
Jun 11
For clinicians..........
Maintain a high index of suspicion for pancreatic cancer in patients >50–60 with new-onset diabetes (especially if accompanied by unexplained weight loss, abdominal/back pain, or steatorrhea), as ~1% of such cases may represent paraneoplastic diabetes from an occult tumor.
Prompt cross-sectional imaging (pancreatic-protocol CT or MRI) is warranted in these scenarios rather than attributing symptoms solely to type 2 diabetes. Refer high-risk individuals (strong family history or germline mutations in BRCA2, PALB2, ATM, CDKN2A, etc.) to multidisciplinary centers for surveillance with alternating MRI/MRCP and EUS, typically starting at age 50 (or 10 years before earliest family diagnosis).
Early detection can dramatically improve resectability and 5-year survival. Also, consider germline genetic testing in all diagnosed pancreatic cancer patients per NCCN guidelines.
Raising awareness of these red flags in primary care could shift more cases from stage IV to earlier, actionable stages.
1
239

Jun 9
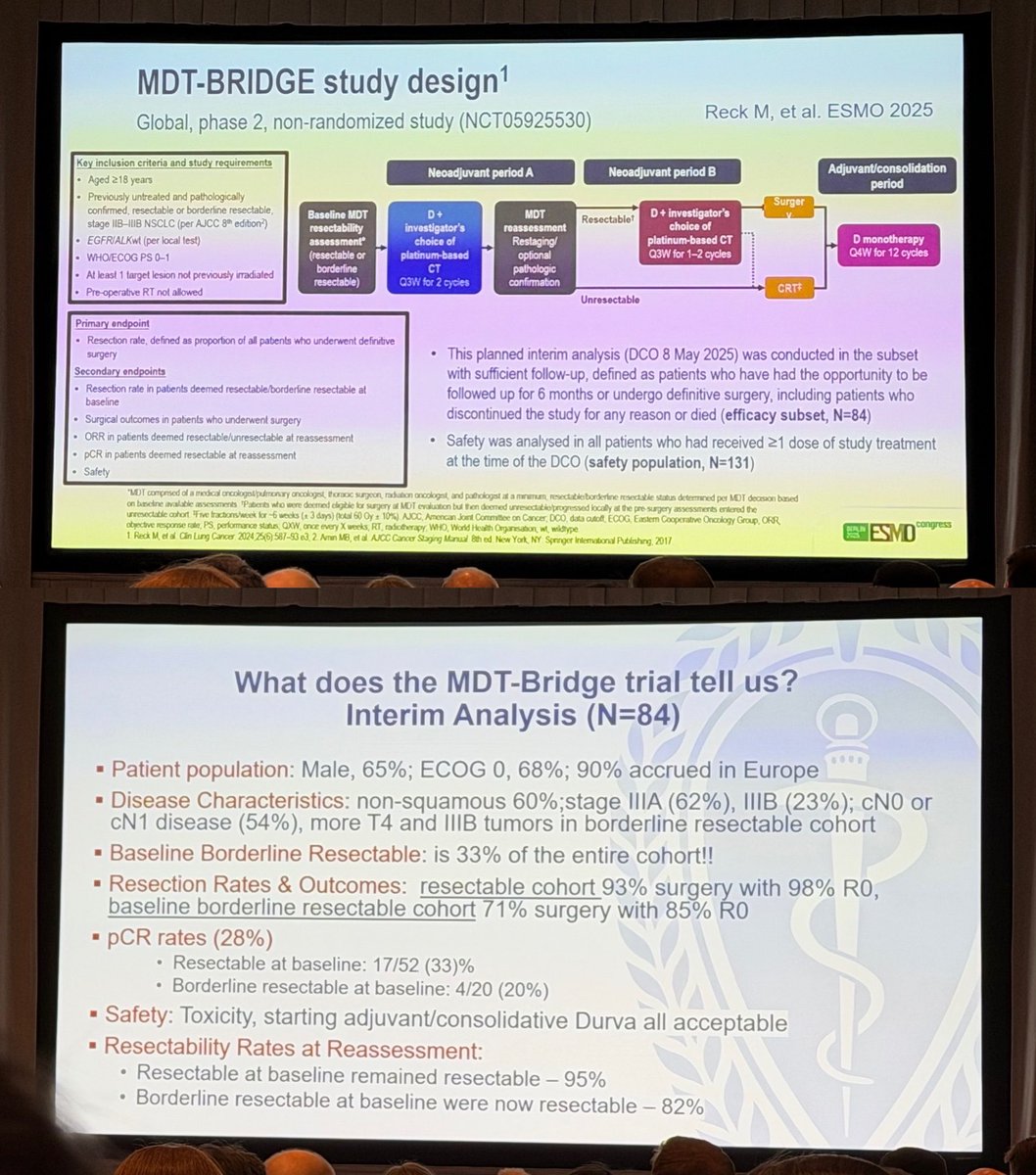
@DoctorJSpicer presenting one of
the hottest topics this year MDT-bridge ... exploring and transforming borderline resectability !

1
12

Stage III Non-small Cell Lung Cancer
Resectability in a Country With Limited
Diagnostic and Therapeutic Resources: A
Colombian Expert Consensus journals.sagepub.com/doi/10.… ❤️🔥❤️🔥❤️🔥
3
99

If we were simply copying protocols, why would Indian MDTs spend hours arguing over borderline resectability, resource constraints, nutrition, compliance, social factors, and follow-up logistics?
1
24

