
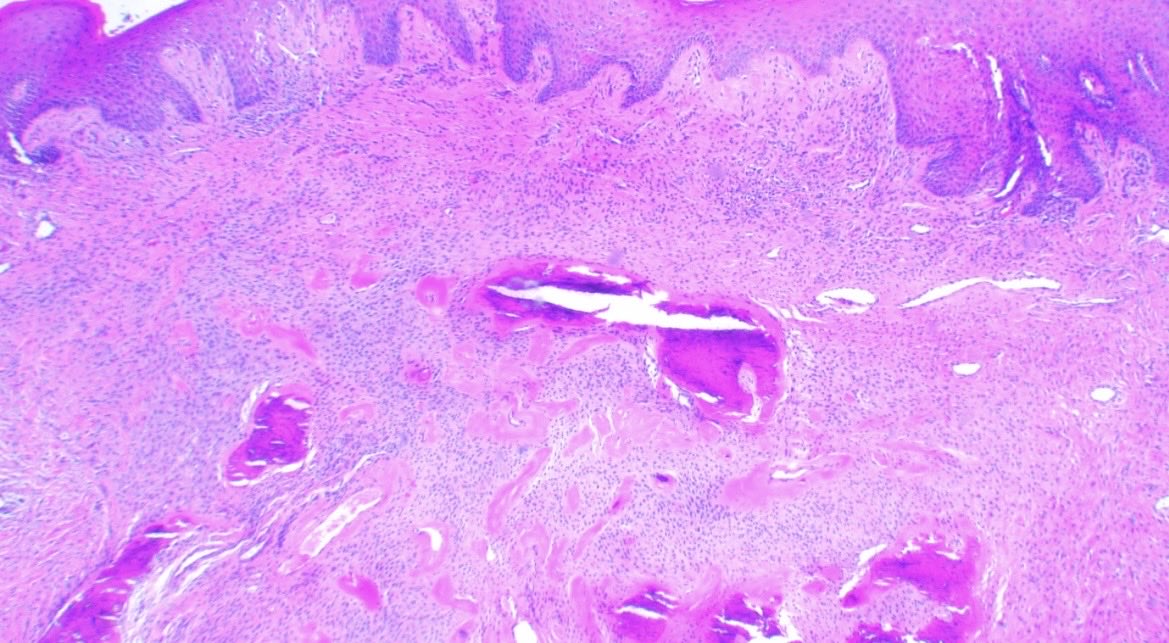
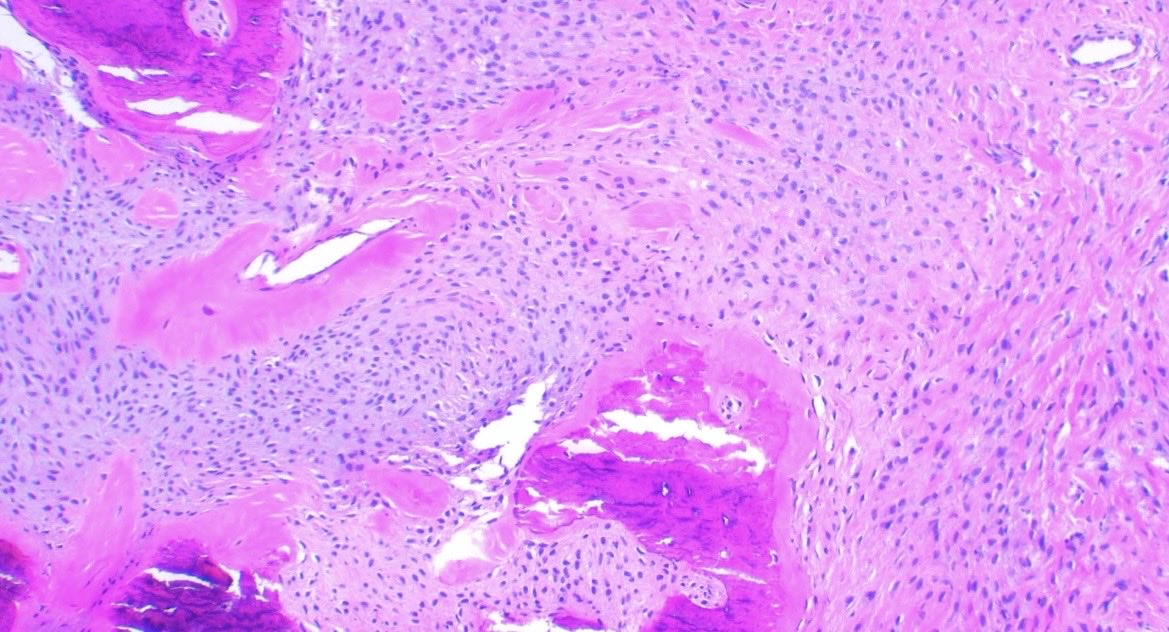
Dear pathologists
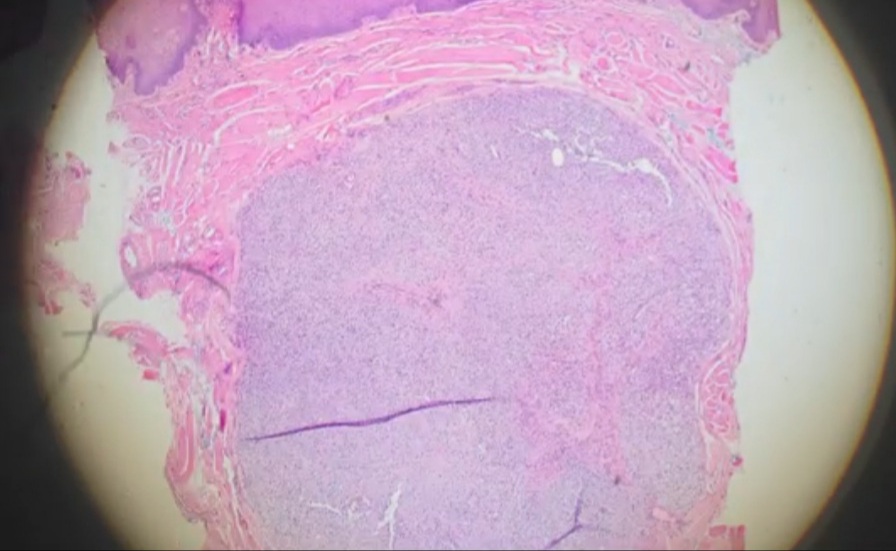
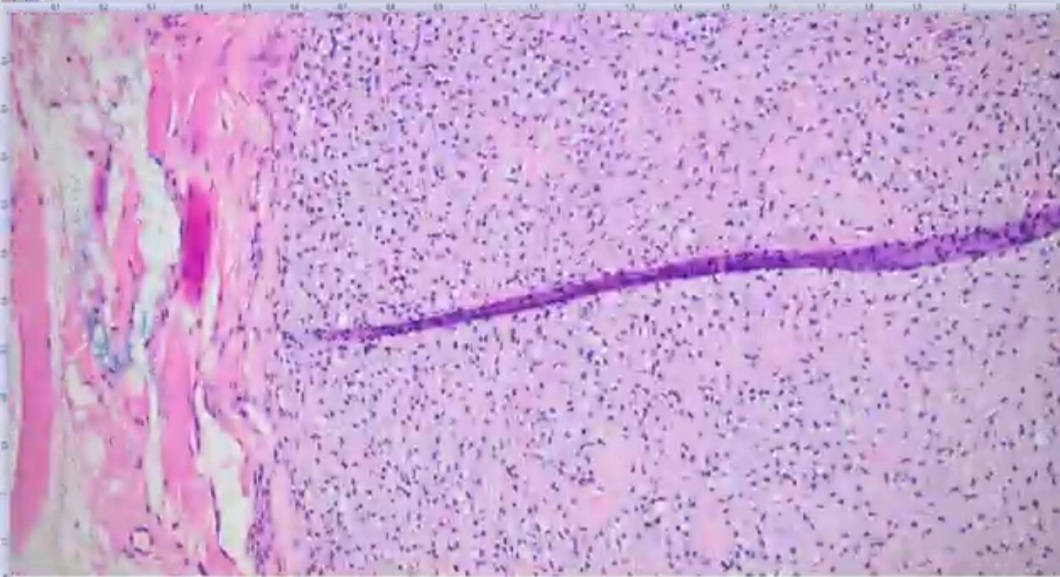
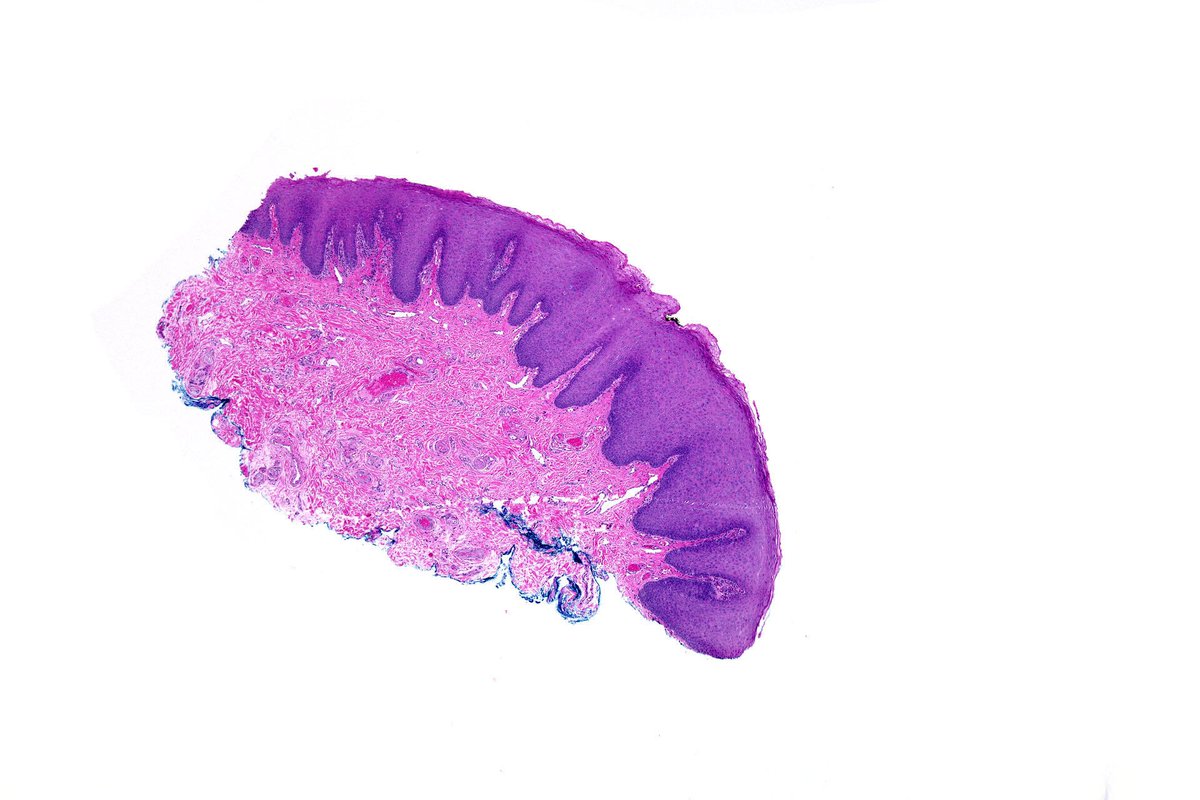
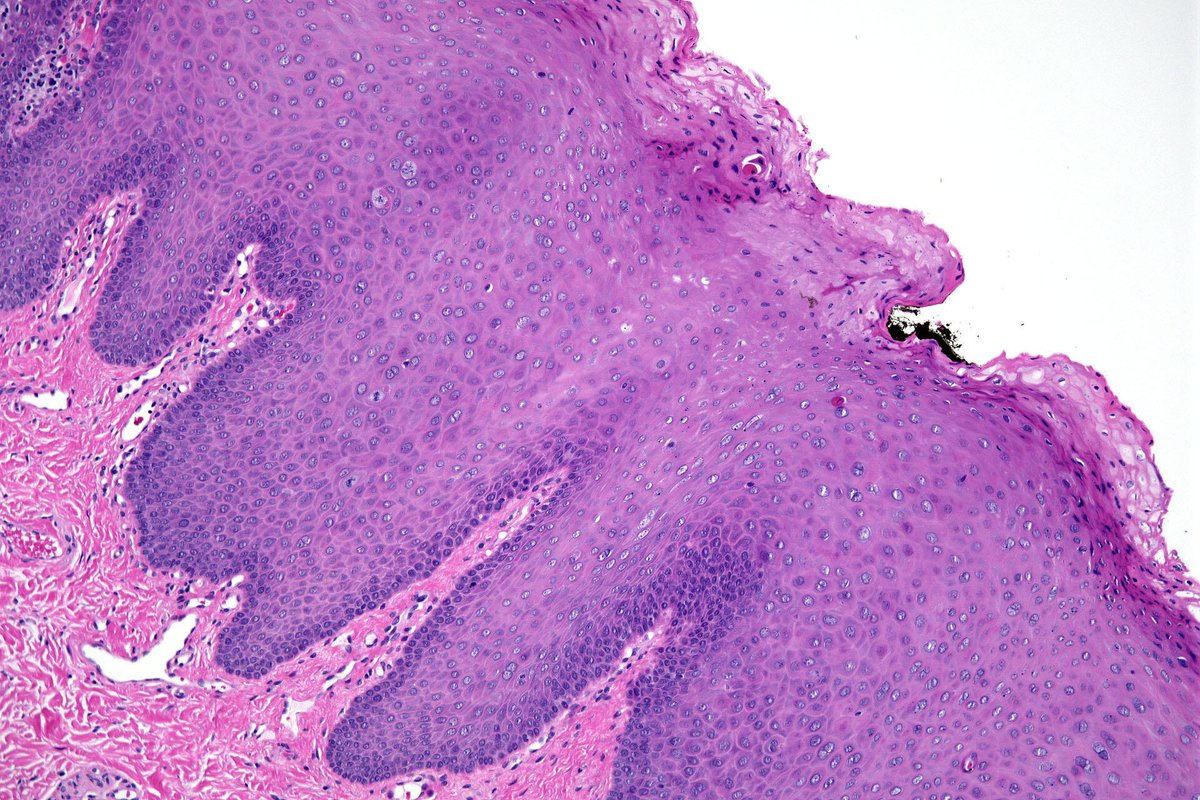
This is a case of radicular cyst
I was wondering why connective tissue became more blue in the area of hyperplastic epithelium? And whether it is described as myxoid?
#pathtwitter #oralpath
80

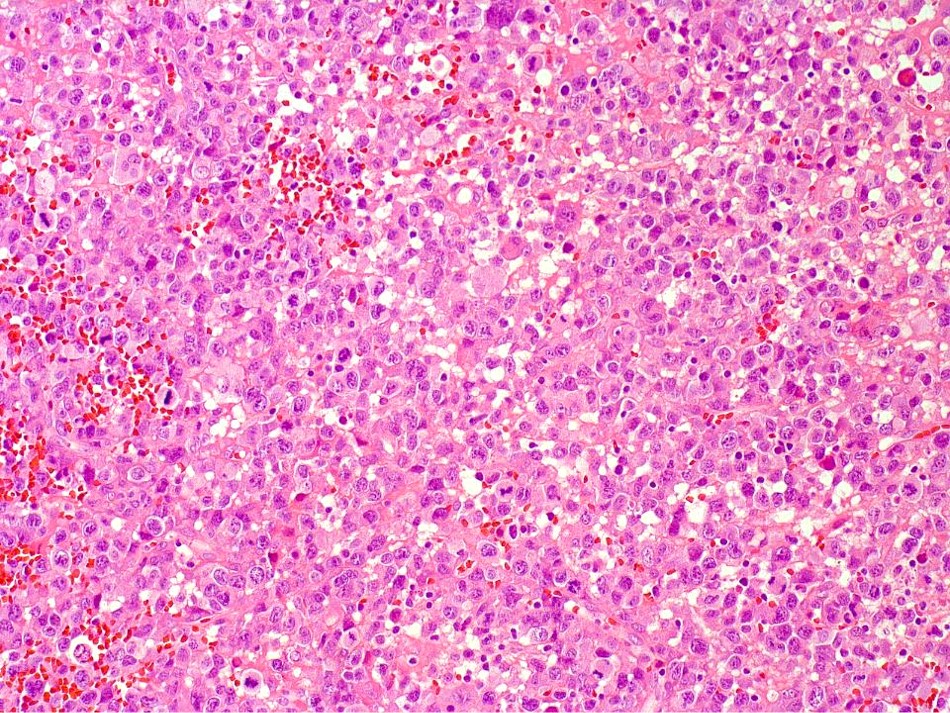
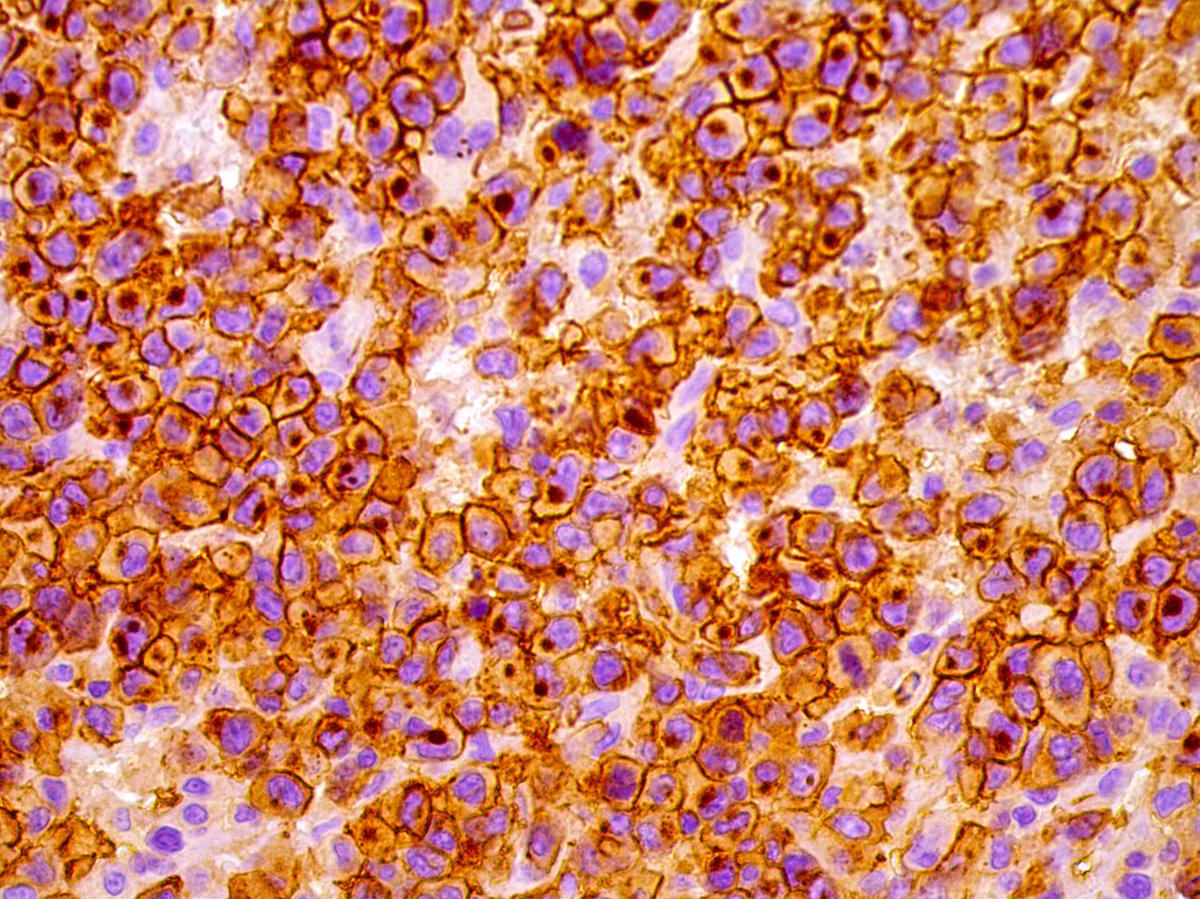
Anaplastic large cell lymphoma affecting the oral cavity (CD30/ALK)! Discover more in our @SpringerNature book Lymphoproliferative and granulomatous disorders of the oral cavity
link.springer.com/book/97830…
#Pathology #OralPath #OralMedicine #lymphoma #PathTwitter #hemepath

