
In honor of AIDS Awareness Day, we’re highlighting a powerful TEDMED talk. Millions are infected each year by something as simple as a syringe. For 30 years, Marc Koska has fought this silent threat, reused needles that spread deadly disease. His auto-disabling syringe is saving lives and transforming how the world handles injections. One innovation can break the chain of infection.
Watch his #TEDMED talk here: ow.ly/aam950Y7GNv
#AIDSAwarenessDay #GlobalHealth #InnovationForGood #MarcKoska #LifeSavingTech #SaferInjections #TEDMED #HealthEquity #BreakTheChain #PreventInfection #Apiject


320

Jan 26
Apiject Holdings will open a drug #manufacturing facility in Apex focused on producing generic injectable #medicines on the FDA's drug shortage list. Read more at: hubs.ly/Q03_Nyr80

1
2
88

7 May 2025
今日もリスナーさんから
ワクチンをワープスピードですすめたトランプは犯罪者、彼こそ裁かれるべき!とゆうアホがメールを送ってきた〜笑笑
私がトランプ信者(笑)だとゆーことを知っていてこのメール。
イラッとするわ💓
ワープスピード作戦 では?
プレドシリンジ 上記の画像 の注射器にワクチンが製造段階で
入った状態の アンプルを差す これを使ったのです。
プレドシリンジ(プレフィルドシリンジ)は、事前フィル医薬品が充填された状態で提供されるシリンジ(注射器)のことです。
ワープスピード作戦
5 月 12 日: 国防総省と HHS は、2020 年末までに米国全土に配布する 1 億本以上のプレフィルド シリンジについて ApiJect と 1 億 3,800 万ドルの契約を締結した。
2021 年に 5 億本以上のプレフィルド シリンジを生産するという最終目標に向けて製造能力の開発も行いました。
• 6 月 9 日: HHS と国防総省は、ワクチンや治療に必要な可能性のあるバイアルの国内製造能力を増強するための共同の取り組みを発表しました::
• 6 月 11 日: HHS は、必要に応じて年間約 1 億 6,400 万本の Valor Glass バイアルを生産できるように国内製造能力を拡大するため、Corning に 2 億 400 万ドルの資金提供を発表しました。
ワープスピード作戦ですね😅
とにかくアンチトランプが酷い笑
🐎🦌なんかな笑
自分で思ってたらいいのに
なぜ私に言う?
しかもお金貸してだと。
貸すわけねーだろ
たいした付き合いもないのに。
答え
➀ファイザーのワクチンは
解凍開始から24時間以内に使用が条件
ワープスピード作戦は?
➁最初から、注射器にワクチンを充填したものを
使用しました。 上の画像にあるような
然るに、➁は、常温で使用できる
内容物が違うワクチン もしくは病理用食塩水
であった可能性が強いのです。
死者が出ている コロナワクチンは全て上記画像の
タイプです
ワープスピード作戦では 注射器に事前に充填されたものが使用された
1
2
21
935
What is our first line of defense against viral outbreaks? Public health measures, explains Ed Kelley (@etkelley419), Chief Global Health Officer at Apiject and former WHO Director of Integrated Health Services. Watch the full TEDMED Conversation here: youtube.com/watch?v=FvITGdwV…
#mpox #publichealth #health #outbreak
573

10 Sep 2024
Reach out to PJ Kim or Morgan Amsler if you would take advantage of the many befits of the Prefilled ApiJect Injector!
#contractpharma #ContractPharmaConference #outsourcing

2
29

4 Aug 2024
I missed this one~
DOD Awards $138 Million Contract Enabling Prefilled Syringes for Future COVID-19 Vaccine (May 12, 2020)
Statement attributed to Lt. Col. Mike Andrews, Department of Defense spokesman:
"Today the Department of Defense and the U.S. Department of Health and Human Services, announce a $138 million contract with ApiJect Systems America for “Project Jumpstart” and “RAPID USA,” which together will dramatically expand U.S. production capability for domestically manufactured, medical-grade injection devices starting by October 2020.
Spearheaded by the DOD’s Joint Acquisition Task Force (JATF), in coordination with the HHS Office of the Assistant Secretary for Preparedness and Response, the contract will support “Jumpstart” to create a U.S.-based, high-speed supply chain for prefilled syringes beginning later this year by using well-established Blow-Fill-Seal (BFS) aseptic plastics manufacturing technology, suitable for combatting COVID-19 when a safe and proven vaccine becomes available.
"Jumpstart” will enable the manufacture of more than 100 million prefilled syringes for distribution across the United States by year-end 2020.
The contract also enables ApiJect Systems America to accelerate the launch of RAPID USA manufactured in new and permanent U.S.-based BFS facilities with the ultimate production goal of over 500 million prefilled syringes (doses) in 2021.
This effort will be executed initially in Connecticut, South Carolina and Illinois, with potential expansion to other U.S.-based locations.
defense.gov/News/Releases/Re…
16 Mar 2024

Operation Warp Speed.......
Come with me and you'll be
In a world of pure imagination
Take a look and you'll see
Into your imagination
We'll begin with a spin
Traveling in the world
Of my creation
What we'll see
Will defy explanation
1
5
12
3,810
4 Jul 2024
U.S. International Development Finance Corporation (DFC)
The United States International Development Finance Corporation (DFC) is a development finance institution and agency of the United States federal government. DFC invests in development projects primarily in lower and middle-income countries.
