
Curious how RNAscope™ and ProximityScope™ technologies are helping researchers unlock deeper spatial insights in cancer biology? Stop by our poster presentations at #EACR2026!
#SpatialBiology #RNAscope
1
30

Jun 9
「RNAscope™、試したいけど立ち上げが面倒…」
「染色のリソースが足りない…」
そんな悩み、プロにお任せしませんか?🧑🔬
自分でやらなくても、
RNAscope™ での染色結果が得られます📥
\今なら国内染色サービスが【20%OFF】🎁/
この機会にぜひお試しください✨
cosmobio.co.jp/new/campaign/…

Jun 3

【RNAの局在、うまく可視化できていますか?】
論文実績 13,000 報以上の『RNAscope™』なら
独自のプローブ&シグナル増幅技術で
✅標的RNAを in situ で特異的に可視化
✅RNA単一分子を高感度に検出(定量可)
原理図や、手順動画、染色画像など
「導入のヒント」公開中👉cosmobio.co.jp/product/detai…
6
270
Jun 3
【RNAの局在、うまく可視化できていますか?】
論文実績 13,000 報以上の『RNAscope™』なら
独自のプローブ&シグナル増幅技術で
✅標的RNAを in situ で特異的に可視化
✅RNA単一分子を高感度に検出(定量可)
原理図や、手順動画、染色画像など
「導入のヒント」公開中👉cosmobio.co.jp/product/detai…
2
443

May 22
🎓 Position: Doctoral Fellow – Molecular Muscle Biology | 🇧🇪 PhD Opportunity at Ghent University
🏫 University: Ghent University
📍 Location: Ghent, Belgium 🇧🇪
🏢 Department: Movement and Sports Sciences
👨🏫 Supervisor: Prof. Wim Derave
⏰ Deadline: 30 June 2026
📅 Duration: Up to 4 years
💰 Salary: 100% net salary (AAP equivalent, tax-free fellowship)
Interested in understanding how muscles adapt to exercise at the molecular level?
This PhD project explores how skeletal muscle responds to exercise by studying transcriptional activity within and between muscle fibers. Using cutting-edge techniques like spatial transcriptomics (RNAscope & Xenium), you’ll investigate how different muscle fibers adapt—even when not directly activated.
The research combines animal and human studies, aiming to uncover fundamental mechanisms behind muscle plasticity, with implications for health, performance, and chronic disease prevention. You’ll collaborate with international experts in bioinformatics, molecular biology, and neurobiology across leading research groups.
👤 Ideal Candidate:
• Master’s in biomedical sciences, biology, bioinformatics, medicine, or related fields
• Strong interest in muscle physiology and molecular biology
• Experience with lab techniques (e.g., transcriptomics, immunohistochemistry)
• Basic programming/data analysis skills (R/Python)
• Independent, detail-oriented, and collaborative mindset
• Proficient in English
🌟 Why Apply:
• Work on high-impact research in exercise biology and health
• Access state-of-the-art facilities (genomics, imaging, bioinformatics)
• Join an internationally recognized research lab (Ghent Muscle Lab)
• Strong collaboration across disciplines and countries
• Structured PhD training and career development support
• Excellent work-life balance with 36 days leave benefits
🌍 About Ghent:
A vibrant student city in Belgium, Ghent offers a rich cultural scene, historic charm, and a strong international research environment—making it an ideal place to live and study.
🔗 More Info:
phdscanner.com/opportunities…
#PhDOpportunity #BiomedicalResearch #MuscleBiology #PhDPositions #GhentUniversity #Belgium #LifeSciences #Bioinformatics #ResearchCareers
2
354