9
20
931

Apr 17

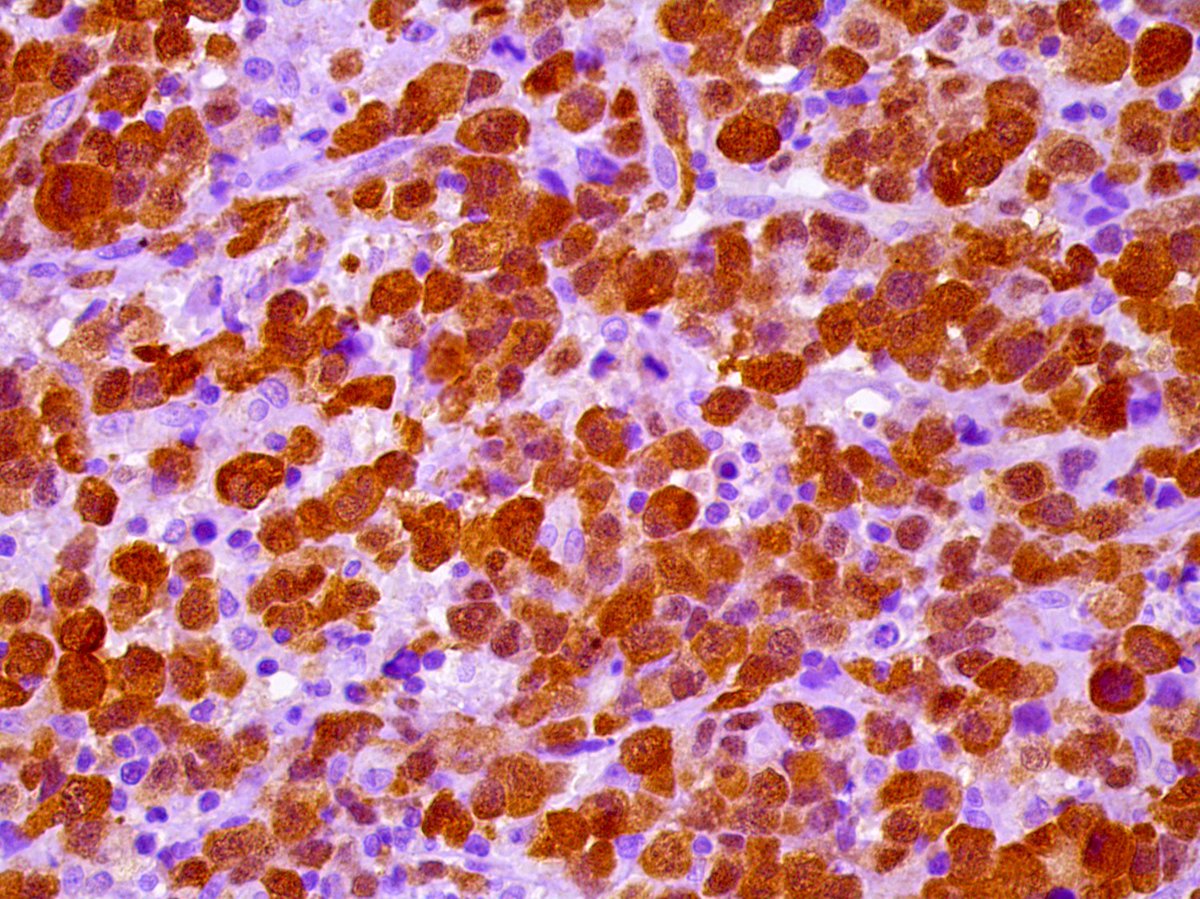
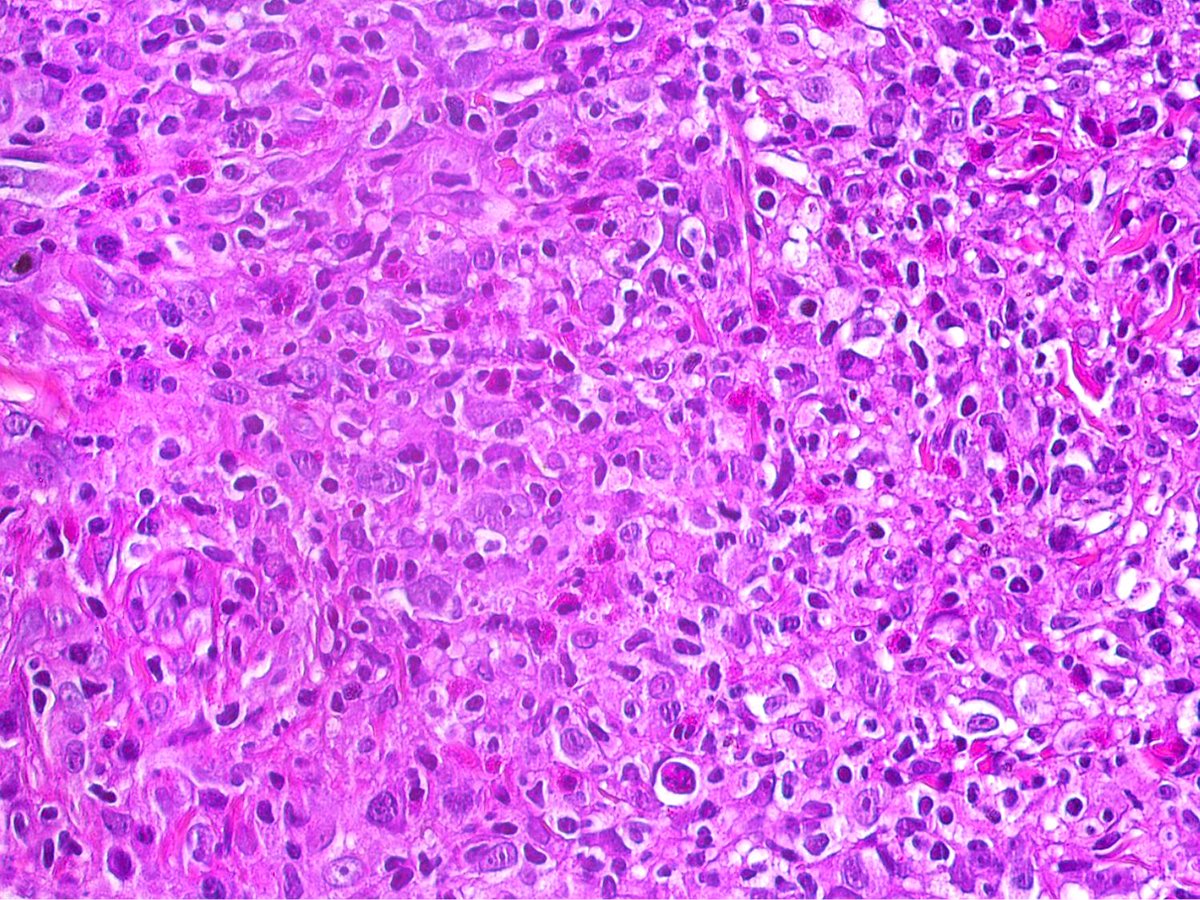
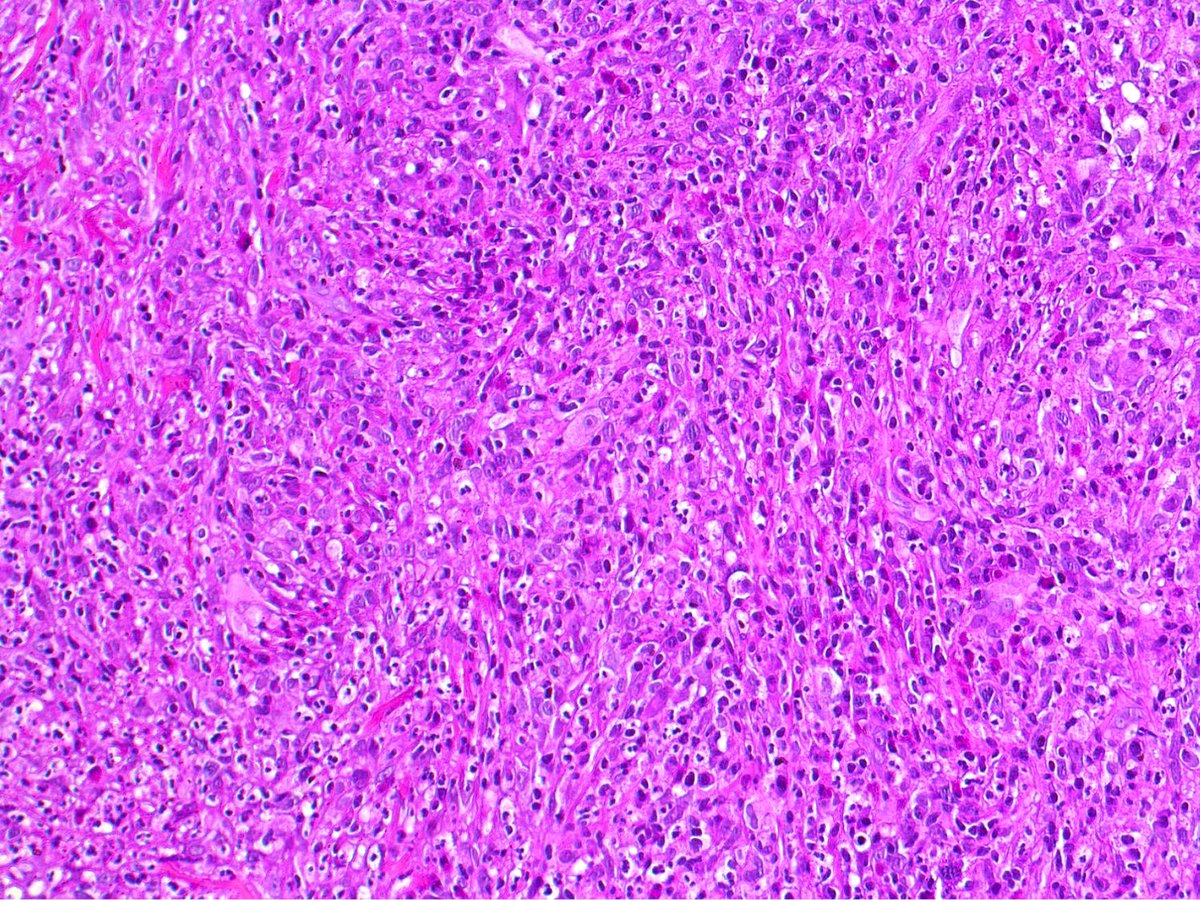
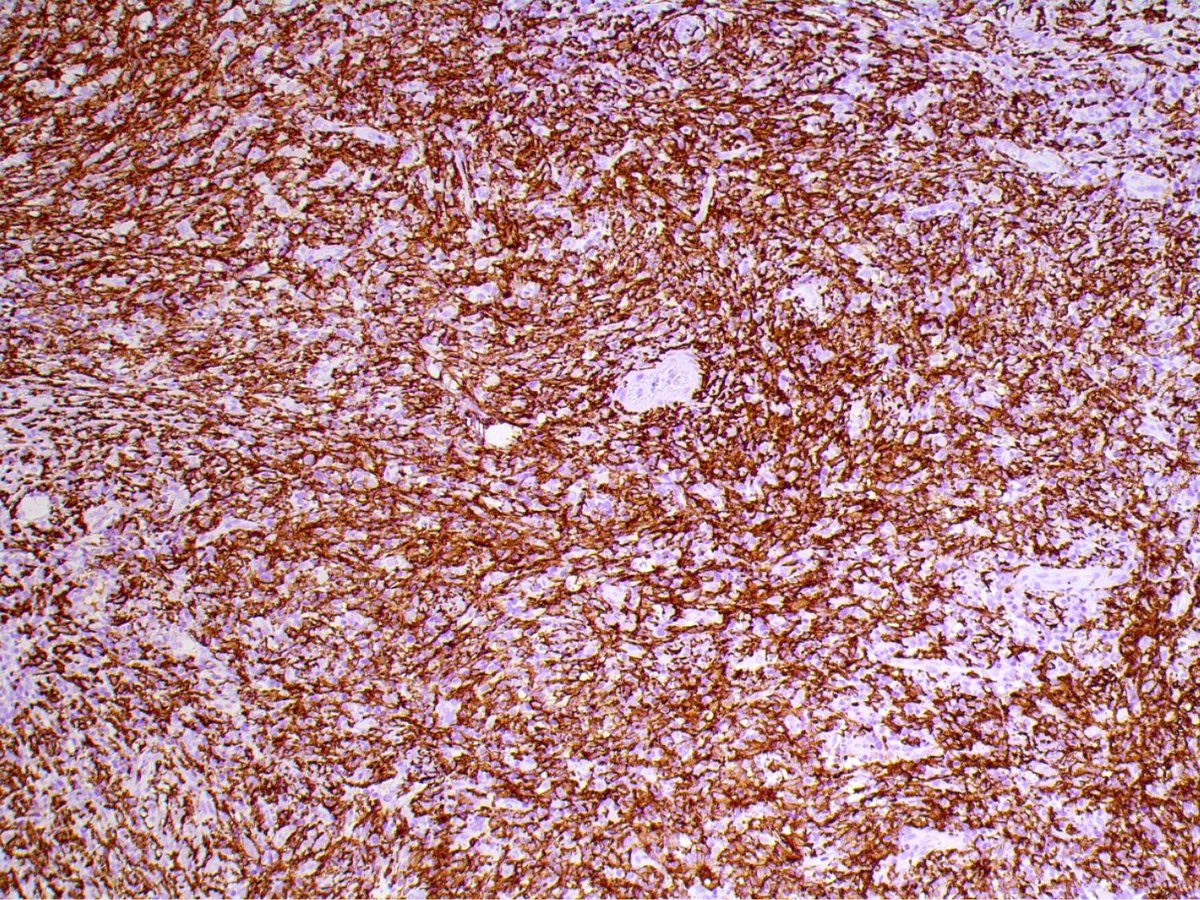
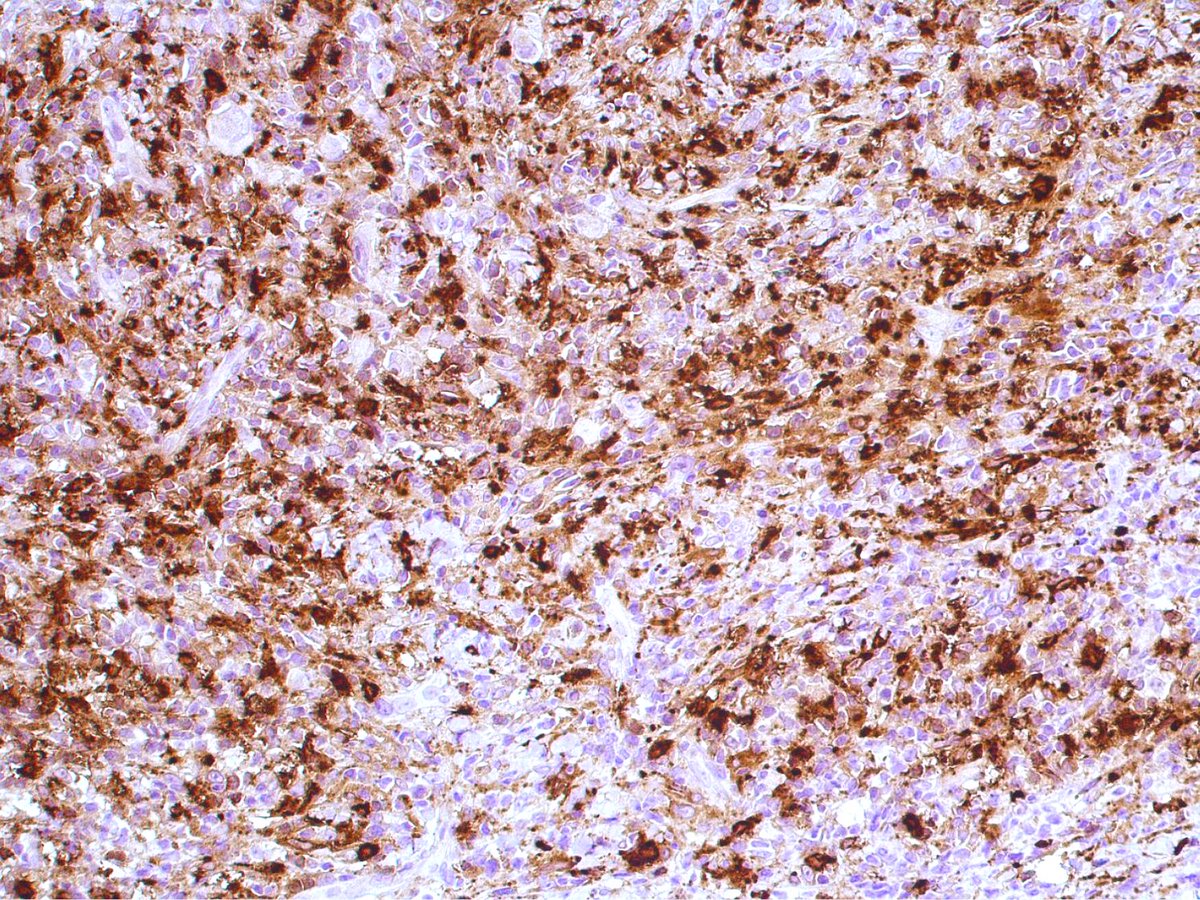
Histiocytic sarcoma affecting the oral cavity (CD163/Lysozyme)! Discover more in our @SpringerNature book Lymphoproliferative and granulomatous disorders of the oral cavity
link.springer.com/book/97830…
#Pathology #OralPathology #OralMedicine #lymphoma #PathTwitter #hemepath
1
2
7
378
Apr 13
Apr 10