May 30
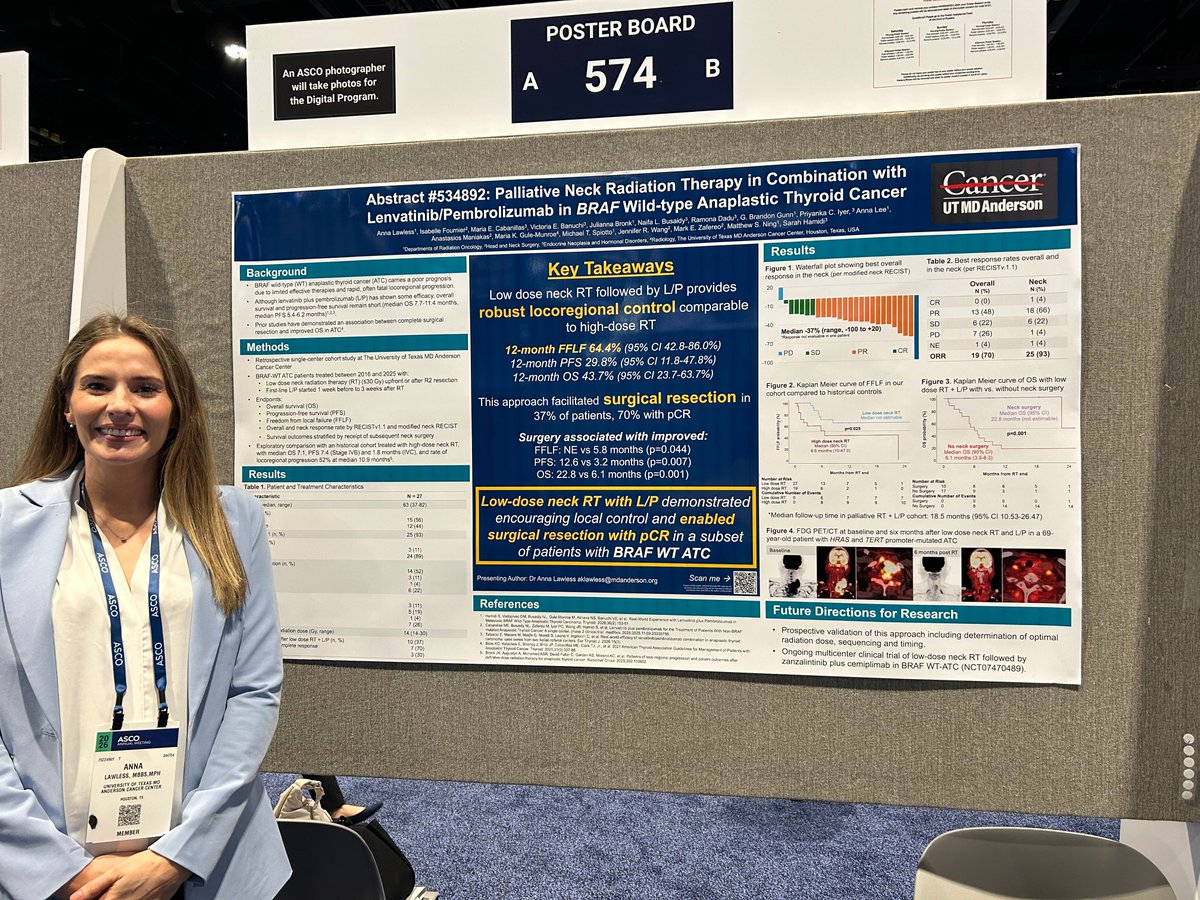
Combining palliative neck radiation with lenvatinib and pembrolizumab may improve outcomes for patients with BRAF wild-type anaplastic thyroid cancer.
At #ASCO26, Dr. Anna Lawless presented research showing this approach was associated with improved surgical resectability, durable locoregional control, and encouraging survival outcomes among patients who proceeded to surgery. #EndCancer 3/5
ALT Dr. Anna Lawless
1
4
7
555

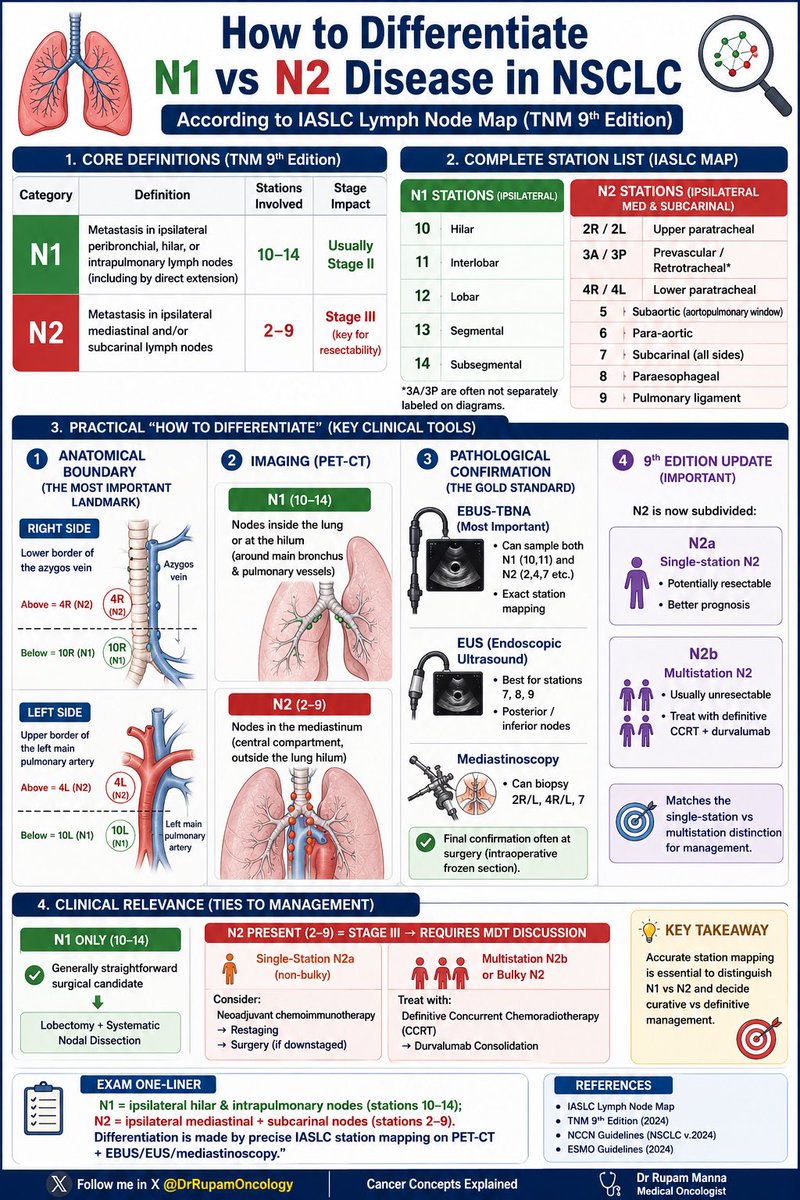
🔥 How to Differentiate N1 vs N2 Disease in NSCLC
(IASLC Lymph Node Map – TNM 9th Edition)
The #1 decision that decides resectability & treatment in Stage III lung cancer!
✅ N1 (stations 10–14) = ipsilateral hilar & intrapulmonary nodes → Usually straightforward surgery
✅ N2 (stations 2–9) = ipsilateral mediastinal subcarinal nodes → Stage III, needs MDT
✅ Crystal-clear anatomical boundaries (Azygos vein on right, left main PA on left)
✅ Brand new 9th edition: N2a (single-station) vs N2b (multistation)
✅ Practical tools: PET-CT → EBUS-TBNA → Mediastinoscopy
Perfect quick reference for DM/DNB Oncology residents, thoracic surgeons, medical oncologists & pulmonologists!
✅ 100% accurate as per IASLC TNM 9th Edition & latest NCCN/ESMO guidelines
Full infographic below 👇
#NSCLC #LungCancer #N1vsN2 #LungCancerStaging #IASLC #StageIII #Oncology #MedTwitter #MedEd #CancerConceptsExplained
Follow @DrRupamOncology for more simplified oncology visuals!
25
73
2,358
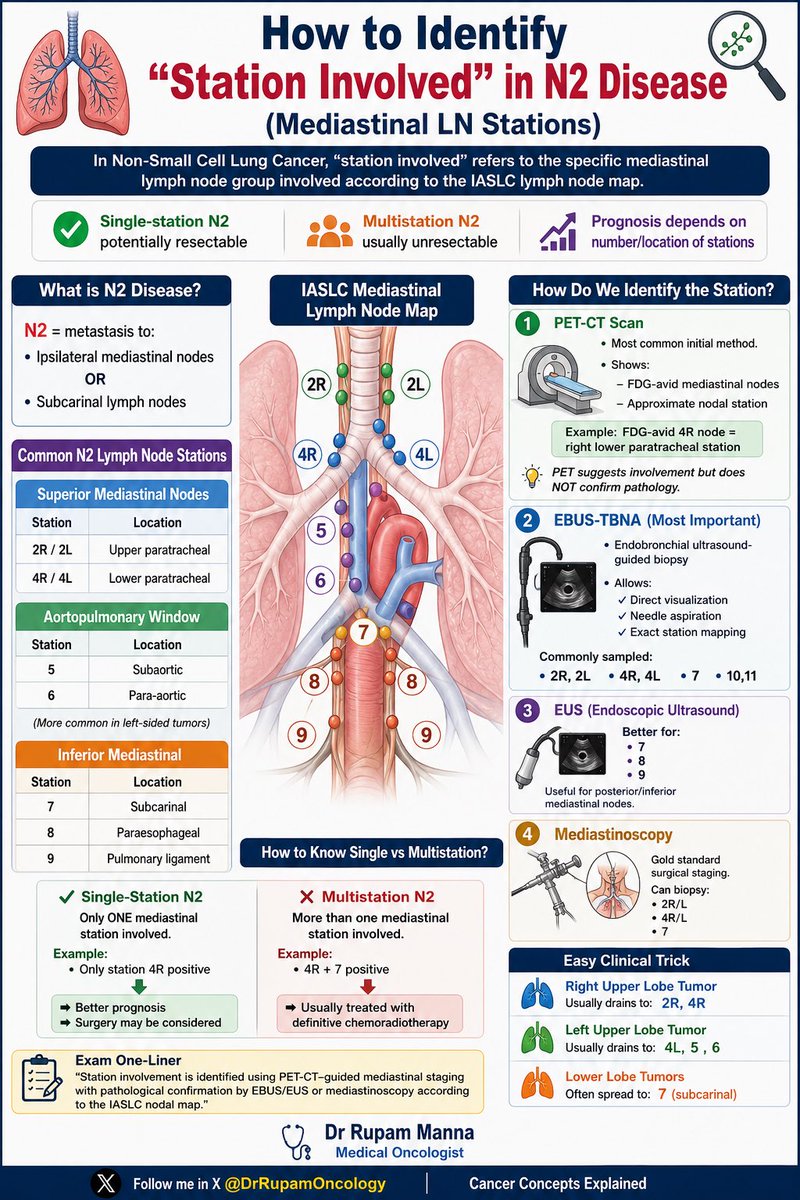
🔥 How to Identify “Station Involved” in N2 Disease
(Mediastinal LN Stations in NSCLC)
The #1 factor that decides resectability & treatment in stage III lung cancer!
✅ Single-station N2 → Potentially resectable (better prognosis)
✅ Multistation N2 → Usually definitive chemoradiotherapy
✅ Full IASLC lymph node map (2R/2L, 4R/4L, 5, 6, 7, 8, 9)
✅ Stepwise staging: PET-CT → EBUS-TBNA (most important) → EUS → Mediastinoscopy
✅ Easy clinical tricks by lobe drainage patterns
Essential quick reference for DM/DNB Oncology residents, thoracic surgeons, medical oncologists & pulmonologists!
✅ Fully accurate as per latest IASLC / NCCN / ESMO guidelines
Full infographic below 👇
#NSCLC #LungCancer #N2Disease #MediastinalStaging #LungCancerStaging #Oncology #MedTwitter #MedEd #CancerConceptsExplained
Follow @DrRupamOncology for more simplified oncology visuals!
11
39
1,320

