Chidambara .ML. retweeted

Jun 14
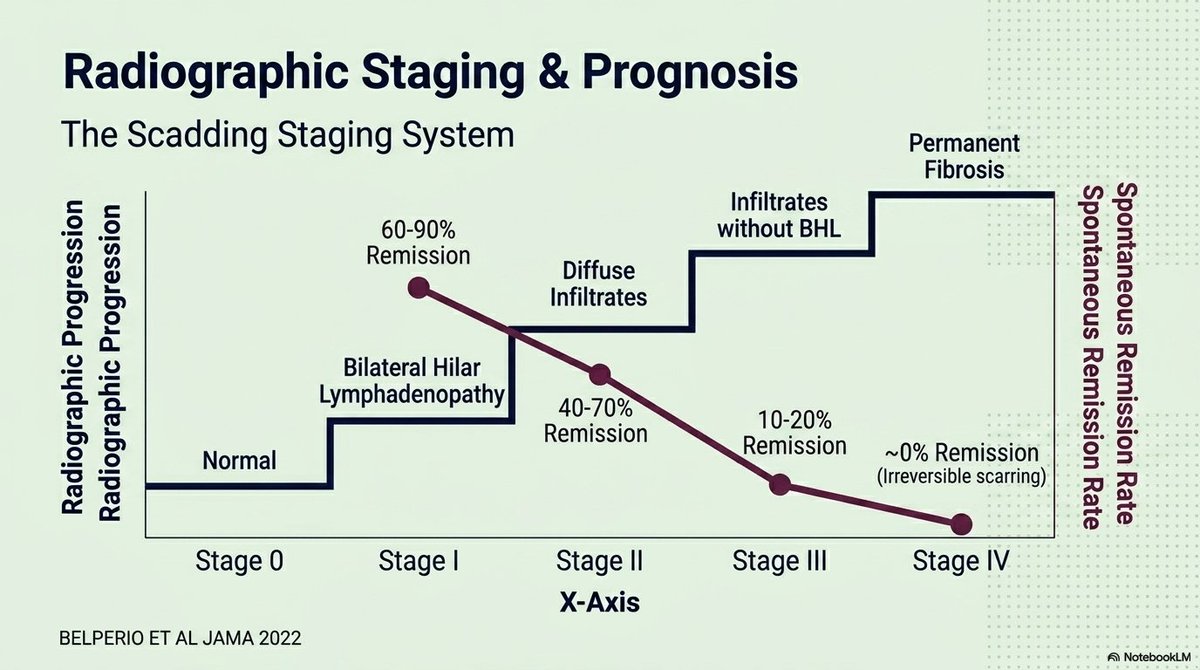
Sarcoidosis Radiographic Staging & Prognosis (Belperio et al., JAMA 2022): The Scadding Staging System mapping progression against spontaneous remission rates.
Stages correlate findings to outcomes: Stage I (BHL, 60-90% remission), Stage II (BHL infiltrates, 40-70%), Stage III (infiltrates alone, 10-20%), and Stage IV (permanent fibrosis, ~0%).
5
10
357

Jun 15
What a way to start any new #AQUABION week on a monday 😎🧢💧
Thanks to Brandon Scadding to „making my day“ today and start the week with the necessary 🚀 power.
#brandonscadding #water ##watertreatment #experts #plumber #plumbing
13


📸🧵NEWCASTLE PHOTO MEGATHREAD! I went to town this early on this morning. Scadding hot, but Bank Holiday quiet. As usual I look loads of photos, trying to capture things from a different perspective. Let's go! 1 / The Central Station water tower, and @nclcathedral

5
25
127
7,182

May 24
Absolutely it is essential for animal health &welfare the shepherd also checks sheep as he shears he check the feet for foot rot & scadding ,
gives medication for parasites and paints keel mark & tag to mark the animal as his own
As the Good shepherd marks His children as His own
4
99

🏆| 𝙎𝙘𝙖𝙙𝙙𝙞𝙣𝙜 at the double! A standout season for Riley as he wins the plaudits from both his management team and the boys around him! Solid all season long and plenty more to come!👏 #UTF


5
656

#DYK that during Doors Open weekend, you can unlock the doors to some of Toronto's hidden gems? ✨
👀 Peer into sites typically closed to the public, like Scadding Cabin, Toronto's oldest surviving building. Built in 1794!