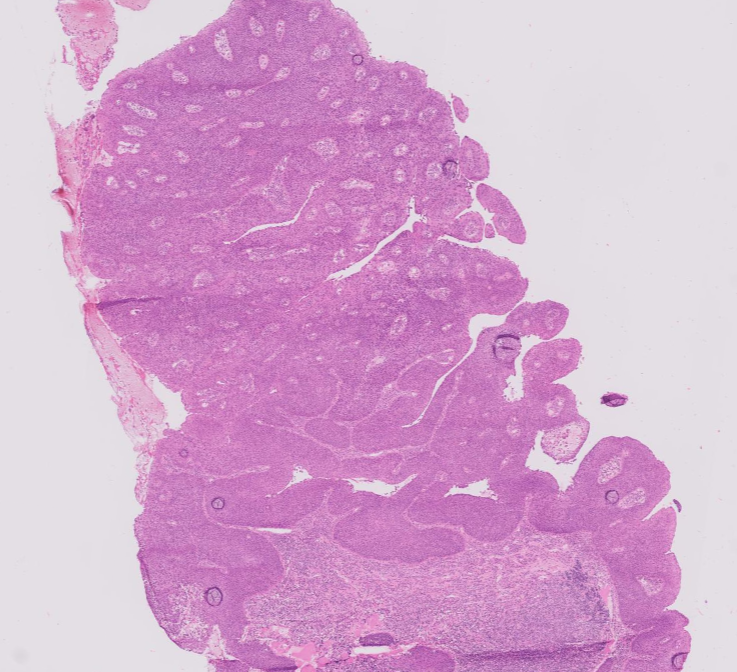
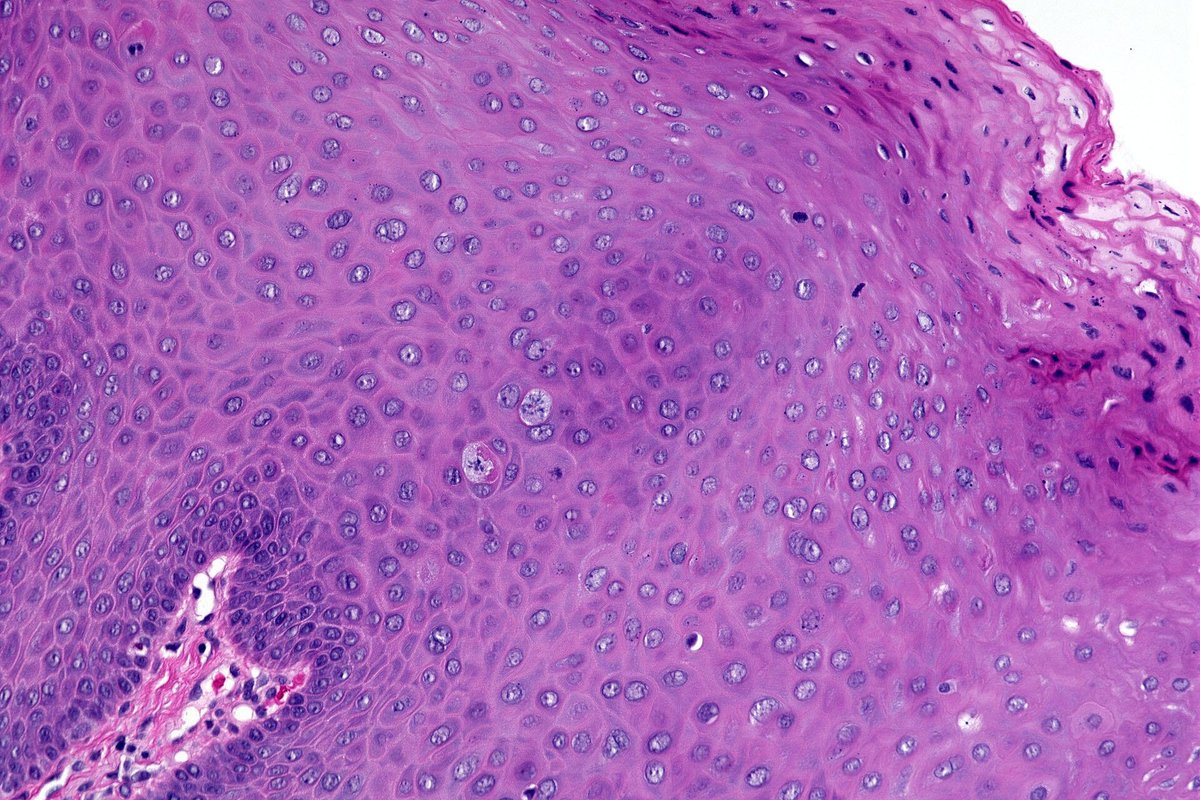
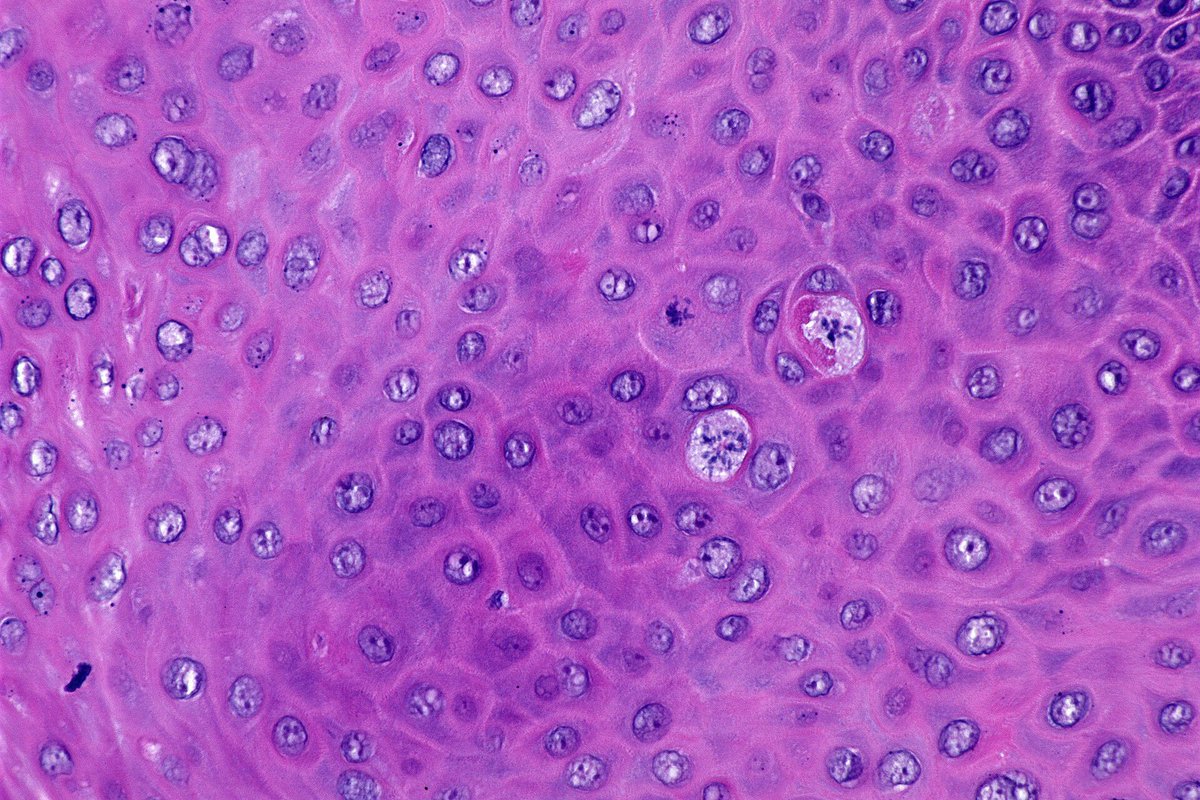
Oropharynx exophytic lesion: SCC?
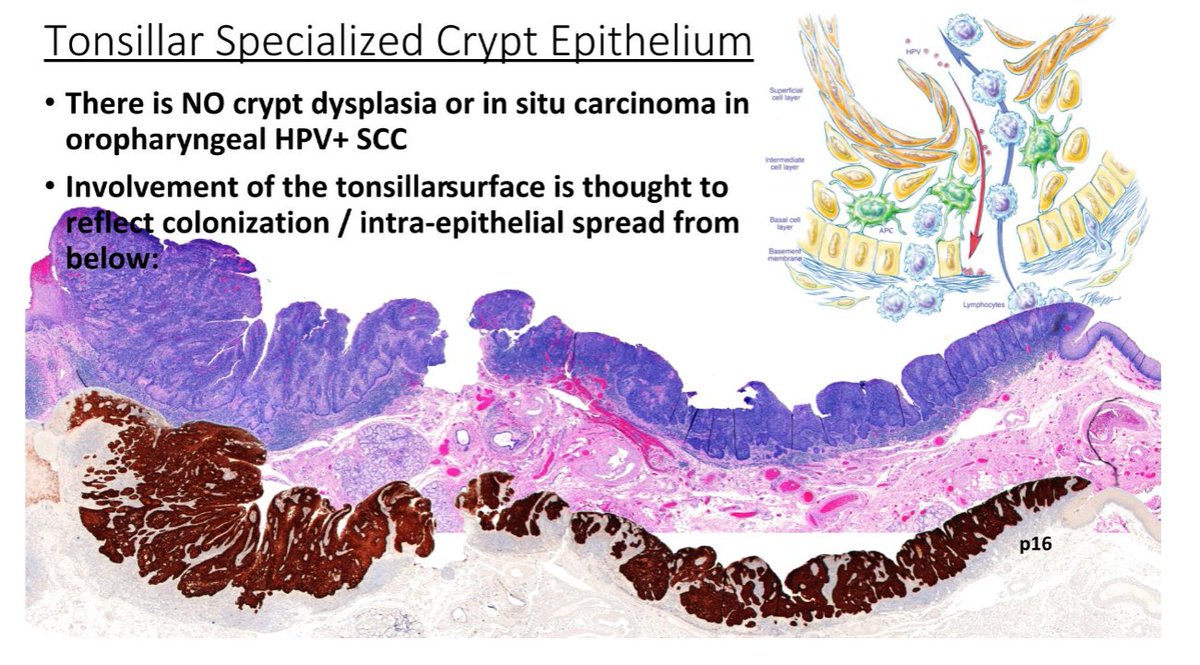
Tonsillar crypts are lined by a unique reticulated epithelium. The basement membrane is disrupted and non-contiguous, allowing the epithelium easy access to lymphatics.
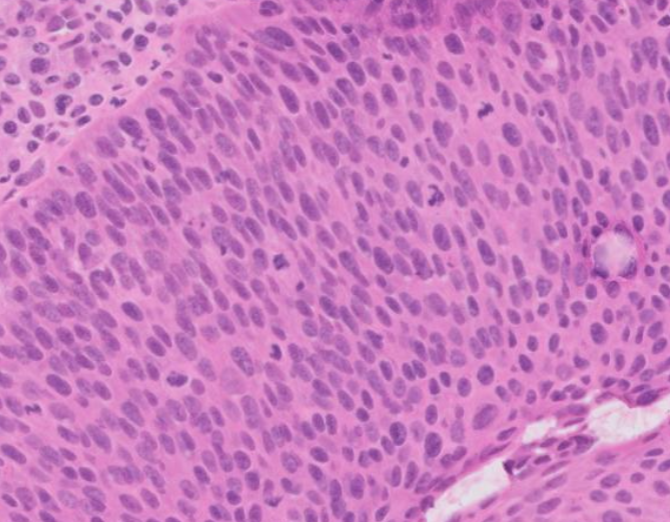
- There is no crypt dysplasia or in situ carcinoma in oropharyngeal HPV SCC.
- All HPV-related neoplasia of the tonsils should be regarded as malignant even in the absence of "classic" histologic features of invasion.
Dr. Cipriani #USCAP2026 #pathology #PathX #PathTwitter
1
8
721