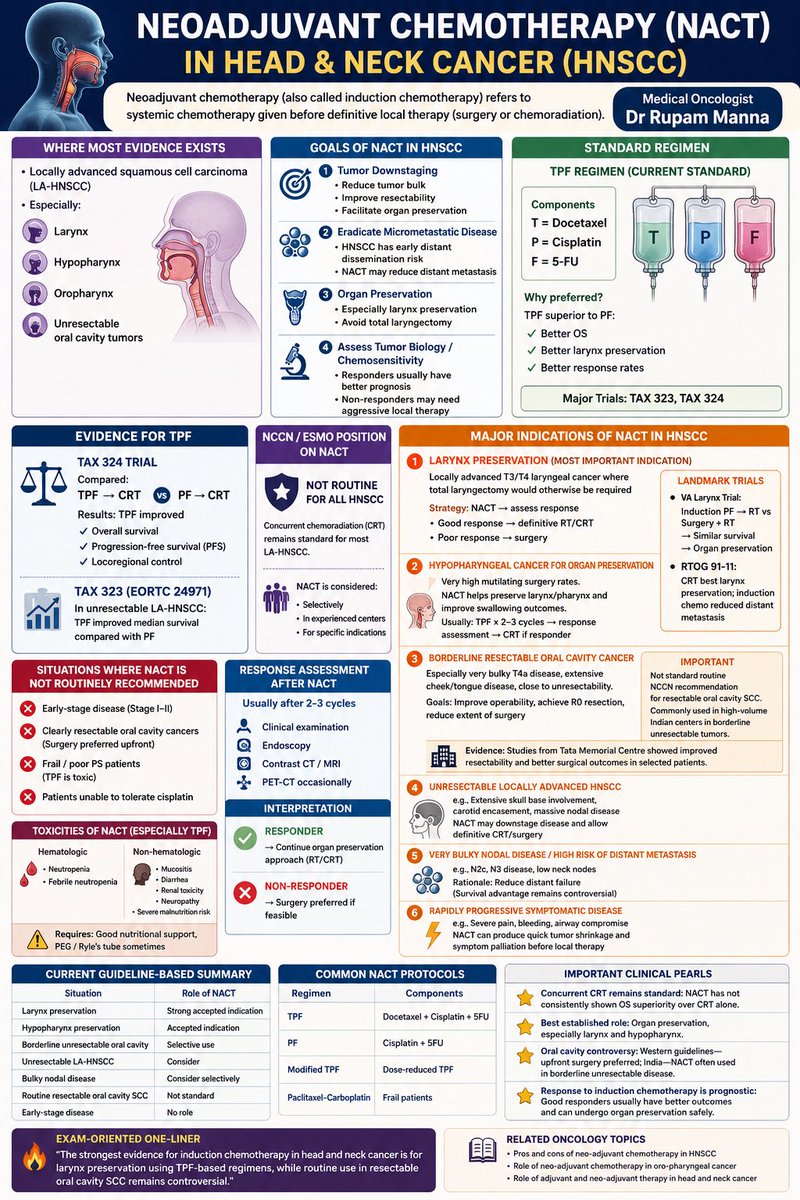
🔶 Neoadjuvant Chemotherapy (NACT) in Head & Neck Cancer (HNSCC)
TPF-based induction chemotherapy has its strongest evidence in organ preservation — especially in laryngeal and hypopharyngeal cancers. While concurrent chemoradiation remains the standard for most LA-HNSCC, selective use of NACT can improve resectability, preserve function, and reduce distant failure in carefully chosen patients.
📘 Key takeaways:
✔️ Best established role → Larynx preservation
✔️ TPF superior to PF (TAX 323 / TAX 324)
✔️ Useful in borderline unresectable oral cavity cancers
✔️ Response assessment after 2–3 cycles is crucial
✔️ Not routine for all resectable oral cavity SCC
— Dr Rupam Manna
#HeadNeckCancer #HNSCC #NACT #InductionChemotherapy #MedicalOncology #Oncology #LarynxCancer #Hypopharynx #OralCancer #TPF #CancerEducation #OncologyLearning #RadiationOncology #SurgicalOncology #CancerMedicine #DrRupamManna
6
17
903

May 6
Oncological Outcomes and Treatment Strategies for Borderline Resectable #Hepatocellular #Carcinoma Based on the Oncological Resectability Classification #some4surgery karger.com/lic/article/doi/1…
1
1
4
77