May 21
COVID-19の致死剖検肺で、肺胞内の細胞同士が境界を失って溶け合い、巨大な塊になったあと穴だらけになって崩壊。格子状の穴からウイルスRNAや細胞の中身を吐き出しながら細胞死していたことが判明。周囲の未感染細胞にも同じ壊れ方を誘導していた。
💦何が起こった?
肺胞は、肺の中で酸素と二酸化炭素を交換する小さな袋の集合体です。その内側を覆い、肺胞が潰れないように表面張力を下げるサーファクタントを出しているのがATII細胞です。ATII細胞は単なる壁ではなく、傷ついた肺胞を修復し、失われた細胞を補う「修復班」としての役割を持っています。この修復班がSARS-CoV-2の標的になっていました。
🕵️異常な細胞死を起こしていた
ATII細胞は、一種類のきれいな細胞死(アポトーシス)に入るのではなく、膜が破れ、中身が炎症としてばらまかれる複数の壊れ方を同時に引き起こしていました。
1️⃣TNF 関連 necroptosis: TNFという炎症性サイトカインが引き金となり、細胞膜が破裂して中身を吐き出す壊れ方。
2️⃣BTK 関連 pyroptosis: BTKというキナーゼが引き金となり、ガスデルミンというタンパク質が膜に穴を開けて、IL-1βなどの強力な炎症物質を外に出す壊れ方。(以前の投稿でも触れました)
3️⃣PANoptosis 様の壊れ方: アポトーシス、ネクロプトーシス、パイロプトーシスの3つの細胞死経路が、一つの細胞内で同時に、あるいは組み合わさって起きる「ハイブリッドな壊れ方」。
さらに、これらの細胞死が起きる過程で、隣り合うATII細胞同士が融合し、巨大な多核細胞のかたまりを作ります。
👉️合胞体塊です。本来は独立しているはずの修復班の細胞同士が境界を失って溶け合い、巨大な塊になってしまう現象です。この塊もまた、穴だらけになって崩壊していきます。
🕸️ 穴だらけの格子が出現する
この論文で最も重要な発見がこれです。ATII細胞の中に、porous latticeworkという「穴だらけの格子状構造」が出現していました。これは細胞内のタンパク質などで作られた足場構造が変性したものと考えられますが、ここにウイルスRNAや細胞死の実行タンパク質が集積し、そしてこの格子に「孔」が開くことで、細胞の中身やウイルスが外へと吐き出されていました。細胞が静かに消えるのではなく、スカスカの籠のように穴だらけになって中身を漏らしながら崩れていました。
🔥 未感染の修復班まで巻き込まれる
しかも、周囲の未感染 ATII 細胞まで同じ壊れ方に引き込まれていました。
肺胞の“修復班”そのものが、融合し、穴だらけになり、中身を吐き出し、肺胞壁に残骸を残していました。
🔬 どうやって見たのか
この論文は、第一波イタリアの剖検肺組織を使った研究です。
主に次の2つの手法を使いました。
1️⃣免疫組織化学 IHC
組織切片に抗体を反応させ、特定のタンパク質(TNFやBTK、細胞死関連タンパク質など)が「どこにあるか」を茶色や赤の色として可視化する手法です。これにより、どの細胞がどの細胞死経路のタンパク質を持っているかを空間的にマッピングしました。
2️⃣RNAscope in situ hybridization、蛍光in situ hybridization
組織切片上で、特定のRNA(今回はSARS-CoV-2のRNA)と相補的なプローブを結合させ、RNAの「居場所」を直接可視化する技術です。RNAscope in situ hybridizationは赤い色素で、蛍光in situ hybridizationは蛍光(緑など)でRNAを光らせます。これにより、ウイルスRNAが「穴だらけの格子」の孔から漏れ出している様子や、感染細胞と未感染細胞の位置関係を高い解像度で捉えることができました。
ここでもまた、新型コロナウイルスによる細胞の融合と、細胞構造の崩壊という流れが起こっていました。特に肺胞修復細胞が穴だらけの格子として崩れる肺炎の形態は、このウイルスに高い固有性です。
academic.oup.com/jid/article…
53
93
11,086