Mar 25
Mar 24

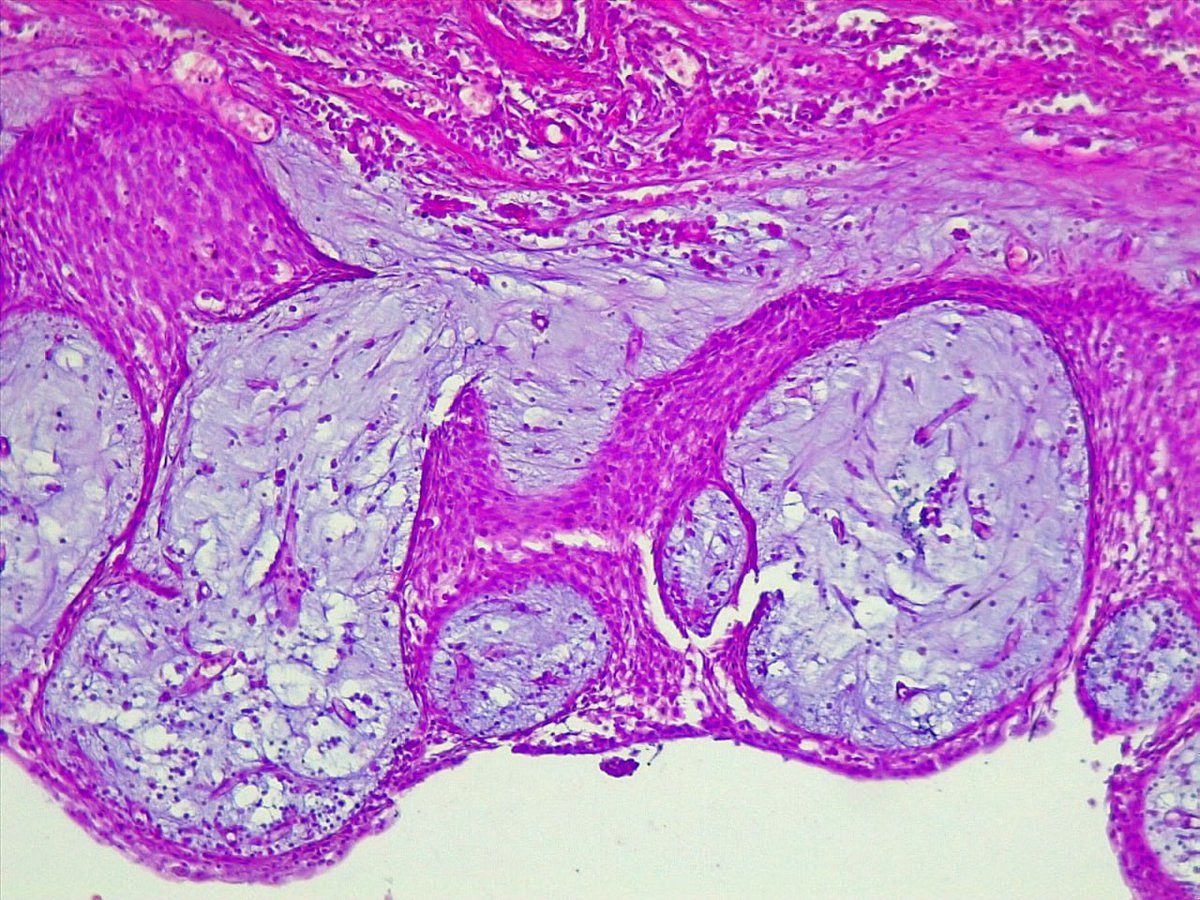
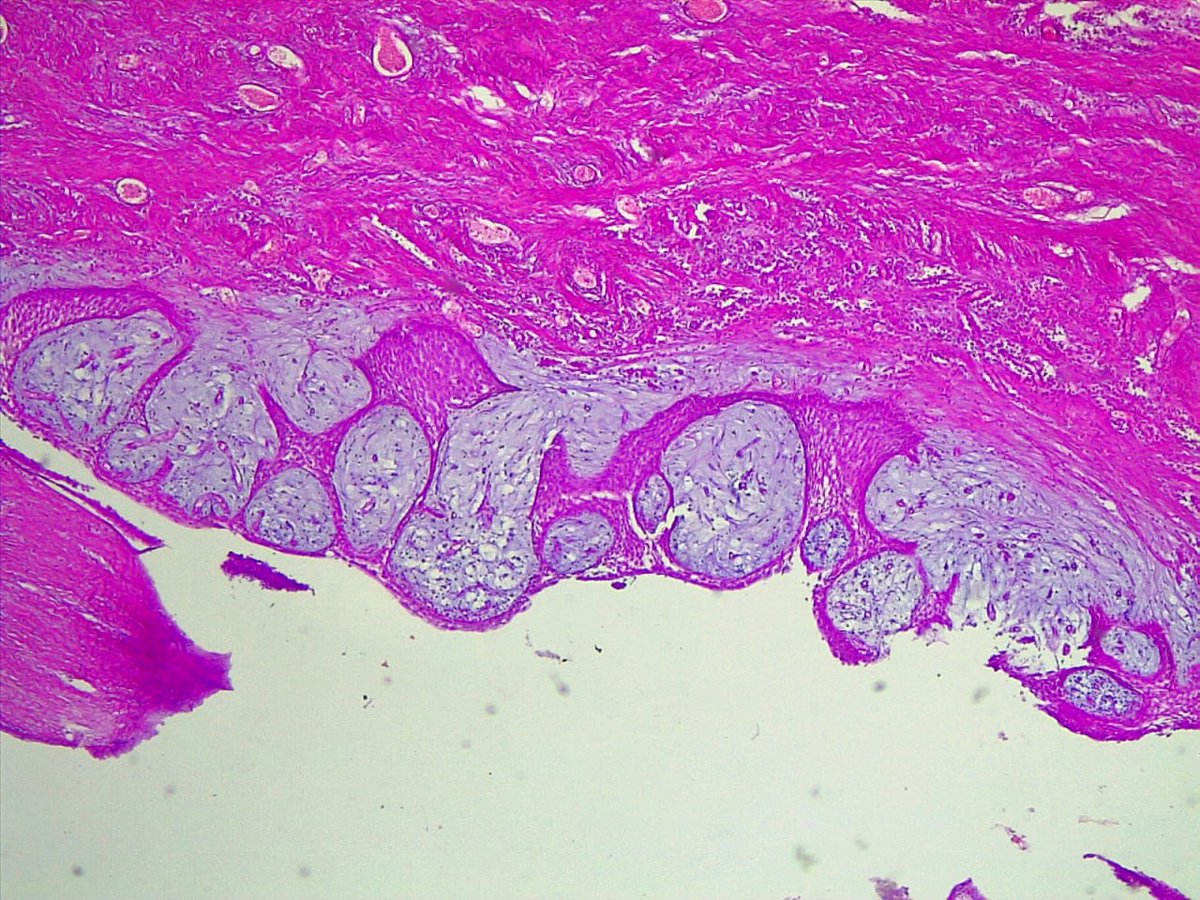
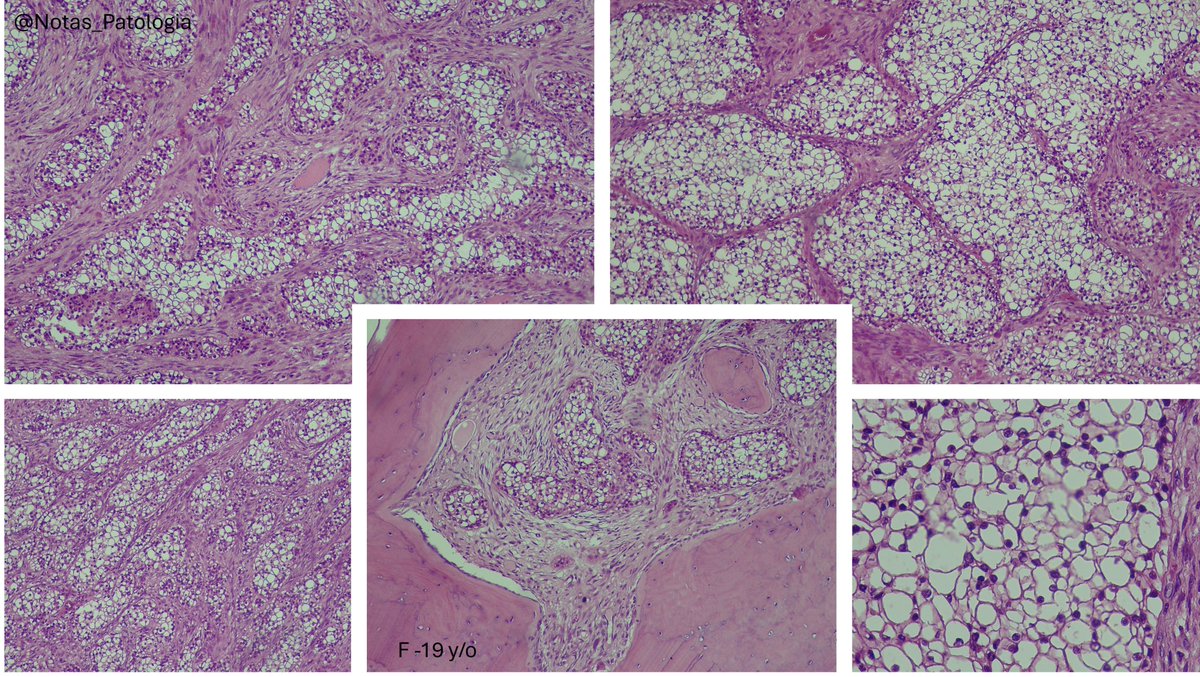
Photos from Biopticka multihead seminars of ectomesenchymal chondromyxoid tumor of the tongue
Benign tumor with predilection for the anterior dorsal tongue
Well demarcated , Stroma may be hyalinized , myxoid or chondromyxoid
sheets of oval, round, bland cells


3
304

Jan 27
30 Female with multiple oral papules. #oralpath #oralpathology #pathology #pathologists #pathTwitter #HeadNeckPathol #HeadandNeckPath #ENTPath #PathologyTweet
1
1
4
569
Jan 21

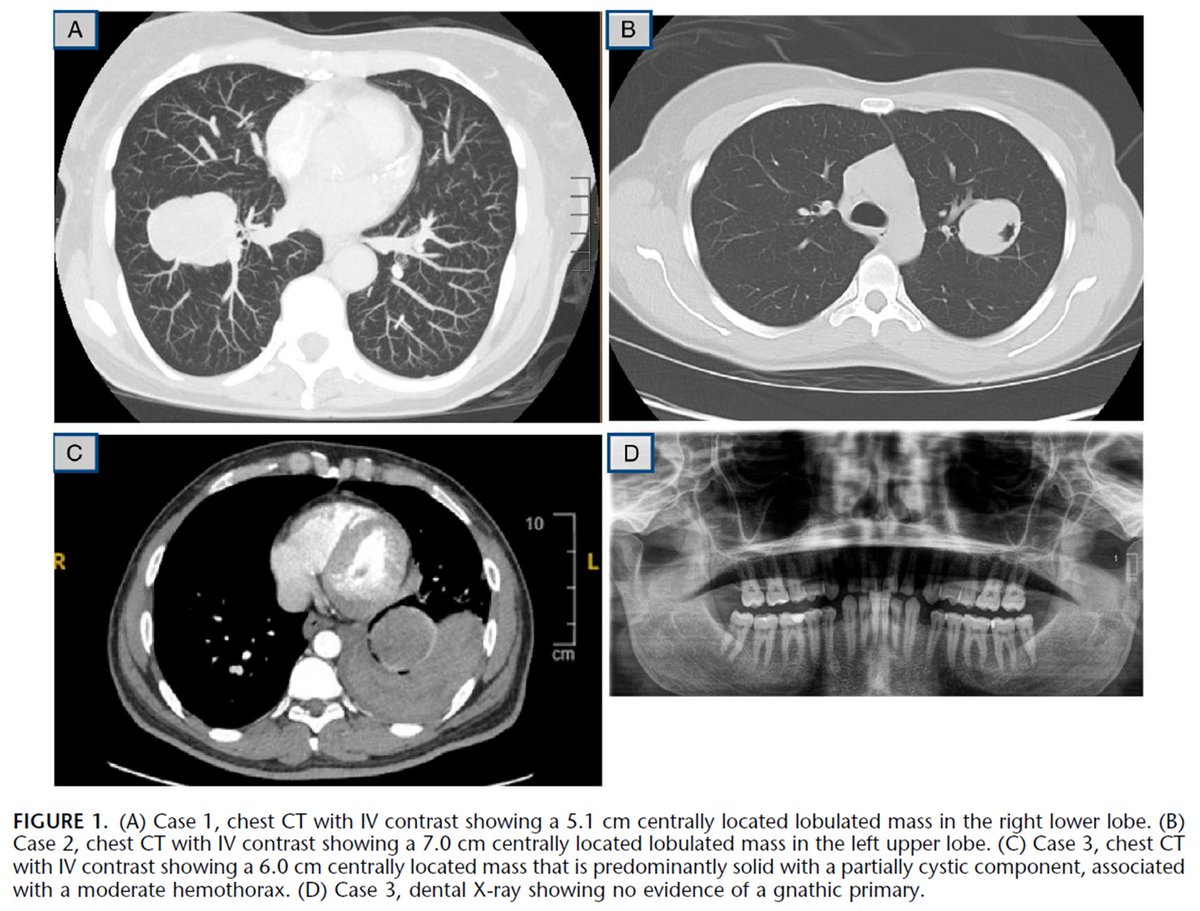
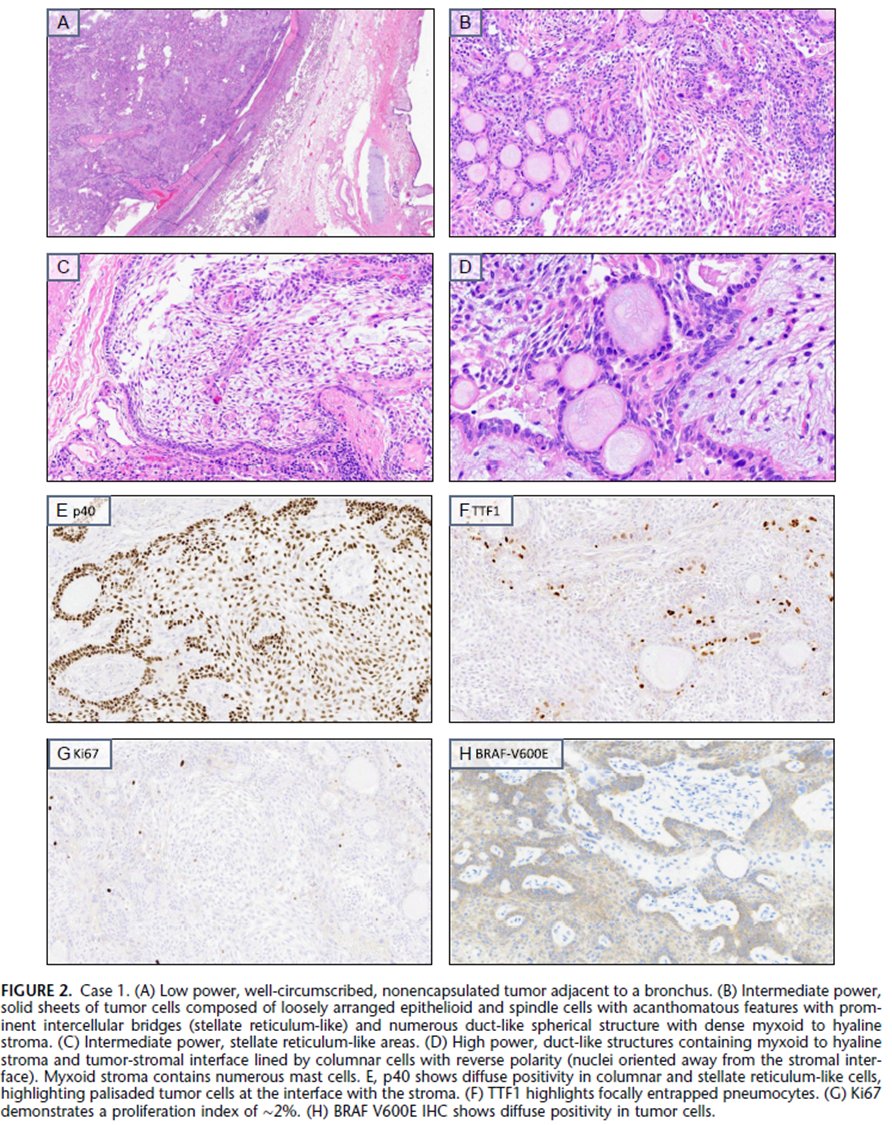
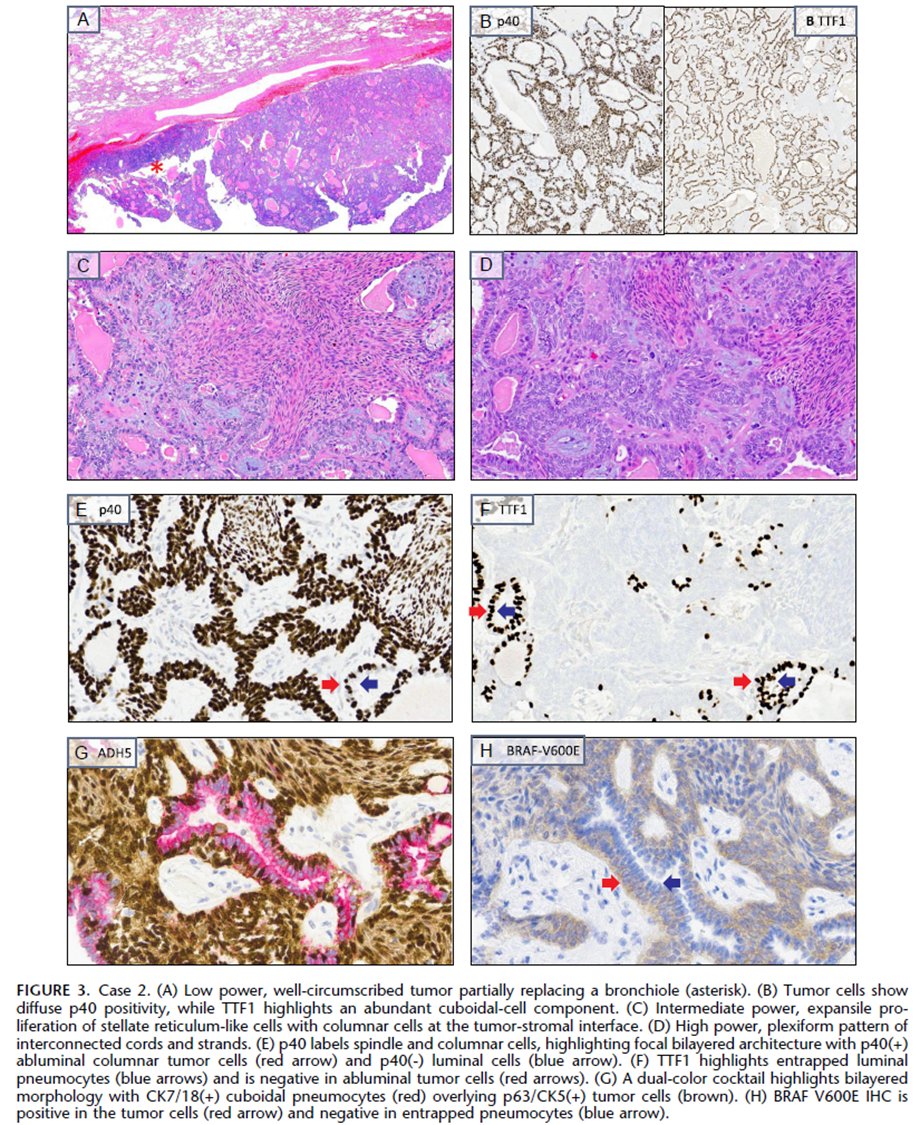
Just out in AJSP – a paper from our group describing a MAJOR new oddity.
Tumors that normally arise in the jaw from tooth🦷precursors (ameloblastoma) – but as lung primaries 🫁!
This was a neat collaboration b/w MSKCC, Mayo and UTSW where these cases were encountered independently, and we put our heads together with the help of original contributors and fellows to tackle this puzzle.
Time will tell if these are truly exceptional or have been underrecognized.
journals.lww.com/ajsp/fullte…
@JLHornick @ENTpathology @MSKPathology @PulmPathSoc @yro854 @thoracicpath @Path_Matt @SansanoValero @AndreMo77438628
4
375

Jan 10
Peripheral ossifying fibroma
Reactive gingival proliferation showing spindle cell proliferation and ossification
#path #pathology #medicine #oralpath
1
11
45
1,618
8 Dec 2025
50 Male with palatal lesion #oralpath #oralpathology #pathology #pathologists #pathTwitter #HeadNeckPathol #HeadandNeckPath #ENTPath #PathologyTweet #dermpath