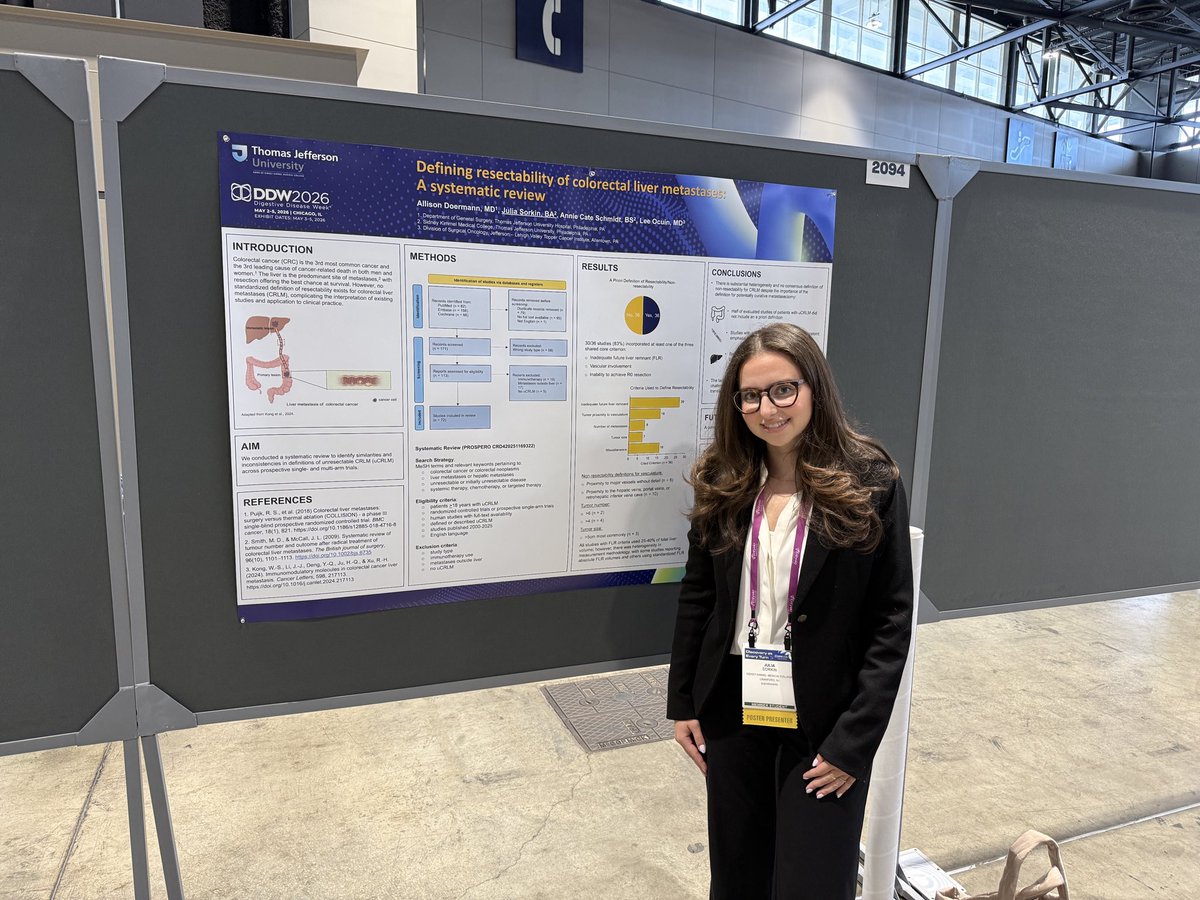
Great last day @DDWMeeting #DDW2026. Our talented M3 Julia Sorkin @JeffersonUniv presenting our systematic review of trials for unresectable colorectal metastases, showing the lack of a uniform definition of non-resectability. @SSATNews @LVHN @TJUHospital @JEFFsurgery
2
21
1,468

