
Open access and free for everyone.
Joined November 2012
- Tweets 3,729
- Following 232
- Followers 1,673
- Likes 7,007
545 Photos and videos


Open Medicine Insights retweeted
Wonderful Murali!
If you get a chance it’s worth looking at the algorithm on Daraxonrasib by @allysonfelix and @MPishvaian and our software team.
If you click on the boxes you get extra info such as dose, toxicity, management, graphs re PFS/OS.
This is an early version and will evolve and grow over time as a living version 🎋🌳
We have listened to the community and our wonderful ‘rising stars’ such as @kor_shah and @allisonoconn
We feel there is a need for a platform that provides the knowledge and nuance of a clinician with the best of software/website design and AI
Thanks for your interest
myopenmedicine.com/algorithm…
2
3
37
Open Medicine Insights retweeted
Great question. I’d probably ask Toni or @DrRanaMcKay @brian_rini @HHammersMD @montypal
I’d like to know grade, sarcomatoid differentiation etc
Age is important IMO
And most importantly what the patient wants…
For this patient I’d be thinking Pembro alone if they wanted this after full explanation
Reserving Pem/Bel for very high risk (T4, N etc) but we need better bio markers (as always) something I know many are making progress with. As @tompowles1has shown in urothelial carcinoma
Great question and as we implement new drugs we need better guidance
Something we are doing @OpenMedInsights
Great episode on this combo on @uromigos post GU ASCO

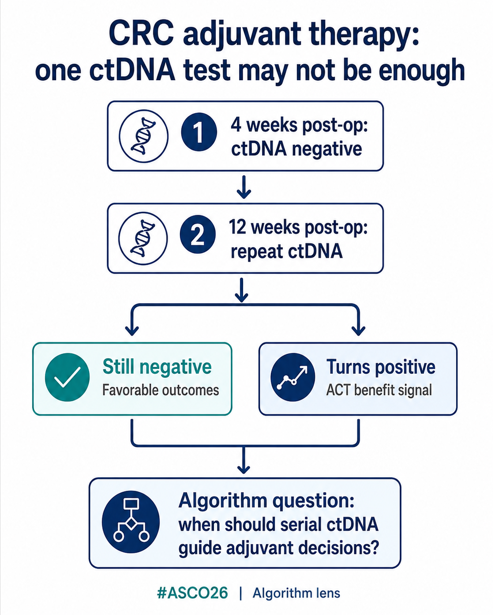
Now that adjuvant pembro plus Belzutifan is approved by @usfda
How will you decide who needs 1 drug vs 2 drugs in adjuvant RCC
pT3 NO clear cell RCC , Fit pt .
What will you u give in adjuvant .
Do vote below and opine 🙂 @OncBrothers @yekeduz_emre @dr_yakupergun @DrChoueiri
2
4
318
Open Medicine Insights retweeted

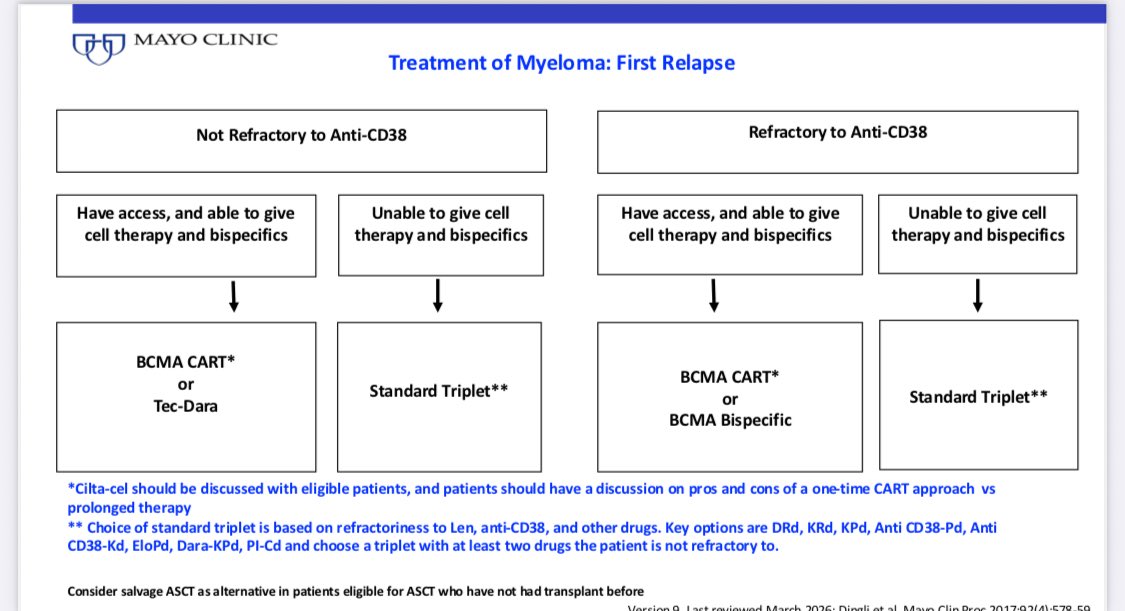
I’ll update my relapsed myeloma algorithm on @OpenMedInsights @OpenMedicineHQ soon. myopenmedicine.com/algorithm… @scserendipity1