4
6
21
1,730
21 Nov 2025
21 Nov 2025

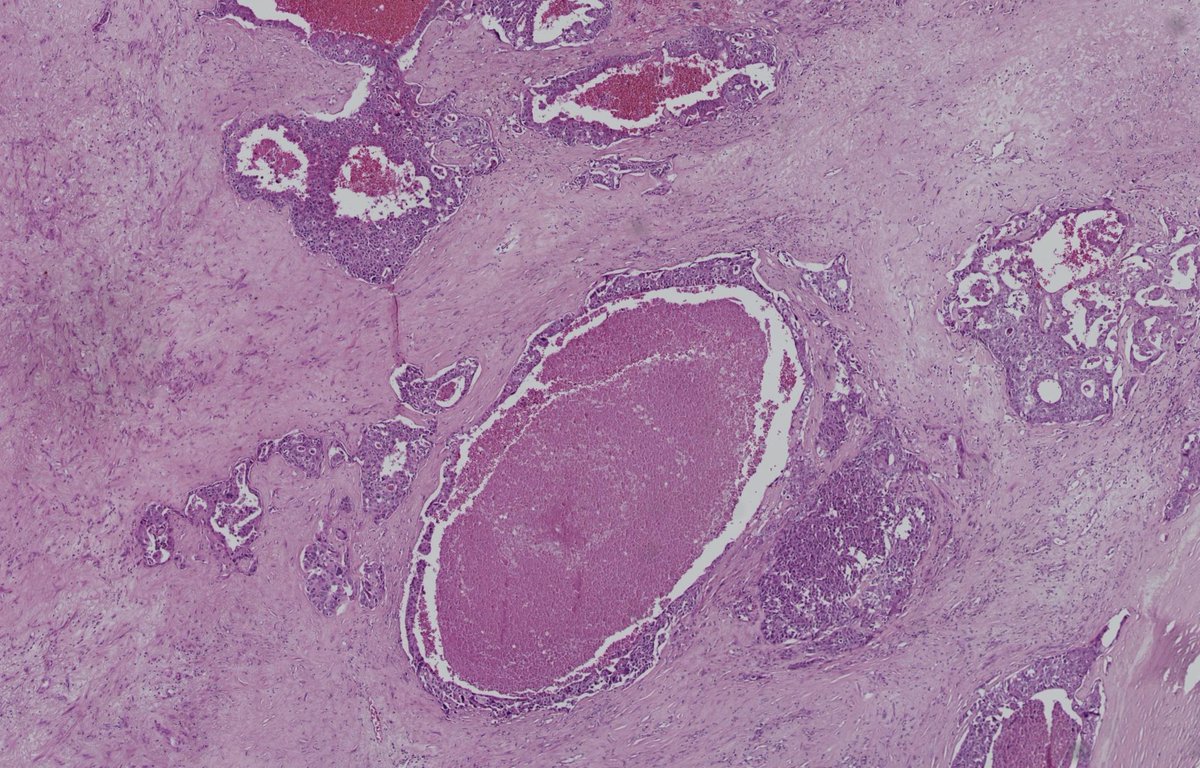
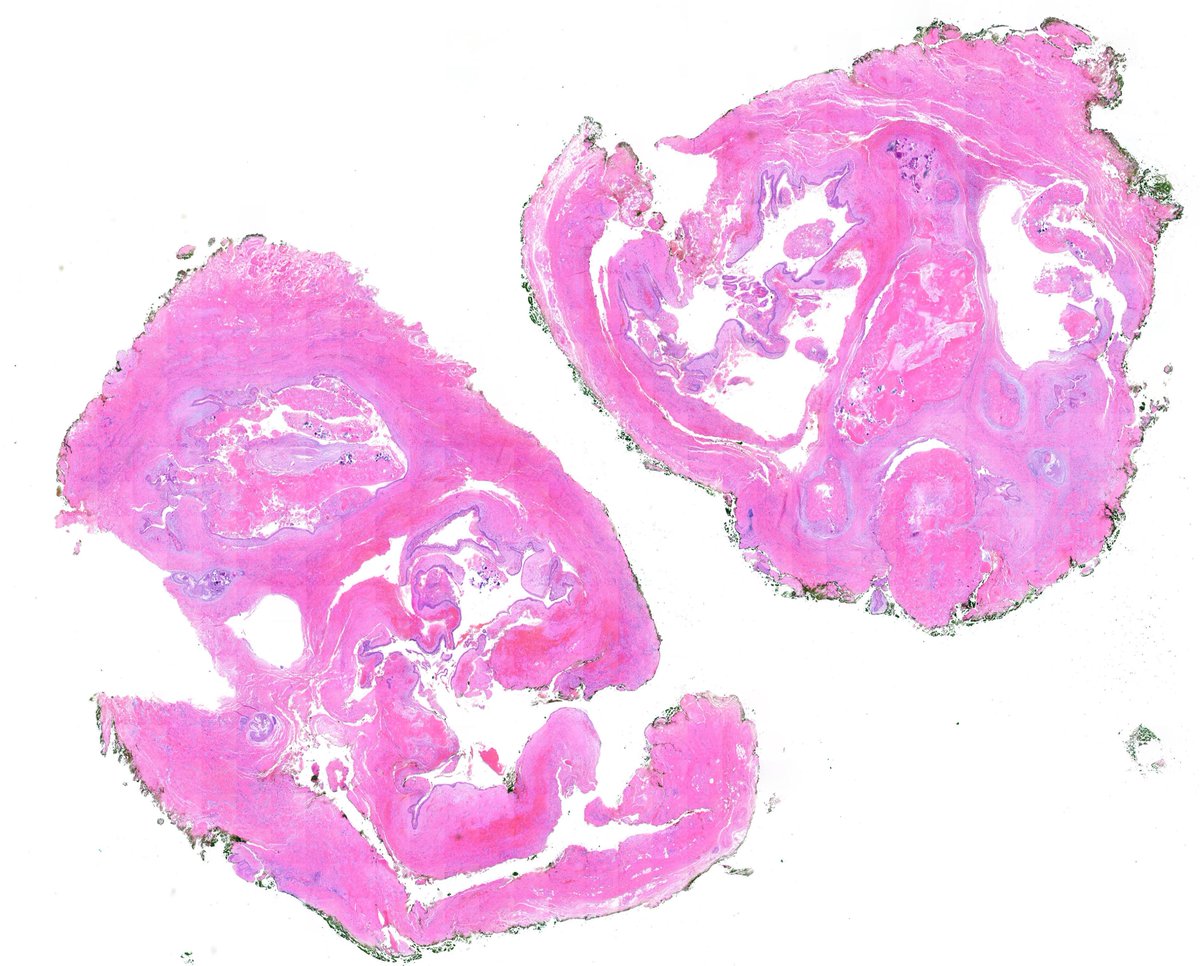
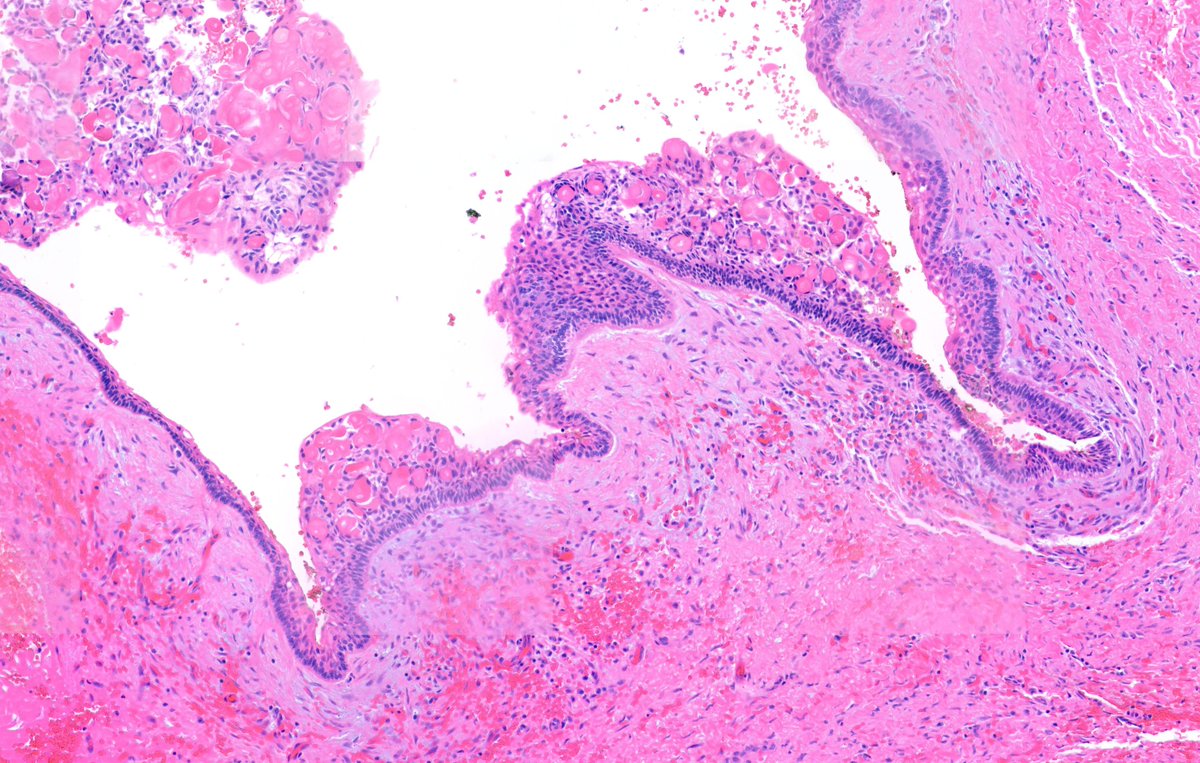
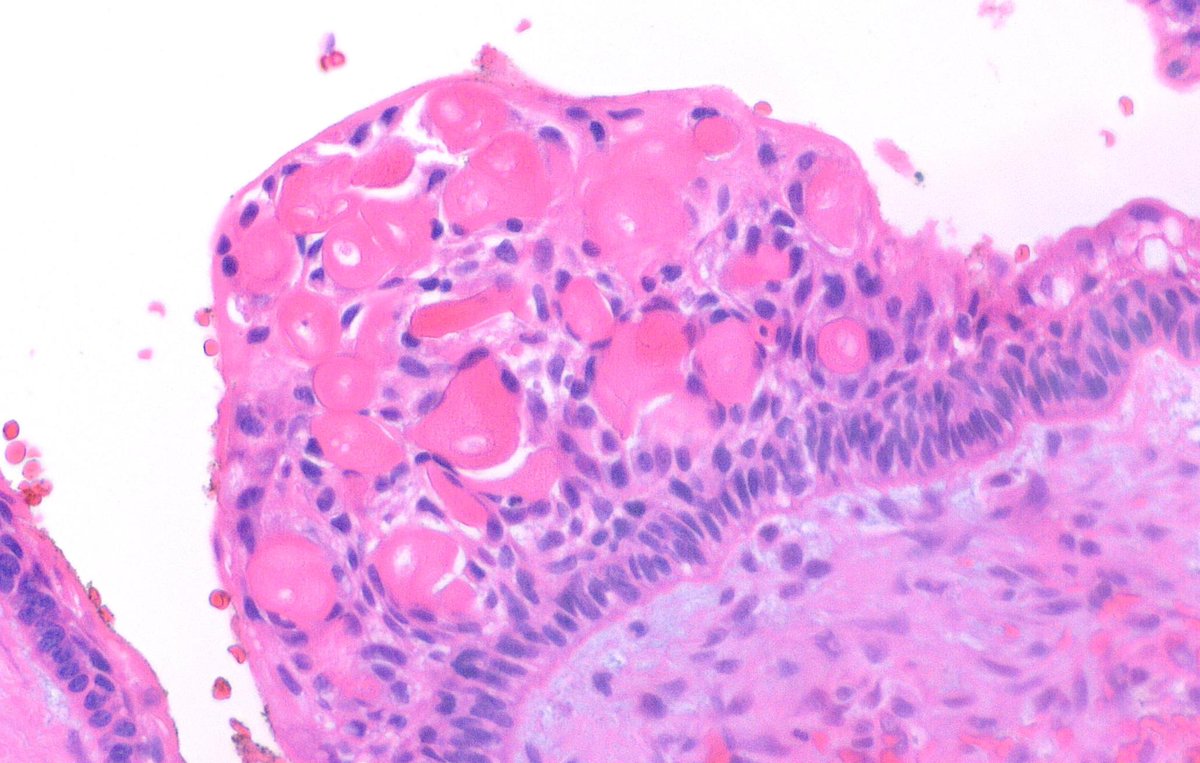
The structures you’re seeing are aberrant products of odontogenesis, I see it often in the wall of many developmental odontogenic cysts or dental follicles, there are not specific.
Also, the respiratory lining can be seen in many odontogenic cysts especially if they are in close proximity to the maxillary sinus. My guess is Dentigerous cyst, but I have to correlate radiographically
3
428
29 Sep 2025
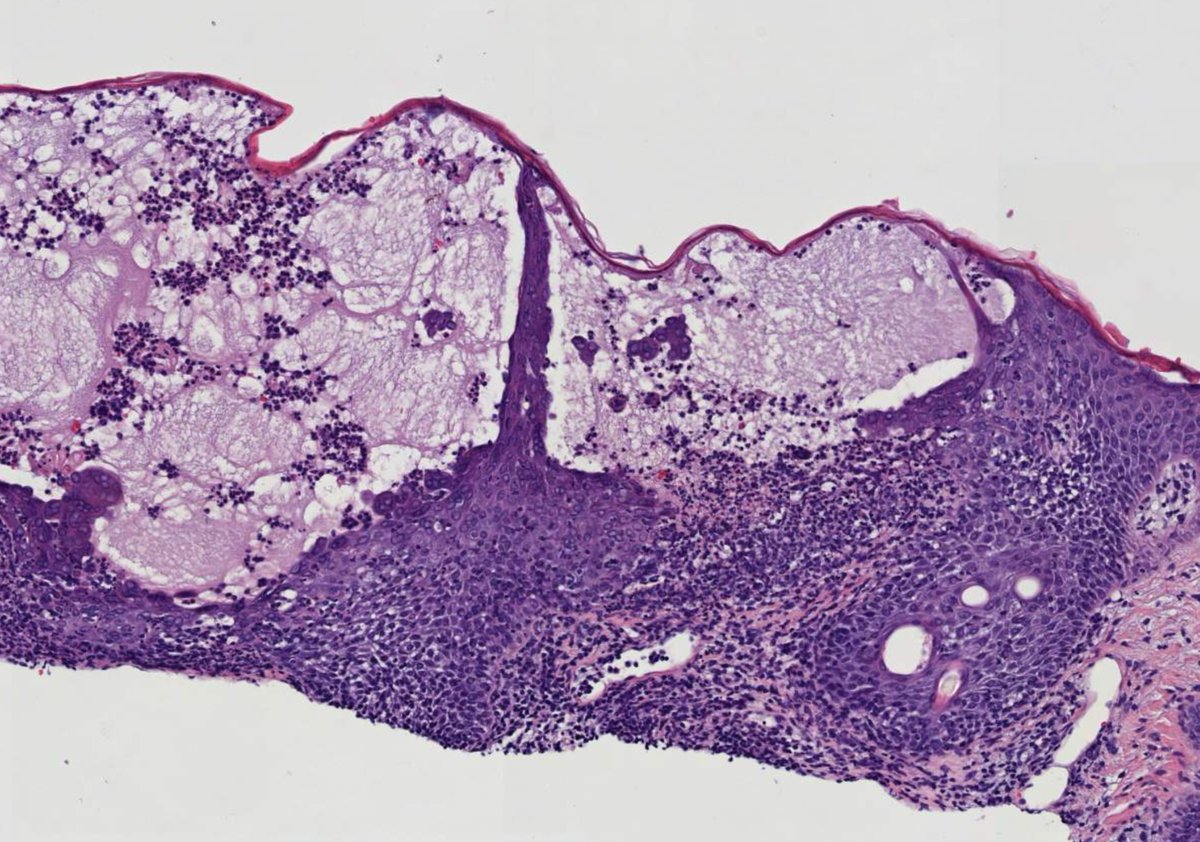
Middle-aged male with unilateral friable nasal polyp. #oralpath #oralpathology #pathology #pathologists #pathTwitter #HeadNeckPathol #HeadandNeckPath #ENTPath #PathologyTweet #dermpath
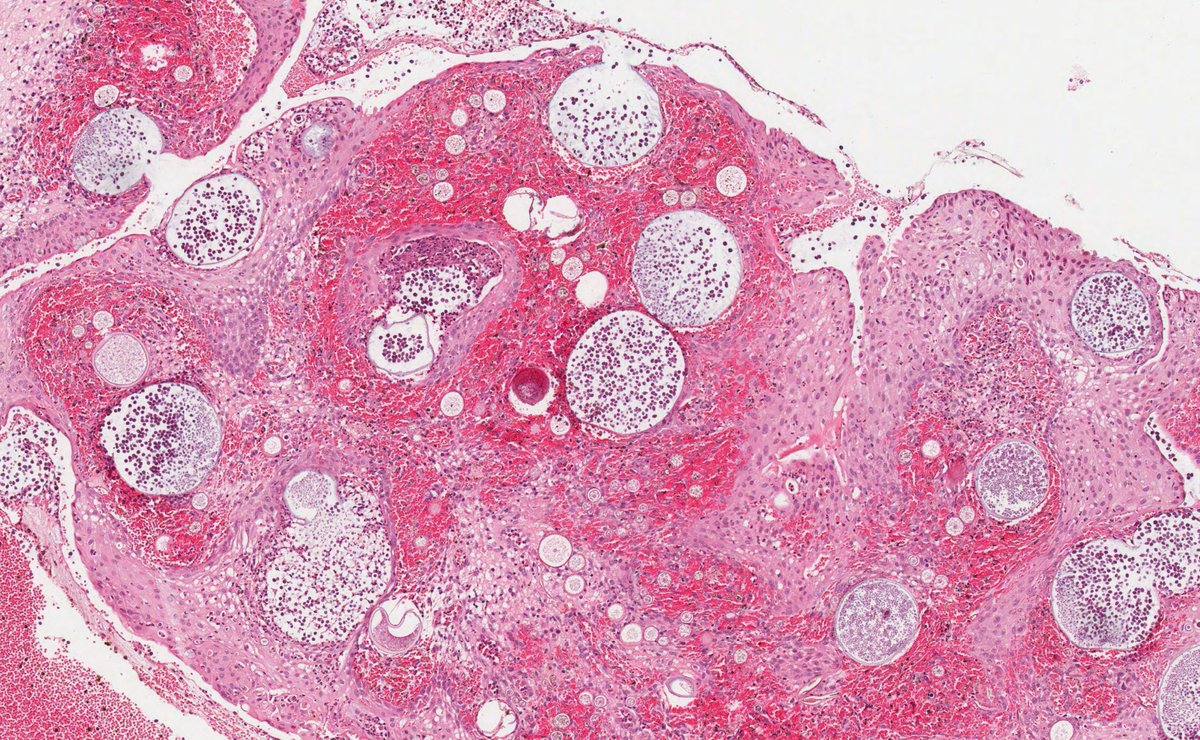
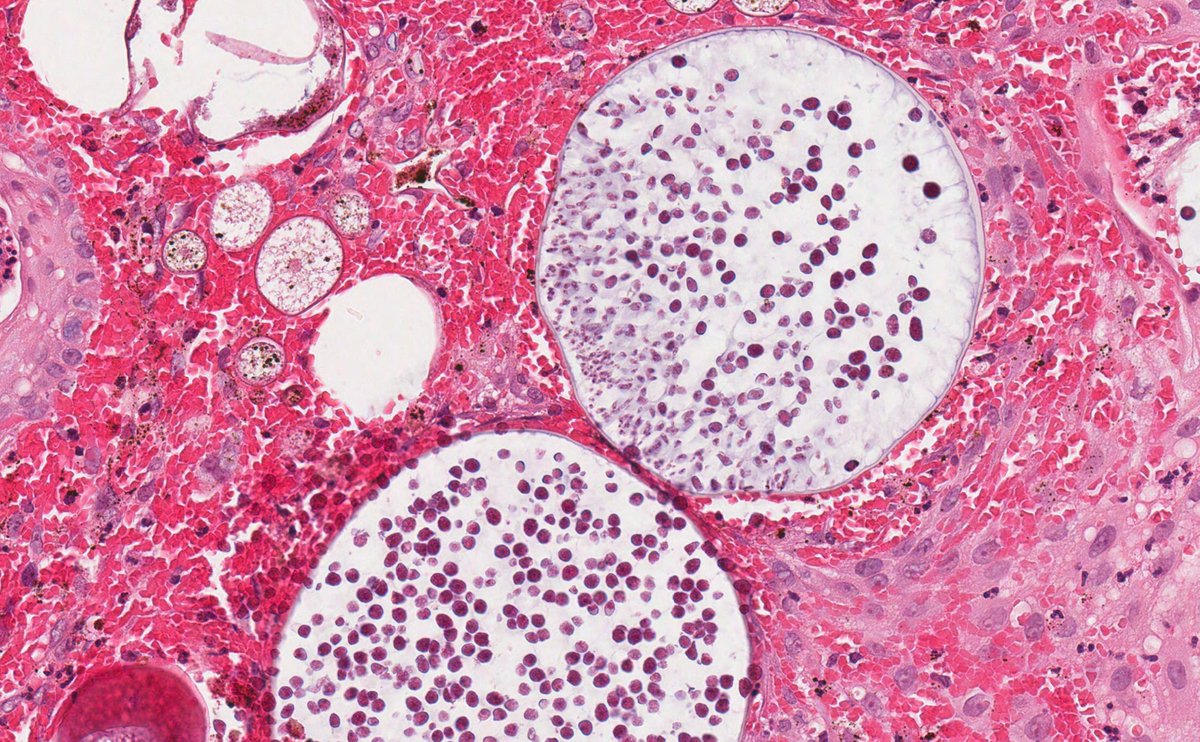
3
7
40
4,428
6 Sep 2025
A 59-year-old female with a lip lesion #oralpath #oralpathology #pathology #pathologists #pathTwitter #HeadNeckPathol #HeadandNeckPath #ENTPath #PathologyTweet #dermpath


