Rachel retweeted

Yes, it's been our experience too: IVIG and SCIG appear to be effective in many patients with #POTS and #Dysautonomia. Access to IVIG is very restricted due a lack of insurance coverage, but we must change that to save years of disability and billions in economic loss.
3
18
111
6,179

Plus, as someone who is immunocompromised, I don't believe I can be in the hospital around patients. Sure, SCIg helped a lot with the simultaneous increase in IgG. But that doesn't mean I can take this for granted
1
33

Jun 13
These therapies impact us all so differently right? For me it was a game-changer, but it is very clear I will need to stay on it for years. I theorize that the good functioning immune cells from IVIG do help clear out the junk over time. I was on SCIG for a year and just went downhill on it, when I went back on IVIG everything got better and I have consistently improved over time. :)
1
4
48

I had that same question @sun_in_winter12 . Of the people I’ve heard from, a few have seen this reaction fade over time (months), one found relief w/ SCIG & another moved on to Baricitinib with very favorable results.
1
1
87

Baricitinib - Reddit anecdote analysis
I used an API to search 3.3 million posts and comments on 14 LC/ME subreddits for every mention of baricitinib, and ran each anecdote through Claude Code with a structured prompt.
Of 38 reports:
- 64% reported a benefit (very effective 10, somewhat 13)
- 25% saw no effect (9)
- 11% got worse (somewhat 1, much 3)
Keep in mind there is a MASSIVE selection bias here, as neutral and even negative responders are less likely to report. The actual outcomes are not this good.
Time to effect
Of 23 positive responders, 11 gave a specific onset time from first dose: 6 within 2 weeks, 5 at 2-6 weeks, 12 didnt say. Four felt something in the first few days, a couple even on day one.
Testing
A chunk of people ran inflammatory labs before and/or after: cytokine panels, interferon, IncellDx immune panels, IL-6/IL-8, ANA.
- The 10 who tested before responded better: 77% got better and zero reported no effect, vs 59% better / 33% no-effect among those who didn't mention testing.
- But testing did not prevent bad reactions. 2 of the 4 who got worse had tested beforehand, one even guided by labs. Though the serious reactions (a hospitalization with electrolyte/kidney issues MCAS flare, a Lyme reactivation, early flares) looked idiosyncratic, not something the panels would have predicted.
Dose
4 mg/day was by far the most common target. Several titrated up from 1-2 mg, usually for tolerability rather than because more worked better. A few held 2 mg (sometimes dose-reduced for kidney function) and still improved. Dose did not appear to affect onset.
What improved (for responders)?
Energy/fatigue 43%, brain fog 39%, PEM 30%, pain 30%, overall/back toward baseline 17%, exercise tolerance 13%, POTS 9%, and sleep/mood/MCAS/gut around 4% each.
Side effects mentioned
Infections (URIs, UTIs, cold sores) 7%, acne/rash 5%, GI upset 5%, headache 5%, MCAS flare 2%. Only 4 of 36 worsened - see the hospitalization, Lyme reactivation, and hard early flares above.
Caveats
- This is self-reported, uncontrolled, selection-biased data. People who improve are really motivated to post, especially about an exotic drug, and Long COVID fluctuates on its own, so some positive responses are noise.
- Many were on concurrent treatments (SCIG, other immune meds, big supplement stacks), so attribution to baricitinib alone is tougher with a non-immediate onset.
Thinking about what to analyze next: maraviroc? Stellate ganglion block? Open to requests!
10
8
34
1,697

Mazguła scig ten mundur zm profilu , bo go obrażasz... stary komunisto.
8

Jun 13
IVIG/SCIG/CAR-T are too expensive so they convince medical authorities we can simply will our diseases out of existence
1
4
89