Just out: presented at #EHA26 and published @NEJM
Randomized trial of 2 talquetamab combinations vs DPd in relapsed myeloma. The Monumental-3 trial.
Both Talq-Dara-Pom and Talq-Dara beat DPd in PFS and OS.
Choice of a Talq combination vs Tec or Tec-Dara in relapsed myeloma will be driven by patient and disease factors and requires significant expertise. Congrats @RobertoMinaMD @PlasmaCellPete @mbeksac56 @paurotero @mvmateos @thanosdimop @RahulBanerjeeMD et al.
nejm.org/doi/full/10.1056/NE…

3
11
32
3,085
Open Medicine Insights retweeted

Jun 12
Two standing ovations. Two impossible moments.
At #ASCO26, daraxonrasib delivered #pancreaticcancer survival data that nobody thought we’d ever see.
@TheGarden the @nyknicks delivered a game-winner that nearly blew the roof off the building.
Turns out there are only two ways to get a crowd on its feet in 2026:
1. Change the future of pancreatic cancer.
2. Beat the @spurs in the @NBA Finals.
One advanced science. 💊
One advanced the Knicks. 🏀
Both gave us something priceless: #HOPE that what once seemed impossible might actually happen.
💊 🔬💜
🏀 💙🧡
1
8
18
1,334
Open Medicine Insights retweeted

Jun 12
Hi friends, it's #ProstateCancer Friday! Here are Top Posts of the Week 🧵
1/ @OncoAlert on integrating ARPIs into practice:
x.com/OncoAlert/status/20643…
Jun 9

Dear Colleagues in #Prostate Cancer
Introducing #APCCC26 Live from Lugano🇨🇭Series
By @APCCC_Lugano
RT ADT ± ARPI in high-risk localized prostate cancer—where do we stand?
Drs. Bertrand Tombal, Christopher Sweeney, and Jeff Michalski discuss patient selection, biomarkers, reimbursement challenges, pelvic nodal RT, and the evidence shaping treatment intensification.
in this video:
👇 How should ARPIs be integrated into practice?
Series Faculty
@BertrandTOMBAL @ChrisSweens1 @jmmrad @drjefstathiou @CaPsurvivorship @LoebStacy @charlesryanmd @AarmstrongDuke @Ecastromarcos @LVM_Walz @piet_ost @Nicola_Fossati @AnthonyMJoshua @Prof_Nick_James @VedangMurthy @AttardLab
@Silke_Gillessen
@AOmlin
Pinging @AmandaNizamMD @scocmem @nataliagandur @gu_onc @tompowles1 @brian_rini @declangmurphy @cdanicas @neerajaiims
1
4
9
680
Open Medicine Insights retweeted

Jun 12
Wonderful and huge thanks to the the @TheIACH team. Mohamad, Amnon and all doing such great work!
Thanks for all your support of @OpenMedInsights
1
3
107
Open Medicine Insights retweeted
Jun 12
Thank you! Already a lot of fun! And we are only just starting!
Great work and energy from our GI group!
@MPishvaian @GIMedOnc @YJanjigianMD @mgfakih @GlopesMd
Great to see the algorithm on Daraxonrasib! @EileenMOReilly
myopenmedicine.com/algorithm…
5
8
360
Open Medicine Insights retweeted
Jun 11
Hi friends, it's #AcuteMyeloidLeukemia Thursday! #EHA2026 edition 🎉🎉🎉
Here are Top Posts of the Week 🧵
1/ @Dr_AmerZeidan on a decade of progress in treating AML:
x.com/Dr_AmerZeidan/status/2…