First authorized on 5 October 2018 by the BUILD Act, the independent agency was formed on 20 December 2019 by merging the Overseas Private Investment Corporation (OPIC) with the Development Credit Authority (DCA) of the United States Agency for International Development (USAID), as well as with several other smaller offices and funds.
The BUILD Act was introduced in the House and Senate in February 2018 with broad bipartisan support, based on proposals drafted by researchers at the Center for Global Development.
DFC invests in sectors that include sanitation, infrastructure, healthcare, and food security. The DFC lists innovation, sustainable jobs, workers' protection, women's economic empowerment, and bolstering global supply chains as broader themes in its investment priorities.
The DFC states that its investments aim to advance global development, U.S. foreign policy, and U.S. taxpayer interests.
On May 14, 2020, President Trump signed an Executive Order which delegates authority to the DFC Chief Executive Officer to make loans to private institutions to support the response to COVID-19 or strengthen relevant supply chains.
Trump administration, through DFC, announced that it planned to give Kodak a $765 million loan for manufacturing ingredients used in pharmaceuticals, in order to rebuild the national stockpile depleted by the COVID-19 pandemic and reduce dependency on foreign factories.
The funding was put on hold as the U.S. Securities and Exchange Commission began probing allegations of insider trading by Kodak executives ahead of the deal's announcement, and DFC's inspector general announced scrutiny into the loan terms.
The agency received criticism for the loan deal. The agency has given millions of dollars to ApiJect Systems.
Current CEO Scott Nathan was nominated by the Biden-Harris Administration in September 2021 and was confirmed February 2022.
en.wikipedia.org/wiki/U.S._I…
wsj.com/articles/kodak-loan-…

4 Jul 2024
On Jan. 2, 2020 it was officially replaced by the U.S. International Development Finance Corporation, or DFC.
2
1
5
798

2 Apr 2024
BTS at the World Vaccine Congress 🎬
One of our excellent confeeence producers Anna Louise Hindley-Skelt has sat down with Edward Kelley to discuss all things #WVCDC for the @ApiJectCorp podcast.
#worldvaccinecongress #apiject

1
1
6
563

22 Dec 2023
APIject means API (application programming interface) injection. Why would the Dept of Defense need this? And for 750 million people? Has to be for them — the enemies among us. To track them on the blockchain.
1
1
31
13 Dec 2023
Operation Warp Speed......Timeline
OWS is a partnership among components of the Department of Health and Human Services (HHS), including the Centers for Disease Control and Prevention (CDC), the National Institutes of Health (NIH), and the Biomedical Advanced Research and Development Authority (BARDA), and the Department of Defense (DoD).
OWS engages with private firms and other federal agencies, including the Department of Veterans Affairs.
It coordinated existing HHS-wide efforts, including the NIH's Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) partnership, NIH's Rapid Acceleration of Diagnostics (RADx) initiative, and work by BARDA.
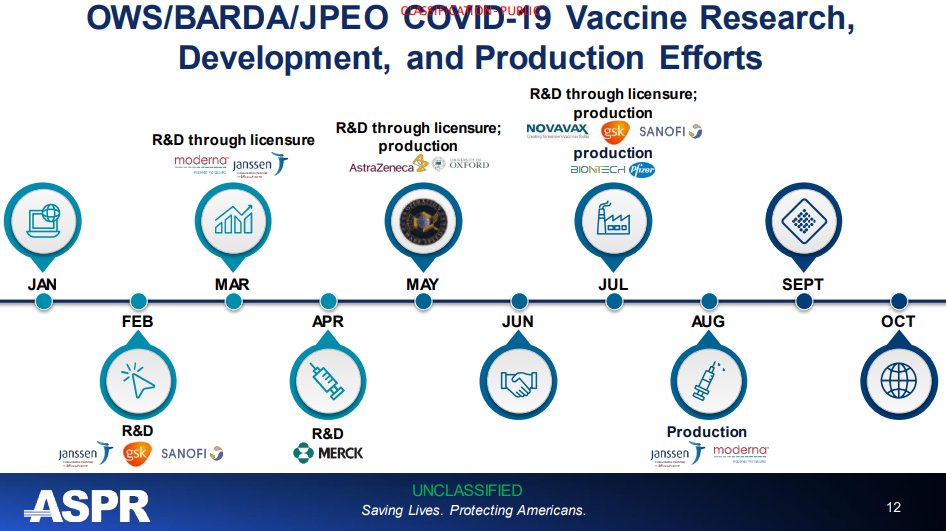
March 30:
HHS announced $456 million in funds for Johnson & Johnson's (Janssen) candidate vaccine. Phase 1 clinical trials began in Belgium on July 24th and in the U.S on July 27th. Janssen's large-scale Phase 3 clinical trial began on September 22, 2020, making them the fourth OWS candidate to enter Phase 3 clinical trials in the United States. Up to 60,000 volunteers will be enrolled in the trial at up to nearly 215 clinical research sites in the United States and internationally.
April 16:
HHS made up to $483 million in support available for Moderna's candidate vaccine, which began Phase 1 trials on March 16 and received a fast-track designation from FDA.
This agreement was expanded on July 26 to include an additional $472 million to support late-stage clinical development, including the expanded Phase 3 study of the company's mRNA vaccine, which began on July 27th.
May
May 21: HHS announced up to $1.2 billion in support for AstraZeneca's candidate vaccine, developed in conjunction with the University of Oxford. The agreement is to make available at least 300 million doses of the vaccine for the United States, with the first doses delivered as early as October 2020, if the product successfully receives FDA EUA or licensure. AstraZeneca's large-scale Phase 3 clinical trial began on August 31, 2020.