ALT Rustic log cabin with a shingled roof surrounded by lush greenery and a wooden fence under blooming white chestnut trees.
1
1
4
327

📢The Doors Are OPEN once again!🚪
Join us May 23 & 24 from 10AM to 5PM at Scadding Cabin for @Doors_OpenTO!
Experience an exhibition of world foods in early York, spinning demonstrations, and children's games!
Details: bit.ly/4nCqnvh & bit.ly/3R6siwa
#DOT26

1
4
70

Apr 23
Chris Bosh foundation was usually at Scadding Court , no way he performed there 😭
1
24
9,854
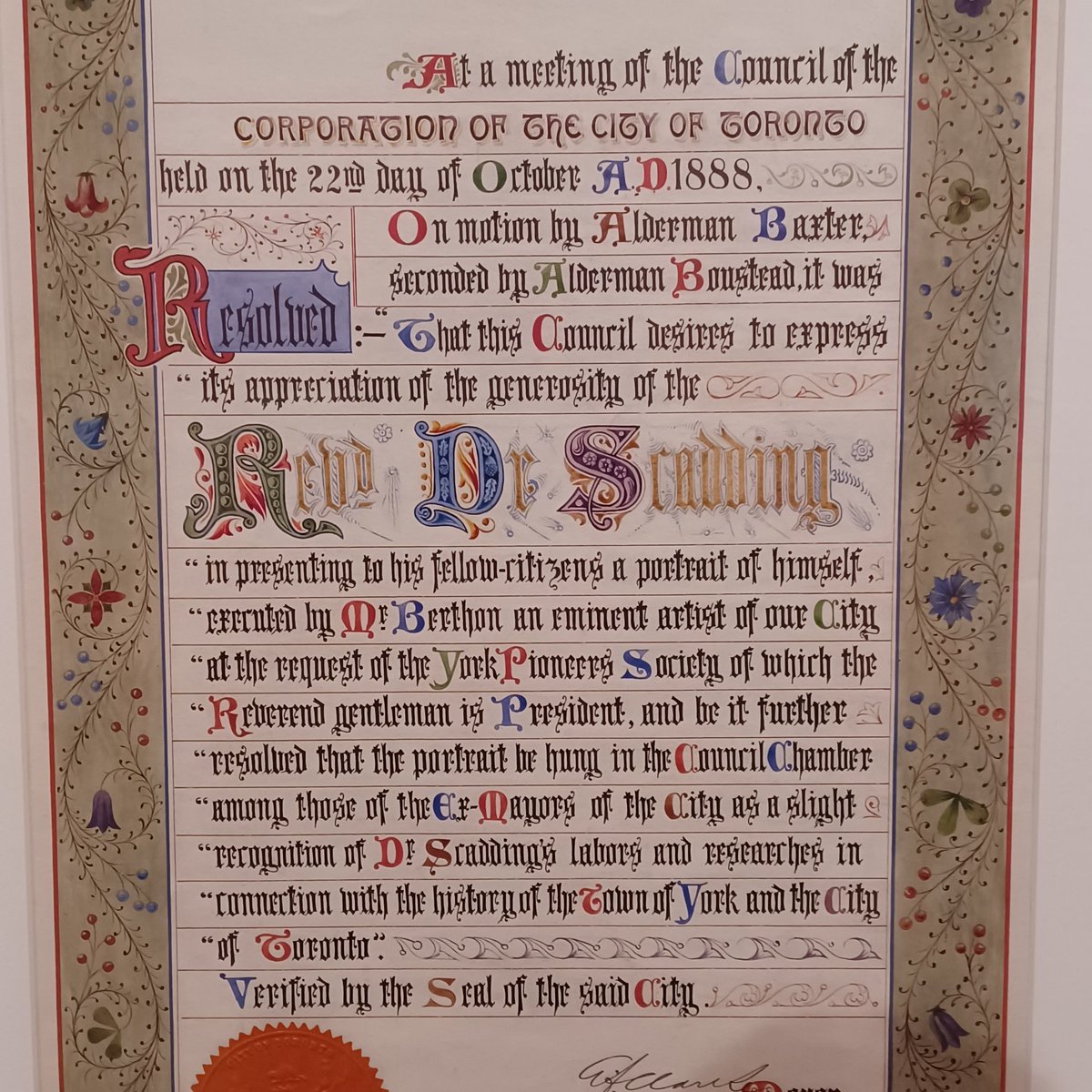
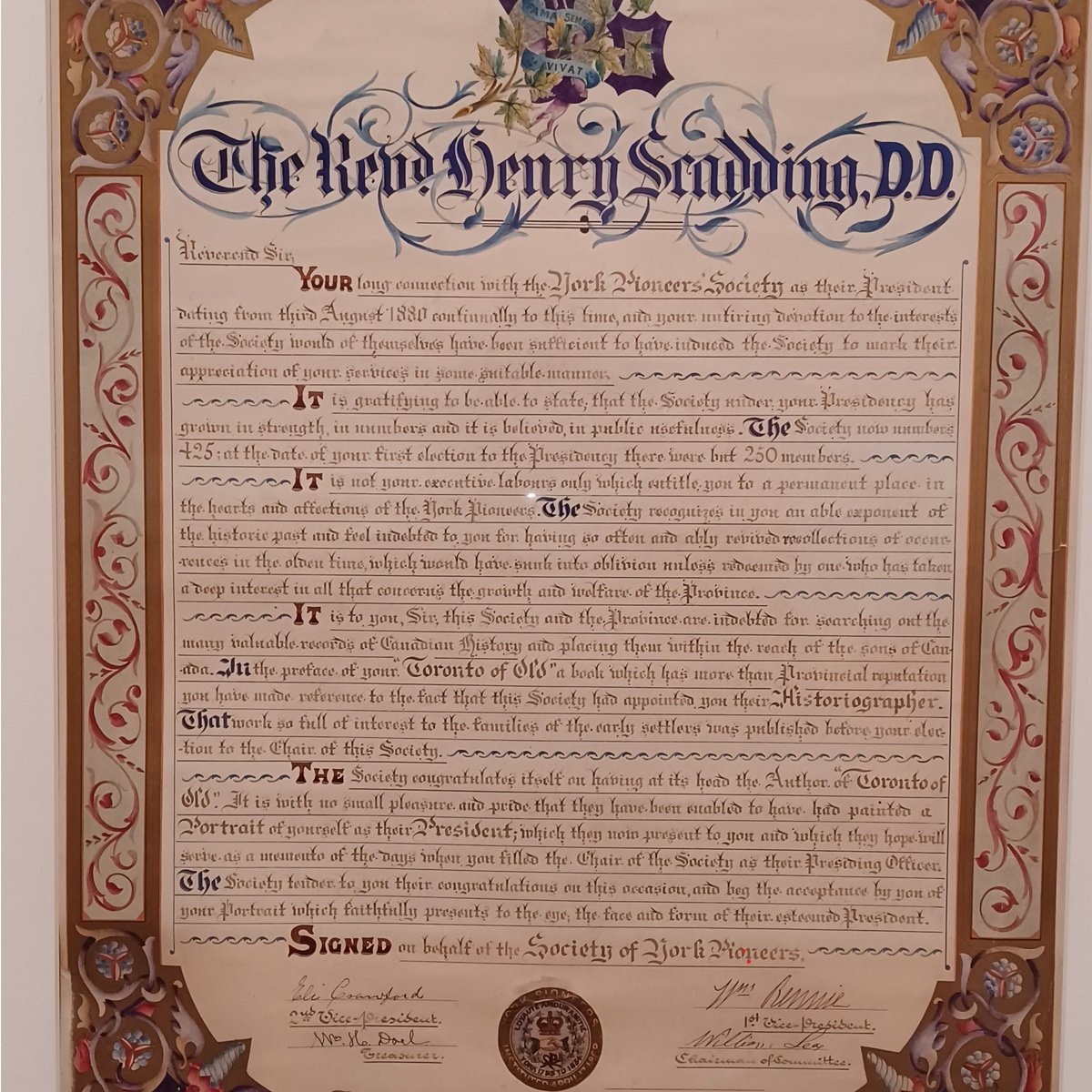
Have you seen "Loops, Swoops & Curlicues: A Legacy of Handwritten History" at the Reference Library? There are beautiful items in recognition of Rev. Dr. Henry Scadding & the York Pioneers! The exhibit is on until May 10 at the TD Gallery! @torontolibrary
📸 : Victoria Moorshead
4
4
664