Ten years ago, no one could have imagined that you could treat acute myeloid leukemia #AMLsm in some patients with just 2 daily pills, especially the older patients who could not tolerate intensive therapies.
Now to see some of our patients in their 80s achieve long lasting remissions and be outpatient for more than 2-3 years is really gratifying, especially when you think the average survival of these patients a decade ago was less than few months.
For a clinical investigator, it is absolutely amazing to see our own patients benefit from trial drugs, but when the trial drugs are approved it is even a better feeling because you know that your efforts will touch the lives of thousands of other patients who you will never meet by benefiting from these drugs.
منذ عشر سنوات، لم يكن بإمكان أحد أن يتخيل أنه يمكن علاج سرطان الدم النخاعي الحاد لدى بعض المرضى بمجرد حبوب يومية، خاصة المرضى الأكبر سناً الذين لم يستطيعوا تحمل العلاجات المكثفة.
الآن، رؤية بعض مرضانا في الثمانينيات من العمر يحققون السيطرة الطويلة الأمد على المرض ويخرجون من المستشفى لأكثر من سنتين إلى ثلاث سنوات هو أمر مرضٍ حقًا، خاصة عندما تفكر في أن متوسط بقاء هؤلاء المرضى المصابين بالسرطان قبل عقد من الزمن كان أقل من بضعة أشهر.
بالنسبة للباحث السريري، من المذهل حقًا رؤية مرضانا يستفيدون من أدوية التجارب، ولكن عندما يتم اعتماد هذه الأدوية للاستخدام العام، يكون الشعور أفضل لأنه يمكنك أن تعرف أن جهودك ستؤثر على حياة آلاف المرضى الآخرين الذين لن تلتقي بهم أبدًا من خلال استفادتهم من هذه الأدوية.
m.yale.edu/djqg
1
4
11
1,128