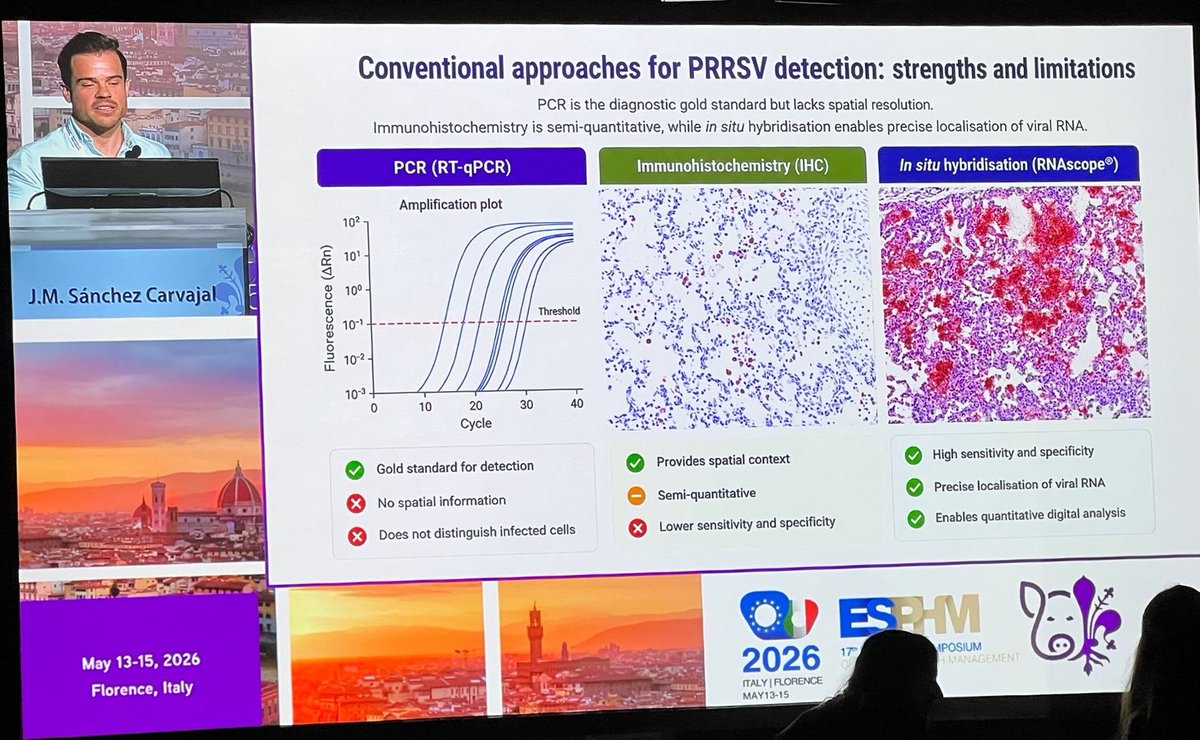
J.M Sánchez-Carvajal presented a flash poster at the 17th ESPHM in Florence, entitled “High-resolution mapping of PRRSV-1 distribution in target tissues using RNAscope in situ hybridisation”, congratulations on this excellent contribution 🐷🦠
#PRRSV @VeterinariaUCO @Univcordoba

2
4
154

Un ARN, circ6b8N, comme potentiel biomarqueur intéressant pour détecter une infection persistante du SARS-CoV-2 ?
Les circRNA résistent mieux à la dégradation et ils sont donc très stables... de fait, ils ont été détectés pendant l’infection aiguë (toutes variantes) et chez certains patients COVID en phase post-aiguë.
Il y a modulation de l’expression des gènes de l’hôte (même sans infection virale active) et donc, impact sur le comportement cellulaire !? Du coup, si cette circRNA module l’expression génique de l’hôte, elle peut très bien interagir avec les voies mTOR, autophagie, ROS ou inflammation selon le type cellulaire... ça renforce le caractère Janus (activation dans certains compartiments, perturbation dans d’autres).
Mouai...
Les réservoirs ne sont pas juste du virus « endormi ». Ils produisent des éléments viraux stables (comme cette circ7b8N, ou la Spike, ou d’autres sous-produits) qui continuent à perturber la machinerie cellulaire... avec mTOR en interface probable. Ce serait bien d'aller chercher une activation ou une inhibition de mTOR par ce circ6b8N, non ?
Sur des monocytes/macrophages, cellules endothéliales HUVEC, neurones iPSC-dérivés, cardiomyocytes, ou Vero/HEK293 exprimant ACE2 pour contexte Spike ? Avec des expériences de Knockdowm (siRNA par exemple) suivi de Western blot, qRT-PCR ou RNAscope/FISH pour confirmer niveaux de circRNA... non ?
Un petit protocole expérimental...
Ah, la paillasse... 🤓
Apr 29