Select actions to support OWS vaccine and therapeutic development so far include:
July 7:
HHS announced $450 million in funds to support the large-scale manufacturing of Regeneron's COVID-19 investigational anti-viral antibody treatment, REGN-COV2. This agreement is the first of a number of OWS awards to support potential therapeutics all the way through to manufacturing. As part of the manufacturing demonstration project, doses of the medicine will be packaged and ready to ship immediately if clinical trials are successful and FDA grants EUA or licensure.
July 7:
HHS announced $1.6 billion in funds to support the large-scale manufacturing of Novavax's vaccine candidate. By funding Novavax's manufacturing effort, the federal government will own the 100 million doses expected to result from the demonstration project.
July 22:
HHS announced up to $1.95 billion in funds to Pfizer for the large-scale manufacturing and nationwide distribution of 100 million doses of their vaccine candidate. The federal government will own the 100 million doses of vaccine initially produced as a result of this agreement, and Pfizer will deliver the doses in the United States if the product successfully receives FDA EUA or licensure, as outlined in FDA guidance, after completing demonstration of safety and efficacy in a large Phase 3 clinical trial, which began July 27th.
July 31:
HHS announced approximately $2 billion in funds to support the advanced development, including clinical trials and large scale manufacturing, of Sanofi and GlaxoSmithKline's (GSK) investigational adjuvanted vaccine. By funding the manufacturing effort, the federal government will own the approximately 100 million doses expected to result from the demonstration project. The adjuvanted vaccine doses could be used in clinical trials or, if the FDA authorizes use, as outlined in agency guidance, the doses would be distributed as part of a COVID-19 vaccination campaign.
August 5:
HHS announced approximately $1 billion in funds to support the large-scale manufacturing and delivery of Johnson & Johnson's (Janssen) investigational vaccine candidate. Under the terms of the agreement, the U.S. Government will own the resulting 100 million doses of vaccine, and will have the option to acquire more. The company's investigational vaccine relies on Janssen's recombinant adenovirus technology, AdVac, a technology used to develop and manufacture Janssen's Ebola vaccine with BARDA support; that vaccine received European Commission approval and was used in the Democratic Republic of the Congo (DRC) and Rwanda during the 2018-2020 Ebola outbreak that began in the DRC.
August 11:
HHS announced up to $1.5 billion in funds to support the large-scale manufacturing and delivery of Moderna's investigational vaccine candidate. Under the terms of the agreement, the U.S. Government will own the resulting 100 million doses of vaccine, and will have the option to acquire more. The vaccine, called mRNA-1273, has been co-developed by Moderna and scientists from the National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health. NIAID has continued to support the vaccine's development including nonclinical studies and clinical trials. Additionally, BARDA has supported phase 2/3 clinical trials, vaccine manufacturing scale up and other development activities for this vaccine. The Phase 3 clinical trial, which began July 27, is the first government-funded Phase 3 clinical trial for a COVID-19 vaccine in the United States.
August 23:
As part of the agency's efforts to combat COVID-19, the FDA issued an emergency use authorization (EUA) for investigational convalescent plasma. Based on available scientific evidence, the FDA determined convalescent plasma may be effective in lessening the severity or shortening the length of COVID-19 illness in hospitalized patients, and that the known and potential benefits of the product outweigh the known and potential risks. The EUA authorizes the distribution of convalescent plasma in the U.S. as well as its administration by health care providers, as appropriate, to treat suspected or confirmed cases of COVID-19. Learn more about EUAs.
October 9:
HHS announced an agreement with AstraZeneca for late-stage development and large-scale manufacturing of the company's COVID-19 investigational product AZD7442, a cocktail of two monoclonal antibodies, that may help treat or prevent COVID-19. The goal of AstraZeneca's partnership with the U.S. Government is to develop a monoclonal antibody cocktail that can help prevent infection. An effective monoclonal antibody that can prevent COVID-19, particularly one that is long-lasting and delivered by intramuscular injection, may be of particular use in certain groups. This includes people who have compromised immune function, those who are over 80 years old, and people undergoing medical treatments that preclude them from receiving a COVID-19 vaccine.
October 28:
HHS announced a $375 million agreement with Eli Lilly and Company to purchase the first doses of the company's COVID-19 investigational antibody therapeutic bamlanivimab, also known as LY-CoV555. Bamlanivimab currently is being evaluated in Phase 3 clinical trials funded by Eli Lilly, in addition to clinical trials as part of the ACTIV public-private partnership. The FDA is reviewing bamlanivimab as a possible treatment for COVID-19 in outpatients. Monoclonal antibodies, which mimic the human immune system, bind to certain proteins of a virus, reducing the ability of the virus to infect human cells.
November 10:
HHS announced plans to allocate initial doses of Eli Lilly and Company's investigational monoclonal antibody therapeutic, bamlanivimab, which received emergency use authorization from the FDA on November 9, for the treatment of non-hospitalized patients with mild or moderate confirmed cases of COVID-19. A data-driven system will ensure continued fair and equitable distribution of these new products. Weekly allocations to state and territorial health departments will be proportionally based on confirmed COVID-19 cases in each state and territory over the previous seven days, based on data hospitals and state health departments enter into the HHS Protect data collection platform. To find out how much bamlanivimab has been allocated to specific states, territories, and jurisdictions, visit the allocation dashboard. This dashboard will be updated each distribution week until the FDA issues a revised EUA indicating the U.S. government involvement in the allocation and distribution process is no longer needed.
