
Cancer surgeon-scientist @PennMedicine. Our lab advances therapy for #headandneckcancer #HPV #hnscm. Opinions my own. Patient appointments 2156626972
Joined May 2019
- Tweets 456
- Following 1,552
- Followers 834
- Likes 1,955
19 Photos and videos




Pinned Tweet

30 Mar 2025
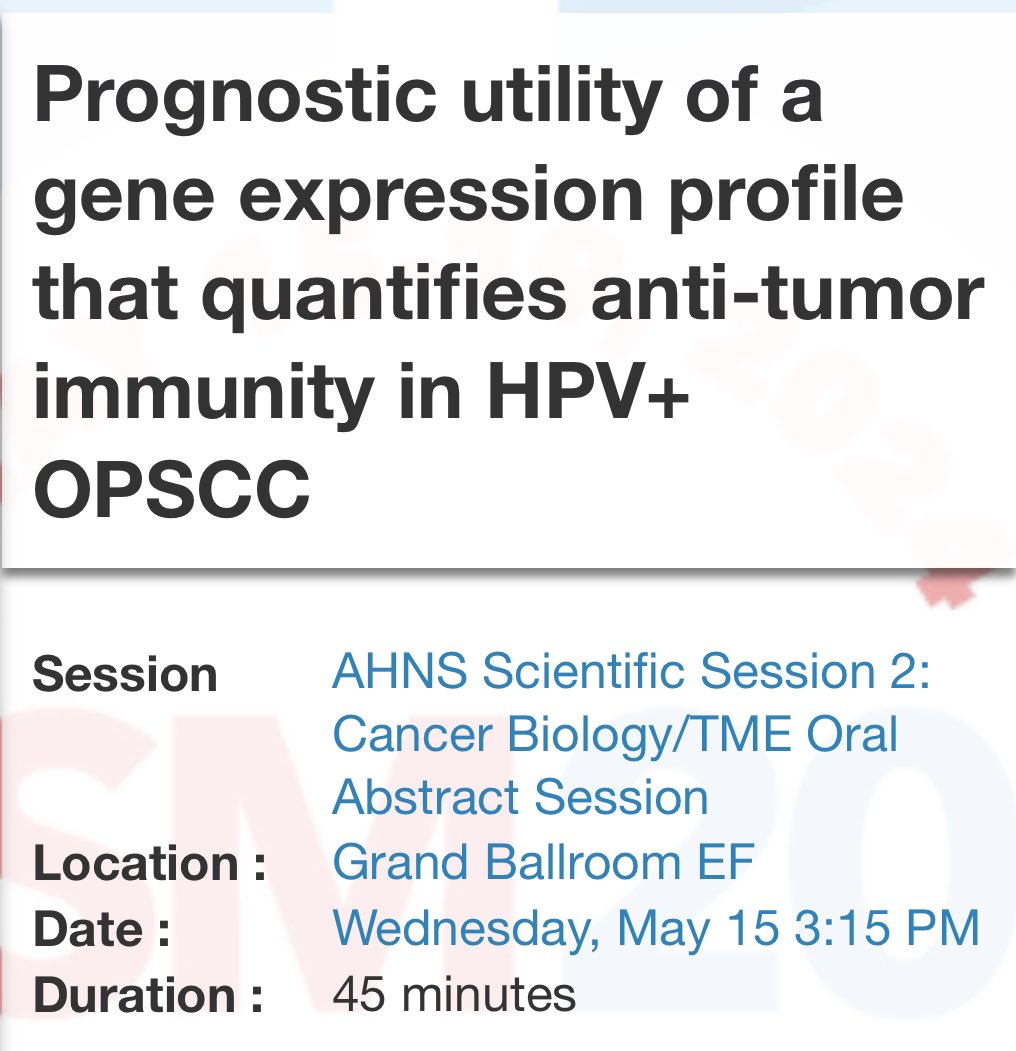
@JNCI_Now We defined the gene expression profiles distinguishing HPV OPSCCs that are prone to recur after TORS-based therapy. These the tumor-intrinsic and immune-related traits were tightly interrelated and generalizeable to nonsurgical cases as well. academic.oup.com/jnci/advanc…
3
4
25
2,470
Devraj Basu, MD, PhD, FACS retweeted

Mark was a phenomenal human being and leader - a great loss.