7
16
60
5,930
31 Aug 2025
A 60-year-old male with a mass at the floor of the mouth #oralpath #oralpathology #pathology #pathologists #pathTwitter #HeadNeckPathol #HeadandNeckPath #ENTPath #PathologyTweet #dermpath

5
15
54
3,433
30 Aug 2025
29 Aug 2025

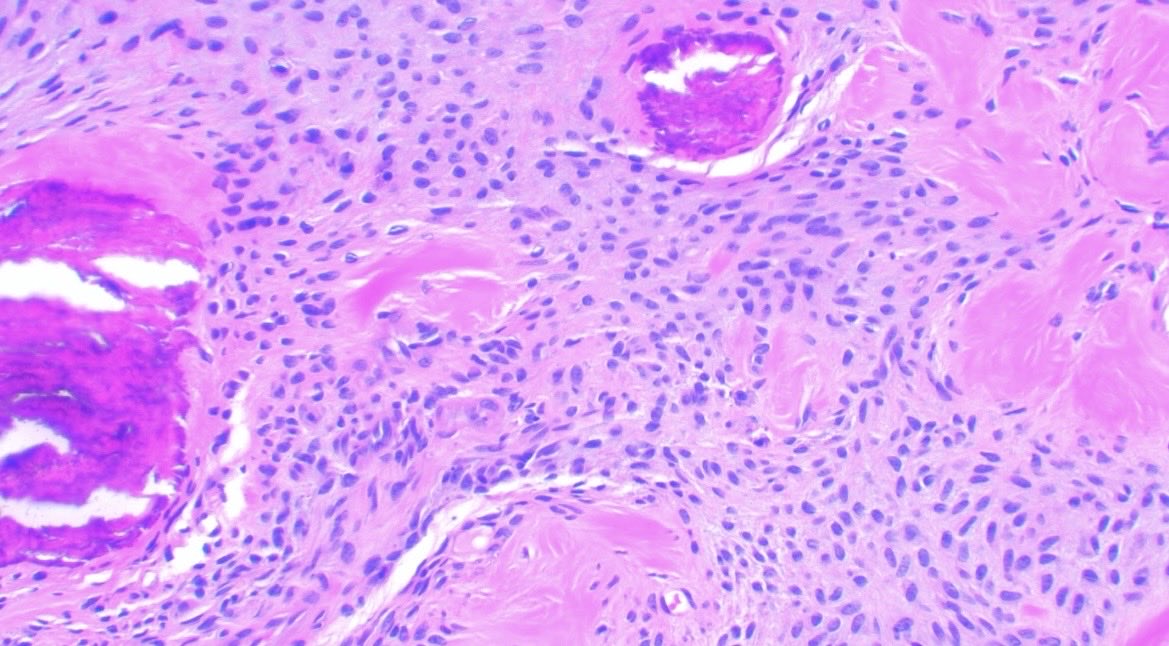
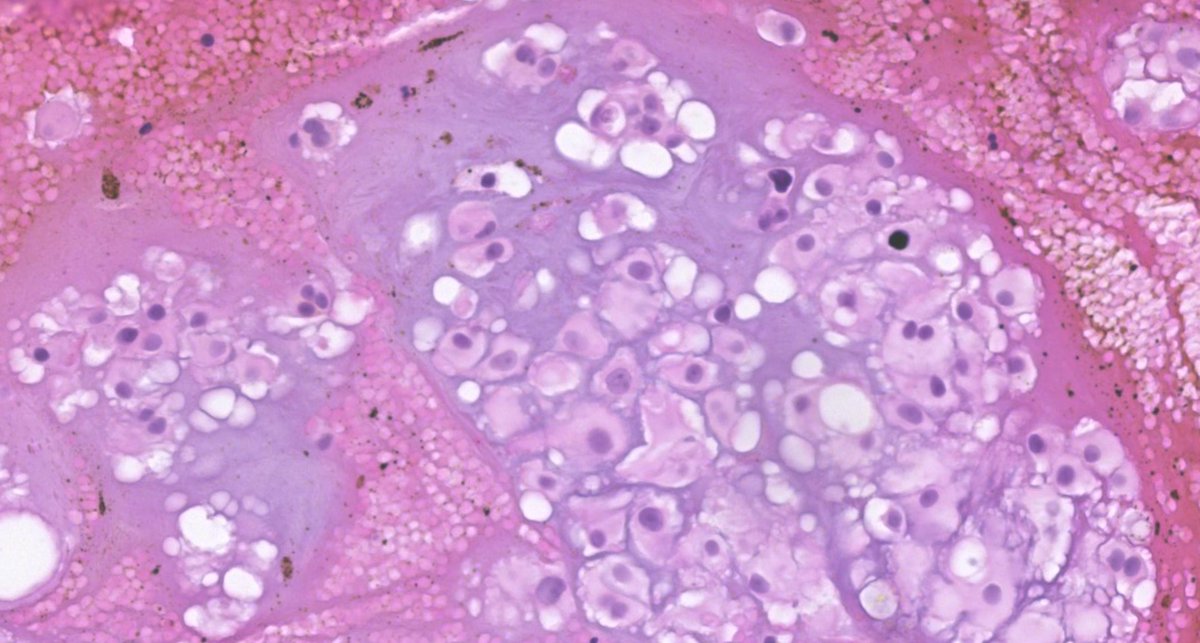
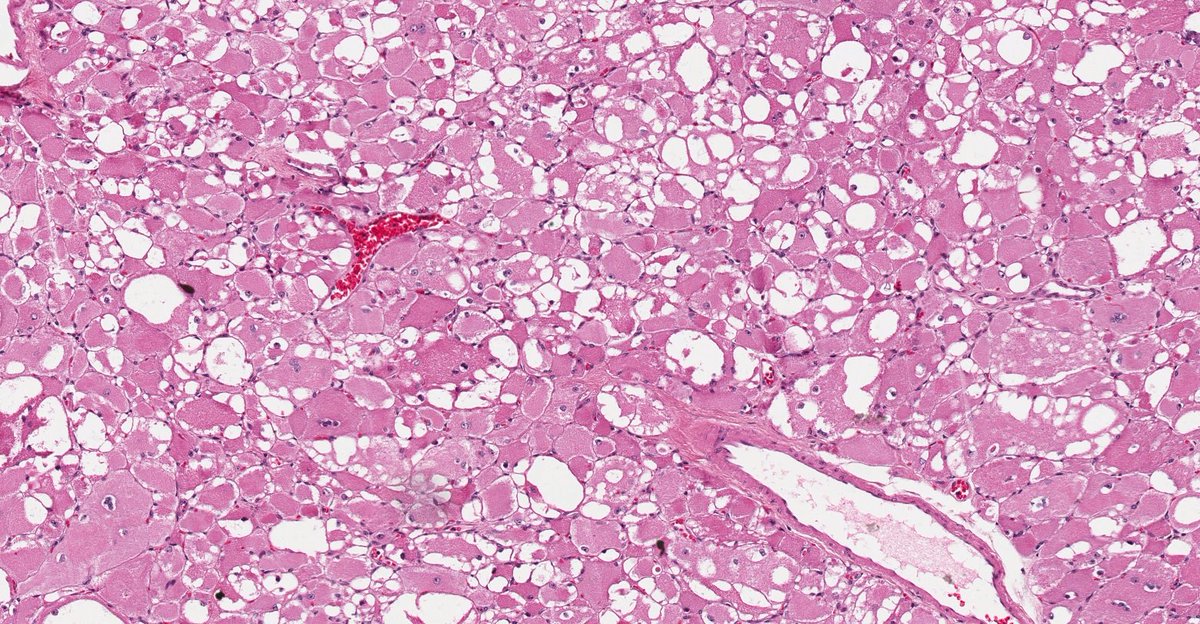
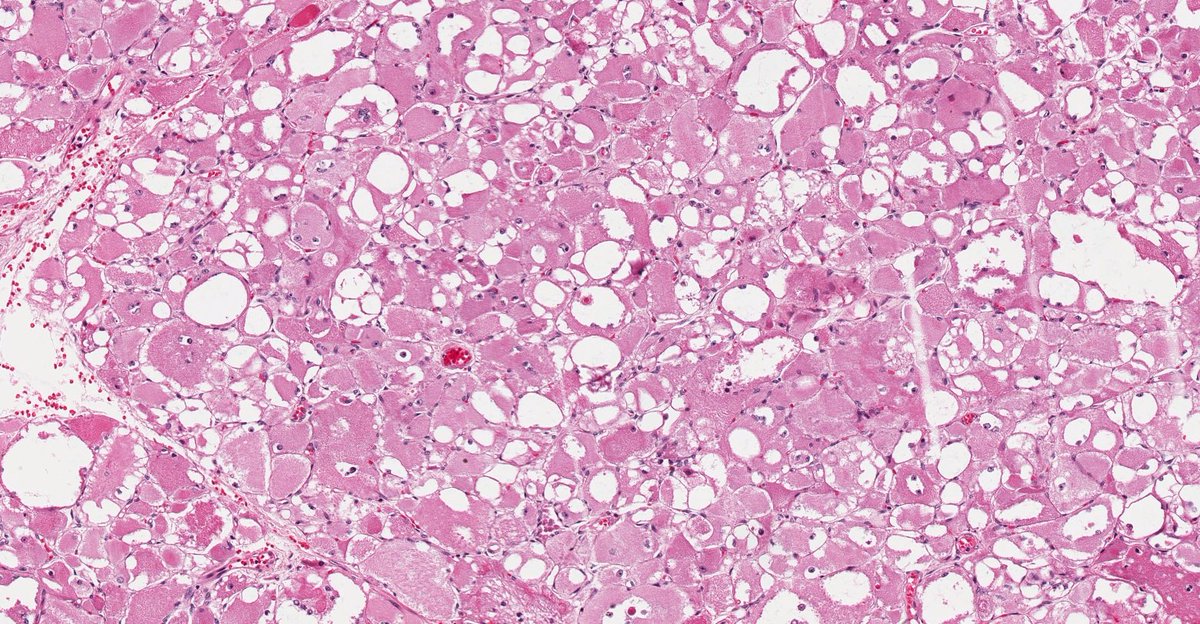
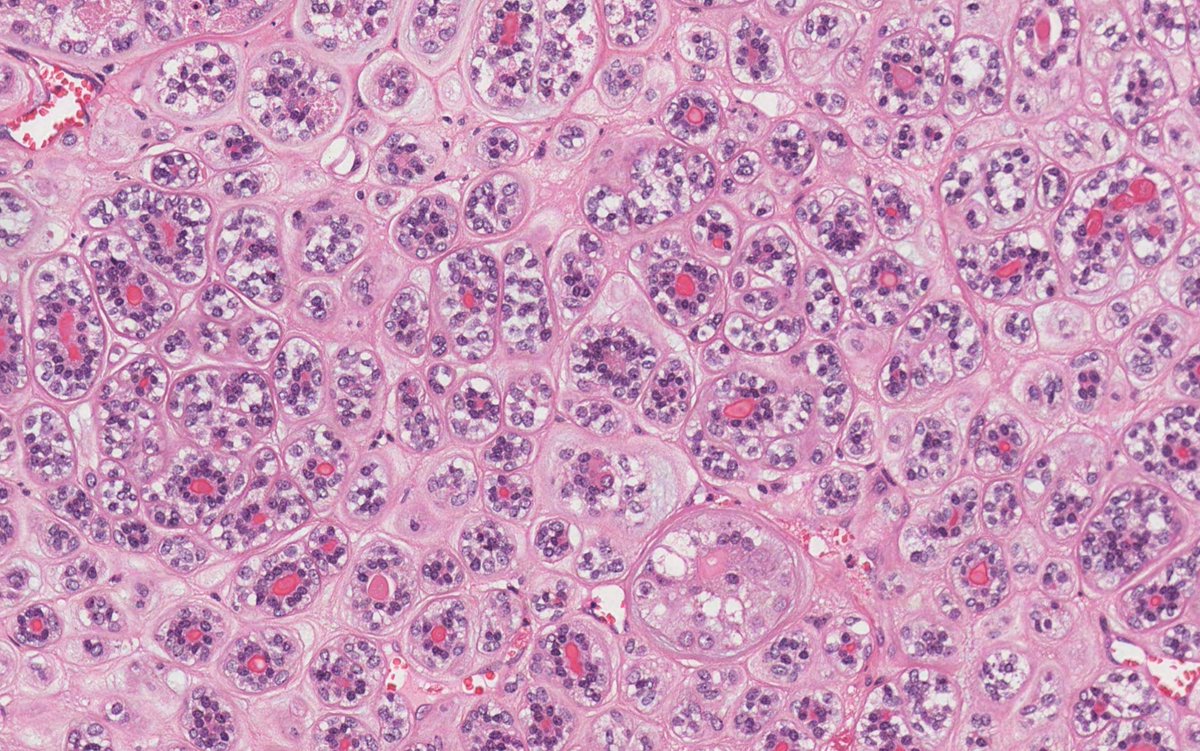
🦷 Granular Cell Ameloblastoma (GCA)
📖 Definition
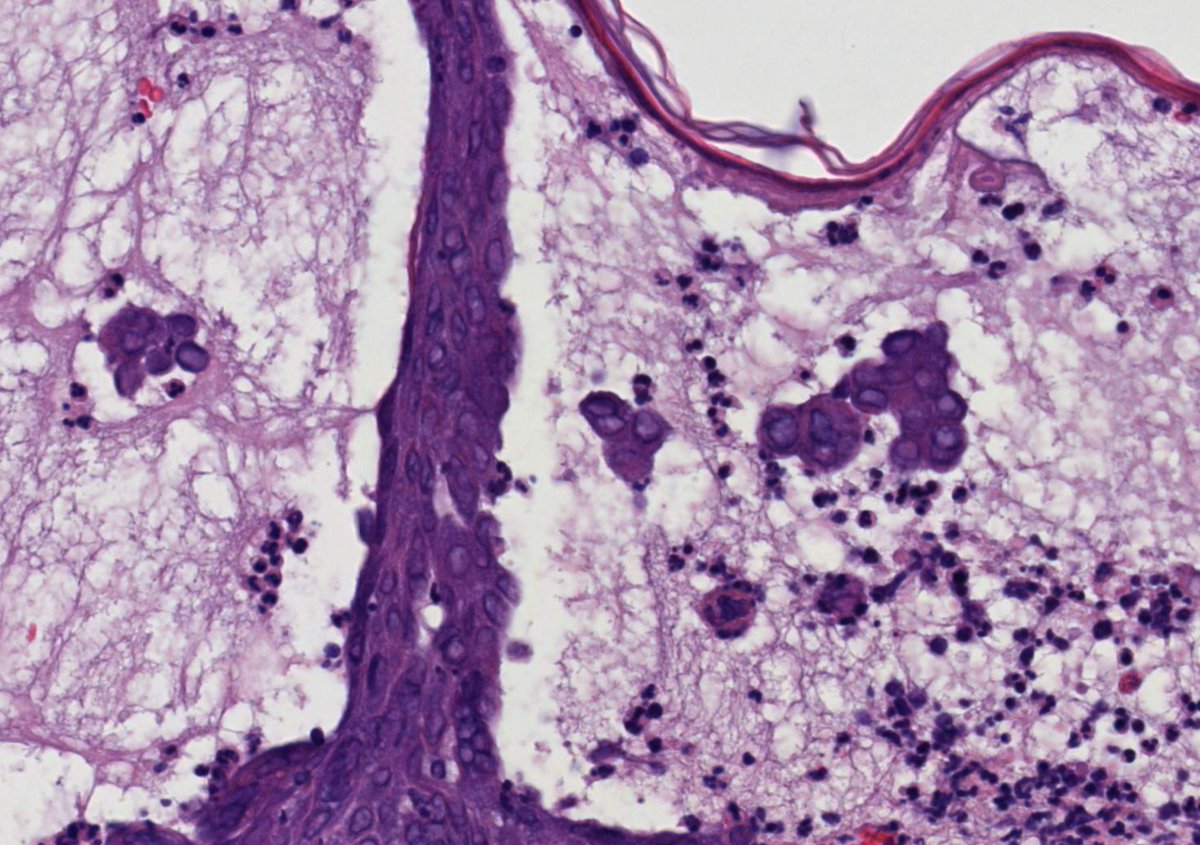
Granular Cell Ameloblastoma (GCA) is a rare histological variant of conventional ameloblastoma, a benign but locally aggressive odontogenic epithelial tumor, characterized by peripheral ameloblast-like cells and a central stellate-reticulum–like component.
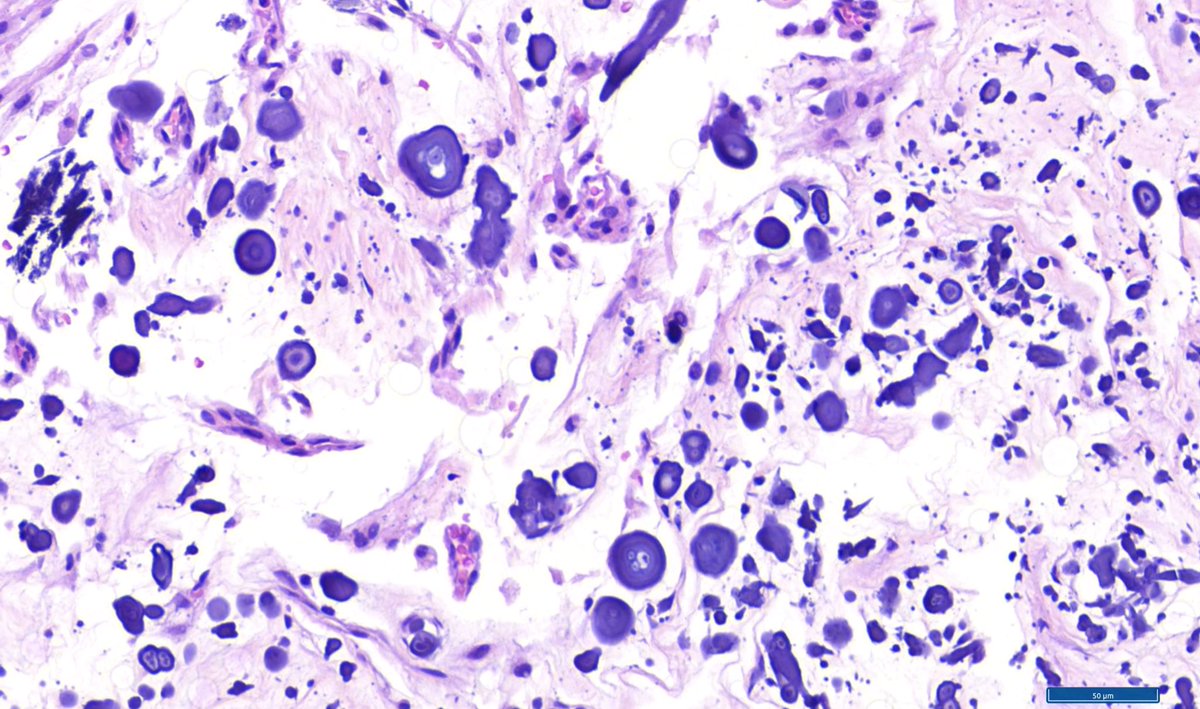
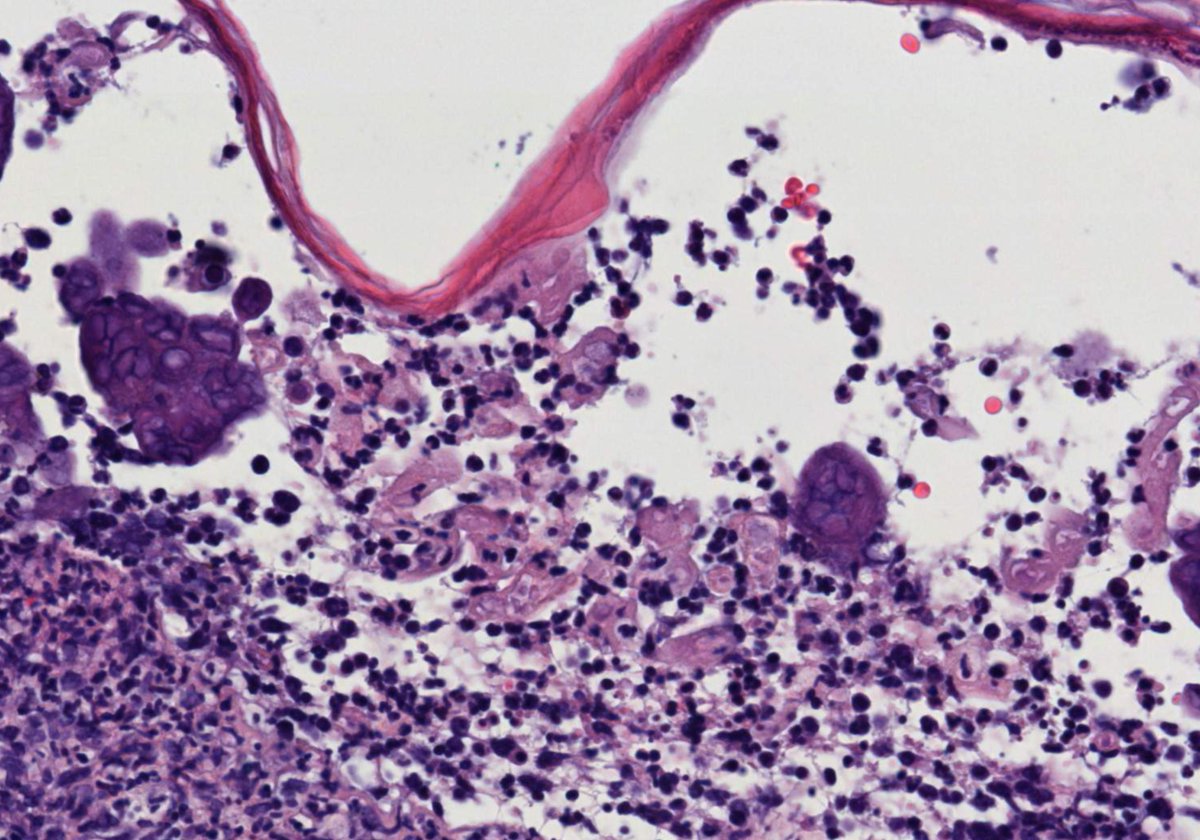
In the granular variant, the central cells acquire abundant eosinophilic granular cytoplasm, due to the accumulation of lysosomes【WHO 2022】.
📊 Epidemiology
Ameloblastoma accounts for about 1% of all head and neck neoplasms.
The granular cell subtype represents approximately 3–5% of cases【PathologyOutlines】.
Most common in the mandible (87%), especially the posterior region.
Age range: adults in the 3rd to 5th decade, though it may occur across a broad age spectrum.
No significant sex predilection.
🧬 Etiology / Pathophysiology
Exact etiology remains unknown.
Molecular pathogenesis:
Alterations in the MAPK/ERK pathway are the most common.
BRAF p.V600E mutation is the most frequent, especially in mandibular tumors.
Less common mutations: RAS and FGFR2.
In the granular subtype, cytoplasmic granularity results from lysosomal accumulation in central cells, interpreted as a degenerative/metabolic process rather than an independent prognostic marker.
🤒 Clinical Manifestations
Slow-growing, painless swelling in the mandible or maxilla.
May cause:
Cortical bone expansion and perforation.
Tooth mobility or loss.
Local paresthesia in larger tumors.
If untreated, it may become large, leading to facial deformity and involvement of adjacent structures.
🧪 Laboratory Diagnosis
No specific serum biomarkers.
Histopathological evaluation is mandatory for diagnosis.
Molecular testing (e.g., BRAF status) may aid in prognostic stratification and targeted therapy selection.
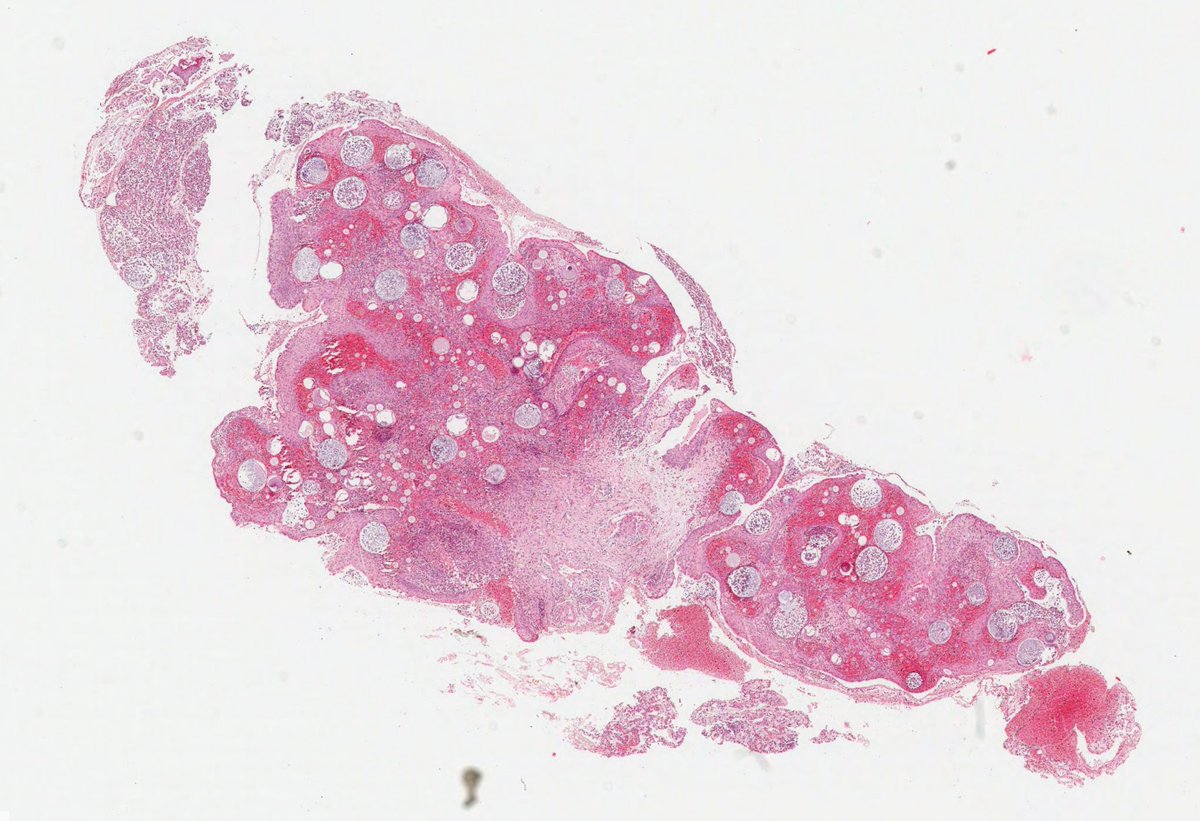
🖼️ Imaging and Pathology Findings
Radiology
Multilocular radiolucency with “soap bubble” or “honeycomb” appearance, well-corticated margins.
CT (preferably contrast-enhanced): better defines size, content, cortical expansion, and perforation.
Associated with impacted teeth in up to 18% of cases.
Histopathology
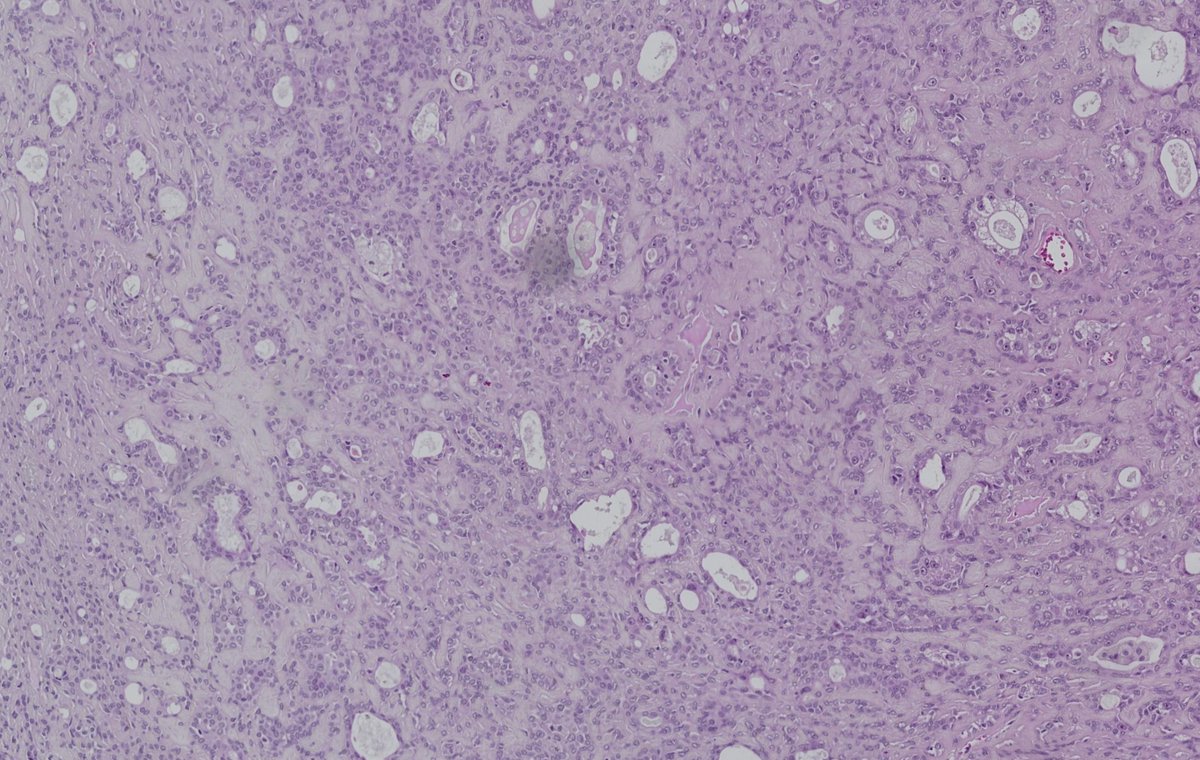
Epithelial islands in fibrous stroma.