50 CLL/RT Pearls — EHA 2026 🧬🩸
From the uploaded EHA guideline.
1️⃣ CLL = ≥5 ×10⁹/L clonal B cells 🧪
2️⃣ Classic markers: CD19 CD5 CD23 🔬
3️⃣ SLL = tissue disease low blood clone 🧫
4️⃣ MBL ≠ CLL unless ≥5 ×10⁹/L ⚠️
5️⃣ CLL-type MBL progresses ~1%/year ⏳
6️⃣ IGHV before 1L therapy 🧬
7️⃣ Mutated IGHV = better biology ✅
8️⃣ Unmutated IGHV = higher-risk course ⚡
9️⃣ TP53 = del17p and/or TP53 mutation 🚨
🔟 Check TP53 before every treatment line 🔁
1️⃣1️⃣ Use FISH for del17p 🧪
1️⃣2️⃣ Use NGS for TP53 mutation 🧬
1️⃣3️⃣ Don’t treat early asymptomatic CLL 👀
1️⃣4️⃣ High-risk biomarkers alone ≠ treatment ❌
1️⃣5️⃣ Start therapy only if iwCLL criteria met ✅
1️⃣6️⃣ Treat if progressive marrow failure 🩸
1️⃣7️⃣ Treat bulky/symptomatic nodes 📍
1️⃣8️⃣ Treat symptomatic splenomegaly 🫛
1️⃣9️⃣ Treat rapid lymphocyte doubling 📈
2️⃣0️⃣ Treat true B symptoms 🌡️
2️⃣1️⃣ CT/MRI mainly for venetoclax TLS risk ⚠️
2️⃣2️⃣ ECG before BTKi ❤️
2️⃣3️⃣ Check anticoagulants before BTKi 💊
2️⃣4️⃣ Check CYP3A interactions before venetoclax 💊
2️⃣5️⃣ Vaccinate: pneumococcus 💉
2️⃣6️⃣ Vaccinate: VZV/Shingrix 💉
2️⃣7️⃣ Vaccinate: HBV 💉
2️⃣8️⃣ Vaccinate: influenza/COVID seasonally 🦠
2️⃣9️⃣ Avoid live vaccines 🚫
3️⃣0️⃣ Routine antimicrobial prophylaxis not needed ❌
3️⃣1️⃣ IVIG/SCIG only if recurrent infections low IgG 🛡️
3️⃣2️⃣ Counsel skin cancer prevention ☀️
3️⃣3️⃣ Encourage routine cancer screening 🎯
3️⃣4️⃣ Vitamin D not routine for CLL control ❌
3️⃣5️⃣ Autoimmune cytopenias occur in CLL 🩸
3️⃣6️⃣ AIHA/ITP without CLL indication → steroids ± IVIG 💉
3️⃣7️⃣ Rituximab can help refractory AIC 🎯
3️⃣8️⃣ If iwCLL criteria present → treat CLL itself ✅
3️⃣9️⃣ Chemoimmunotherapy is largely out 🚫
4️⃣0️⃣ Targeted therapy is the modern standard 🚀
4️⃣1️⃣ No TP53 aberration → prefer time-limited therapy ⏱️
4️⃣2️⃣ Mutated IGHV → avoid indefinite therapy when possible ✅
4️⃣3️⃣ Key option: venetoclax obinutuzumab 💊
4️⃣4️⃣ New option: acalabrutinib venetoclax ± obinutuzumab 💊
4️⃣5️⃣ BTKi continuous therapy: prefer acalabrutinib/zanubrutinib ✅
4️⃣6️⃣ Ibrutinib tolerated? no automatic switch 🔁
4️⃣7️⃣ TP53 disruption → continuous BTKi often preferred 🚨
4️⃣8️⃣ After cBTKi progression → don’t use another cBTKi ❌
4️⃣9️⃣ Double-refractory CLL → pirtobrutinib, trial, ± allo-HSCT 🎯
5️⃣0️⃣ Richter transformation → biopsy first, trial if possible 🔬
#CLL #RichterTransformation #EHA2026 #Hematology #BTKi #Venetoclax #Pirtobrutinib #AdultHematology #KFSHRC

4
13
590


Jun 10
Senior Deputy Inspector General(SCIG) of Police Waruna Jayasundera has filed a writ petition before the Court of Appeal seeking an order preventing his arrest without reasonable cause in connection with investigations into the Easter Sunday attacks.
The Inspector General of Police and the Attorney General have been named as respondents in the petition.
172