Mark A. Varvares, MD, FACS, passed away on May 20, 2026 surrounded by his family leaving behind a legacy defined by the countless lives he has touched
Viewing and funeral service will be Saturday, May 30th, St Nicholas Greek Orthodox Church in St Louis, MO
buff.ly/iORf2w8

1
1
5
1,135
Some interesting results to unpack here

Sharing the results of ReACT 1.0 in @NatureComms -- the first study to use HPV ctDNA to guide CRT de-escalation in higher risk HPV OPC. ctDNA metrics may improve risk stratification. Grateful to our coauthors. @Naveris_inc @DanaFarberNews @jdschoenfeld1
nature.com/articles/s41467-0…
1
174
Devraj Basu, MD, PhD, FACS retweeted

19 Feb 2020
So, you want to lead a randomized trial?
I ran a poll: How many people have near veto power over the approval & design of an investigator initiated oncology randomized trial? Only 23% guessed right.
Answer: >50! @RielyMD @mtmdphd
Here are the steps to do an RCT? Thread 1/
6
94
250
Devraj Basu, MD, PhD, FACS retweeted

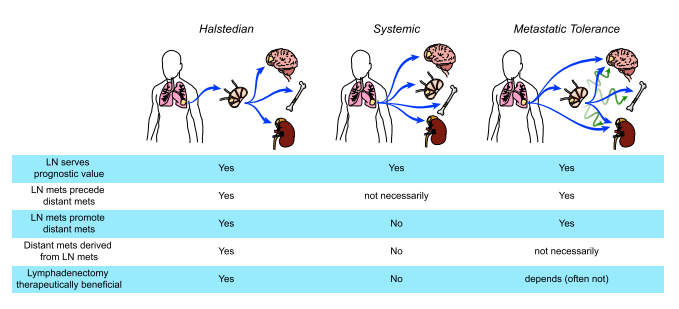
New @Nature study: >50% of lung cancer metastases are seeded by other metastases, not the primary tumor. This "seeding from seeding" reveals a complex evolutionary cascade that allows cancer to colonize the body.
nature.com/articles/s41586-0…
7
176
634
69,204
Devraj Basu, MD, PhD, FACS retweeted

Mar 25
It is a well-written editorial, and I agree with some parts and disagree with others.
However, I am very disappointed that @TheLancet would choose a member of the scientific advisory board of IBA (a proton manufacturer) to write an editorial about protons.
The author of an important commentary should not have such an intrinsic conflict of interest with the subject matter.

📢Thoughtful discussion of the utility of #protontherapy
"[...] importance of integrating patient-reported outcomes into trial design and focusing on endpoints that matter most to long-term survivors. The goal is [...] thoughtful selection of patients"
thelancet.com/journals/lance…
2
7
43
5,705
Devraj Basu, MD, PhD, FACS retweeted

Now published: New study on the controversial role of confirmatory HPV testing in p16 OPCs 📚
Corresponding author: @BasuLab1
Read more: ascopubs.org/doi/10.1200/PO-… link in our bio 🔗
#AcademicMedicine #Research #HPV #headandneckcancer

1
6
9
989
Devraj Basu, MD, PhD, FACS retweeted

📢Thoughtful discussion of the utility of #protontherapy
"[...] importance of integrating patient-reported outcomes into trial design and focusing on endpoints that matter most to long-term survivors. The goal is [...] thoughtful selection of patients"
thelancet.com/journals/lance…
1
3
6,451
Devraj Basu, MD, PhD, FACS retweeted
Mar 21
Come for the critically important data on protons for oropharyngeal cancer, stay for the beautifully written paper.
TORPEdO is out, and it is fascinating and instructive.
I will warn you upfront that this is a long thread, but there is a lot here to discuss!
thelancet.com/journals/lance…
14
40
114
11,863
Devraj Basu, MD, PhD, FACS retweeted