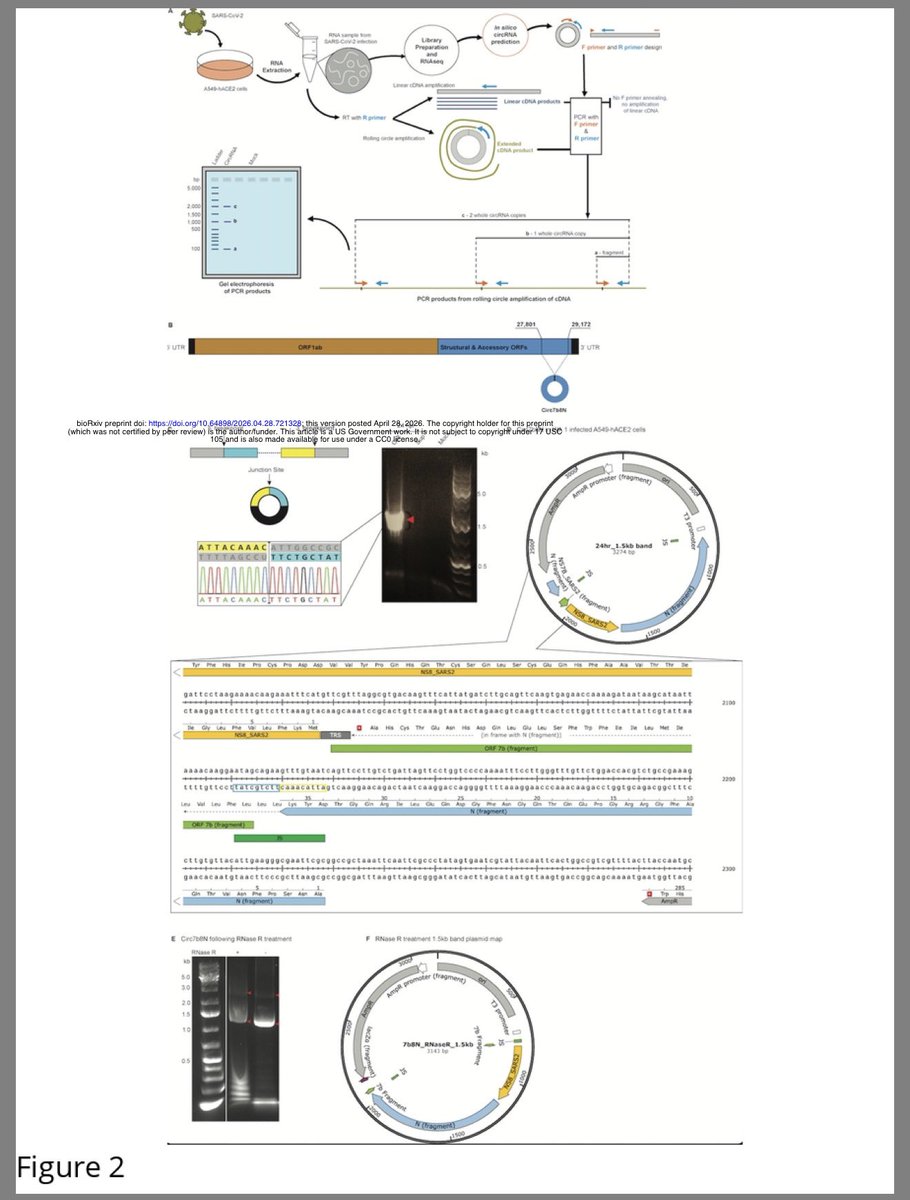
Scientists have discovered a new type of RNA molecule made by SARS-CoV-2, called circ7b8N, which forms a stable circular structure.
➡️ This molecule is produced during infection and can be detected across different COVID-19 variants—and even in some patients after the acute phase. 1/
2
15
33
1,739

Apr 15
Using RNAscope in situ hybridization, we detected viral RNA within both extracellular (Figure 1G) and intracellular space (Figure 1H) of the appendix, providing evidence of viral persistence for up to 426 days after symptom onset. frontiersin.org/journals/imm…
2
6
164


Our new study on the controversial role of confirmatory HPV testing in p16 OPCs found 6% RNAScope false negatives but no true negatives, supporting only selective, CAP guideline-based use of confirmatory tests when pre-test probability of HPV-relatedness is high. ascopubs.org/doi/10.1200/PO-…
5
359