November 23:
HHS announced plans to allocate initial doses of Regeneron's investigational monoclonal antibody therapeutic, casirivimab and imdevimab, which received emergency use authorization from the U.S. Food and Drug Administration on November 21, 2020, for treatment of non-hospitalized patients with mild or moderate confirmed cases of COVID-19 at high risk of hospitalization. In July, the federal government announced federal funding to support large-scale manufacturing of the therapeutic with approximately 300,000 doses of the medicine expected to result from the project. HHS will allocate these government-owned doses equitably on a weekly basis to state and territorial health departments which, in turn, will determine which healthcare facilities receive the infusion drug. To find out how much of Regeneron's therapeutic has been allocated to specific states, territories, and jurisdictions, visit the allocation dashboard. This dashboard will be updated each distribution week until the FDA issues a revised EUA indicating the U.S. government involvement in the allocation and distribution process is no longer needed.
December 11, 2020:
HHS announced an agreement with Moderna to acquire an additional 100 million doses of their COVID-19 vaccine candidate, bringing the total doses of mRNA-1273 owned by the federal government to 200 million. Under the agreement, Moderna will leverage its U.S.-based manufacturing capacity to fill, finish and ship vials of mRNA-1273 as the bulk material is produced. The additional doses ordered today provide for continuous delivery through the end of June 2021. This federal funding brings the total provided to Moderna for this vaccine, including vaccine development, clinical trials and manufacturing, to $4.1 billion. The government also has the option to acquire up to an additional 300 million doses of the Moderna vaccine.
December 11, 2020:
The FDA issued an Emergency Use Authorization (EUA) for Pfizer-BioNTech’s COVID-19 vaccine candidate, allowing the vaccine to be distributed in the U.S. The totality of the available data provides clear evidence that the known and potential benefits outweigh the known and potential risks, supporting the vaccine’s use in millions of people 16 years of age and older, including healthy individuals. In making this determination, the FDA can assure the public and medical community that it has conducted a thorough evaluation of the available safety, effectiveness and manufacturing quality information. The Pfizer-BioNTech COVID-19 vaccine contains messenger RNA (mRNA), which is genetic material. The vaccine contains a small piece of the SARS-CoV-2 virus’s mRNA that instructs cells in the body to make the virus’s distinctive “spike” protein. When a person receives this vaccine, their body produces copies of the spike protein, which does not cause disease, but triggers the immune system to learn to react defensively, producing an immune response against SARS-CoV-2. Read more about the EUA.
December 18, 2020:
The FDA issued an Emergency Use Authorization (EUA) for Moderna's COVID-19 vaccine candidate, the second COVID-19 vaccine authorized for distribution in the U.S. The totality of the available data provides clear evidence that the known and potential benefits outweigh the known and potential risks, supporting the vaccine's use in millions of people 18 years of age and older. In making this determination, the FDA can assure the public and medical community that it has conducted a thorough evaluation of the available safety, effectiveness and manufacturing quality information. The Moderna COVID-19 Vaccine contains messenger RNA (mRNA), which is genetic material. The vaccine contains a small piece of the SARS-CoV-2 virus's mRNA that instructs cells in the body to make the virus's distinctive "spike" protein. After a person receives this vaccine, their body produces copies of the spike protein, which does not cause disease, but triggers the immune system to learn to react defensively, producing an immune response against SARS-CoV-2.
Select actions to support OWS manufacturing efforts so far include:
May
The May 21, April 16, and March 30 HHS agreements with AstraZeneca, Moderna, and Johnson & Johnson respectively include investments in manufacturing capabilities.
June
June 1: HHS announced a task order with Emergent BioSolutions to advance domestic manufacturing capabilities and capacity for a potential COVID-19 vaccine as well as therapeutics, worth approximately $628 million, using Emergent's BARDA-supported Center for Innovation in Advanced Department and Manufacturing.
July
July 27: HHS announced a task order with Texas A&M University and FUJIFILM to advance domestic manufacturing capabilities and capacity for a potential COVID-19 vaccine, worth approximately $265 million, using another BARDA-supported CIADM.
August
August 4: Grand River Aseptic Manufacturing Inc., (GRAM) Grand Rapids, Michigan, was awarded a $160 million firm-fixed-price contract for domestic aseptic fill and finish manufacturing capacity for critical vaccines and therapeutics in response to the COVID-19 pandemic.
October
October 13: HHS announced a $31 million agreement with Cytiva to expand the company's manufacturing capacity for products that are essential in producing COVID-19 vaccines, such as liquid and dry powder cell culture media, cell culture buffers, mixer bags, and XDR bioreactors. Cytiva is a major manufacturer of pharmaceutical consumables and hardware products and the primary supplier to many of the companies currently working with the U.S. government to develop COVID-19 vaccines. This capacity expansion will help Cytiva respond to the demand for COVID-19 vaccine consumables and hardware products without impacting on current manufacturing output.