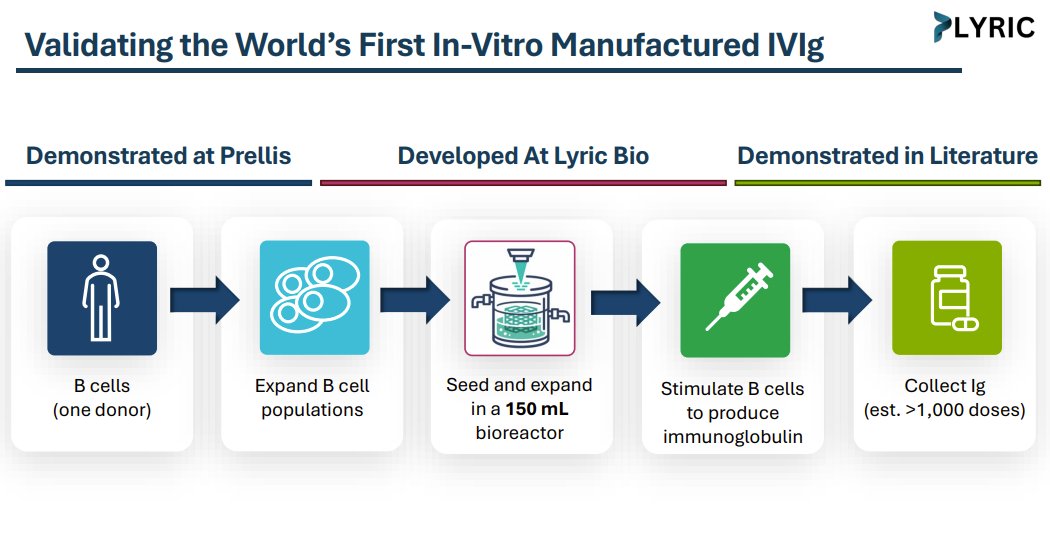
Next is @LyricBio
What it does: Lyric Bio is developing bioreactors to manufacture immunoglobulin without relying on human plasma donation.
Why it’s cool: IVIg is probably one of the most underappreciated therapeutic advances in modern medicine. It’s essentially a cocktail of donor antibodies pooled from human plasma donations. It started as antibody replacement in the 40s / 50s for people with conditions that prevented them from producing enough of their own. Then sometime in the 80s, we figured out that these same pooled antibodies could also modulate the immune system and effectively treat many autoimmune conditions.
Today, IVIg / SCIg is used across 100 autoimmune and immunodeficiency conditions and represents a market in the ~$10Bs, consolidated around a few major plasma players like CSL Behring, Takeda, and Grifols.
The obvious problem is the same with any donation-based therapy: we don’t have enough of it. The less obvious problem is that it’s hard to replace. Recombinant antibody technology works well when you know the antibody you want. IVIg is the opposite. Its therapeutic effect seems to come from the diversity and complexity of pooled human antibodies, which is exactly what makes it so hard to manufacture.
While some like @nuvigtx are attempting to recreate this effect in a single therapeutic, Lyric’s approach is to go one layer upstream. If IVIg comes from donor B cells, why not culture the B cells directly instead of continuously collecting plasma?
They’re licensing @Prellisbio ’s tissue engineering technology to recreate lymph node-like tissue through high-density donor B cell culture. If they’re successful in a) recreating the right antibody diversity and b) scaling the process, they could create B cell bioreactors that churn out IVIg-like product at a scale that meaningfully outpaces the current donation, pooling, and purification process in both quantity and hopefully, quality.
This is the kind of bioengineering I like: not forcing the medicine into a simpler manufacturing model, but building a manufacturing system that can handle the biology.
95

Jun 6
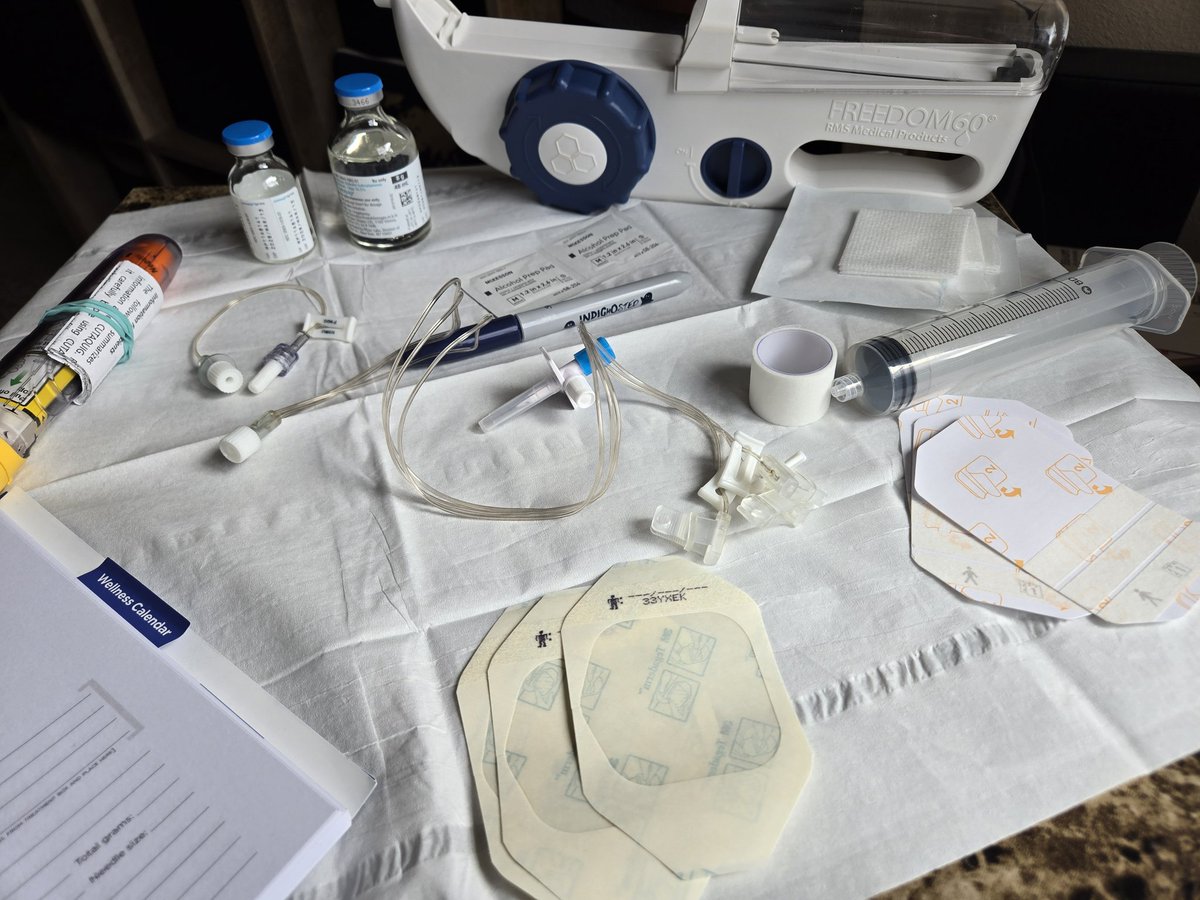
6月5日 ハイゼントラSCIg
半量超えると体がスッキリ
唾液の流れがスムーズに
元気な時と変わらない
朝担当医に嚥下が悪いことを
伝えてほしいと言ったら
担当医師がきてくれ
トロミ食に変えなきゃいけないと
思ったと
昨日の検査用紙6枚を
ホチキス止めして持ってきてくれた
3
81