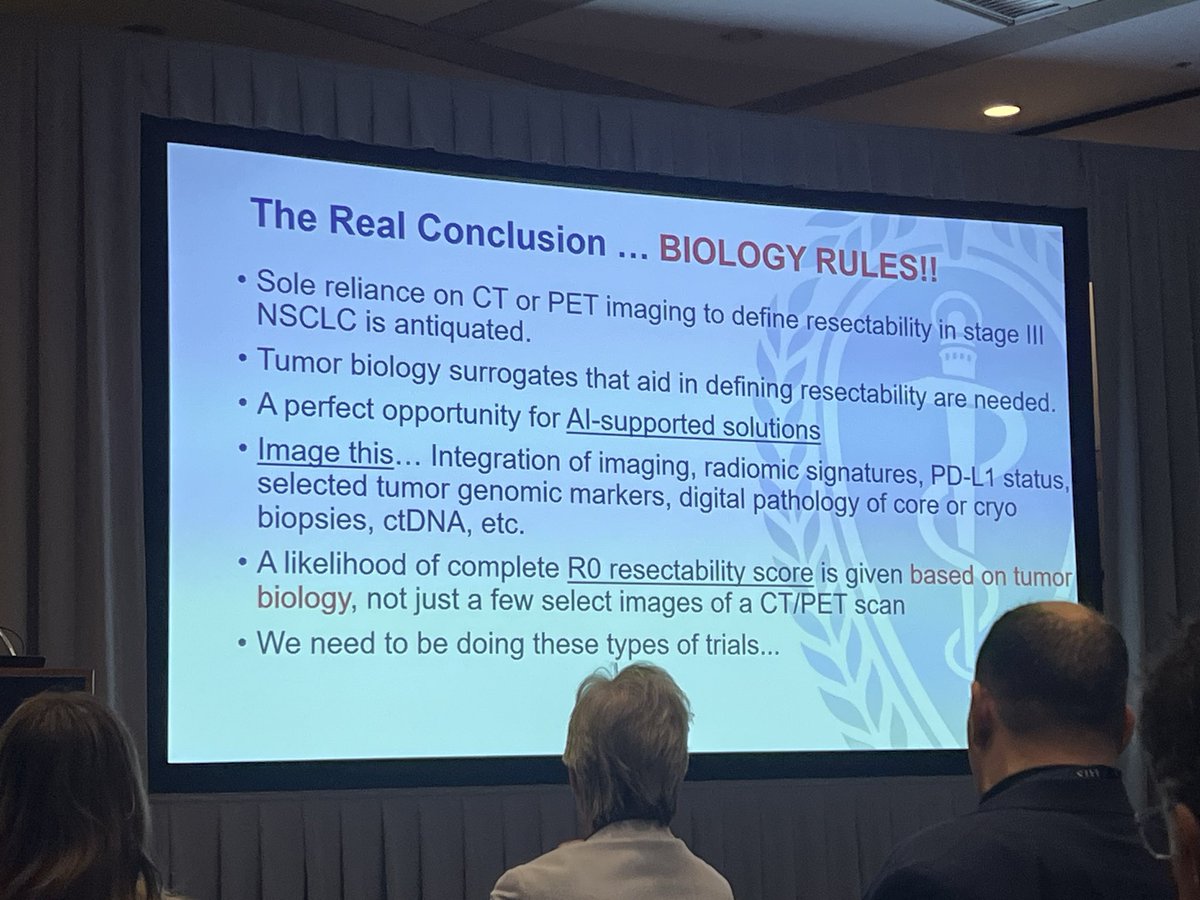
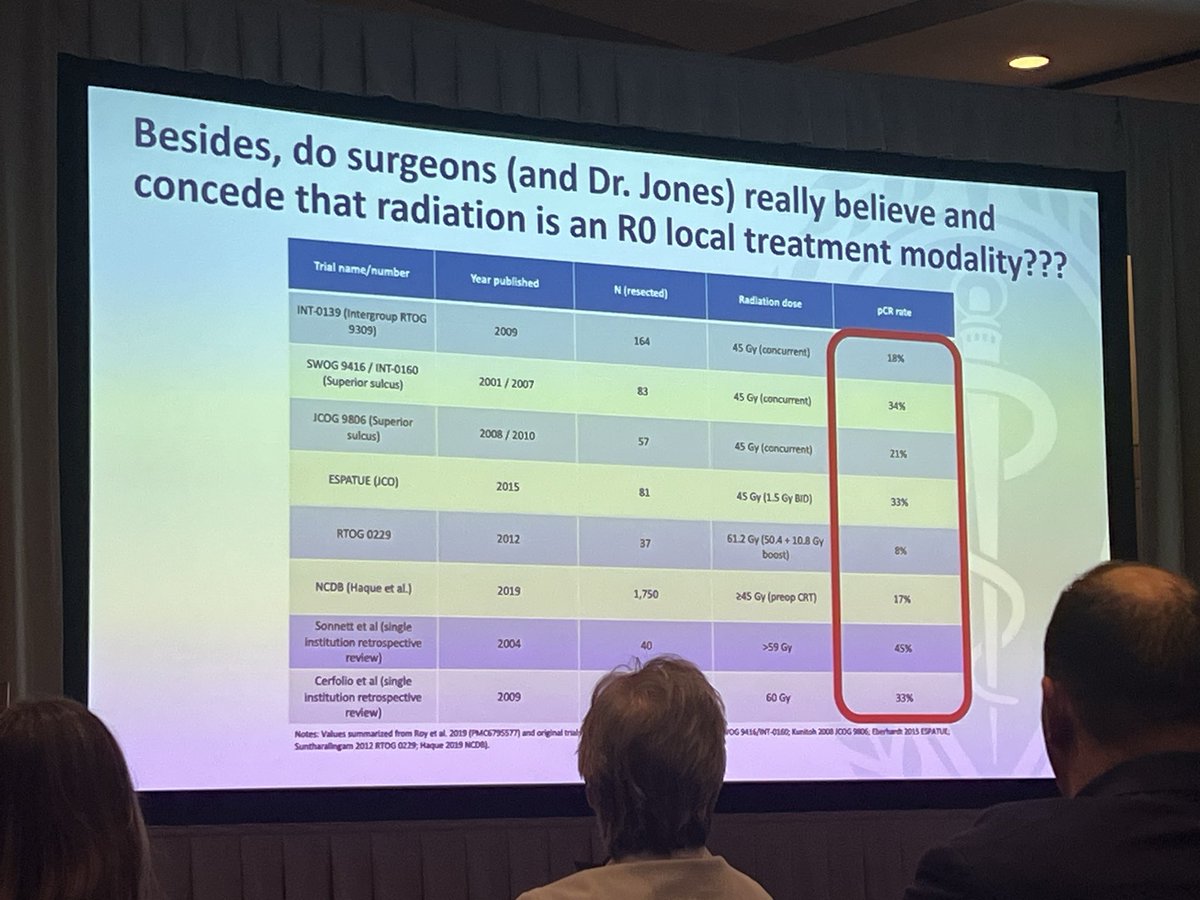
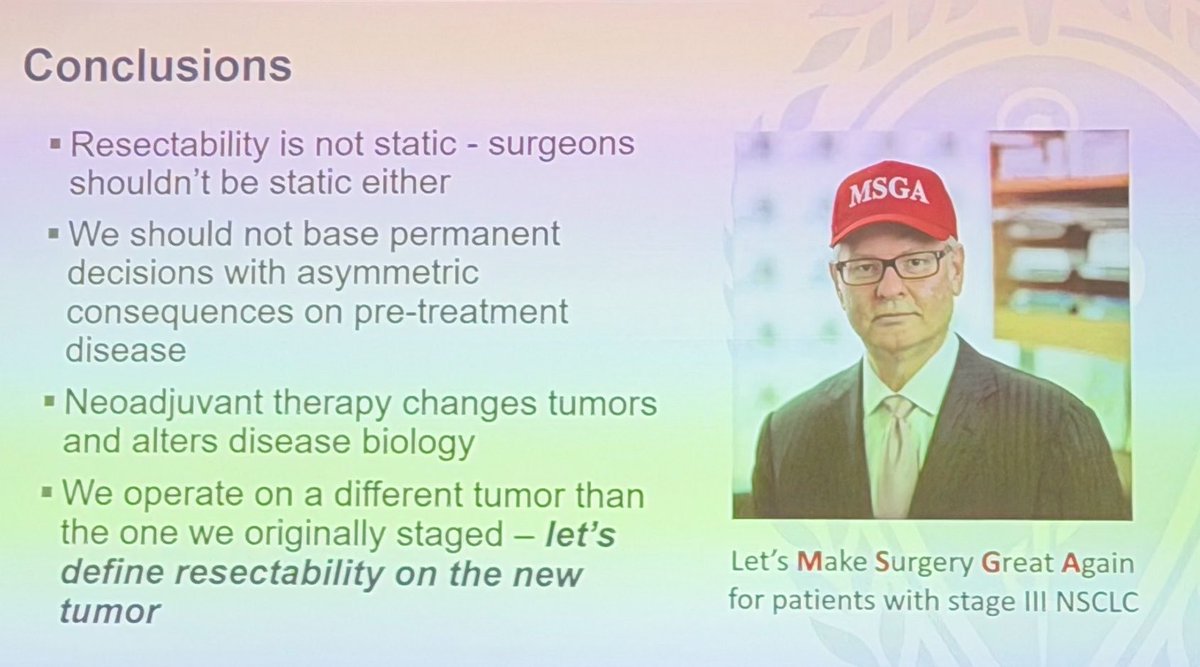
The debate if resectability should be decided prior to induction therapy btwn @JonesDavid2013 and @BrendonStilesMD did not disappoint!!
More agreement than debate w take aways:
-biology rules
-surgery is best local control
-give best systemic therapy 1st then eval for resection