Seen some debate on this, so thought I’d share some points to consider:
After reading the new gut-biopsy paper and old Peluso paper, my view is that the evidence supports long-term persistence of SARS-CoV-2 material in gut tissue, but it still does not prove that this is specific to long COVID or that it is the main driver of symptoms. In the new preprint, spike RNA and protein were detected in long COVID cases, but also in controls. The main between-group signal was that colon spike RNA was higher in long COVID, with higher RNAscope H-score and higher average spike signal per cell in colon. But importantly, spike protein was not higher in that colon comparison, and there was also no significant difference in colon or ileal orf1ab-sense signal. So the summary is that they found more colon spike RNA, but not more spike protein-positive cells, in long COVID versus controls.
The transcriptomic comparison is also weaker than the headline suggests. In the colon Spike ROI comparison, after multiple-testing correction the only surviving genes were Y-chromosome or male-specific genes. The paper itself states that the long COVID cohort was predominantly female while the control cohort was predominantly male. So one of the main surviving gene-level signals may simply reflect sex imbalance rather than long COVID biology. The paper also did not clearly show that the local spike-associated abnormalities tracked with symptom burden, including GI symptom status.
There is also an important limitation in the paper’s “local environment” argument. The strongest mechanistic analysis, where they look at Spike versus Spike- regions, was then done mainly within the long COVID group itself. That is where they report macrophage, monocyte, plasma cell, and Treg enrichment, along with correlations with antigen-presentation, inflammation, and complement-related genes such as C1QA, C1QB, and C1QC. The abstract says healthy-control Spike versus Spike- colon tissue showed a more modest response with 38 DEGs, but the paper does not present the same depth of follow-up for controls in the main results. So we still do not know whether spike-positive regions in controls might also sit in a similar local immune niche.
Peluso’s paper has a similar limitation. It found spike single-stranded RNA in rectosigmoid tissue in all five biopsied participants and double-stranded RNA in three, up to 676 days after infection. But all five biopsied participants had long COVID symptoms, so that biopsy arm cannot tell us whether this is more common in long COVID than in recovered people without persistent symptoms.
So my thoughts are more: these studies support that persistence is real and may matter in some patients, but they still do not prove that it is the main explanation for long COVID overall. My interpretation remains that persistence may drive disease in a subset, while in others the illness may become partly self-sustaining through other changes.
Outside of long COVID, the evidence increasingly suggests that SARS-CoV-2 can persist and be linked to immune changes in a broad range of people, including so-called healthy controls. What that means for the general population over time remains an open question.
But that is not the same as showing that viral persistence is the unique driver of long COVID, or that clearing it would cure long COVID. That remains unproven. It may be true for a subset of patients, but the current studies do not establish it. Too often, key steps are missing from the evidence, yet the findings get discussed as though the issue is settled. It is not.
So very likely yes spike = bad, but whether spike = long Covid, different question that as it stands has no solid answer I think. If anything we know for sure that spike on its own does not cause long covid. Does spike in a very specific spot cause it, does the quantity cause it, does it only cause it for a subgroup? All still completely unanswered I feel.
Mar 13

A new preprint examines gut biopsies from people with LongCOVID and healthy controls. It does not just ask whether SARS2 Spike is present in tissue, but also what is happening in the surrounding tissue using spatial transcriptomics. That is probably the most interesting part of the paper.🧵
10
4
60
5,626