Jun 5
My therapist said her other Long Covid patient saw a noticeable improvement on SCIG (subcutaneous immunoglobulins).
2
9
409


1) Xolair bei trotz Standardtherapie (Antihistaminika, etc) ausgeprägtem MCAS mit erhöhten IgE
2) scIG bei enger Indikation (z.B. schwer betroffen immunologische Auffälligkeiten wie IgG (Subklassen)mangel, etc)
3) Medikamente an GABA - Glutamat Achse bei enger Indikation
2
33

Jun 2
Patient-Led Research Collaborative (@patientled) and RTHM Clinic recently released the Long COVID Treatment Guide to support more informed conversations between patients and their clinicians.
The guide covers over 30 different interventions. Today, we’re highlighting intravenous immunoglobulin (IVIG) and subcutaneous immunoglobulin (SCIG), immunoglobulin therapies that may be especially relevant for people with Long COVID who have developed certain types of neuropathy, ME/CFS, immune deficiency, autoimmune disease, autonomic dysfunction, or who have not responded to other therapies.
Across reviewed data, IVIG demonstrated therapeutic potential for infection-associated and immune-mediated conditions. Five papers on post-COVID small fiber neuropathy reported 60–100% response rates, and two studies on autoimmune dysautonomia reported 40–80% functional improvement. In ME/CFS, three studies reported positive outcomes, and several mechanistic or review papers supported IVIG’s immunomodulatory rationale.
In the Harvard/Stanford/OMF TREATME study, 42% of individuals with Long COVID or ME/CFS who tried IVIG/SCIG reported moderate to much better symptom improvement. The NIH RECOVER IVIG study is also underway to further evaluate efficacy in Long COVID.
As with all treatments in the guide, IVIG/SCIG should be discussed with a qualified clinician to determine whether it is appropriate for an individual case, including review of risks, contraindications, drug interactions, allergies, and potential side effects. The treatment guide is an evidence-grounded resource designed to support patients and clinicians in making informed decisions together.
Download the guide here: rthm.com/treatmentguide
ALT Intravenous Immunoglobulin (IVIG) and Subcutaneous Immunoglobulin (SCIG) Medications in the Long COVID Treatment Guide RTHM and PLRC logo at the bottom
1
3
7
451

May 31
I understand. I also have low IgG & IgA. I still take scig/ivig bc I kept losing ability to walk & digest normally & tolerate being upright without it. I'm still better than b4 but I'm concerned that donors will have had covid & donate pathologic covid antibodies into the ivig
1
3
61

May 31
SCIG is used mainly for immunoglobulin replacement therapy and for some chronic autoimmune or neurological conditions.
For LC, we simply do not have the same amount of data yet.
2
25