
🌉 𝐁𝐫𝐢𝐝𝐠𝐢𝐧𝐠 𝐏𝐚𝐢𝐧, 𝐍𝐨𝐭 𝐉𝐮𝐬𝐭 𝐓𝐫𝐞𝐚𝐭𝐢𝐧𝐠 𝐈𝐭: 𝐓𝐡𝐞 𝐌𝐢𝐬𝐬𝐞𝐝 𝐋𝐢𝐧𝐤 𝐢𝐧 𝐓𝐫𝐚𝐧𝐬𝐢𝐭𝐢𝐨𝐧𝐚𝐥 𝐏𝐚𝐢𝐧 𝐂𝐚𝐫𝐞
#TransitionalPain #BeyondTheBlock #PainContinuum #MedTwitter #ChronicPainPrevention #RAInsights #RegionalAnesthesia #PainMedicine #AcuteToChronic #PainPathways #MultimodalAnalgesia #TPS #PainTrajectory
#GrayZonesInRA
#GrayAreasInRA
𝐆𝐑𝐀𝐘 𝐙𝐎𝐍𝐄𝐒 𝐢𝐧 𝐑𝐀
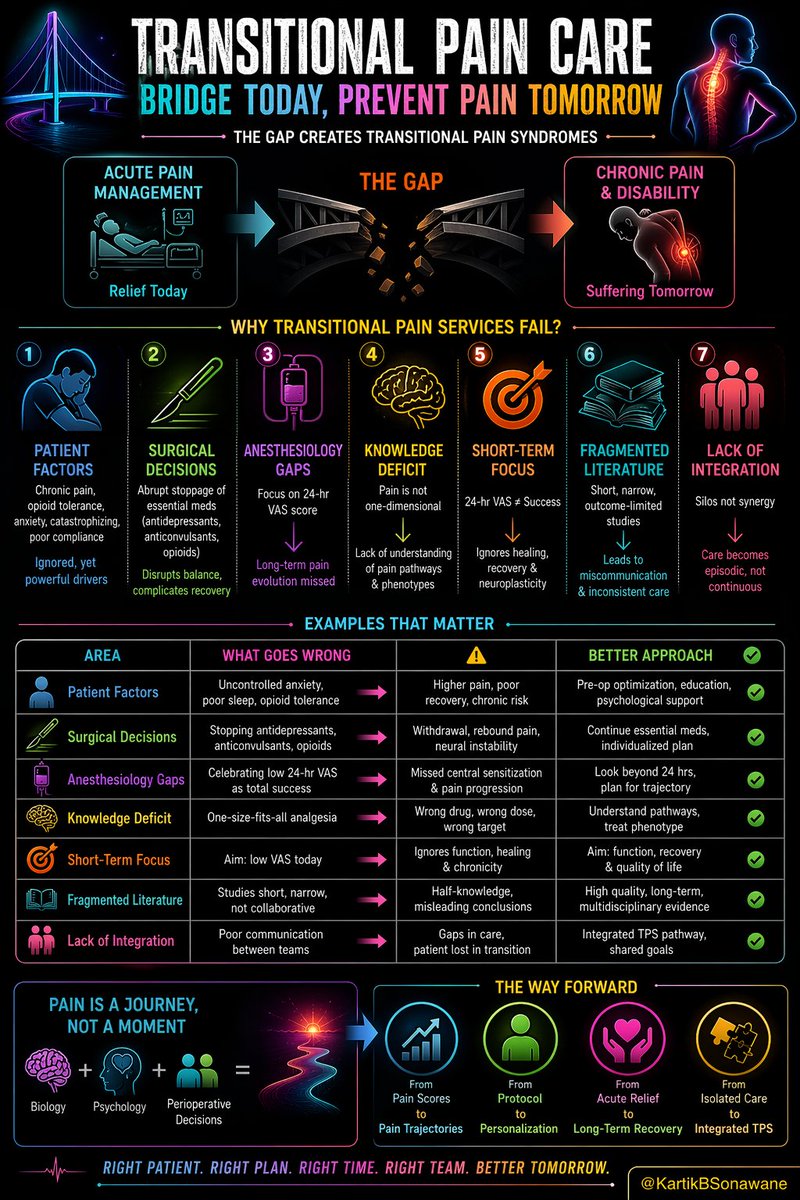
➤ Transitional Pain Services (TPS) were never meant to be a formality.
➤ They were designed as a continuum of care, preventing the silent drift from acute pain to chronic suffering.
➤ Yet, what we often witness is the rise of Transitional Pain Syndromes - where pain lingers, evolves, and embeds itself into the patient’s life.
➤ Regional anesthesia is excellent for blocking pain, but not always for modulating long-term pain trajectories.
Whats going 𝐖𝐑𝐎𝐍𝐆? 👇
🔵 👤 𝐏𝐀𝐓𝐈𝐄𝐍𝐓 𝐅𝐀𝐂𝐓𝐎𝐑𝐒 - 𝐓𝐡𝐞 𝐈𝐠𝐧𝐨𝐫𝐞𝐝 𝐅𝐨𝐮𝐧𝐝𝐚𝐭𝐢𝐨𝐧
🔹Pre-existing chronic pain, opioid tolerance, anxiety, catastrophizing, poor compliance.
🔹These are not side notes, they are primary drivers.
🔹Ignoring them is like treating symptoms while fueling the disease.
🔴 🔪 𝐒𝐔𝐑𝐆𝐈𝐂𝐀𝐋 𝐃𝐄𝐂𝐈𝐒𝐈𝐎𝐍𝐒 - 𝐔𝐧𝐢𝐧𝐭𝐞𝐧𝐝𝐞𝐝 𝐇𝐚𝐫𝐦
🔸 Abrupt stoppage of essential medications (antidepressants, anticonvulsants, baseline opioids) disrupts neurochemical balance.
🔸In trying to “simplify,” we often complicate recovery.
⚫ 💉 𝐀𝐍𝐄𝐒𝐓𝐇𝐄𝐒𝐈𝐎𝐋𝐎𝐆𝐘 𝐆𝐀𝐏𝐒 - 𝐀𝐜𝐮𝐭𝐞 𝐋𝐞𝐧𝐬, 𝐂𝐡𝐫𝐨𝐧𝐢𝐜 𝐂𝐨𝐧𝐬𝐞𝐪𝐮𝐞𝐧𝐜𝐞𝐬
◾Brilliant at managing immediate pain, yet often limited by a 24-hour VAS mindset.
◾Pain relief is celebrated early, while long-term pain evolution goes untracked.
🟣 🧠 𝐊𝐍𝐎𝐖𝐋𝐄𝐃𝐆𝐄 𝐃𝐄𝐅𝐈𝐂𝐈𝐓- 𝐏𝐚𝐢𝐧 𝐈𝐬 𝐍𝐨𝐭 𝐎𝐧𝐞-𝐃𝐢𝐦𝐞𝐧𝐬𝐢𝐨𝐧𝐚𝐥
🔹 Nociceptive ≠ Neuropathic ≠ Nociplastic.