Mar 21
Background: We cure most locally advanced OPSCC patients with IMRT cisplatin, but late dysphagia, xerostomia, dysgeusia, and weight loss still wreck QoL.
Protons spare OARs beautifully on paper. Does that actually help patients?
TORPEdO was built to answer exactly that.
1
1
8
1,596
Our new study on the controversial role of confirmatory HPV testing in p16 OPCs found 6% RNAScope false negatives but no true negatives, supporting only selective, CAP guideline-based use of confirmatory tests when pre-test probability of HPV-relatedness is high. ascopubs.org/doi/10.1200/PO-…
5
359
Devraj Basu, MD, PhD, FACS retweeted
Jan 19
@Jdcramer has made a critical point below about KEYNOTE-689.
The EFS rules in KN-689 require careful review to interpret these results. A protocol-specific event was determined by blind independent central review (BICR), but if growth in the pre-surgical CT was perceived to be a “flare” (i.e. potential progression), surgery was supposed to proceed unless unresectable (protocol quote below). In order to be considered an event, repeat imaging was required 4-8 weeks later, and obviously if the tumor was still resectable the patient would go to surgery before then.
This definition means it was extremely difficult to have an event before surgery, even if the tumor grew and the surgery was more extensive than initially anticipated. Thus some patients may have been harmed by neoadjuvant treatment, but we would not see that in the event data.
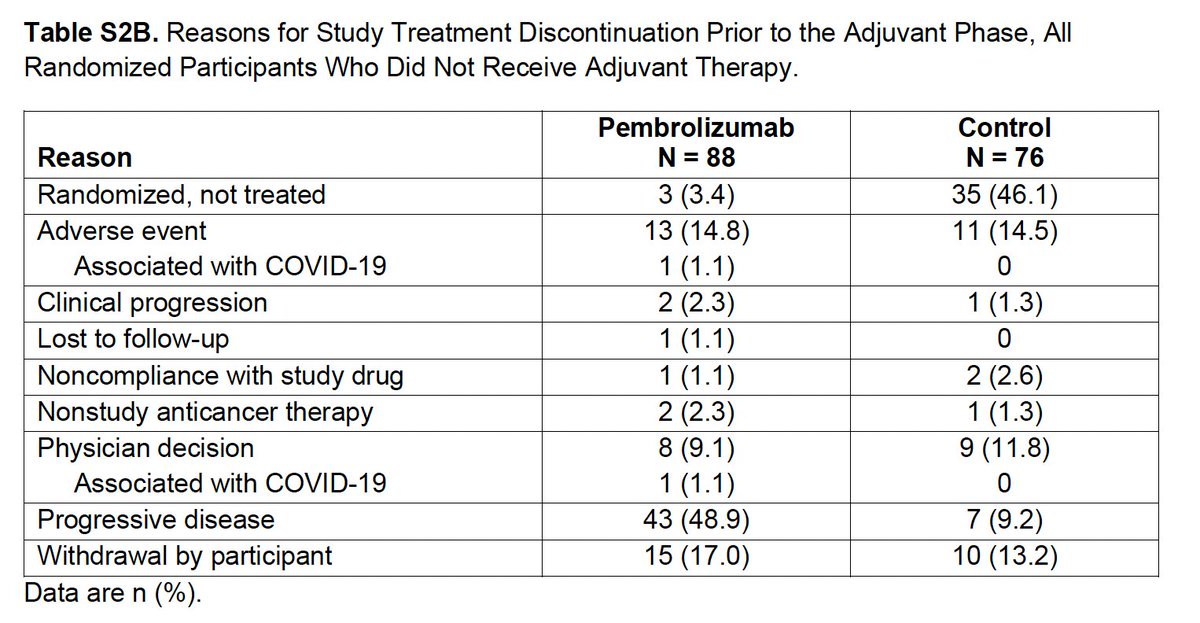
Thus there is this important disconnect: 82 patients in the pembro arm stopped the drug due to progression (by the investigator, as shown in the CONSORT diagram), even though there were only 69 progression events (by BICR, used for endpoint analyses).
Is perioperative immunotherapy doing something favorable and important in a subset of these patients? Yes, and hopefully we can refine its use to the right population and with the right regimen (adding neoadjuvant chemo or RT?).
Is it distinctly possible/probable that some patients are progressing on neoadjuvant pembro, leading to a worse outcome in some domain, but we cannot see that in these data? Yes, unfortunately, also true.