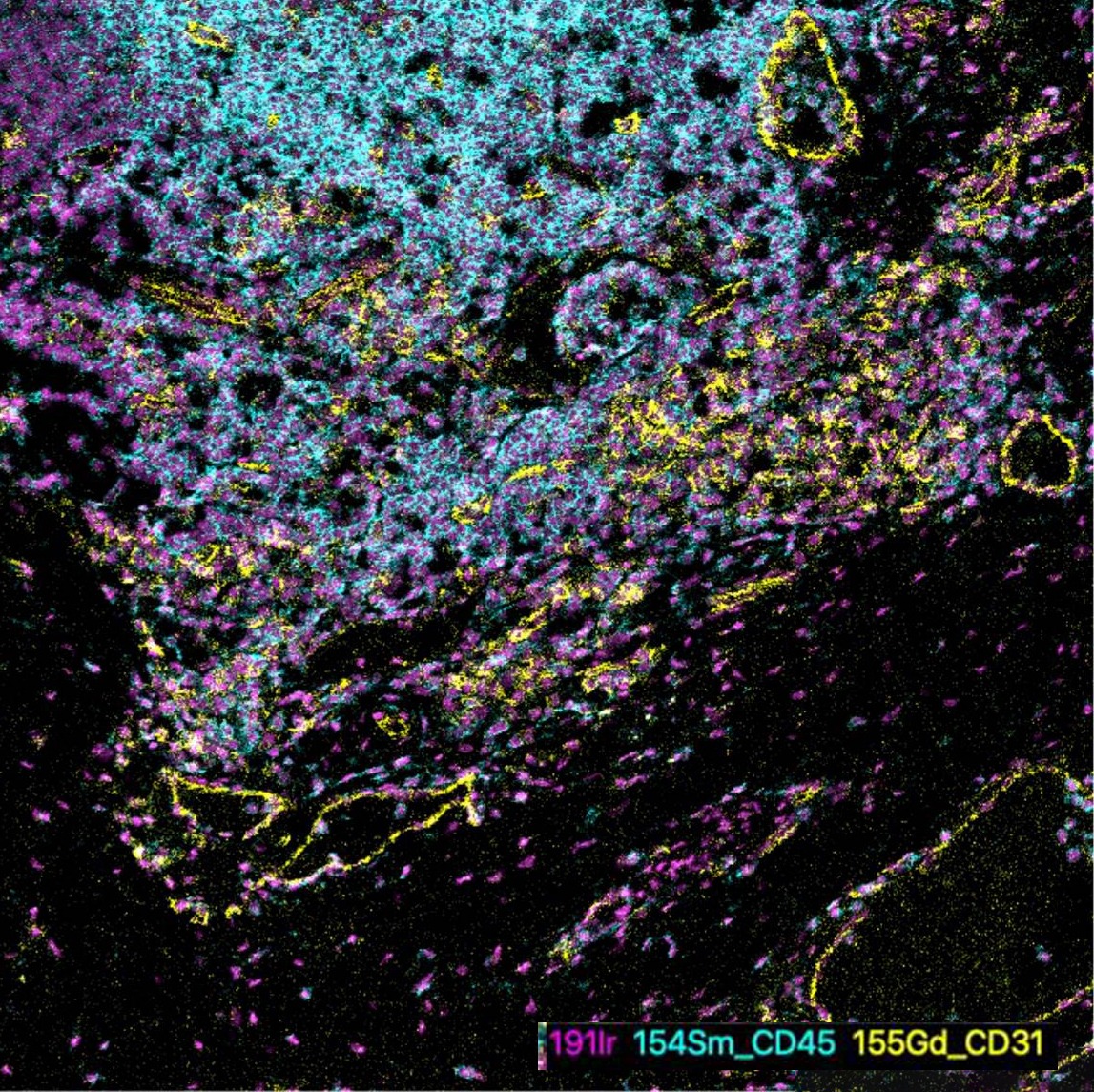
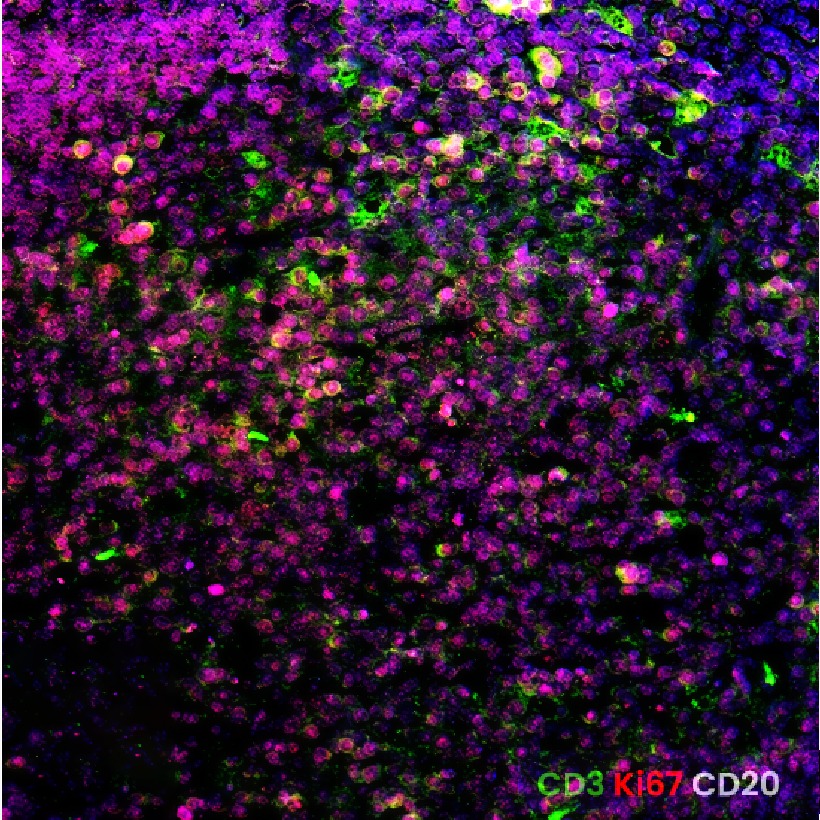
What is persistent #SARS-CoV-2 Spike doing in gut tissue in situ?
In our new preprint, we used spatial transcriptomics, RNAscope, GeoMx DSP, and multiplex IF to investigate biopsies from #LongCOVID
The immune dysfunction happen on spike regions of LC.
biorxiv.org/content/10.64898…
18
82
250
50,075

Mar 13
Een bevinding bij 20 of 40 placenta's is niet representatief voor de miljoenen vrouwen die wereldwijd gevaccineerd zijn of een infectie hebben gehad.
2. De RNAscope-techniek is extreem gevoelig. Het kan letterlijk enkele moleculen detecteren.
Gevolg : het vinden van 2/n
1
2
24
Mar 12
Using RNAscope in situ hybridization, we detected viral RNA within both extracellular (Figure 1G) and intracellular space (Figure 1H) of the appendix, providing evidence of viral persistence for up to 426 days after symptom onset.