1
10
27
1,783

Lively “debate” to close out #AATS2026 Thoracic Sessions between Dr. Jones and @BrendonStilesMD about Should Resectability be Determined Prior to Induction? @AATSHQ @MSK_Thoracic @MontefioreCTS
Consensus?
- “It’s in the eye of the beholder”
- “Make surgery great again”
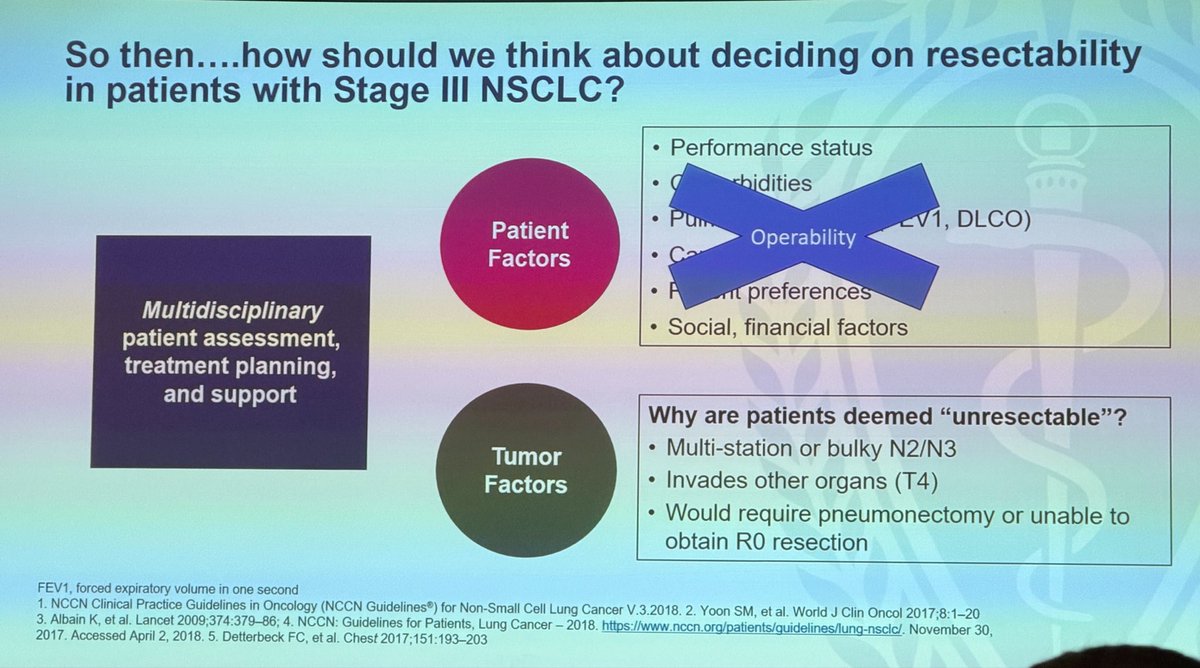
- Definition of resectability is variable
- MDT-BRIDGE and other trials are needed to answer these questions

1
3
205

Bring the popcorn Saturday @AATSHQ as I debate the (almost) undebatable @JonesDavid2013 on when resectability should be decided - how can I possibly beat this giant and convince the crowd that it is ok to decide resectability AFTER giving our best systemic therapy? #AATS2026
6
7
29
4,712

#LiverCancer
▶️Significance of Evaluating Tumor Markers in the Oncological Criteria for Resectability in Hepatocellular Carcinoma
👉doi.org/10.1111/hepr.70096
#LiverX @WileyHealth
5
116

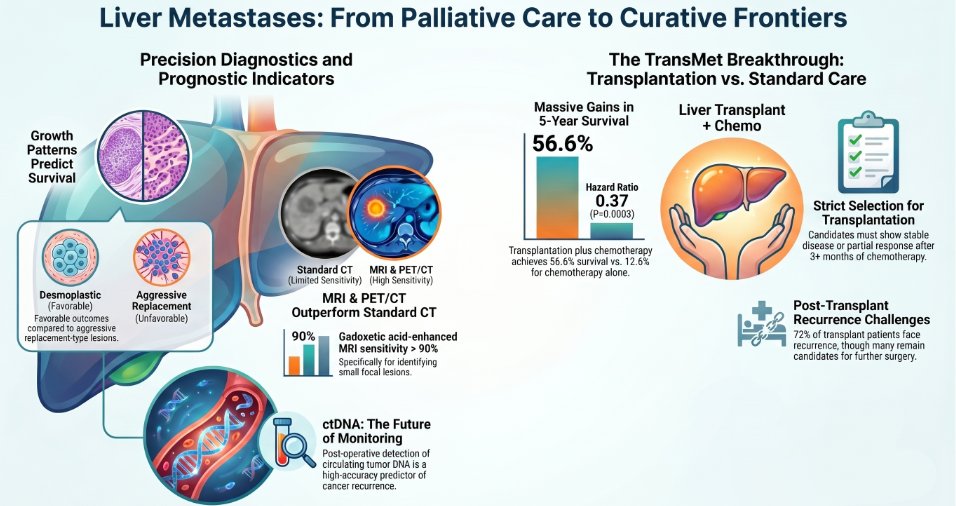
🚨 Liver transplant in metastatic CRC? From taboo to therapeutic frontierA new review (Cancer Treat Rev) reframes transplant oncology for unresectable colorectal liver metastases 👇
🔬 Key insights:
• Liver-only mCRC → historically poor prognosis without resection
• TransMet data show a clear survival advantage with transplantation in highly selected patients
• Patient selection = everything (biology > burden)
• Peri-transplant strategies integrate systemic therapy surveillance🧬 Where it gets disruptive:
• ctDNA emerges as a tool for:
– risk stratification
– minimal residual disease detection
– post-transplant monitoring
⚖️ Unresolved challenges:
• Organ allocation ethics
• Recurrence risk under immunosuppression
• Defining who truly benefits
💡 Medical Watch take:
This is not just a surgical advance…
👉 it’s the rise of transplant oncology as precision oncologyAre we ready to select patients for transplant based on biology, not resectability? 👀🔗
@CathyEngMD @BRicciutiMD @g_mountzios @matteolambe @hoperugo @stolaney1
doi.org/10.1016/j.ctrv.2026.… #LiverMetastases #TransplantOncology #ctDNA #PrecisionOncology #OncoTwitter #MedicalWatch
3
3
5
438