#ASCO26 through an algorithm lens
@ASCO
#PANKU-Breast02 / LBA1003
Official ASCO/JCO abstract:
ascopubs.org/doi/pdf/10.1200…
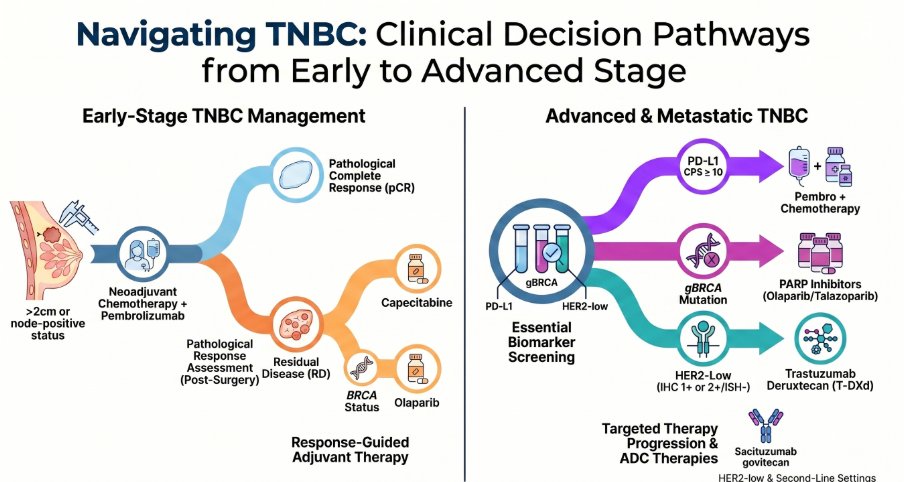
Clinical decision point:
In pretreated metastatic TNBC, should a bispecific EGFR × HER3 ADC replace physician’s choice chemotherapy when available?
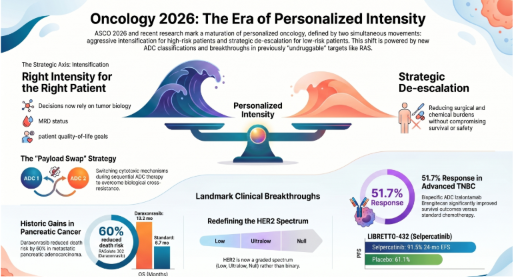
PANKU-Breast02 tested izalontamab brengitecan, or iza-bren, versus physician’s choice chemotherapy in unresectable locally advanced or metastatic TNBC after 1–2 prior systemic lines for advanced disease.
Key data:
• randomized phase III trial
• 418 patients
• iza-bren vs eribulin, capecitabine, gemcitabine or vinorelbine
• PFS: 8.5 vs 3.1 months
• PFS HR: 0.29
• OS: 15.9 vs 12.5 months
• OS HR: 0.60
• ORR: 51.7% vs 20.5%
• hematologic toxicity common
• investigational agent; global access pending
Potential algorithm impact:
PANKU-Breast02 adds a future ADC decision node in metastatic TNBC.
The key question becomes:
After taxane-containing therapy, which ADC should come next — and for whom?
@DrRanaMcKay @mgfakih @drallysonocean @MPishvaian @GIMedOnc @YJanjigianMD @glopesmd @CaPsurvivorship @AzadOncology @amerseburger @brian_rini @neerajaiims @DrChoueiri @DrYukselUrun @DrMLChua @BraunMDPhD @OmidHamidMD @alisonbirtle @DrHBurstein @IlanaSchlam @PTarantinoMD @drsarahsam @hoperugo @sanamloghavi @montypal @allisonoconn @rajshekharucms @CharuAggarwalMD @jennifermarksmd @StephenVLiu @DrSapnaPatel @parthaskar @Rfonsi1 @VincentRK @VivekSubbiah @NiuSanford @TylerSbrt @UroDocAsh @ehlJAMA
1
3
9
625
⭐️ Open Medicine Algorithm Spotlight ⭐️
Sharing a practical @OpenMedicineHQ algorithm by @CharuAggarwalMD and @BenBleibergMD on STK11/KEAP1-altered advanced/metastatic non-squamous NSCLC.
In this setting, molecular context matters — and STK11/KEAP1 alterations often make first-line treatment selection more nuanced.
🔹 Comprehensive NGS before treatment selection
🔹 Rule out actionable oncogenic drivers
🔹 PD-L1 expression still matters, but is not the whole story
🔹 Consider chemoimmunotherapy strategy and CTLA-4–containing approaches when appropriate
🔹 Reassess contraindications, comorbidities, toxicity, and clinical trial options
A useful framework for a challenging NSCLC subgroup where biology, biomarkers, and treatment intensity intersect.
How are you approaching 1L therapy selection in STK11/KEAP1-altered non-squamous NSCLC?
#LCSM #NSCLC #MedOnc #OpenMedicine
@DrRanaMcKay @mgfakih @drallysonocean @MPishvaian @GIMedOnc @YJanjigianMD @glopesmd @CaPsurvivorship @AzadOncology @amerseburger @brian_rini @neerajaiims @DrChoueiri @DrYukselUrun @DrMLChua @BraunMDPhD @nataliagandur @OmidHamidMD @alisonbirtle @DrHBurstein @IlanaSchlam @PTarantinoMD @drsarahsam @hoperugo @sanamloghavi @montypal @allisonoconn @rajshekharucms @CharuAggarwalMD @jennifermarksmd @StephenVLiu @DrSapnaPatel @parthaskar @Rfonsi1 @VincentRK @VivekSubbiah @NiuSanford @TylerSbrt @UroDocAsh @ehlJAMA
Interactive, evidence-linked, open for discussion. Feedback welcome. #LivingAlgorithms
myopenmedicine.com/algorithm…
6
7
627
Open Medicine Insights retweeted
Jun 10
Hi friends, it's #LungCancer Wednesday! Here are Top Posts of the Week 🧵
1/ @jennifermarksmd on neoadjuvant lorlatinib in stage 2 ALK NSCLC: x.com/jennifermarksmd/status…

Neoadjuvant lorlatinib x12 wks in stage III ALK NSCLC: pCR*47%, MPR 81%, ORR 84% resected. R0 in 97%, pN downstaging of most but less likely in N3 (not surprising); 1-yr EFS 97.1%. Translation data regarding DTPCs was most provocative #ASCO26 @ASCO #LCSM @ALKPositiveinc