🔹Without understanding pain pathways and phenotypes, we end up applying uniform solutions to diverse problems.
💠 🎯 𝐒𝐇𝐎𝐑𝐓-𝐓𝐄𝐑𝐌 𝐆𝐎𝐀𝐋𝐒 - 𝐓𝐡𝐞 𝐁𝐢𝐠𝐠𝐞𝐬𝐭 𝐓𝐫𝐚𝐩
🔹 A low VAS score at 24 hours is not success - it’s just a snapshot.
🔹 True success lies in functional recovery, prevention of central sensitization, and avoiding chronicity.
🔘 📚 𝐅𝐑𝐀𝐆𝐌𝐄𝐍𝐓𝐄𝐃 𝐋𝐈𝐓𝐄𝐑𝐀𝐓𝐔𝐑𝐄 - 𝐌𝐢𝐬𝐥𝐞𝐚𝐝𝐢𝐧𝐠 𝐒𝐢𝐦𝐩𝐥𝐢𝐜𝐢𝐭𝐲
➜ Short, procedure-focused, and outcome-limited studies create half-knowledge.
➜ This leads to miscommunication, inconsistent practices, and silo-based decision-making.
✳️ 🤝 𝐋𝐀𝐂𝐊 𝐎𝐅 𝐈𝐍𝐓𝐄𝐆𝐑𝐀𝐓𝐈𝐎𝐍 - 𝐓𝐡𝐞 𝐂𝐨𝐫𝐞 𝐅𝐚𝐢𝐥𝐮𝐫𝐞
✅ Surgeons, anesthesiologists, and pain physicians often work in parallel, not in sync.
✅ TPS fails when care is episodic instead of continuous.
⚪ 🚀 𝐓𝐡𝐞 𝐖𝐚𝐲 𝐅𝐨𝐫𝐰𝐚𝐫𝐝
✔️ Shift from Pain Scores → Pain Trajectories
✔️ Shift from Protocol → Personalization
✔️ Shift from Acute Relief → Long-Term Recovery
✔️ Shift from Isolated Care → Integrated TPS Model
🔥 𝐅𝐈𝐍𝐀𝐋 𝐓𝐀𝐊𝐄𝐀𝐖𝐀𝐘𝐒
👉 Pain is not a 24-hour event. It is a biological journey, influenced by neural plasticity, psychology, and perioperative decisions.
👉 If we continue to measure success in hours, we will continue to create suffering for months… even years.
👉 Transitional Pain Care is not about crossing the bridge quickly - it’s about making sure the patient never falls off it.
👉 Even a “perfect block” can fail the patient if:
▫️ TPS is absent
▫️ Baseline meds are stopped
▫️ Pain phenotype is misunderstood
👉 Move from: “Did my block work?”
To: “Did my intervention alter the patient’s pain journey?”
👉 RA may start the story… but transitional pain care decides the ending.
6
427