Jan 17

Question for those who’ve dug into KEYNOTE-689:
If 43 pts had early ‘clinical progression’ (Table S2B), why isn’t there an early drop in EFS with neoadjuvant pembro?
How do you reconcile this?
3
11
28
7,732
Devraj Basu, MD, PhD, FACS retweeted

Mar 2
What REALLY makes a good oncologist? in @JCO_ASCO
After 10 years and 203 JCO essays, one thing became clear: expertise alone isn’t enough.
Patient-centered care.
Clear, authentic communication.
Emotional intelligence.
And the harder work
Showing up again and again.
Openness to uncertainty.
Carrying the burden of cancer care.
Continuous growth.
Clinical competence is expected
Human connection makes the difference.
Science treats disease.
Presence treats fear.
ascopubs.org/doi/pdf/10.1200… @OncoAlert
5
88
260
23,307
Devraj Basu, MD, PhD, FACS retweeted

Feb 26
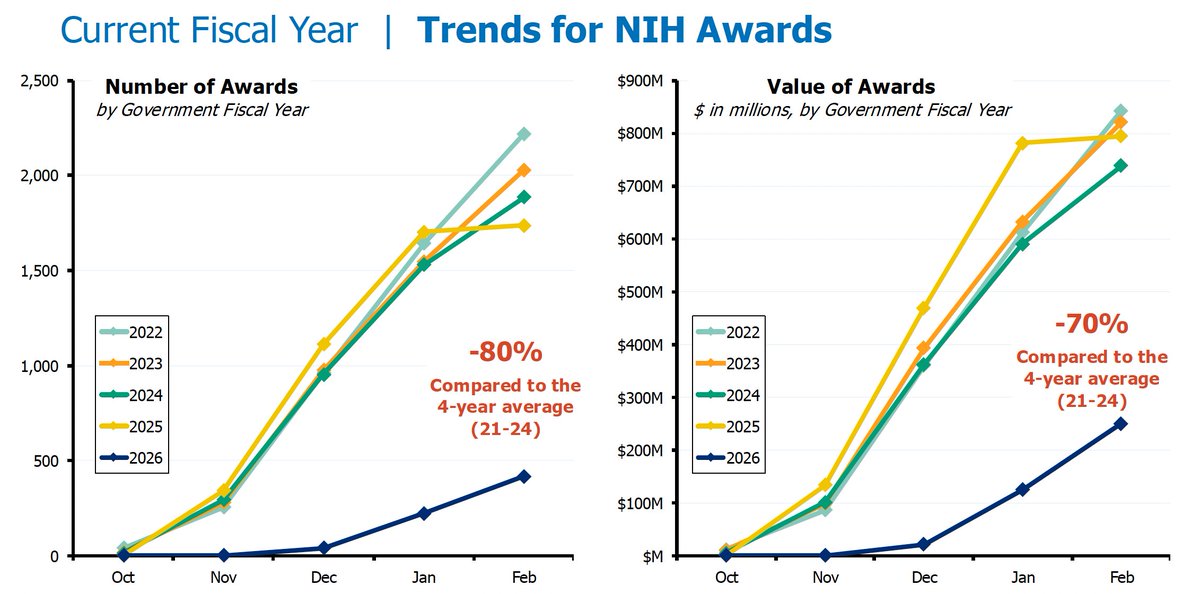
Federal funding for US biomedical research is moribund.
Since October 1 2025, NIH is -80% in new grants and -70% in values (total dollars).
Labs are closing down and researchers are leaving science.
To what end?
40
338
728
178,526
Devraj Basu, MD, PhD, FACS retweeted

At long last, the surgical outcomes from KN671! Some very useful and informative data within this manuscript:
annalsthoracicsurgery.org/ar…
6
20
2,437
It was a privilege to present today at the 9th annual DDR Summit in Boston , representing the @PennCancer
team advancing translational science and clinical trials for HPV head and neck cancer @DiabLabPenn @DrNickLukens @LovaSunMD



2
1
3
263
Devraj Basu, MD, PhD, FACS retweeted

Jan 2
Two papers in @NatureCancer highlighting the role of intratumoral bacteria & associated immune architecture (e.g., neutrophil influx) in mediating resistance to immunotherapy in head & neck cancer.
nature.com/articles/s43018-0…
nature.com/articles/s43018-0…
@GeneCollector @xrtGenomics
6
42
185
30,697