1
4
8
1,127
#ASCO26 GU #PLUDO CCTG PR.21
@OncoAlert @ASCO
Official ASCO abstract:
asco.org/abstracts-presentat…
annalsofoncology.org/article…
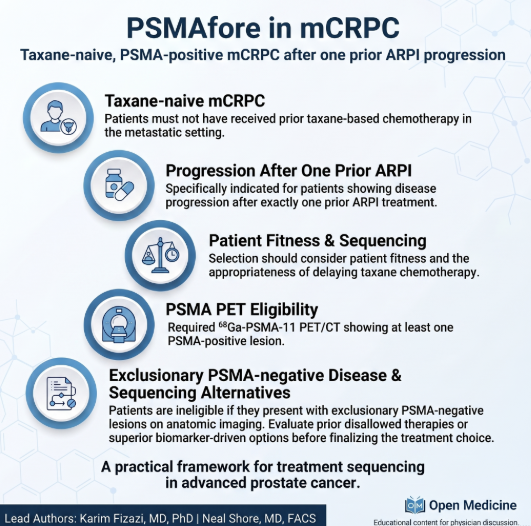
Important sequencing question in PSMA mCRPC after ARPI:
177Lu-PSMA-617 first?
Or docetaxel first?
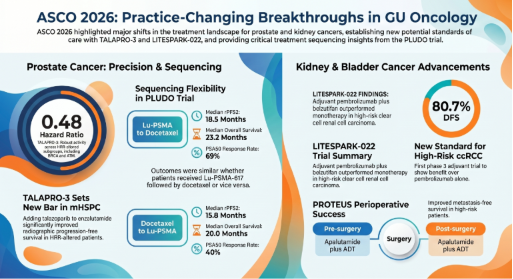
In the crossover analysis, among patients who received both therapies, there were no significant differences between LuPSMA→docetaxel and docetaxel→LuPSMA for rPFS2 or OS.
Key data:
• rPFS2: 18.5 vs 15.8 months
• HR 0.91
• OS: 23.2 vs 20.0 months
• HR 0.88
• PSA50 after crossover: 69% vs 40%
My take:
PLUDO does not create a single correct sequence.
It reminds us that sequencing in mCRPC is clinical.
PSMA PET status, symptoms, disease tempo, marrow reserve, taxane fitness, neuropathy risk, access to LuPSMA and patient preference all matter.
This is exactly where algorithms need decision nodes, not rigid rules.
@OncoAlert
@rksayyid
@DrChoueiri
@neerajaiims
@DrYukselUrun
@Uromigos
@NucMedDoc
@ecancer
@urotoday
@UrologyTimes
#ProstateCancer #GUonc #mCRPC #ASCO26
1
6
10
767
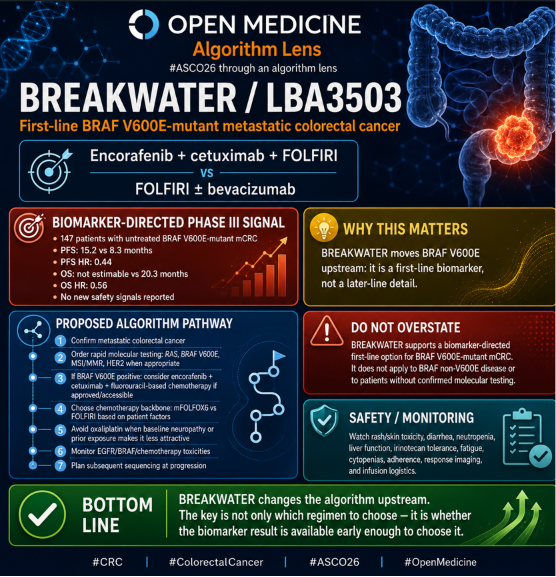
#ASCO26 through an algorithm lens
BREAKWATER / LBA3503
Primary publication in Annals of Oncology:
annalsofoncology.org/article…
Official ASCO/JCO abstract:
ascopubs.org/doi/10.1200/JCO…
Clinical decision point:
In newly diagnosed metastatic colorectal cancer, should BRAF V600E testing guide the first-line chemotherapy targeted therapy backbone?
BREAKWATER Cohort 3 tested:
• encorafenib cetuximab FOLFIRI
versus
• FOLFIRI ± bevacizumab
Key data:
• randomized phase III Cohort 3
• 147 patients with untreated BRAF V600E-mutant mCRC
• PFS: 15.2 vs 8.3 months
• PFS HR: 0.44
• OS: not estimable vs 20.3 months
• OS HR: 0.56
• no new safety signals reported
Potential algorithm impact:
BREAKWATER reinforces that BRAF V600E is a first-line biomarker, not a later-line detail.