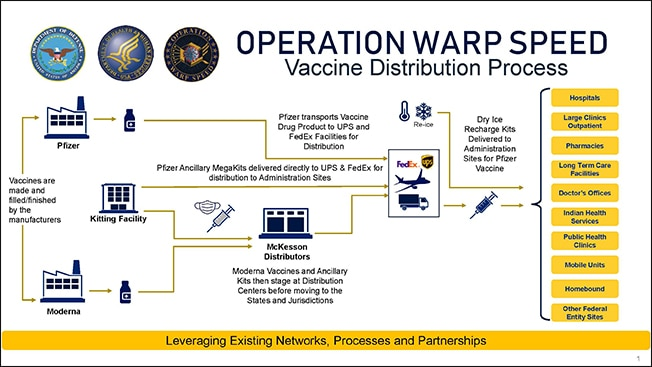
Distribution
OWS and our private partners are developing a plan for delivering a safe and effective product to Americans as quickly and reliably as possible. Experts from HHS are leading vaccine development, while experts from DoD are partnering with the CDC and other parts of HHS to coordinate supply, production, and distribution of vaccines.
Select actions to support OWS distribution efforts include:
May 12:
DoD and HHS announced a $138 million contract with ApiJect for more than 100 million prefilled syringes for distribution across the United States by year-end 2020, as well as the development of manufacturing capacity for the ultimate production goal of over 500 million prefilled syringes in 2021.
June 9:
HHS and DoD announced a joint effort to increase domestic manufacturing capacity for vials that may be needed for vaccines and treatments
June 11:
HHS announced $204 million in funds to Corning to expand the domestic manufacturing capacity to produce approximately 164 million Valor Glass vials per year if needed. Valor Glass provides chemical durability to minimize particulate contamination. The specialized glass allows for rapid filling and capping methods that can increase manufacturing throughput by as much as 50 percent compared with conventional filling lines, which in turn can reduce the overall manufacturing time for vaccines and therapies.
June 11:
HHS announced $143 million to SiO2 Materials Science to ramp up capacity to produce the company's glass-coated plastic container, which can be used for drugs and vaccines. The new lines provide the capacity to produce an additional 120 million vials per year if needed.
August 14:
HHS and DoD announced that McKesson Corporation will be a central distributor of future COVID-19 vaccines and related supplies needed to administer the pandemic vaccinations. The CDC is executing an existing contract option with McKesson to support vaccine distribution. The company also distributed the H1N1 vaccine during the H1N1 pandemic in 2009-2010.
The current contract with McKesson, awarded as part of a competitive bidding process in 2016, includes an option for the distribution of vaccines in the event of a pandemic. Detailed planning is underway to ensure rapid distribution as soon as the FDA authorizes one or more vaccines. Once these decisions are made, McKesson will work under CDC's guidance to ship COVID-19 vaccines to administration sites.
September 16:
HHS and DoD released two documents outlining the Trump Administration's detailed strategy to deliver safe and effective COVID-19 vaccine doses to the American people as quickly and reliably as possible. The documents, developed by HHS in coordination with DoD and the Centers for Disease Control and Prevention (CDC), provide a strategic distribution overview - PDF for state, tribal, territorial, and local public health programs and their partners on how to plan and operationalize a vaccination response to COVID-19 within their respective jurisdictions.
October 16:
HHS and DoD announced agreements with CVS and Walgreens to provide and administer COVID-19 vaccines to residents of long-term care facilities (LTCF) nationwide with no out-of-pocket costs. Protecting especially vulnerable Americans has been a critical part of the Trump Administration's work to combat COVID-19, and LTCF residents may be part of the prioritized groups for initial COVID-19 vaccination efforts until there are enough doses available for every American who wishes to be vaccinated. The Pharmacy Partnership for Long-Term Care Program provides complete management of the COVID-19 vaccination process. This means LTCF residents and staff across the country will be able to safely and efficiently get vaccinated once vaccines are available and recommended for them, if they have not been previously vaccinated. It will also minimize the burden on LTCF sites and jurisdictional health departments of vaccine handling, administration, and fulfilling reporting requirements.
November 12:
HHS and DoD announced partnerships with large chain pharmacies and networks that represent independent pharmacies and regional chains.
Through the partnership with pharmacy chains, this program covers approximately 60 percent of pharmacies throughout the 50 states, the District of Columbia, Puerto Rico, and the U.S. Virgin Islands. Through the partnerships with network administrators, independent pharmacies and regional chains will also be part of the federal pharmacy program, further increasing access to vaccine across the country—particularly in traditionally underserved areas.
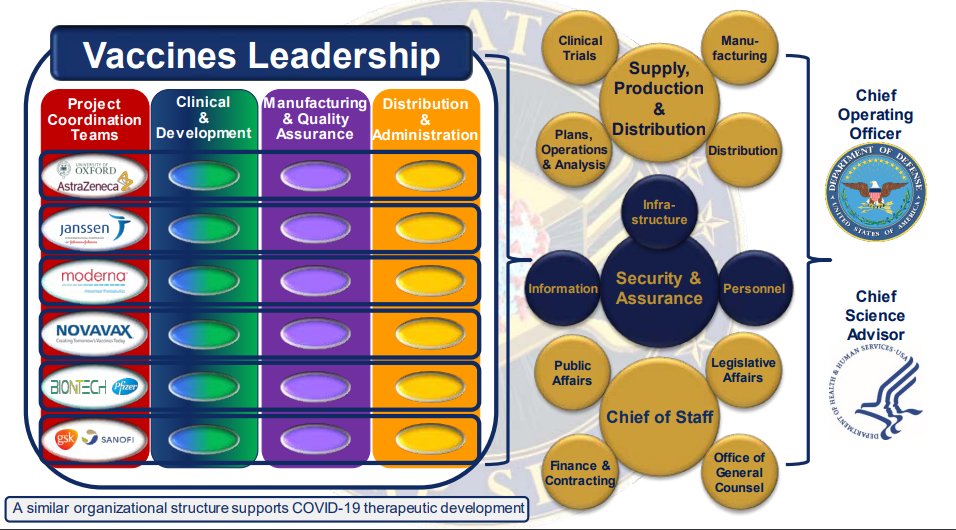
HHS Secretary Alex Azar and Acting Defense Secretary Christopher Miller oversee OWS, with Dr. Moncef Slaoui designated as chief advisor and General Gustave F. Perna confirmed as the chief operating officer.