🎥 PEARL in motion, a powerful day in Brussels with EUFOREA
Last Friday’s Patient Experts in Airways and Respiratory Leadership Patient Course brought together individuals living with airway diseases and leading experts for a day focused on clarity, confidence, and community.
Through open discussions and practical insights, participants explored how to understand their condition better and take an active role in their care.
👉 Step back into the experience and catch the highlights in our aftermovie!
A big thank you to everyone who made this day so meaningful 👏
This course received unrestricted educational grants from @sanofi regeneron and @EliLillyandCo
Course Co-Directors:
Dr. Xander Bertels | Dr. Sophie Scheire | Dr. Catherine Shire
Faculty:
Mrs Tonya Winders | Mrs Ellen Bonne | Prof Philippe Gevaert | Dr Sven Schneider | Prof Gert-Jan Braunstahl | Mrs Lana Hannant | Dr Sebastian Riemann | Prof Glenis Scadding
1
2
202

Leave @ExPlaceTO alone @fordnation it is jewel on the waterfront of Toronto & an historic site, so of course @fordnation wants it. The Rose Garden, Fort Rouile, Scadding cabin & the Peace Memorial are some of the meaningful parts of the site. There is history in every step.

1
40
70
646


Apr 9
Been like that since Scadding Court days @yu5ali
Apr 9

When people talk about Yusuf Ali the first thing they mention are his industry connections to get big time athletes, but i’m told by people in the scouting industry his best trait is identifying and evaluating hidden gems.
Ross Hodge and the staff have a reputation for getting more out of kids compared to their previous coaches. The development of his players cannot be overstated.
I can’t wait to see the roster construction in its totality after the portal season.
High End Prospects 🤝 Under the Radar Sleepers