@DrRanaMcKay @mgfakih @drallysonocean @MPishvaian @GIMedOnc @YJanjigianMD @glopesmd @CaPsurvivorship @AzadOncology @amerseburger @brian_rini @neerajaiims @DrChoueiri @DrYukselUrun @DrMLChua @BraunMDPhD @OmidHamidMD @alisonbirtle @DrHBurstein @IlanaSchlam @PTarantinoMD @drsarahsam @hoperugo @sanamloghavi @montypal @allisonoconn @rajshekharucms @CharuAggarwalMD @jennifermarksmd @StephenVLiu @DrSapnaPatel @parthaskar @Rfonsi1 @VincentRK @VivekSubbiah @NiuSanford @TylerSbrt @UroDocAsh @ehlJAMA
1
8
9
889
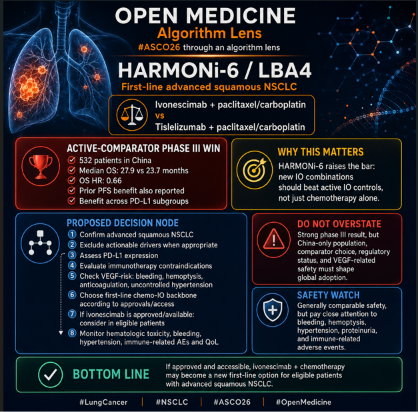
#ASCO26 through an algorithm lens
HARMONi-6 / LBA4
Primary Lancet OS publication:
thelancet.com/journals/lance…
Official ASCO abstract:
asco.org/abstracts-presentat…
Clinical decision point:
In untreated advanced squamous NSCLC, can PD-1/VEGF bispecific therapy plus chemotherapy improve outcomes over active PD-1 inhibitor plus chemotherapy?
HARMONi-6 tested:
• ivonescimab paclitaxel/carboplatin
vs
• tislelizumab paclitaxel/carboplatin
Key data:
• phase III randomized trial
• 532 patients in China
• active PD-1 comparator
• median OS: 27.9 vs 23.7 months
• OS HR: 0.66
• prior PFS benefit also reported
• benefit across PD-L1 subgroups
• safety generally comparable, but VEGF-related risks require attention
Potential algorithm impact:
HARMONi-6 creates a new question in first-line squamous NSCLC:
If PD-1 chemotherapy is the standard backbone, can dual PD-1/VEGF targeting improve the first-line node?
@DrRanaMcKay @mgfakih @drallysonocean @MPishvaian @GIMedOnc @YJanjigianMD @glopesmd @CaPsurvivorship @AzadOncology @amerseburger @brian_rini @neerajaiims @DrChoueiri @DrYukselUrun @DrMLChua @BraunMDPhD @OmidHamidMD @alisonbirtle @DrHBurstein @IlanaSchlam @PTarantinoMD @drsarahsam @hoperugo @sanamloghavi @montypal @allisonoconn @rajshekharucms @CharuAggarwalMD @jennifermarksmd @StephenVLiu @DrSapnaPatel @parthaskar @Rfonsi1 @VincentRK @VivekSubbiah @NiuSanford @TylerSbrt @UroDocAsh @ehlJAMA
1
6
7
864
Open Medicine Insights retweeted

