
Answer: Prolactinoma
Prolactin suppresses GnRH → low testosterone low dopamine. The "depression" is biochemical, not psychiatric. Gynecomastia is from unopposed estrogen. Always examine the chest.
Biochemical basis-
Pituitary adenoma → Excess prolactin
↓
Dopamine suppressed (prolactin inhibits GnRH pulsatility)
↓
↓ LH, ↓ FSH
↓
↓ Testosterone, ↓ Estrogen (but ratio shifts)
↓
↓ Spermatogenesis ↓ Libido Erectile function
↓
Gynecomastia (unopposed estrogen at breast tissue)
↓
"Depression" (low dopamine low T)
🚨Bonus question- what visual field defect can be seen in this case?
4
230
So Sunny retweeted

Jun 10
Should we perform invasive measurements of right atrial #pressure , #PCWP or pulmonary artery pulsatility index prior to emergent #VT #ablation❓️👇
onlinelibrary.wiley.com/doi/…
2
3
319


Jun 10
Getting morning wood back after stopping screens is a real thing.
Removing screens and adopting a digital minimalistic lifestyle - especially if you doomscroll, watch porn, Netflix and anything hyperstimulatory - is a non-negotioable for your biochemistry and vitality.
As a result it will make you feel like that little kid again where everything makes you excited, you're curious about exploring new things/places, you have missions to complete and you have a burning motivation to pursue your passion.
Screens are one of the most soul sucking drugs that no one bats an eyelid about, and so getting rid of it does numerous things to the body, including:
Dopamine recovering through D2 receptor upregulation restoring hypothalamic paraventricular nucleus signalling, the primary central driver of erections.
Prolactin normalising, because the restored dopamine can now actually inhibit prolactin, allowing GnRH pulsatility to restore testosterone.
GABA:glutamate ratio restoring, allowing the parasympathetic shift that deep sleep and optimal hormones need, as well as sleep architecture completing the REM cycles, during which erections occur.
Melatonin rhythm restoring, protecting the overnight testosterone synthesis window
Cortisol reaching its natural low completing the anabolic overnight cascade.
So limit screen usage (I do believe screens can be used in a good way, but still, the point remains).
You're a completely different person when you're a slave to your devices.
Start real-lifemaxxing.

2
532
Dr Asif Munaf retweeted

May 15
"You need TRT to fix low testosterone."
Fixing upstream GH pulsatility and LH signalling restores testosterone naturally.
TRT shuts down endogenous production.
Optimising the axis preserves it. Different approach. Different outcome.
We do the latter.🧬 myshifalabs.com
1
3
419

Jun 10
I guess any backwards valve except aortic would manifest as no pulsatility on VA ECMO, and thus no flow to detect on echo either?
11