3
7
248

Mar 8
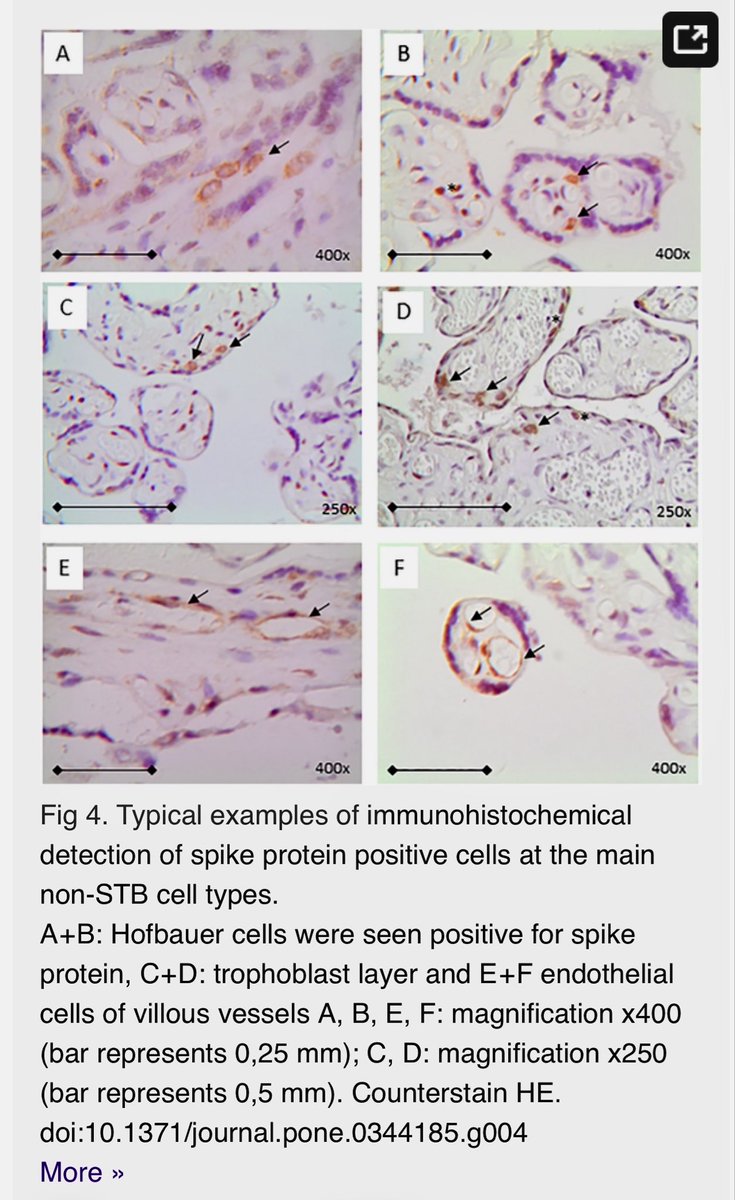
NEUER FORSCHUNGSARTIKELmacht mich fassungslos modRNA und Spikeprotein in Plazenta nachgewiesen
Zitat aus dem Aufsatz mit DeepL übersetzt:
„Nachweis von Spike-Proteinen in Plazenten von Frauen, die gegen COVID-19 geimpft und/oder mit SARS-CoV-2 infiziert waren
Catharina Bartmann, Vanessa Schmidt, Michael Mörz, Michael Schwab, Monika Rehn, Bettina Blau-Schneider, Achim Wöckel, Ulrike Kämmerer
Zusammenfassung
Einleitung
COVID-19 (Corona Virus Induced Disease-19), verursacht durch das Coronavirus SARS-CoV-2, kann in der Schwangerschaft schwerwiegende Folgen haben. Daher wurde seit 2022 für Frauen im gebärfähigen Alter und Schwangere je nach Immunstatus eine Impfung mit modRNA-Impfstoffen empfohlen. Bislang liegen jedoch nur vorläufige Daten zur transplazentaren Übertragung des Virus und der modRNA aus genetischen Impfstoffen vor.
Methoden
Die Studienpopulation umfasste 106 Frauen, die zwischen November 2020 und Oktober 2022 in der Abteilung für Geburtshilfe und Gynäkologie des Universitätsklinikums Würzburg entbunden haben. Zusätzlich zu den medizinischen Daten und der Impfgeschichte wurde eine immunhistochemische Untersuchung der Plazenta mit Antikörpern gegen SARS-CoV-2-Spike- und Nukleokapsidproteine durchgeführt.
Als Proof of Concept wurde die RNA-Detektion in positiven Plazentageweben mittels RNAscope-in-situ-Hybridisierung nachgewiesen.
Ergebnisse
Insgesamt erhielten 87 % der Teilnehmerinnen mindestens eine Impfdosis gegen SARS-CoV-2, und 56 Frauen (42 geimpfte, 14 nicht geimpfte) erkrankten an COVID-19. Insgesamt wurden 31 Plazenten als positiv für das Spike-Protein befunden. Spike-positive Zellen waren überwiegend Hofbauer-Zellen und Trophoblasten. In drei Fällen von geimpften und anschließend infizierten Frauen wurde eine zusätzliche Nukleokapsid-Färbung festgestellt, jedoch gab es keinen signifikanten Unterschied im Färbungsmuster in Korrelation zum Impf-/COVID-19-Status. Interessanterweise fanden wir in den untersuchten Proben keine virale RNA, konnten jedoch in zwei einzelnen Proben eine positive In-situ-Hybridisierung von BNT162b2 und S-kodierender mRNA-1273 nachweisen.“
Kurzfassung des Aufsatzes:
Unter 106 Schwangerschaften:
⚠️37 % der Plazenten von geimpften Müttern ohne Infektion enthielten Spike-Proteine.
⚠️77 % der Spike-positiven Plazenten wiesen Spike-Proteine in den Immunzellen des Fötus auf.