To allow these OWS leaders to focus on operational work, in the near future the program will be announcing separate points of contact, with deep expertise and involvement in the program, for communication with Congress and the public.
Congress has directed almost $10 billion to this effort through supplemental funding, including the CARES Act. Congress has also appropriated other flexible funding.
The almost $10 billion specifically directed includes more than $6.5 billion designated for countermeasure development through BARDA and $3 billion for NIH research.
public3.pagefreezer.com/cont…
12 Dec 2023
THE SHOT HEARD AROUND THE WORLD~ @RandPaul @RepThomasMassie @LmBubba @I_Am_JohnCullen @Leeshotfury1966
According to news accounts, the virus so far had infected only 41 people and killed one. The story in The Washington Post about it that morning was buried inside the paper.
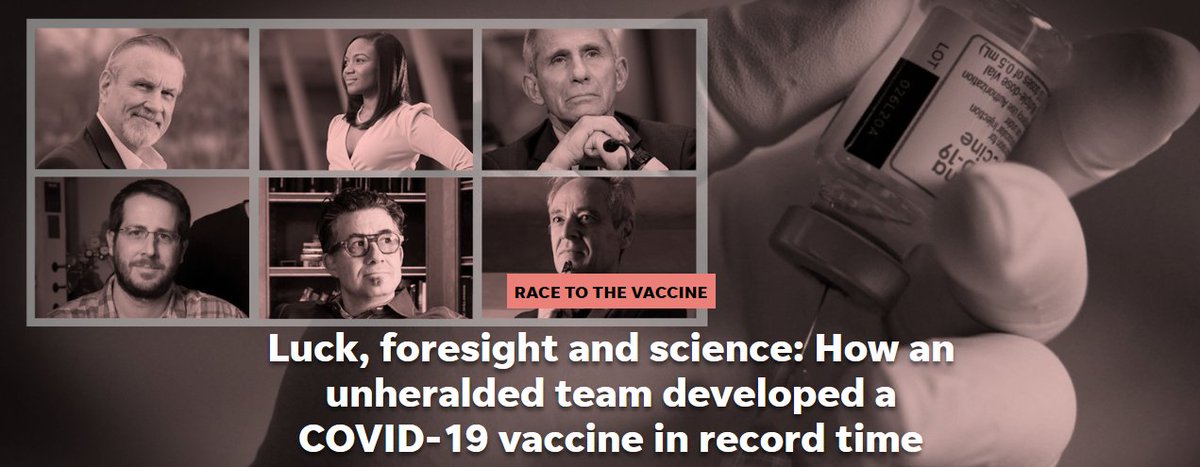
RACE TO THE VACCINE
Luck, foresight and science: How an unheralded team developed a COVID-19 vaccine in record time.
Dr. Anthony Fauci, who had quickly become the voice of the scientific community, was already predicting a vaccine within as little as a year, a projection many of his colleagues considered wildly optimistic.
But Fauci knew something many did not. Members of his team at the National Institutes of Health and an affiliated biotech company had been preparing for years for just this moment, just this vaccine. The liquid about to go into Haller’s arm was the culmination of years of research by a handful of scientists who, by virtue of incredible luck and incredible foresight, were prepared for one virus more than almost any other: a coronavirus.
Had this virus come 10 years earlier – or even five – science would not have been ready.
At the start of the pandemic, no one could have foreseen how controversial a COVID-19 vaccine would become – that the country would soon be stewing in anti-science and anti-vaccine sentiment, awash in misinformation and cleaved by mistrust.
A pharmacist in an N95 mask, protective goggles and blue latex gloves held up a syringe labeled with an expiration a few hours away. The photographers focused their lenses on Haller’s shoulder. The needle slid in.
The experiment had begun.
Donald Trump credited his Operation Warp Speed for the fast development of the vaccine, and marshaling the resources of public health agencies no doubt played a critical role. So did committing $9 billion for human trials and manufacturing the vaccine even before it was tested, banking on a green light from the U.S. Food and Drug Administration.
But the real credit for the rapid turnaround belongs to a series of uncelebrated discoveries dating back at least 15 years – and a constellation of unsung scientists.
Chief among them is Barney Graham, now 67, who had spent much of his career trying to understand why two infants died in a disastrous 1966 vaccine trial for a virus that remains the leading cause of hospitalization for young children. The tragedy slowed the development of a vaccine for respiratory syncytial virus (RSV) for decades, and it haunted Graham. He continued his research for 31 years until, in 2013, he had a major breakthrough – one that would become vital to developing a COVID-19 vaccine.
In recent years, as deputy director of the National Institutes of Health’s Vaccine Research Center, Graham’s mission had been to make a vaccine fast enough to stop a pandemic. He was looking for a good virus candidate.
Graham had gotten close once before when the mosquito-borne Zika virus reached the U.S. in 2016.
The Zika vaccine candidate held the speed record for getting from initial research into a clinical trial – roughly seven months – but that pandemic subsided before Graham could complete the small trial, leaving the world with no vaccine for Zika.