Peripheral cells: columnar/cuboidal, hyperchromatic nuclei, reverse polarity, subnuclear vacuolization.
Central cells: stellate-reticulum–like, but with abundant eosinophilic granular cytoplasm filled with lysosomes.
No significant atypia or mitotic activity.
May coexist with other histological patterns (follicular, plexiform, etc.).
🔍 Differential Diagnosis
Granular cell tumor (Abrikossoff’s tumor): soft tissue lesion, S100 , lacks ameloblastomatous architecture.
Oncocytic odontogenic tumor: granular cytoplasm, different growth pattern.
Other ameloblastoma subtypes (acanthomatous, follicular, plexiform, etc.).
Odontogenic carcinoma (rare, in atypical or aggressive cases).
📉 Prognosis / Complications
Locally aggressive behavior, similar to conventional ameloblastoma.
Recurrence risk is high with conservative treatment (simple curettage → up to 60–80%).
No evidence that the granular morphology alone alters prognosis compared with other variants.
Potential for significant local destruction and functional impairment.
Malignant transformation (malignant ameloblastoma / ameloblastic carcinoma) is exceedingly rare.
💊 Treatment
Radical surgical resection with negative margins (>1 cm beyond radiographic limits).
Options: segmental mandibulectomy or maxillectomy, depending on size and location.
Conservative approaches carry high recurrence rates.
Long-term follow-up (10–20 years) is essential due to late recurrences.
Emerging therapies: BRAF inhibitors (± MEK inhibitors) in unresectable or metastatic cases, with early promising results.
📝 Summary
Granular Cell Ameloblastoma (GCA) is a rare variant of ameloblastoma, histologically defined by eosinophilic granular cytoplasm in central tumor cells. Despite its peculiar morphology, its biological behavior is comparable to conventional ameloblastoma: benign but infiltrative, slow-growing, locally destructive, and prone to recurrence after conservative surgery. Management requires radical resection with long-term surveillance.
#️⃣ #MedicalEducation #NotasDePatologia
⚠️ Disclaimer: This text is intended for educational purposes only and does not replace individualized medical or pathological evaluation.
📚 References:
WHO Classification of Tumours Editorial Board. Head and Neck Tumours. 5th ed. Lyon: IARC; 2022.
PathologyOutlines.com. Ameloblastoma. Available at: pathologyoutlines.com
🖋️ Case and slide coloration courtesy of Dr. Alexandre Carneiro (@AmcarneiroMD), as part of an academic partnership project.
3
10
613
26 Aug 2025
A 66-year-old male with a blister on the lip commissure. #oralpath #oralpathology #pathology #pathologists #pathTwitter #HeadNeckPathol #HeadandNeckPath #ENTPath #PathologyTweet #dermpath
2
8
36
2,897
24 Aug 2025
A 60-year-old man with a parotid mass. #oralpath #oralpathology #pathology #pathologists #pathTwitter #HeadNeckPathol #HeadandNeckPath #ENTPath #PathologyTweet