Apr 23
Type A Thymoma (with emphasis on morphology and differential diagnosis) 🫁🔬
Among thymic epithelial tumors, type A thymoma is one of the most distinctive and usually one of the most indolent subtypes. It is composed of neoplastic epithelial cells with a spindle/oval morphology and contains very few immature T lymphocytes, which helps separate it from more lymphocyte-rich thymomas. In general, it carries an excellent prognosis, although rare atypical/aggressive examples have been described.
Definition 📌
Type A thymoma is a thymic epithelial tumor composed of relatively bland spindle to oval neoplastic epithelial cells, typically arranged in fascicles, storiform areas, or sheets, with minimal to absent nuclear atypia and a paucity of non-neoplastic immature thymocytes. It is recognized as a distinct WHO subtype within thymomas.
Epidemiology 📊
Thymomas are rare tumors of the anterior mediastinum, usually occurring in adults. Type A thymoma represents a minority of thymomas and is generally considered a low-risk histologic subtype compared with B2/B3 thymomas and thymic carcinoma. Thymic epithelial tumors overall may be associated with myasthenia gravis and other autoimmune/paraneoplastic disorders, although these associations are less prominent in type A thymoma than in some other subtypes.
Sites 📍
The classic site is the anterior (prevascular) mediastinum. Imaging-pathology reviews of thymic epithelial neoplasms consistently place thymomas in this compartment, where they enter the differential diagnosis of anterior mediastinal masses.
Pathogenesis 🧬
At the molecular level, thymic epithelial tumors show heterogeneous alterations. A well-known association in thymomas, particularly indolent forms, is mutation in GTF2I (TFII-I), which has been linked to more favorable biology in thymic epithelial tumors. Molecular testing is not routinely required for the diagnosis of conventional type A thymoma, but it supports the concept that this subtype belongs to the more indolent end of the thymoma spectrum.
Clinical Features 🩺
Patients may be asymptomatic, with incidental detection on imaging, or may present with symptoms related to mass effect, such as chest discomfort, cough, or dyspnea. As with thymomas in general, clinical outcome depends strongly on stage and completeness of resection.
Laboratory Diagnosis 🧪
The diagnosis is primarily histopathologic, often supported by imaging and, when needed, immunohistochemistry. In limited biopsy material, the main challenge is distinguishing type A thymoma from other spindle cell anterior mediastinal lesions, including metaplastic thymoma, spindle cell thymic carcinoma, and mesenchymal neoplasms.
Histopathology 🔍
• Tumor composed of spindle to oval epithelial cells with bland cytology.
• Cells often arranged in fascicles, whorls, storiform areas, or sheets.
• Very few immature lymphocytes in the background.
• Perivascular spaces may be present, supporting thymoma.
• Nuclear atypia is usually minimal; brisk mitotic activity and necrosis are not typical in conventional type A thymoma.
• Rare reports describe atypical type A thymoma with hypercellularity, increased mitoses, and/or necrosis, features that may correlate with less indolent behavior.
Immunohistochemistry 🧫
• Positive: pancytokeratins, CK19 and broad epithelial markers, confirming epithelial nature.
• p63/p40: may be variable and usually less diagnostically central than in squamoid lesions.
• TdT: typically highlights only scattered residual immature thymocytes, if present.
• CD5/CD117: usually not expressed by the neoplastic epithelial cells, helping in the differential diagnosis with thymic carcinoma.
Differential Diagnosis ⚖️
• Metaplastic thymoma – also spindle-predominant, but typically biphasic, with epithelial and stromal components.
• Spindle cell thymic carcinoma – usually shows more overt cytologic atypia and more aggressive behavior; CD5/CD117 may support carcinoma.
• Solitary fibrous tumor – mesenchymal tumor; keratin negativity and STAT6 positivity favor SFT.
• Synovial sarcoma – can arise in mediastinum and mimic spindle lesions; molecular confirmation may be needed.
• Peripheral nerve sheath tumor – S100/SOX10 profile and lack of epithelial marker expression help separate it.
• Type AB thymoma – shares spindle areas but shows conspicuous lymphocyte-rich areas admixed with type A-like regions.
Prognosis 📈
Conventional type A thymoma is generally associated with an excellent prognosis, especially when completely resected and confined to the thymus. Across recent reviews and outcome series, thymoma prognosis remains driven mainly by stage and resection status, but type A histology belongs to the most favorable end of the spectrum. Rare atypical type A thymomas may behave more aggressively than conventional examples.
Treatment 💉
The cornerstone of management is complete surgical resection whenever feasible. Additional therapy depends mainly on tumor stage, local invasion, and resectability. Thymomas are managed differently from thymic carcinomas, and systemic therapy is generally reserved for unresectable, recurrent, or advanced cases.
Take-Home Messages @Notas_Patologia 📚
• Type A thymoma is a bland spindle/oval epithelial thymoma with very few immature lymphocytes.
• The main histologic clue is the combination of spindle epithelial cells paucity of TdT thymocytes.
• It usually has an excellent prognosis, especially when completely resected.
• The key differentials are other spindle cell anterior mediastinal tumors.
• Rare atypical type A thymomas with necrosis or increased mitotic activity deserve extra caution.
Selected References 📖
• WHO Classification of Thoracic Tumours, 5th edition.
• Recent narrative reviews on thymic epithelial tumors and management.
• Reviews on thymoma biology and GTF2I/TFII-I.
• Recent reports on atypical type A thymoma.
Disclaimer⚠️
This text is an educational summary for healthcare professionals and students. It does not replace full pathology reports, local guidelines, or individualized clinical decision-making.
Hashtags
#MedicalEducation #NotasDePatologia #pathology #PathTwitter #ThoracicPathology #MediastinalPathology #Thymoma