At the end of 2019, Graham was months into plans to make another vaccine at supersonic speeds. He had chosen a brutal virus called Nipah that inspired the 2011 film “Contagion.” Spread by bats, it last broke out in India in 2018, killing 17 of the 19 people it infected in Kerala.
Though he's reflexively modest, Graham had a bold goal. He’d even picked a biotech company to make the Nipah vaccine: Moderna. During the Zika experiment, Moderna had developed a vaccine 10 times more potent than the DNA vaccine Graham himself had created. It relied on messenger RNA, sometimes called the “software of life” because it carries out the instructions of our DNA. In a vaccine, mRNA instructs our bodies to produce just a piece of the virus, the protein on its surface.
Although in its decadelong existence Moderna had never brought a vaccine to market, it had tested several experimental vaccines in a dozen small clinical trials.
As Graham got word through back channels that the new virus in China was probably a coronavirus, he reached out to Moderna’s CEO, who was vacationing in France. We should scratch the Nipah plan, he urged Stephane Bancel in a Jan. 6 email, in favor of a different proof of concept related to the Wuhan outbreak.
“If it’s a SARS-like coronavirus, we know what to do,” Graham wrote. “This would be a great time to run the drill for how quickly can you have a scalable vaccine.”
Graham later laid out the idea for Fauci, his boss’s boss, in a conference room at NIH. Fauci is no micromanager; he hadn’t even been aware until then how confident Graham was in his ability to make a coronavirus vaccine.
There had been two other novel coronaviruses since 2003, although neither SARS nor MERS were terribly contagious and neither became pandemics. In early January, there was no reason to assume COVID-19 would be any different. Yet Graham already had his team diving into how to defeat the new coronavirus just to prove it could be done. Fauci was sold.
“Let’s go full-blown,” he said. “Let’s make a vaccine.”
Fauci had already set aside $5 million for the small Nipah demonstration project. Graham asked if there would there be millions more available.
“Barney, let me worry about the money,” Fauci replied.
If everything went perfectly, Graham said a vaccine could be ready within 12 to 18 months – the prediction Fauci would soon make public.
CLOSE TO MIDNIGHT on Jan. 10, Graham was relaxing at his suburban Maryland home when he finally got the news he’d been expecting: Chinese scientists had posted the genetic sequence for what they called the “Wuhan seafood market pneumonia virus.”
Early the next morning, Graham fired up his laptop in his home office, overlooking his front yard. He navigated to a website used by scientists worldwide to share information and saw hundreds of rows of four letters – a, c, g and t – that revealed the virus’s unique identity. The reports were true. It was a novel coronavirus, SARS-CoV-2, a new version of a family of infectious diseases.
Graham began texting, emailing and calling a handful of close associates. He reached one, a former NIH scientist now at the University of Texas, Jason McLellan, just back from a Utah ski trip. Another was a rising star he had known since she was a teenager, when she applied for an internship. Kizzmekia Corbett had been working in Graham's lab since 2014, studying the best way to defeat coronaviruses with a vaccine.
The team began to tailor a vaccine to the new coronavirus. They had a big head start, having experimented on coronavirus vaccines in mice for years in collaboration with Moderna. The work happened on laptops, not in labs.
Graham convened over the phone with scientists at Moderna two days later to sketch out the road map. Moderna would produce the vaccine, using the genetic code Graham provided. It would be the only vaccine for which the government would lead the first clinical trial, a trial Graham wanted to launch in a matter of weeks.
On Jan. 27, a year ago today, Dr. Lisa Jackson at Kaiser Permanente Washington in Seattle learned that she would oversee that trial. Jackson dropped all her other work to focus on the vaccine.
Graham had spent much of his career at Vanderbilt University, where he focused on HIV as well as RSV. He brought that work with him to NIH when he was recruited there in 2000.
RSV sends as many as 125,000 children to the hospital each year. It also holds a special place in the history of vaccines. In one clinical trial in 1966, 31 infants were given the trial vaccine. Twenty of them later caught the disease. Of those, 16 ended up in the hospital and two died.
When MERS broke out in Saudi Arabia in September 2012, his team, including McLellan, immediately began researching the structures of proteins on coronaviruses.
McLellan continued to work with Graham to identify the spike protein on coronaviruses, even after he moved on to Dartmouth College and later the University of Texas. By 2017, they had figured out how to defeat coronaviruses with a vaccine and published a major scientific article, one that nearly all vaccine makers would one day rely on for COVID-19.
Subsequently, Corbett at NIH worked with others to test possible vaccines, with a special focus on MERS, also known as camel flu. Working with Moderna, she helped inject mice, then drew blood to test for antibodies.
That preparation left them ready when another novel coronavirus appeared.
Haller’s shot marked an enormous milestone for Graham and his team. It had been only 66 days since the Chinese posted the genetic sequence.
They had proven that vaccines can be ready for human tests quickly. Graham remained fully confident in the vaccine, later confiding to a reporter that at that point he already expected it to be about 80% effective.
If he turned out to be right, expectations about the speed of vaccine development would change forever.
A key part of the analysis, being done largely at Vanderbilt University, was to test the subjects’ blood samples for antibodies that would block the virus. That data was discussed in regular conference calls with Graham and the team at NIH, along with others involved in analyzing the data.
Accounts vary on exactly when the researchers knew the trial was a success. Anderson remembers seeing the data on his computer; Jackson remembers hearing about it in a conference call.