5
12
39
4,728
20 Aug 2025
A 40-year-old female presented with a maxillary lesion. #oralpath #oralpathology #pathology #pathologists #pathTwitter #HeadNeckPathol #HeadandNeckPath #ENTPath #PathologyTweet
4
4
26
3,463
19 Aug 2025
18 Aug 2025
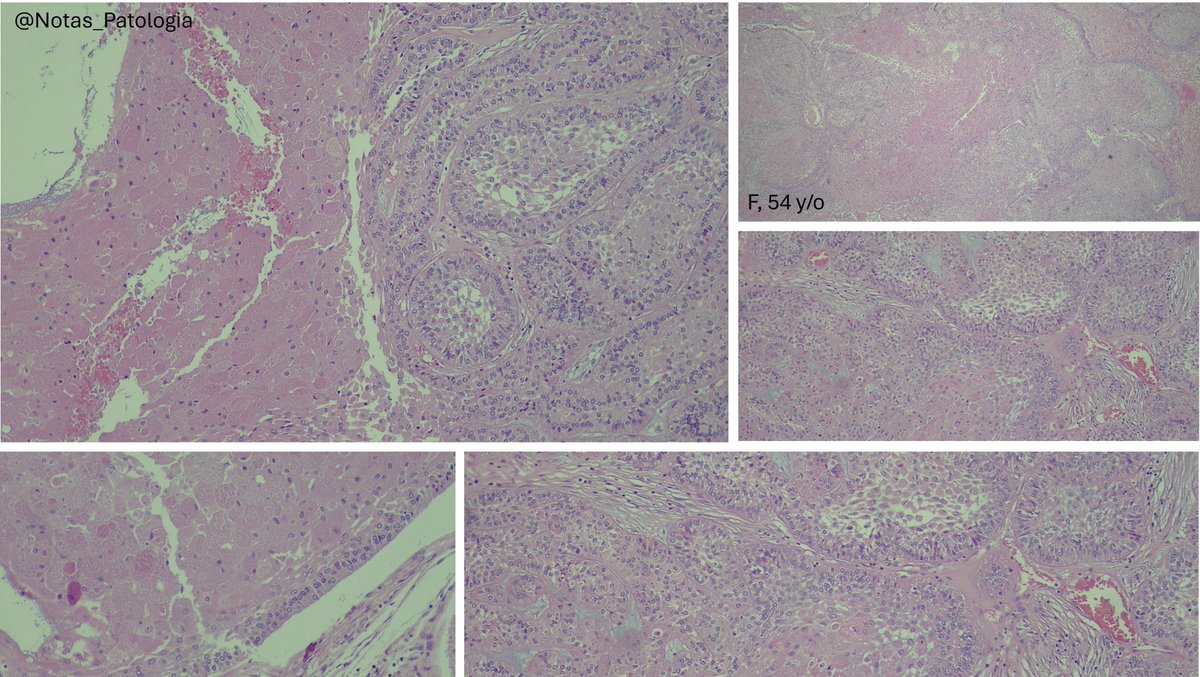
🦷 Clear Cell Odontogenic Carcinoma
📌 Definition
Clear cell odontogenic carcinoma (CCOdC) is a rare malignant odontogenic tumor characterized by sheets, nests, or cords of clear cells within a fibrocellular or hyalinized stroma. It is considered a locally aggressive carcinoma with potential for recurrence and metastasis.
🌍 Epidemiology
Fewer than 150 cases reported.
Mean age: ~53 years.
Female predominance (~63%).
Mandible is the most frequent site (≈75%), especially posterior body and ascending ramus.
🧬 Etiology & Pathogenesis
Etiology remains unknown.
Molecular hallmark: EWSR1 rearrangements (>80% of cases).
Most common partner: ATF1.
Less frequent partners: CREB1 and CREM.
Morphological and immunophenotypic overlap with salivary gland hyalinizing clear cell carcinoma, suggesting a shared pathogenetic mechanism.
🧑⚕️ Clinical Features
Slowly progressive jaw swelling.
May present with:
Pain or tenderness.
Tooth mobility.
Paraesthesia.
Mucosal ulceration (advanced cases).
Less frequent: lymphadenopathy and distant metastases.
🩻 Imaging Findings
Expansile, poorly defined radiolucencies.
Frequent tooth root resorption.
🔬 Pathology
Macroscopic
Intraosseous, tan-white mass.
Ill-defined borders.
May extend into adjacent soft tissues.
Histopathology
Lobular sheets, nests, or trabeculae of polygonal cells with clear to eosinophilic cytoplasm.
Hyalinized or fibrocellular stroma.
Peripheral palisading may be seen.
Clear cells: PAS-positive, diastase-sensitive (glycogen-rich).
Low mitotic index, but perineural invasion can occur.
Necrosis and angiolymphatic invasion uncommon.
Immunohistochemistry
Positive: AE1/AE3, CK5/6, CK19, p63, EMA.
Negative: SMA, calponin, S100.
🧾 Differential Diagnosis
Odontogenic tumors:
Clear cell calcifying epithelial odontogenic tumor.
Odontogenic fibroma (amyloid subtype).
Salivary tumors (intraosseous or metastatic):
Mucoepidermoid carcinoma.
Epithelial-myoepithelial carcinoma.
Metastatic neoplasms:
Renal cell carcinoma.
Melanoma.
Other odontogenic carcinomas:
Odontogenic carcinoma with dentinoid (may show clear cells, but produces dentinoid).
🧪 Diagnostic Molecular Pathology
Detection of EWSR1 rearrangement supports diagnosis.
Interpretation may be challenging in decalcified samples.
📊 Staging
No specific AJCC/UICC TNM system.
ICCR (International Collaboration on Cancer Reporting) datasets recommended for structured reporting.
📉 Prognosis & Complications
High recurrence risk (~40%).
Metastases: cervical lymph nodes most common; lungs and bones less frequent.
Mortality: ~11%.
Late recurrences/metastases may occur, underscoring need for long-term follow-up.
💊 Treatment
First-line therapy: complete surgical resection with wide margins.
Role of adjuvant radiotherapy/chemotherapy: not well defined, may be considered in recurrent/metastatic cases.
📝 Summary
Clear cell odontogenic carcinoma is a rare and aggressive odontogenic malignancy. It primarily affects the mandible, often presents with swelling and pain, and shows distinctive clear cell morphology with EWSR1 rearrangements. Despite its rarity, it requires aggressive surgical management due to high recurrence rates and potential for metastasis.
📚 Reference
WHO Classification of Head and Neck Tumours, 5th Edition, 2022.
⚠️ Disclaimer: Educational content only. Not a substitute for clinical diagnosis or patient management.
🖋️ Case and slide coloration courtesy of Dr. Alexandre Carneiro (@AmcarneiroMD), as part of an academic partnership project.
#MedicalEducation #NotasDePatologia
5
395
18 Aug 2025
58-year-old female with a nasal mass. What is your diagnosis and/or IHC panel? #oralpath #oralpathology #pathology #pathologists #pathTwitter #HeadNeckPathol #HeadandNeckPath #ENTPath #PathologyTweet
4
17
48
4,384
16 Aug 2025
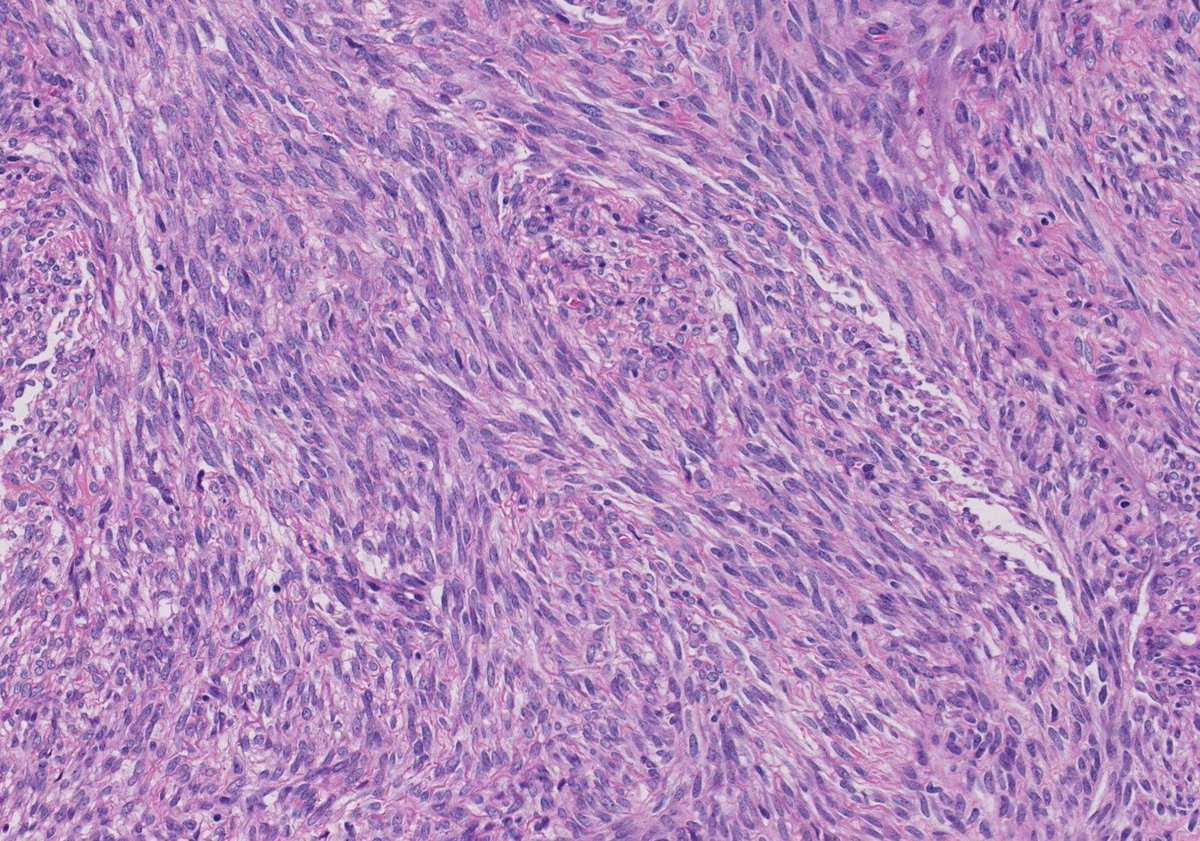
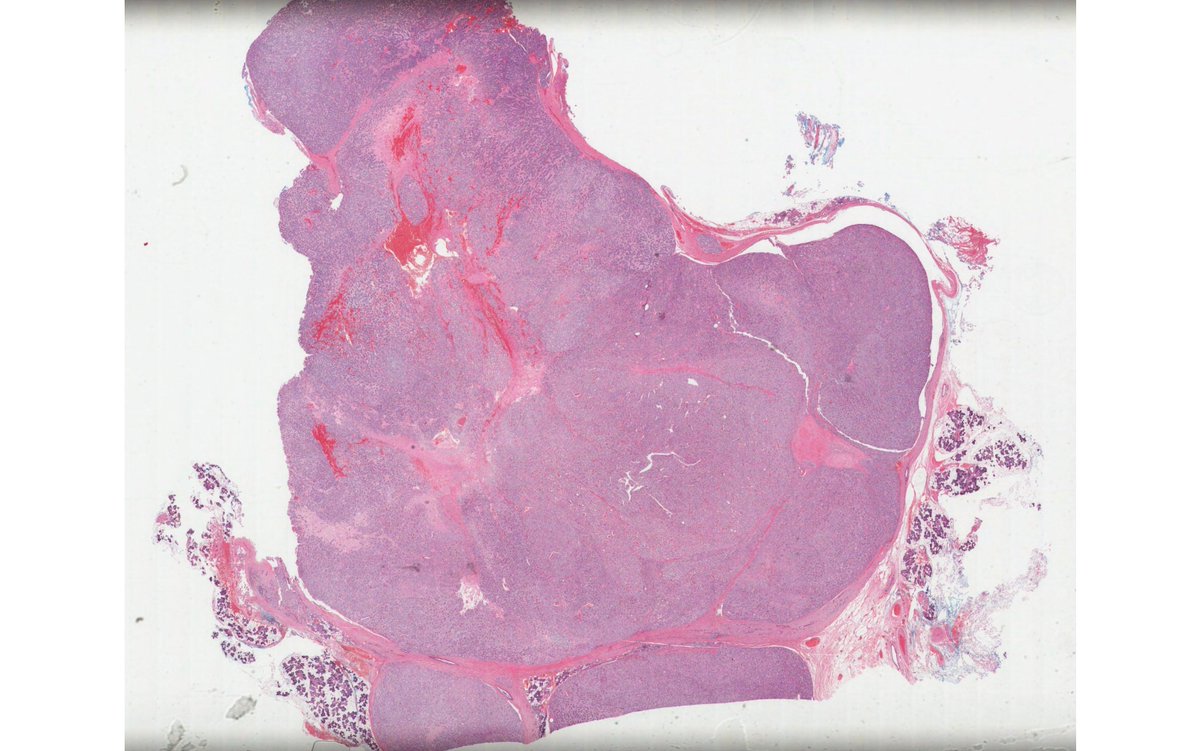
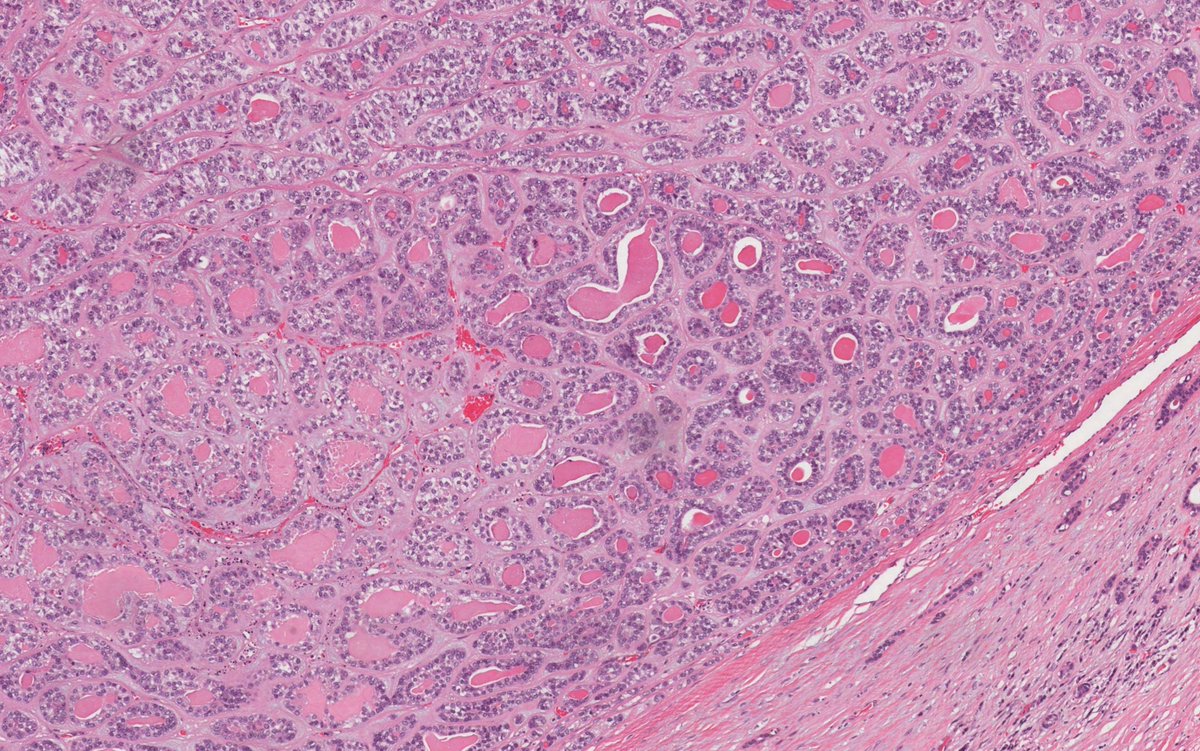
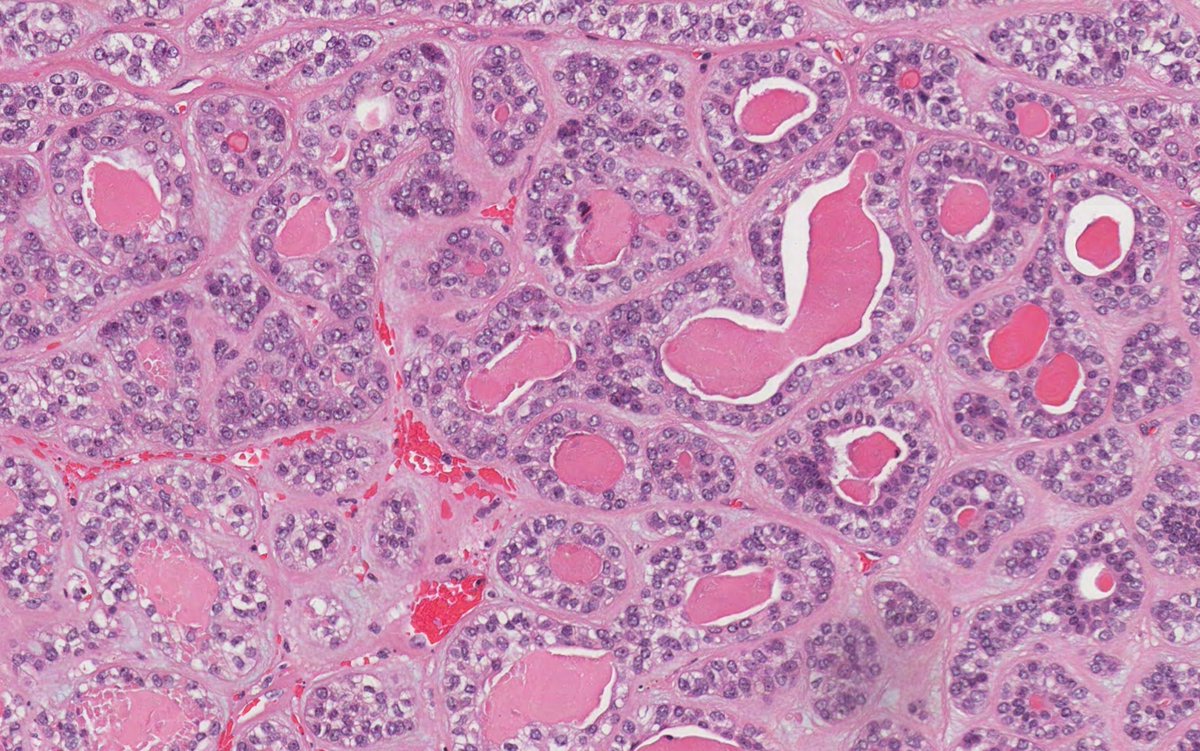
70M with parotid mass. What is your diagnosis?
#oralpath #oralpathology #pathology #pathologists #pathTwitter #HeadNeckPathol #HeadandNeckPath #ENTPath #PathologyTweet
7
17
59
5,159