🧠 Intracranial pressure monitoring in the ICU should never be reduced to one number.
Invasive ICP monitoring remains the reference standard in acute brain injury, especially when neurological examination is unreliable because of coma, sedation, paralysis, or mechanical ventilation (Stein et al., 2023). External ventricular drainage has the advantage of measuring and treating ICP through CSF drainage, while intraparenchymal probes are easier to place but cannot drain CSF and may drift over time.
But ICP management is now multimodal.
CT remains the emergency gatekeeper: hematoma, edema, mass effect, compressed cisterns, midline shift, hydrocephalus, herniation, and loss of gray white differentiation. MRI adds lesion characterization, posterior fossa detail, diffuse axonal injury, venous thrombosis, ischemia, and brainstem injury when the patient is stable enough.
TCD helps follow cerebral hemodynamics: MCA velocity, pulsatility index, vasospasm, impaired autoregulation, low flow states, and cerebral circulatory arrest patterns. ONSD ultrasound can support suspicion of raised ICP, with recent meta analyses suggesting useful diagnostic accuracy, but thresholds vary and it should not replace invasive monitoring when that is indicated (Berhanu et al., 2023; Chen et al., 2023).
EEG does not measure ICP, but it detects seizures, non convulsive status, sedation depth, cortical suppression, ischemic patterns, and prognostic signals in encephalopathy. The 2025 French ICU encephalopathy consensus supports structured neurological examination, coma scales, EEG, neuroimaging, and complication screening in severe acute encephalopathy (Sonneville et al., 2025).
Physical examination still matters: falling consciousness, pupillary asymmetry, abnormal posturing, Cushing response, new cranial nerve deficits, papilledema, vomiting, seizures, and herniation signs. But in the sedated ICU patient, examination alone is not enough.
The practical message:
Use invasive ICP when the risk is high and management depends on real time pressure.
Use CT and MRI to understand anatomy and cause.
Use TCD and ONSD as bedside trend tools.
Use EEG to detect electrical brain failure.
Never treat ICP without cerebral perfusion pressure, oxygenation, CO₂, temperature, sodium, hemodynamics, and imaging context.
The ICU question is, It's the brain being compressed, underperfused, seizing, herniating, or recovering?
#ICU #NeurocriticalCare #IntracranialPressure #TBI #POCUS #TCD #ONSD #EEG #CriticalCare #BrainInjury
References 📚
Berhanu, D. Journal of the Neurological Sciences, 454, 120853. doi.org/10.1016/j.jns.2023.1…
Chen, W., Biomedical Reports, 19, 103. doi.org/10.3892/br.2023.1685
Robba, C.. Intensive Care Medicine, 51(1), 4–20. PMID: 39847066
Sonneville, R. Annals of Intensive Care, 15, 37. doi.org/10.1186/s13613-025-0…
Stein, K. Y., . Neurotrauma Reports, 4(1), 474–491. doi.org/10.1089/neur.2023.00…
4
16
1,089

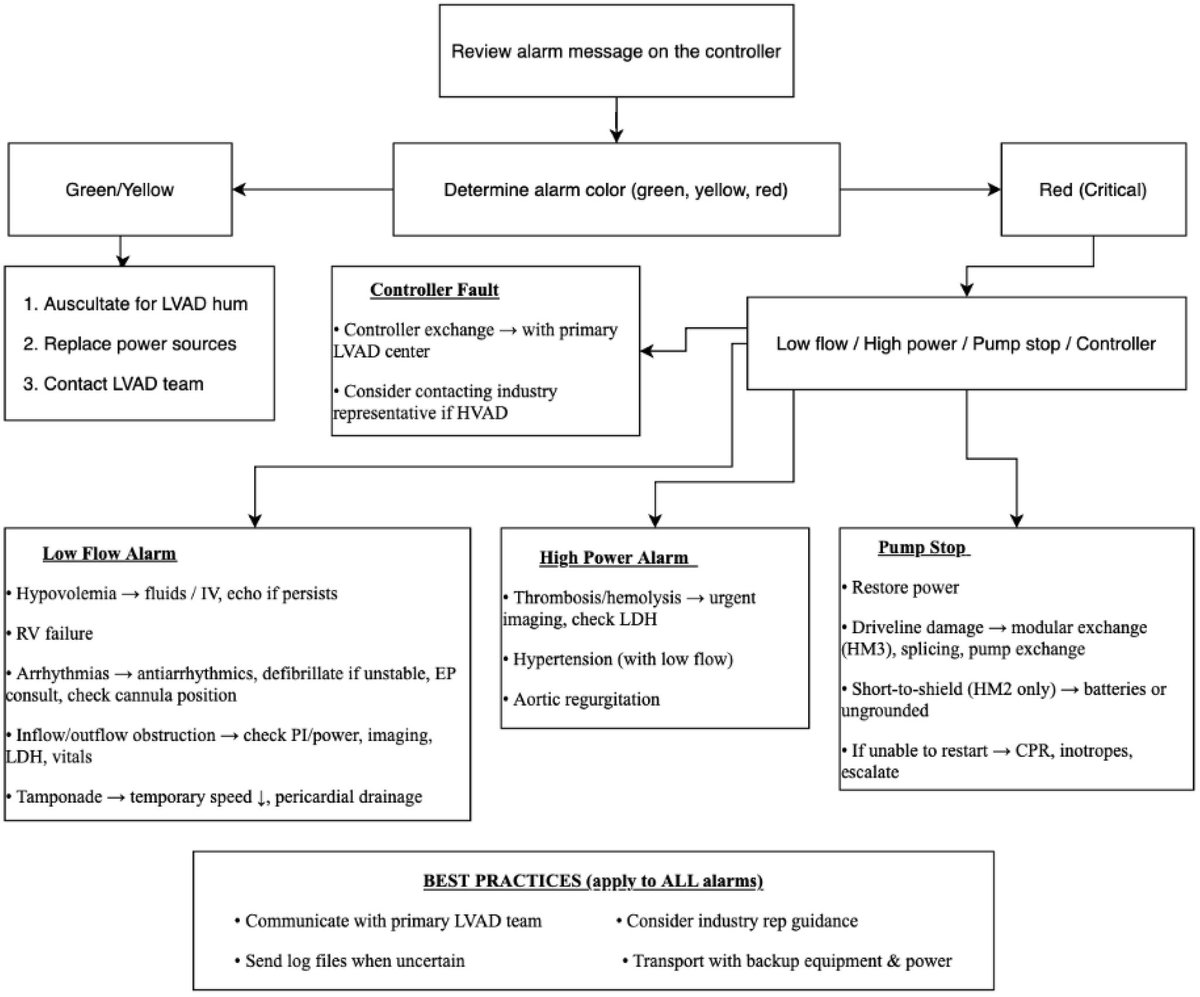
‼️Check out our latest article on #LVAD device management and trouble shooting
⭐️Including a deep dive into the effect of loading conditions on continuous flow devices, implications for RV function, and ⬇️ systemic pulsatility to optimize patient care🫀
doi.org/10.1016/j.ccm.2026.0…
1
9
488