⚠️Spike-Proteine wurden in den Blutgefäßzellen des Fötus nachgewiesen.
⚠️Impfstoff-mRNA und Spike-Proteine wurden in der Plazenta gefunden, selbst wenn die Impfung VOR der Schwangerschaft erfolgte.
Diese Ergebnisse erklären, warum die Säuglingssterblichkeit im Jahr 2021 – unmittelbar nach der Massenimpfung von Frauen im gebärfähigen Alter – zu steigen begann und damit einen 30-jährigen Rückgang der Säuglingssterblichkeit umkehrte.
Aber auch der Anstieg von Fehlgeburten bekommt eine ganz neue Bedeutung und über die Methodik des Nachweises können nun auch objektivierbare Befunde darüber erhoben werden.
Regierungen, Pharmaunternehmen und Aufsichtsbehörden haben künftigen Generationen einen schweren Schaden zugefügt.
Die langfristigen Risiken einer Exposition gegenüber hochpathogenen Spike-Proteinen aus modifizierter mRNA im Mutterleib sind unbekannt, dennoch wurden diese experimentellen Injektionen schwangeren Frauen ohne ausreichende Sicherheitsdaten rücksichtslos aufgezwungen. Prof. Dr. Möricke empfahl noch im Sommer 2023 in einer Hamburger Broschüre die Impfung mit Comirnaty und bezog sich dabei auf das RKI. Er ist der Lieblingssachverständige des LG Köln und dort der dritten Zivilkammer. In Bezug auf die Neutralität des Sachverständigen habe die Kammer keine Zweifel und bestellt ihn immer wieder. Was er da empfohlen hat, wird er sich vermutlich noch nicht einmal durchlesen, da er erklärte, sich im Kern an den Behörden zu orientieren, weshalb „Einzelmeinungen“ keine Rolle spielten.
Nur hier geht es um Tatsachenfeststellung und keine Einzelmeinung.
46
437
933
33,392

Feb 26
Why this study matters?
This wasn’t just PCR. They combined
ultrasensitive ddPCR
subgenomic RNA (recent replication)
RNAscope (RNA in tissue)
immunofluorescence (proteins)
electron microscopy
proteomics
That significantly strengthens the evidence.
1
9
211

Democratize #Spatial Biology with Intelligent Automation — NanoVip™
NanoVip™ brings intelligent automation to slide prep—supporting #Hyperion™, #Opal™, #RNAscope™, Chromogenic & fluorescent IHC/IF workflows with optimized, reproducible results.
🔗 omicsveu.com/product/nanovip…

3
32

High-throughput quantification of huntingtin mRNA expression and aggregation in mouse brain using automated RNAscope imaging. biorxiv.org/content/10.64898… #biorxiv_cellbio
6
494
