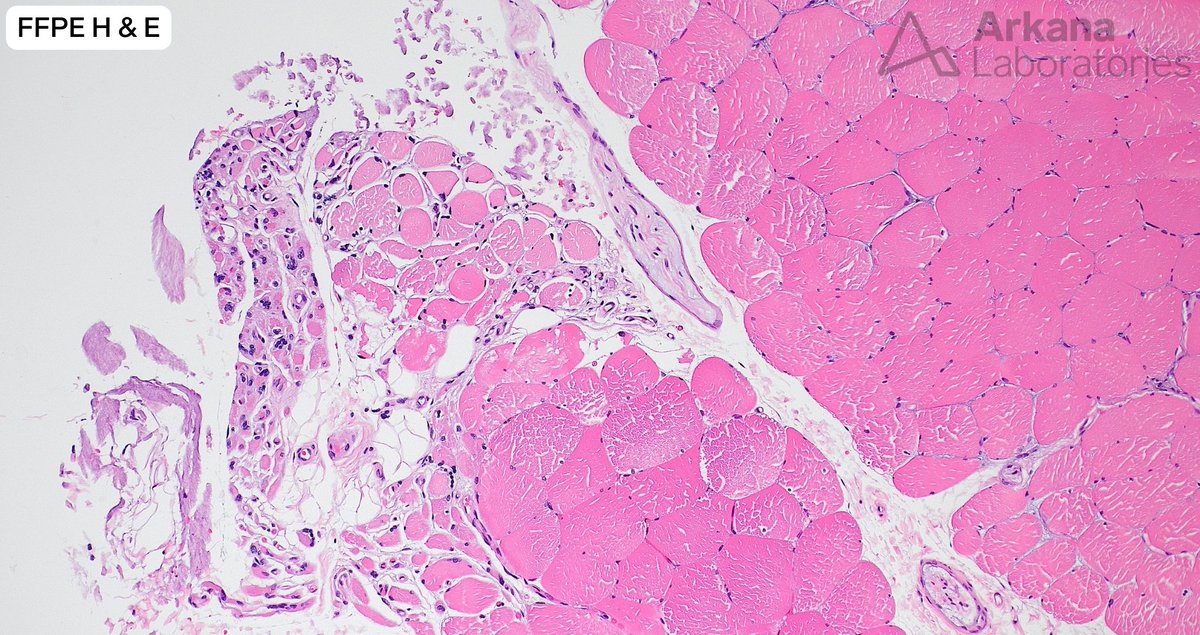
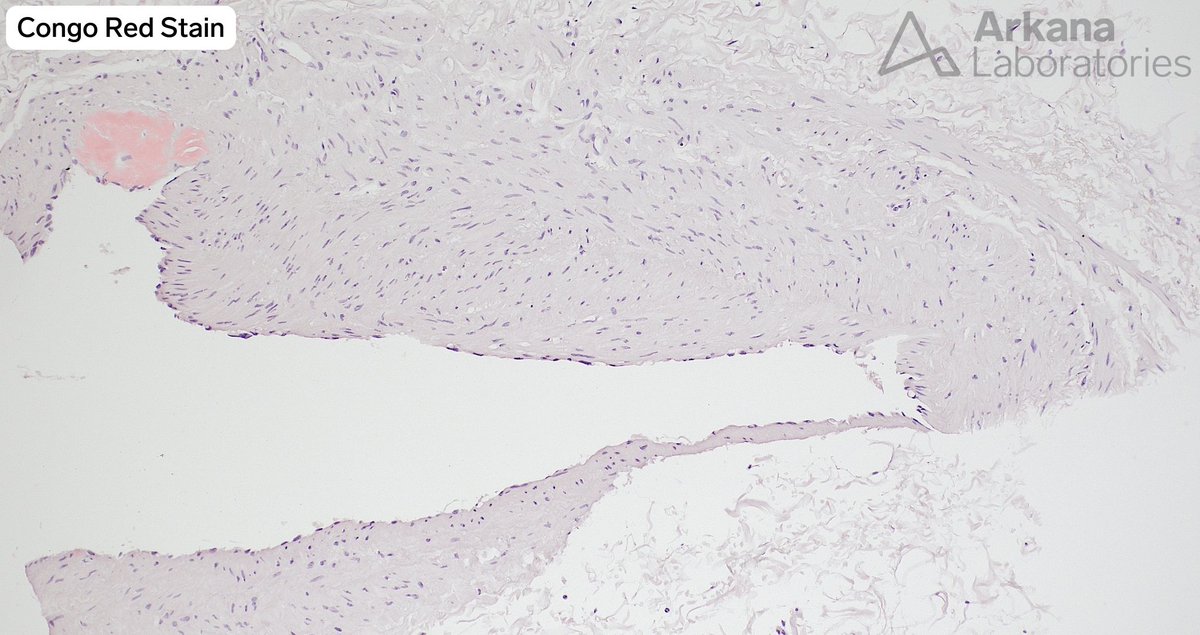
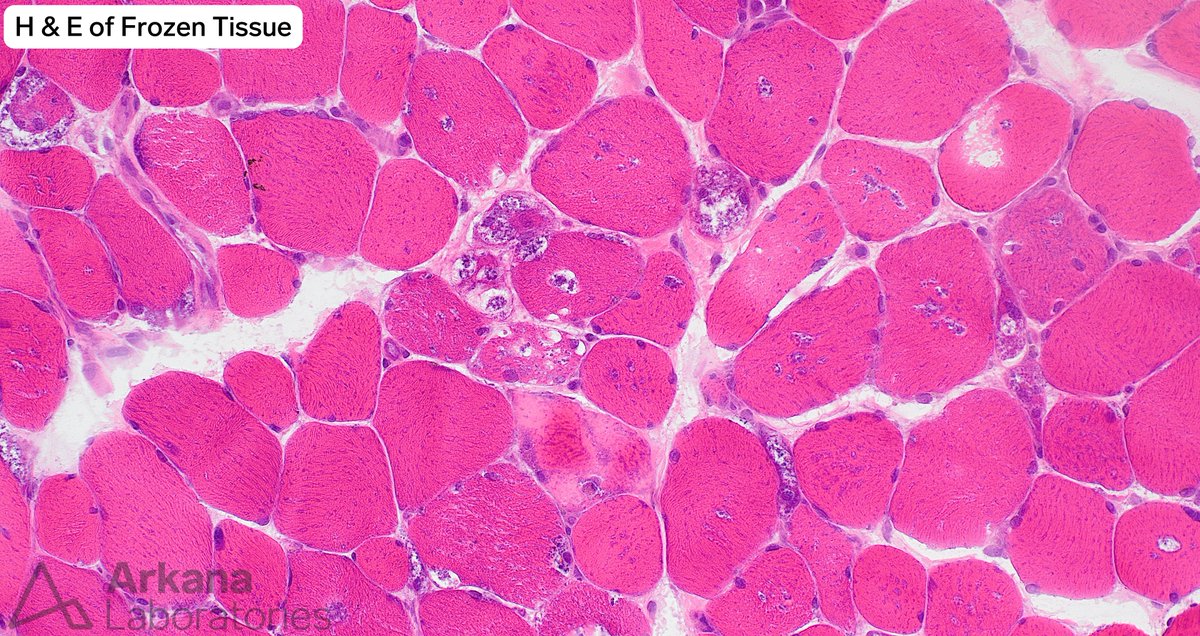
This 76-year-old male presented with complaints of muscle pain. Their past medical history is significant for Sjogren’s syndrome, fibromyalgia, peripheral neuropathy, hypertension and hyperlipidemia. Laboratory studies showed normal CPK and elevated CRP. No myotoxic medications were noted in the patient’s home medication list.
What are your diagnoses for the changes seen in the muscle biopsy (image #1) and the incidental finding that was seen in multiple blood vessels (images #2 and #3)? #neuronotes #neuropath
1
12
1,473
This 50-year-old patient presented with a one yearhistory of of persistent muscle weakness. They also had shortness of breath with exertion. Their past medical history is significant for seropositive rheumatoid arthritis which has been well-managed symptomatically for several years with hydroxychloroquine. Laboratory studies showed elevated CPK (1000-1600 range), positive rheumatoid factor (>120), ANA (1:120), positive SSA/SSB, and negative/normal myositis specific autoantibody panel, CCP, dsDNA, Scl-70, Smith/RNP, smooth muscle and ANCA autoantibodies. Electrodiagnostic studies (EMG/NCS) showed features of a chronic active distal symmetric length dependent axonal polyneuropathy. The patient’s home medication list also included CellCept and prednisone. Simvastatin had been previously discontinued without significant improvement in the patient’s symptoms. On physical examination the patient was noted to have weakness involving both lower legs.
What is your diagnosis based on clinical history, light microscopy and electron microscopy?