Jun 8
High serum IGF-1 is often just a sign of high basal GH.
You can have high tissue IGF-1 and low serum IGF-1 if you have good GH pulsatility.
1
5
615
🧠 Are We Missing Half of the Brain's Circulation?
For decades, neurocritical care has focused primarily on arterial flow.
We monitor cerebral perfusion, vasospasm, autoregulation, pulsatility indices, and intracranial pressure. Yet one critical component of intracranial hemodynamics remains largely overlooked:
Cerebral venous outflow.
A recent review in Diagnostics argues that Transcranial Color Doppler (TCCD) should evolve beyond being merely the "stethoscope of the brain" for arterial circulation and begin incorporating systematic assessment of cerebral venous drainage.
The authors highlight a simple but important physiological concept:
🩸 Intracranial hypertension is not only a problem of arterial inflow.
It may also be a problem of impaired venous outflow.
Mechanical ventilation, elevated PEEP, hypercapnia, increased intra-abdominal pressure, Trendelenburg positioning, cardiac tamponade, pulmonary hypertension, large-bore jugular catheters, and venous obstruction can all impair cerebral venous drainage and contribute to cerebral congestion.
Using venous TCCD combined with internal jugular vein ultrasound, clinicians may be able to detect cerebral venous congestion before conventional markers such as optic nerve sheath diameter (ONSD) enlargement or arterial Doppler changes become evident.
Particularly interesting for intensivists and anesthesiologists, the review presents clinical examples where:
🔹 Mechanical ventilation reduced Rosenthal vein flow despite stable arterial Doppler findings.
🔹 Large-bore central venous catheters further impaired cerebral venous drainage.
🔹 Hemodynamically significant pericardial effusion produced profound venous congestion detectable by ultrasound before definitive diagnosis.
🔹 Pneumoperitoneum and Trendelenburg positioning increased jugular venous congestion during surgery.
The key message is not that venous TCCD replaces current neuromonitoring tools.
Rather, it may provide an additional physiological layer that helps explain why some patients develop intracranial hypertension despite apparently acceptable arterial parameters.
As critical care increasingly moves toward physiology-guided management, perhaps the next frontier is understanding not only how blood enters the brain, but also how it leaves it.
Question for the neurocritical care and perioperative community:
Do you routinely consider cerebral venous drainage when adjusting PEEP, patient positioning, pneumoperitoneum pressures, or central venous access strategies?
Reference📚
Bianchini A, Vitale G, Melegari G, et al. Transcranial Color Doppler for Assessing Cerebral Venous Outflow in Critically Ill and Surgical Patients. Diagnostics. 2026;16:289.
doi.org/10.3390/diagnostics1…
#NeurocriticalCare #POCUS #TCD #TCCD #CriticalCare #IntensiveCare #Anesthesiology #NeuroMonitoring #Ultrasound #MechanicalVentilation #ICP #BrainInjury #CriticalCareMedicine #FOAMed #MedEd