7 Feb 2025
Thrilled to see our work published in @RAPMOnline! Building a transitional pain service is both complex and rewarding. Honored to collaborate with such an incredible team. Thanks @EMARIANOMD @ESchwenkMD @TobiHunterDNP @KyleHarrisonMD @VAPaloAlto @stanfordanes! #TransitionalPain
2
2
613

1 Feb 2025
@200UB313 teaching us about the pelvic pain in pregnant women which is not given enough attention but is a serious problem which needs addressing urgently. A very passionate talk @DaraEsra @ESRA_Society
#transitionalpain services need to be set up for these patients

1
1
4
129

12 Oct 2024
Calling all Pain Nurses interested in Transitional Pain and Service Development!! Come and join our free workshop available to Pain Nurse Network members!! #Painnurse #transitionalpain #qualityimprovement @RNPainNet
6
7
519

27 Sep 2024
Cash-strapped Pakistan gets $7 billion loan from IMF, Finance Minister says will face 'transitional pain'
newsboxer.com/blog/blogdesc/…
#cashtrapped #PakistanGovt #IMF #transitionalpain #IMFLoan
4
4
53

23 Aug 2023
The post-op pain experience varies for each patient. However, incorporating a multimodal approach that involves #cryoNB can play a crucial role in minimizing #TransitionalPain and facilitating the recovery process.
Learn more at bit.ly/transitionalpain
2
2
325

11 Apr 2023
I am pleased to share with you our new publication; addressing a very important and emerging topic (Transitional Pain Medicine).
@vafisalmasi @DrOttestad @DrSeanMackey @StanfordPain @stanfordanes
Enjoy!
sciencedirect.com/.../pii/S1…...
#painmanagement #chronicpain #TransitionalPain
3
5
23
4,231