4
9
545

Apr 23
Infantile Osteosarcoma (IOS), a rare and very aggressive bone cancer that develops in children, adolescents, and young adults. It is caused by deletions of chromosome 13q14 that inactivate the retinoblastoma gene associated with high risk of OS. OS is may be associated with Paget disease and fibrous dysplasia. There is a higher incidence of OS in Li-Fraumeni syndrome (germline TP53 inactivation); hereditary retinoblastoma (germline RB1 inactivation); Rothmund-Thompson syndrome (germline RECQLA inactivation); and Bloom and Werner syndromes (germlines BLM and WRN inactivations respectively, which encode proteins necessary to stabilize the genome. OS occurs very rarely on the hands as it has a predeliction for metaphyseal regions of long bones like distal femur, proximal tibia and humerus, around the knees, shoulders, ribs, pelvis, and mandible.
The X-ray of the hand shows a well-circumscribed large lesion with cortical destruction on metacarpals and phalanges with a "moth-Eaten" appearance, and "ballooning" effect with calcifications. There is an osteoid matrix with fluffy "cloud-like" appearance of the tumor. IOS presents with periosteal pain that worsens at night, with large localized palpable swelling with limited joint motion, and sudden fractures. OS has the possibility to metastasize to the lungs. Ddx. Enchondroma, fibrous dysplasia, chondrosarcoma, osteoblastoma, Ewing sarcoma, giant cell tumor, aneurysmal bone cysts, and reactive myositis ossificans. Dx. X- ray showing sunburst appearance, Codman sign with soft tissue mass; CT-scan, and MRI; biopsy with histopathology showing tumor cells with nuclear pleomorphism, less so in cells entrapped in neoplastic bone matrix; chest X-ray, in case of metastasis, showing solitary or multiple round nodules mostly on lower lobes. Lab. tests showing elevated ALP and LDH. Management: limb-salvage surgery that removes as much of the tumor to save the limb. If this isn't feasible, then limb amputation with neoadjuvant and adjuvant combination chemotherapy: high dose methotrexate with leucoverin, cisplatin, adriamycin, ifosfamide and bleomycin; cyclophosphamide and dactinomycin (BCD); etoposide, muramyl tripeptide, and mifamurtide; radiotherapy Targeted therapy with tyrosine kinase inhibitors may also be considered. Prognosis depends on staging, size of tumor, location, whether there is metastasis, resectability, and histopathology of the tumor such as the degree of necrosis of the primary tumor, degree of P-glycoprotein, and whether the tumor is CXCR4-positive or HER2-positive.
2
4
452
Apr 23
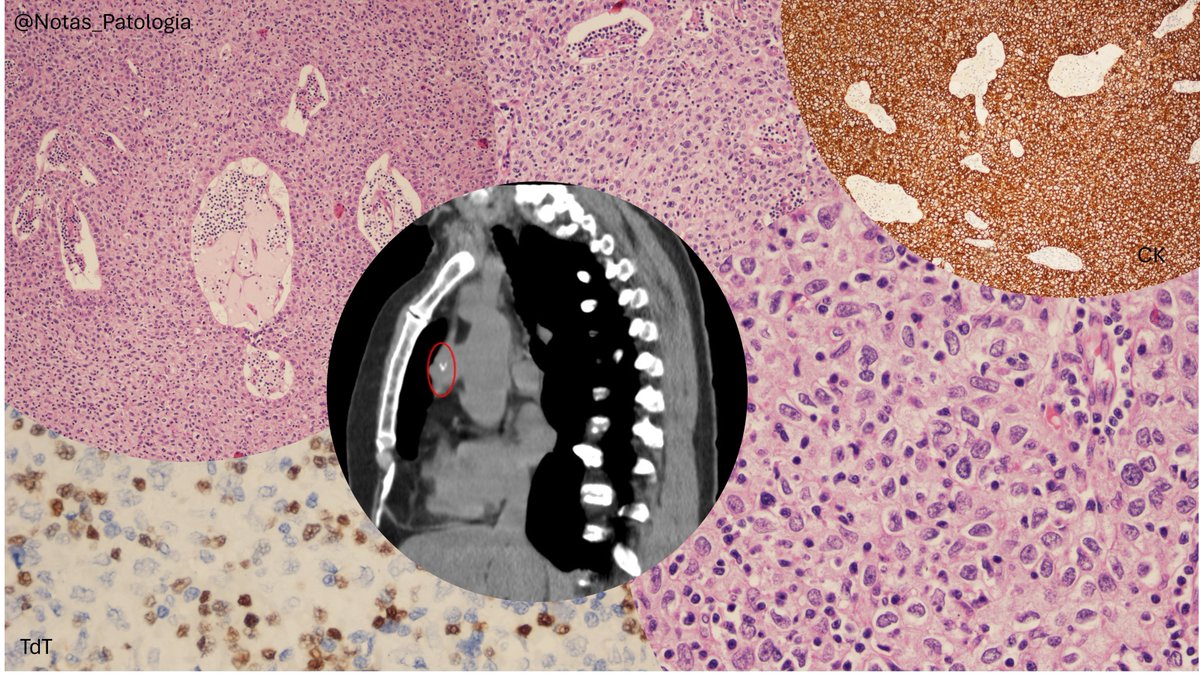
Thymoma B3 (with emphasis on diagnostic pitfalls and differential diagnosis with thymic carcinoma) 🫁🔬
Thymic epithelial neoplasms can be challenging, and B3 thymoma sits exactly in that “gray zone” between lymphocyte-rich thymomas and tumors with a more overtly epithelial appearance. It is an important subtype because it tends to behave more aggressively than A/AB/B1 thymomas and may mimic thymic squamous carcinoma, especially in small biopsies.
Definition 📌
B3 thymoma is a thymic epithelial tumor composed predominantly of polygonal neoplastic epithelial cells, showing mild to moderate atypia, usually with a lobulated growth pattern and a relative paucity of immature lymphocytes, although small clusters of TdT thymocytes may still be present.
Epidemiology 📊
Thymomas are rare tumors of the anterior mediastinum. Within the thymoma spectrum, B2 and B3 subtypes are generally regarded as higher-risk histologic categories than A, AB, and B1. Thymomas as a group may also be associated with myasthenia gravis and other autoimmune disorders.
Sites 📍
The typical location is the anterior (prevascular) mediastinum. More rarely, thymic epithelial tumors may arise in ectopic sites, but the classic setting for B3 thymoma is an anterior mediastinal mass in an adult patient.
Pathogenesis 🧬
The molecular biology of thymic tumors is less “driver-defined” than in many other solid neoplasms. Current reviews suggest that thymoma progression involves alterations in immune regulation, thymic architecture, and, in some cases, less common molecular events, without a single universal driver routinely used in daily diagnostic practice for B3 thymoma.
Clinical Features 🩺
Patients may be asymptomatic, with incidental detection on imaging, or may present with mass effect symptoms such as chest pain, cough, or dyspnea. Paraneoplastic associations, especially myasthenia gravis, are also important. Clinical behavior depends strongly on stage and resectability, more than on histologic subtype alone.
Laboratory Diagnosis 🧪
In small biopsies, the main challenge is not only recognizing a “thymoma,” but specifically distinguishing B3 thymoma from well- or moderately differentiated thymic squamous carcinoma. Integration of morphology, radiologic context, and immunohistochemistry is essential. Limited samples may preclude confident subtyping.
Histopathology 🔍
• Lobulated growth, often with fibrous septa.
• Perivascular spaces are often a useful clue favoring thymoma.
• Predominance of polygonal epithelial cells with eosinophilic cytoplasm and mild to moderate atypia.
• Few immature lymphocytes, usually in small scattered groups.
• A “pseudo-squamoid” appearance may occur, but marked desmoplasia, overt keratinization, and pronounced atypia favor thymic carcinoma.
Immunohistochemistry 🧫
• Positive: pancytokeratins/CKAE1-AE3, p40/p63 (often), and TdT highlighting residual immature thymocytes.
• Negative or typically not expressed in the epithelial tumor cells: CD5 and CD117/c-KIT, unlike what is often seen in thymic carcinoma.
• Notes: the presence of TdT immature thymocytes and the absence of CD5/CD117 in epithelial cells are very helpful in the differential diagnosis with thymic squamous carcinoma.
Differential Diagnosis ⚖️
• Thymic squamous carcinoma – more atypical, more destructive, often expresses CD5/CD117, and lacks the typical background of immature thymocytes.
• B2 thymoma – usually more lymphocyte-rich, with a less dominant epithelial component.
• Metaplastic thymoma / other epithelioid thymomas – architecture and overall morphologic context are key; not every epithelioid thymoma is B3.
• T-lymphoblastic lymphoma – mediastinal mass with TdT , but in this setting the neoplastic component is lymphoid rather than epithelial; cytokeratin helps demonstrate the thymic epithelial network in thymoma.
• Metastatic squamous cell carcinoma to the mediastinum – clinical history, imaging, and lack of typical thymoma architecture are critical.
Prognosis 📈
Although B3 thymoma is, on average, considered a higher-risk thymoma, prognosis still depends heavily on stage, invasion, and completeness of resection. In recent cohorts, higher-risk histologic subtypes such as B2/B3 have shown a worse prognostic profile than low-risk thymomas.
Treatment 💉
The mainstay of treatment is complete surgical resection, whenever feasible. In more advanced disease or selected scenarios, postoperative radiotherapy may play a role, especially in patients with higher-risk features.
Take-Home Messages @Notas_Patologia 📚
• B3 thymoma is an epithelial-predominant thymoma with few immature thymocytes.
• The main pitfall is the differential diagnosis with thymic squamous carcinoma.
• Perivascular spaces small groups of TdT cells lack of CD5/CD117 support B3 thymoma.
• In thymoma, stage and resectability are major prognostic factors.
• In small biopsies, a descriptive and contextual diagnosis may be safer than forcing definitive subtyping.
Selected References 📖
• WHO Classification of Thoracic Tumours, 5th edition.
• PathologyOutlines: Thymoma / thymic epithelial tumors.
• Recent reviews on thymic epithelial tumors and thymoma biology.
• Studies addressing the immunohistochemical distinction between B3 thymoma and thymic squamous carcinoma.
Disclaimer⚠️
This text is an educational summary for healthcare professionals and students. It does not replace full pathology reports, local guidelines, or individualized clinical decision-making.
Hashtags
#MedicalEducation #NotasDePatologia #pathology #PathTwitter #ThoracicPathology #MediastinalPathology #Thymoma
2
5
296

An exciting morning session here in @myESMO advanced course in early stage #NSCLC with a “deep dive” into :
➡️ Environmental Carcinogenesis
➡️screening
➡️ molecular pathology and MRD/ctDNA
➡️Defining Resectability
➡️Presurgical assessment post-chemoIO
➡️RT and AI applications
➡️Periop strategies in both AGA/ non-AGA




3
4
21
835