Jun 9
Newly Diagnosed Myeloma from @VincentRK: myopenmedicine.com/algorithm…
1
8
15
2,215
Open Medicine Insights retweeted
Jun 9
Hi friends, it's #BreastCancer Tuesday! Here are Top Posts of the Week 🧵
1/ @DrHBurstein and @dr_yakupergun on the most important discussion at #ASCO26:
x.com/DrHBurstein/status/206…

Perhaps the most important breast cancer discussion this year at ASCO. A brilliant analysis of PFS2 and its meaning (or lack thereof) in advanced breast cancer. Required viewing for all clinical investigators.
1
4
5
1,211
Open Medicine Insights retweeted
Jun 8
STK11/KEAP1 Advanced/Metastatic Squamous NSCLC from @CharuAggarwalMD @BenBleibergMD: myopenmedicine.com/algorithm…
1
6
10
908
Open Medicine Insights retweeted
Jun 8
Hi friends, it's #Myeloma Monday! Here are Top Posts of the Week 🧵
1/ @VincentRK on bispecifics in first relapse:
x.com/VincentRK/status/20632…
Jun 6
Based on the latest data at #ASCO26 awe can consider bispecifics especially teclistamab (has the most data) alone or in combination with daratumumab in first relapse of myeloma.
Here is our latest mSMART.org approach to first relapse.
1
15
27
6,044
#ASCO26 through an algorithm lens
@ASCO
RASolute-302 LBA5
Primary publication in NEJM:
nejm.org/doi/full/10.1056/NE…
Clinical decision point:
In previously treated metastatic pancreatic ductal adenocarcinoma, should RAS-targeted therapy replace standard second-line chemotherapy when available?
RASolute-302 tested daraxonrasib, an oral RAS(ON) multi-selective inhibitor, versus investigator’s choice chemotherapy.
Key data:
• randomized phase III trial
• 500 patients in overall population
• daraxonrasib 300 mg orally once daily
• comparator: investigator’s choice standard chemotherapy
• OS overall population: 13.2 vs 6.7 months
• HR for death: 0.40
• PFS: 7.2 vs 3.6 months
• ORR: 31.6% vs 11.2%
• pain and global health/QoL deterioration delayed
Potential algorithm impact:
RASolute-302 creates a new post-progression decision node in metastatic PDAC.
The key question becomes:
After progression on first-line chemotherapy, is daraxonrasib available and appropriate?
A future pathway may include:
Confirm metastatic PDAC
Document prior systemic therapy
Assess RAS status and assay quality
Confirm eligibility for daraxonrasib if approved/accessible
Compare against chemotherapy options
Monitor rash, diarrhea, stomatitis/mucositis, nausea and fatigue
Plan resistance and next-line strategy
Consider clinical trials for combinations or earlier-line use
Bottom line:
RASolute-302 may transform second-line metastatic PDAC.
But implementation will require regulatory access, molecular testing, toxicity management and sequencing logic.
@CathyEngMD
@ronanhsieh
@GillSharlene
@ArndtVogel
@coffman_kelley
@ryanhuey
2
5
6
491
#ASCO26 through an algorithm lens
@ASCO
LIBRETTO-432 / LBA3
Primary publication in NEJM:
nejm.org/doi/full/10.1056/NE…
Clinical decision point:
In early-stage NSCLC, should comprehensive molecular testing at diagnosis guide adjuvant targeted therapy after definitive local treatment?
LIBRETTO-432 tested adjuvant selpercatinib vs placebo in early-stage RET fusion–positive NSCLC after definitive therapy.
Key data:
• global phase III randomized trial
• 151 patients with stage IB–IIIA RET fusion–positive NSCLC
• selpercatinib for up to 3 years
• primary efficacy population: stage II–IIIA
• median EFS: not reached vs 31.8 months
• 2-year EFS: 91.5% vs 61.1%
• EFS HR: 0.172
• OS immature
@lungoncdoc @StephenVLiu @GlopesMd @ADesaiMD @M_Torasawa @Tony_Calles
Potential algorithm impact:
LIBRETTO-432 changes the early-stage NSCLC algorithm at the testing node.
The key step is not only:
“Which adjuvant treatment?”
It is:
“Was molecular testing done early enough to identify the adjuvant option?”
A future pathway should include:
Diagnose potentially curable NSCLC
Stage accurately
Preserve tissue for comprehensive molecular testing
Test for actionable drivers, including RET fusions
Complete surgery or definitive radiation ± systemic therapy when indicated
If RET fusion-positive and eligible: consider adjuvant selpercatinib
Monitor liver enzymes, blood pressure, diarrhea, dry mouth, QT/drug interactions and adherence
Continue surveillance and long-term follow-up
Bottom line:
LIBRETTO-432 is not only an adjuvant RET-inhibitor trial.
It is an early-stage molecular-testing trial in practice.
6
11
950