#NeuroNotes #neuropath #pathology #neuromuscularpath

1
2
5
536
29 Dec 2025
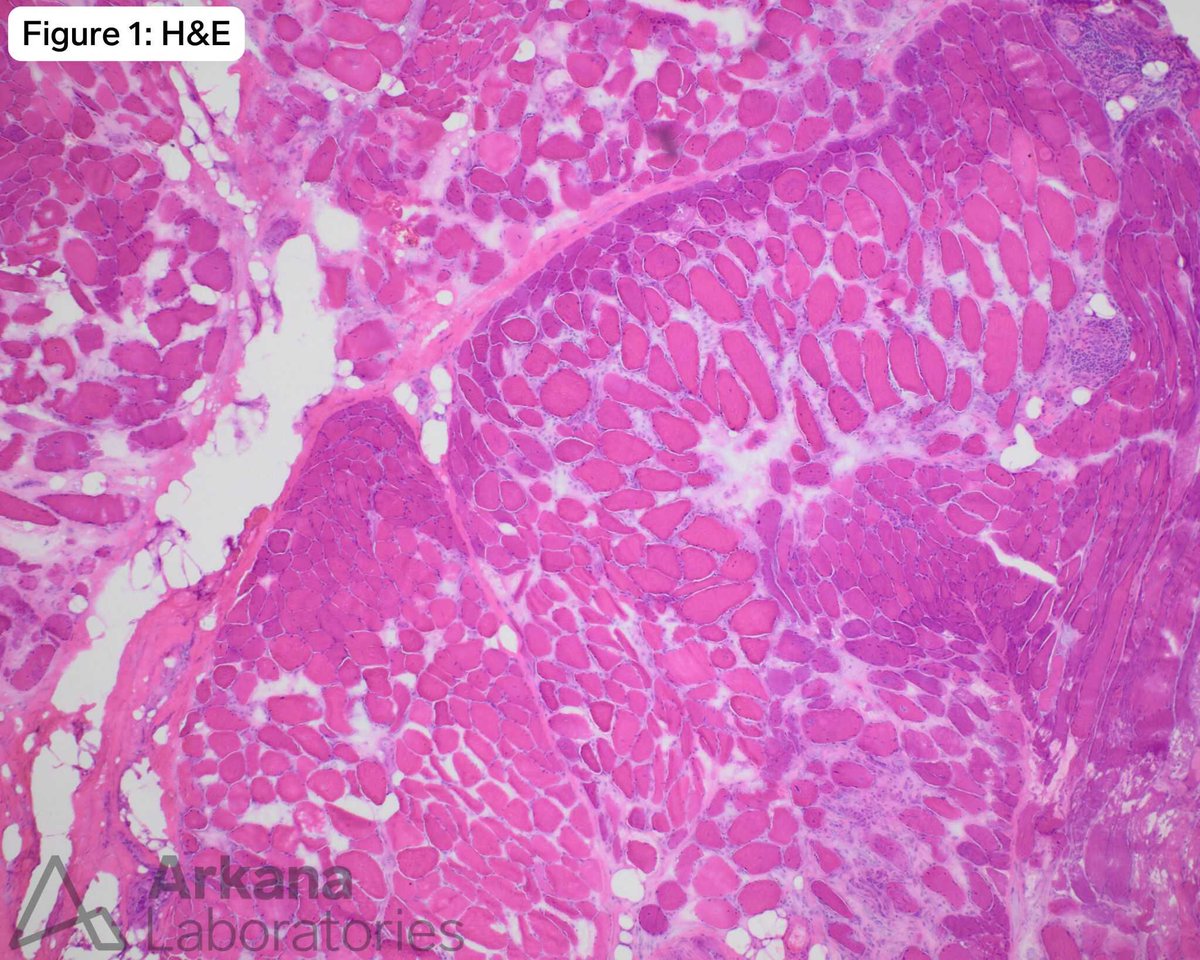
The patient is a 69-year-old male who presented with complaints of proximal lower extremity muscle weakness and BMI of 37. His home medication list includes atorvastatin. Bilateral thigh biopsies were performed to evaluate for myopathy.
The significant finding can be seen in all of the following, except:
A.SLONM
B. ACTA1 mutations
C.HIV
D.Duchenne muscular dystrophy
#NeuroNotes #neuropath #pathology #neuromuscularpath
1
3
12
1,157
23 Dec 2025
The answer is: Riboflavin
To learn more, head to our blog: arkanalabs.com/lipid-storage…
#neuropath #neuromuscular #neuronotes #pathology
2
308
22 Dec 2025
The patient is a 77-year-old female with several months of progressive muscle weakness predominantly in her upper and lower proximal extremities. Medications include levothyroxine and atorvastatin. Lab results include a reportedly low CK, aldolase 92 U/L, negative myositis autoantibody panel, negative HMGCR autoantibody testing.
What treatment should be given immediately?
#NeuroNotes #neuropath #pathology #neuromuscularpath
3
8
992