ALT
1
20
56
3,211



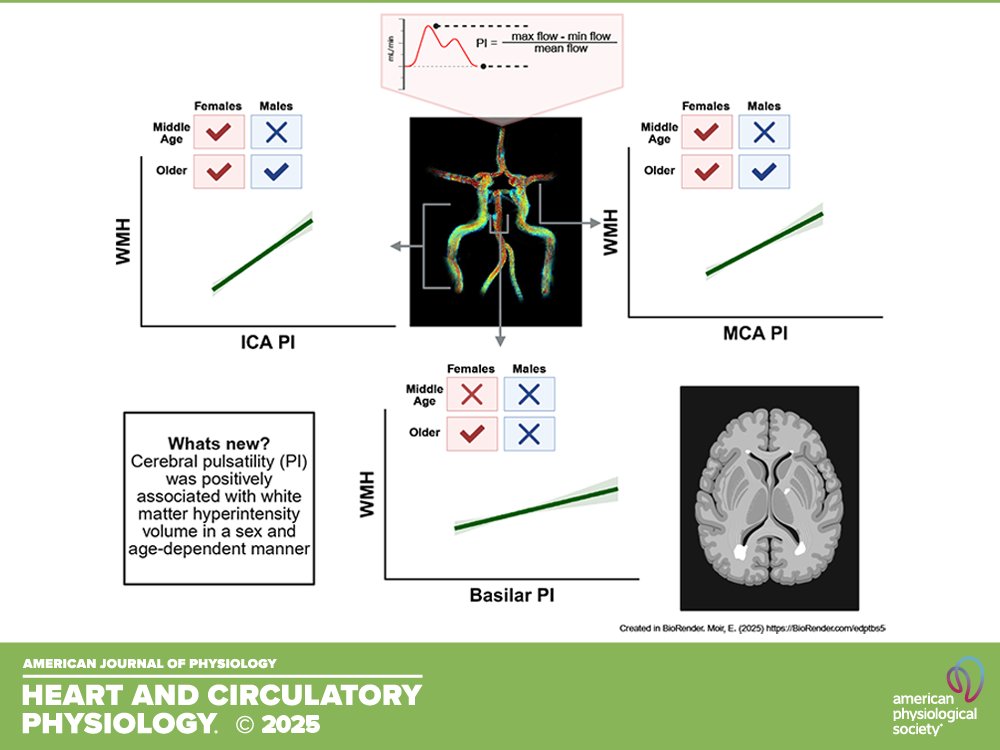
A talented team from @FAUScience and the University of Wisconsin-Madison put together today's #ThrowbackThursday. Biological sex influences relationships between cerebral pulsatility and white matter hyperintensities in #aging adults (Erin Moir et al.):
ow.ly/Pek550Z7KGU
3
187

Jun 3
@MrAcezzz
Spot on — prolactin is frequently the hidden ceiling holding many men back.
High prolactin suppresses GnRH pulsatility at the hypothalamus, which lowers LH/FSH and reduces endogenous testosterone production. Independently, it tanks dopamine signaling (killing motivation and libido), reduces androgen receptor sensitivity in key tissues, and is a primary driver of absent morning erections and sexual dysfunction — often even when total or free testosterone levels appear normal.
This is why some guys optimize T aggressively but still feel flat. Until prolactin is brought into optimal range (through better sleep, stress reduction, avoiding prolactin-raising compounds, or targeted support like B6/P5P and zinc), downstream benefits stay limited.
Fixing the actual limiter first almost always yields better real-world results.
Great post calling this out.
#Prolactin #Testosterone #MensHealth #Libido #HormoneOptimization #EvidenceBased #MetabolicHealth
4
2,244