20 Mar 2023
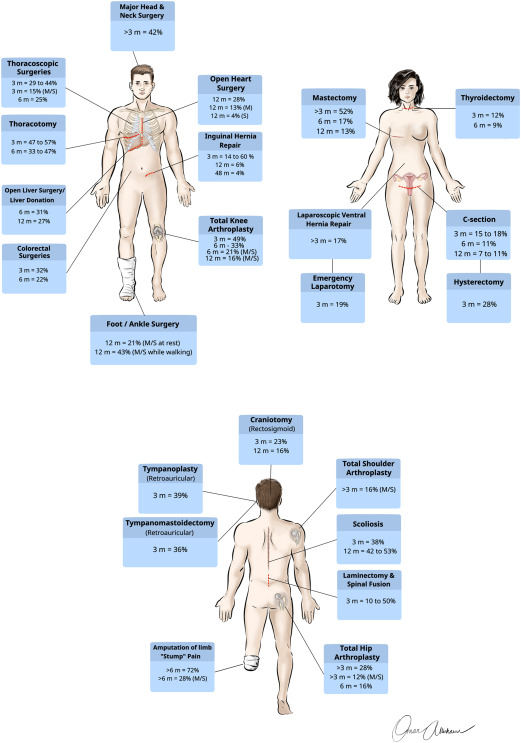
Saphenous nerve block @ mid-thigh remains an important tool in diagnosing & treating
▶️persistent post-surgical pain
➡️ s/p Ankle Surgery
⏩ s/p Knee Surgery/Replacement
#postsurgicalpain #transitionalpain #orthopedics #chronicpain @ASPSP_Pain
1
7
666
4 Mar 2023
I am thrilled to share with you my new lecture on “Transitional Pain Medicine”! In this lecture, I will take you over the rational and potential of this new field, as well as my personal vision.
Enjoy: youtu.be/XYml45jr_GE
#TransitionalPain #CPSP #PPSP #ChronicPain
1
4
21
1,948

15 Feb 2023
Thank you @DrKimBaylessNP for all what you do for the pain community #TransitionalPain
@ASRA_Society
1
5
79
2 Feb 2023
I have a manuscript coming soon in this topic – stay tuned. @kaohesham @Vafisalmasi @DrOttestad @NarouzeMD @EMARIANOMD @Drhaclarke
#TransitionalPain #CPSP #PPSP #ChronicPain #AcutePain #PainPhysician
1
808

16 Jan 2023
Are you attending #STS2023? Don't miss Nathalie Cote, our TPS physiotherapist, speaking about "Non-Pharmaceutical Approaches to Pain Management" on Jan 21st. More info here: cdmcd.co/rMkJMB
#TransitionalPain #ChronicPain
2
6
593

11 Jan 2023

Improving perioperative care to prevent chronic post-surgical #pain. Don’t miss @Drhaclarke at the @a2cps_pain Journal Club on Jan 26 to learn more. Register here: surveymonkey.com/r/VPYRM72
#transitionalpain
3
6
601
11 Jan 2023
Improving perioperative care to prevent chronic post-surgical #pain. Don’t miss @Drhaclarke at the @a2cps_pain Journal Club on Jan 26 to learn more. Register here: surveymonkey.com/r/VPYRM72
#transitionalpain
5
12
1,933

7 Dec 2022
I had a great time giving a talk about nerve blocks to our new #acutepain and #transitionalpain nurses while we created medication vial ornaments 🎄


1
11

30 Nov 2022
Check out our publication! We adapted a #ChronicPain questionnaire for the #TransitionalPain setting through #pediatric patient & family feedback. Grateful for this team! @DrLisaIsaac @JenniferTyrre14 @lallooc @rachelgoren @SKAnesthesia
#PatientEngagement
doi.org/10.1186/s41687-022-0…
2
2
19 Nov 2022
@DrKimBaylessNP reviews the benefits of the #transitionalpain service and the need for #opioid stewardship. #APPRNSIG @ASRA_Society
1
4