3
1,058

Apr 8
Diagnosis: Stage II Sarcoidosis
Clinical Presentation Analysis
The patient is a young male in his 20s with a 5-month history of progressive respiratory symptoms:
➜ Chronic Dry Cough & Exertional Dyspnea: These symptoms, combined with the lack of response to antibiotics and bronchodilators, point toward a granulomatous or interstitial lung disease rather than an infectious or reactive airway etiology.
➜ Palpitations and Chest Tightness: In the context of suspected sarcoidosis, these are clinical "red flags" that may indicate Cardiac Sarcoidosis (conduction blocks or arrhythmias) or secondary pulmonary hypertension.
➜ Demographic Factor: Sarcoidosis frequently affects young adults (20–40 years) and typically presents with this indolent, non-productive cough.
Radiological Findings (CXR Analysis)
The provided chest radiograph shows classic signs of a systemic granulomatous process:
➜ Bilateral Hilar Lymphadenopathy: Symmetrical, well-defined enlargement of the hilar nodes (the "potato nodes" sign).
➜ Right Paratracheal Lymphadenopathy: Prominent widening of the right paratracheal stripe, completing the "Garland Triad."
➜ Interstitial Opacities: Presence of subtle reticulonodular infiltrates in the mid-to-upper lung zones, which classifies this as Scadding Stage II (Lymphadenopathy Parenchymal involvement).
➜ Normal Cardiac Silhouette: Suggests that the reported palpitations are likely due to electrical conduction issues or pulmonary pressure rather than overt congestive heart failure.
Differential Diagnosis
➜ Sarcoidosis: Most likely given the symmetry of lymphadenopathy and the patient's age.
➜ Lymphoma: Usually presents with asymmetrical mediastinal widening and constitutional "B-symptoms" (fever, weight loss).
➜ Tuberculosis (TB): Typically presents with unilateral lymphadenopathy and apical infiltrates or cavitation in adults.
➜ Hypersensitivity Pneumonitis: Possible, but less likely to cause such discrete, bulky hilar lymphadenopathy.
Recommended Management Plan
➜ Cardiac Evaluation: Immediate ECG and Echocardiogram are mandatory to investigate the palpitations and rule out cardiac sarcoidosis.
➜ High-Resolution CT (HRCT): To confirm the perilymphatic distribution of nodules.
➜ Biopsy: The gold standard for diagnosis is identifying non-caseating granulomas via EBUS-TBNA (Endobronchial Ultrasound-guided biopsy).
➜ Laboratory Workup: Serum Calcium (to check for hypercalcemia) and Pulmonary Function Tests (PFTs) with DLCO.
2
2
182
Apr 8
Diagnosis: Stage II Sarcoidosis
Clinical Presentation Analysis
The patient is a young male in his 20s with a 5-month history of progressive respiratory symptoms:
➜ Chronic Dry Cough & Exertional Dyspnea: These symptoms, combined with the lack of response to antibiotics and bronchodilators, point toward a granulomatous or interstitial lung disease rather than an infectious or reactive airway etiology.
➜ Palpitations and Chest Tightness: In the context of suspected sarcoidosis, these are clinical "red flags" that may indicate Cardiac Sarcoidosis (conduction blocks or arrhythmias) or secondary pulmonary hypertension.
➜ Demographic Factor: Sarcoidosis frequently affects young adults (20–40 years) and typically presents with this indolent, non-productive cough.
Radiological Findings (CXR Analysis)
The provided chest radiograph shows classic signs of a systemic granulomatous process:
➜ Bilateral Hilar Lymphadenopathy: Symmetrical, well-defined enlargement of the hilar nodes (the "potato nodes" sign).
➜ Right Paratracheal Lymphadenopathy: Prominent widening of the right paratracheal stripe, completing the "Garland Triad."
➜ Interstitial Opacities: Presence of subtle reticulonodular infiltrates in the mid-to-upper lung zones, which classifies this as Scadding Stage II (Lymphadenopathy Parenchymal involvement).
➜ Normal Cardiac Silhouette: Suggests that the reported palpitations are likely due to electrical conduction issues or pulmonary pressure rather than overt congestive heart failure.
Differential Diagnosis
➜ Sarcoidosis: Most likely given the symmetry of lymphadenopathy and the patient's age.
➜ Lymphoma: Usually presents with asymmetrical mediastinal widening and constitutional "B-symptoms" (fever, weight loss).
➜ Tuberculosis (TB): Typically presents with unilateral lymphadenopathy and apical infiltrates or cavitation in adults.
➜ Hypersensitivity Pneumonitis: Possible, but less likely to cause such discrete, bulky hilar lymphadenopathy.
Recommended Management Plan
➜ Cardiac Evaluation: Immediate ECG and Echocardiogram are mandatory to investigate the palpitations and rule out cardiac sarcoidosis.
➜ High-Resolution CT (HRCT): To confirm the perilymphatic distribution of nodules.
➜ Biopsy: The gold standard for diagnosis is identifying non-caseating granulomas via EBUS-TBNA (Endobronchial Ultrasound-guided biopsy).
➜ Laboratory Workup: Serum Calcium (to check for hypercalcemia) and Pulmonary Function Tests (PFTs) with DLCO.
2
27

Jordan Scadding is awarded Man of the Match following a strong all-round performance.
Jordan Scadding is sponsored by AngieH Driving Academy.
#UpTheBriz #BrislingtonFC

13
1,290