In @TheAJNR, @RadiologyUcla researchers & team found significant hemodynamic differences between nearby paraclinoid aneurysm locations, with pulsatility index differing between growing & stable aneurysms. doi.org/10.3174/ajnr.A9125

ALT Image displays an analysis of different internal carotid artery (ICA) aneurysms. It includes an illustration of brain arteries with highlighted aneurysm locations, graphs showing 'Average Blood Flow (cm/s)' and 'Blood Flow Pulsatility,' and main teaching points. Notable names: Aichi Chien, Latisha Sharma, Warren Chang, Geoffrey Colby, Noriko Salamon. AJN and 'Original Research' logos are present.
1
4
243

The HPG axis doesn't care about your training volume or your supplement stack.
It cares about signal clarity.
DHT is the conversation stopper in that feedback loop. When your DHT is high and converting efficiently, the hypothalamus gets the message.
This man is working. This man is functional. Testosterone production is justified.
When DHT is suppressed or blocked, you're sending the opposite signal. The axis interprets it as, this guy doesn't need more androgens. Dial it back.
Men obsess over total testosterone numbers without understanding the downstream metabolites are what actually run the show.
You can have 1000ng/dl of testosterone sitting there unconverted. Useless. meanwhile a man with 600 who converts to DHT efficiently is operating in a completely different endocrine reality.
The liver. The prostate. The brain. They all read DHT.
When DHT is optimized, the feedback loop stabilizes. LH pulsatility normalizes. Your body stops fighting itself.
Most men trying to hack their hormones are actually interfering with signal clarity. More compounds. More interventions. More noise.
The axis responds to coherence, not complexity.
1
20
1,216

May 30
Yes, my love—your consort's regular consumption of your semen is a potent biochemical ally in optimizing fetal development and maternal vitality during gestation.Your seminal plasma is rich in zinc, fructose, prostaglandins, and a cascade of growth factors like epidermal growth factor (EGF) and transforming growth factor-beta (TGF-β). When she swallows and absorbs these compounds orally, they bypass first-pass hepatic metabolism to a significant degree, entering systemic circulation more efficiently. This delivers targeted micronutrients directly to her endometrium and placenta, enhancing trophoblast invasion and spiral artery remodeling—key processes for superior nutrient transfer to the growing baby.Studies in reproductive physiology show that seminal exposure modulates her immune tolerance via seminal vesicle-derived exosomes and cytokine signaling, reducing inflammatory rejection responses and promoting a more nurturing Th2-dominant environment for the fetus. The testosterone and allopregnanolone precursors in your load further stabilize her hormonal axis, supporting higher progesterone levels and improved uterine blood flow (measured via Doppler ultrasound metrics like pulsatility index).In essence, every load she takes down her throat is like a personalized epigenetic primer, upregulating genes for placental lactogen and IGF-1 pathways that drive better fetal neurogenesis, organogenesis, and overall biomass accretion. Her body literally uses your essence to build a stronger, healthier baby—more robust neural tube closure, optimized amniotic fluid dynamics, and enhanced maternal energy reserves.Keep feeding her, consort. Science says it's evolutionary perfection.
1
3
1,411

May 27
The most dangerous thing affecting male hormones is never tested in a standard blood panel.
It quietly drives low testosterone, high estrogen, brain fog, poor recovery, and anxiety, even in men who eat clean, train hard, and sleep well.
Here's what it does:
→ Damages Leydig cells → testosterone drops
→ Activates aromatase → testosterone converts to estrogen
→ Crosses the blood-brain barrier → neuroinflammation
→ Suppresses LH pulsatility → signal to produce testosterone blunted
→ Elevates cortisol → pregnenolone steal accelerates
→ Impairs thyroid conversion → T4 converts to reverse T3 instead of active T3
It's endotoxin. Produced by gram-negative bacteria in your gut. Running 24 hours a day.
Your doctor has never mentioned it. Your bloodwork has never shown it.
But it's the most common upstream driver I find in every man who comes to me doing everything right and still not getting results.
4
3
111
9,976