27 Jul 2021
New from @RAPMOnline: Making a business plan for a transitional pain service in the U.S.
ow.ly/FdM450FywvV
#TransitionalPain #Regionalanesthesa #Pain #ChronicPain
@NarouzeMD @RodneyGabrielMD @kaohesham @KyleHarrisonMD @EMARIANOMD
@dr_rajgupta @ESchwenkMD
7
10

21 Jul 2021
It is normal to experience pain after surgery, but what happens when it is months, years post surgery and still experiencing #pain? Wish there was services like this when I had my 1st shoulder surgery. Check it out #TransitionalPain services
21 Jul 2021
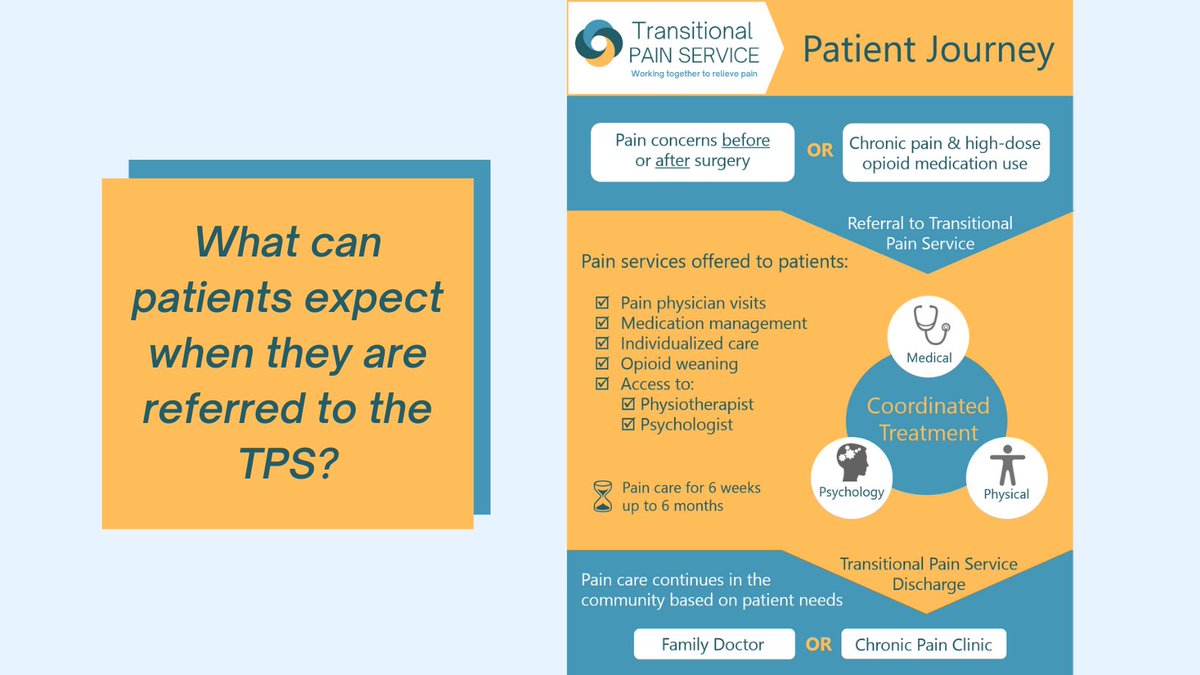
What can patients expect at the #transitionalpain service? Find out more about our approach to patient care on our website: transitionalpainservice.ca/f…
2
5
21 Jul 2021
What can patients expect at the #transitionalpain service? Find out more about our approach to patient care on our website: transitionalpainservice.ca/f…
1
5