Devraj Basu, MD, PhD, FACS retweeted
24 Oct 2025
The field is understandably desperate to improve outcomes in this high-risk population of HPV-negative HNSCC.
However, we also have to be cautious in interpreting phase II studies. This sub-100 patient trial led to a truly immense amount of additional work (and money) that ultimately led nowhere.
Sometimes, that will happen, despite the best intentions (as in this case). A few final thoughts:
1. Choose endpoints wisely, and make them meaningful for clinical inference and the follow-up trial. It is atypical to use alive with locoregional control (with a chi-squared test) as a primary endpoint, especially for a systemic drug with a variety of other activities (good or bad).
2. Power the study with sufficient numbers to ask the relevant question. It was quite small, with baseline imbalances in a critical clinical characteristics, with unfortunate, random deaths further compromising interpretation. Smaller trials are cheaper and faster (and the preference for efficiency is understandable), but they can lead to this exact scenario.
3. When transitioning from a phase II to III, don’t change the experimental arm unless there are real data supporting it. I doubt the addition of the 3 extra cycles did anything – the study was bound to be negative – but there was no reason to do it, and patients may have been hurt if it increased the metastatic potential of the tumor.
4. Ensure there are safety guardrails. The interim analysis was performed after 65% of total events. Many trials use 50%, and that would have saved time (and maybe patient enrollment) here. Given the small phase II study, the group should have looked at the results sooner, before enrolling 700 patients.
5. I deeply share the impatience with wanting to improve outcomes, but more caution is needed in interpreting phase II outcomes, especially when there are intrinsic limitations to the study itself.
6. It is an imperative to deploy more creative phase II (and phase III) designs to more quickly and accurately identify novel, successful therapies.
1
6
20
1,565
Devraj Basu, MD, PhD, FACS retweeted
23 Oct 2025
The optimal management of oligometastatic HNSCC is a debated and important question. How can we improve *overall survival* in this more favorable population?
EA3211 is a phase III randomized trial studying this exact issue.
Enrollment is even more streamlined with the most recently activated amendment:
- Patients may be enrolled 3 months after completing the first course of radiotherapy
- Patients may be enrolled after starting a compliant chemoimmunotherapy regimen (chemo dose prior to enrollment at discretion of physician)
- Timelines for imaging more flexible given logistical challenges of work-up
Please contact me with any questions! We are always looking to expand enrollment!
22 Oct 2025

#ClinicalTrial EA3211, led by @DavidSherMD of @utswcancer, aims to improve results for patients with #HeadAndNeckCancer that has spread to a limited number of places. Learn more: bit.ly/ea3211-study
10
35
3,682
Devraj Basu, MD, PhD, FACS retweeted

13 Oct 2025
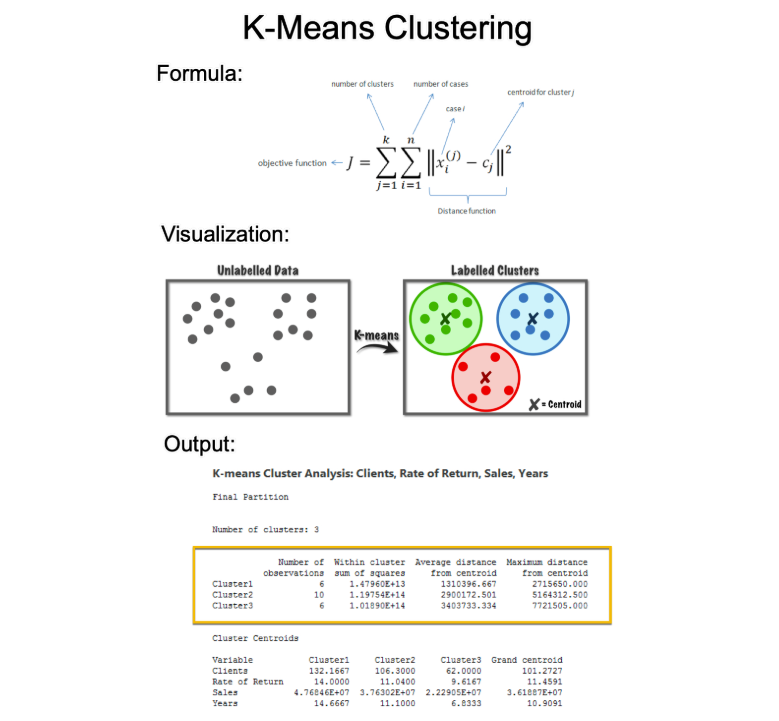
K-means is one of the most powerful algorithms for data scientists.
But it's confusing for beginners. Let's fix that:
7
88
638
29,789