Graham pegs it to an email from researchers at Vanderbilt on May 9. They had the results of antibodies examined from the first eight volunteers, including Haller. The tall S curves on the chart told the story – the higher the top of the S, the better. When Vanderbilt researchers took antibodies from the volunteers’ blood and tested them on infected cells in the laboratory, the virus stopped replicating.
Graham was expecting the vaccine to produce neutralizing antibodies, but not this strong. The highest dose tested was dropped because it produced the most side effects, including fever, but otherwise there were no major safety concerns.
In a conference call with all the key players, the team gave each other verbal high fives – “Wow!” and “Thank you!” – for a job well done.
If a COVID-19 vaccine was going to be available as soon as possible, the U.S. government was going to have to open the Treasury to pay for research, buy doses in advance and get the manufacturing started on spec, well before the vaccines were even up for approval. It did. Two weeks after Dolly Parton made her Instagram news, on April 16, the Department of Health and Human Services pledged to spend $483 million on the Moderna vaccine. Later, it would add another $472 million to pay for the trial.
Other vaccines in development could save millions of lives each year worldwide with similar infusions of funds. When asked why so much money was being poured into a COVID-19 vaccine, Corbett, one of the leaders of vaccine development at NIH, said, “I don’t really have an answer other than people are dying. And also, frankly, people in the United States are dying, which changes a lot.”
Having fully taken the reins from Graham and his colleagues, the company now needed to recruit 30,000 people – a massive number set by the FDA – which Bancel estimated would take up to eight weeks. Infection rates would determine when they would have results; the worse the outbreak, the faster they would have data showing whether the vaccine worked.
“October, maybe November,” Bancel said. “It’s tough to know right now.”
Bancel had been CEO since October 2010, recruited by venture capital firm Flagship Ventures to run the company it recently had funded. A chemical engineer with an MBA from Harvard, Bancel had held the top job at a French biotechnology company, BioMérieux, at 36 and pushed the company to dramatically increase its market share. Bancel flew to Boston and was intrigued by the idea of leading a company that could revolutionize medical science. He talked to his wife about it and said, “Look, this could change the world.”
Early employees describe Bancel as focused on filing patents. Once he realized there were 22,000 proteins in the human body, one employee said, he wanted his scientists to produce as many as possible – regardless of their scientific significance – to corner patents on RNA technology. In meetings, Bancel would stand before a whiteboard and often curse at his staff. Resignations, firings and poor reviews on Glassdoor followed.
Bancel was an excellent evangelist for the company, though. In a 2013 TED talk, he predicted based on mouse studies that RNA could regrow damaged heart tissue after a cardiac arrest – research that Moderna is working on today in collaboration with AstraZeneca.
The message was clear: Moderna intended to revolutionize medical science.
Moderna owes its existence to a Harvard professor, Derrick Rossi. Both Moderna and BioNTech also were built upon the discoveries of two researchers at the University of Pennsylvania, Kaitlin Kariko and Drew Weissman.
The stories of the three academic scientists weave together. But while Kariko now works for BioNTech and Weissman is consulting for the company, Rossi has largely been written out of Moderna’s history.
I highly encourage you to read the full article-!!!
kpwashingtonresearch.org/new…
usatoday.com/in-depth/news/i…
wtamu.edu/_files/docs/resear…



30
34
59
9,794
There has been a massive interruption in routine immunizations for kids. Watch our #TEDMEDconversations with Ed Kelly, PhD, Chief Global Health Officer, Apiject Systems Corp., and Kelly Thomas, PhD, Director of Scientific Content, TEDMED.
Full Video: youtu.be/byHR1YPFUl0?si=q1x8…
1
1,153

23 Oct 2023
Bo Kowalczyk, the Chief Commercial Officer at ApiJect, a global medical technology company creating the future of pharmaceutical injections, discusses sterile fill and finish market trends, and ApiJect’s platform technology.
Sponsored by @ApiJectCorp
2
2,415
How has the pandemic shaped positive change in product design? The answer is in this #TEDMEDconversations with Heidi Larson, MA, PhD, and Marc Koska, OBE, Co-Founder of Apiject. #TEDMED #Covid #ProductDesign #ProductDevelopment
Full Video: youtu.be/4cizO9eRgYw?si=Gqk3…
1
1,274
People thought technology helped them during COVID. Heidi Larson, MA, PhD, Professor of Anthropology & Risk, and Marc Koska, OBE, Co-Founder of Apiject, discuss how it did impact us. #TEDMEDconversations #TEDMED #Covid19 #ProductDesign #ProductDevelopment
youtu.be/4cizO9eRgYw?si=4m_e…
1
1,318
We are hopeful for advances in the future of therapeutic design. Watch our #TEDMEDconversations with Heidi Larson, MA, PhD, Professor of Anthropology & Risk, and Marc Koska, OBE, Co-Founder of Apiject. #Covid #ProductDesign #ProductDevelopment
Watch here: youtu.be/4cizO9eRgYw?si=PGNT…
2
1,235
What is necessary for good product design? Watch our #TEDMEDconversations with Heidi Larson, MA, PhD, Professor of Anthropology & Risk, and Marc Koska, OBE, Co-Founder of Apiject. #TEDMEDcommunity #TEDMED #Covid #ProductDesign
Full Video: youtu.be/4cizO9eRgYw?si=9YR_…
2
1,237
Successful product design needs to understand where the product is going to land. Watch our #TEDMEDconversations with Heidi Larson, MA, PhD, Professor of Anthropology & Risk, and Marc Koska, OBE, Co-Founder of Apiject. #Covid19 #ProductDesign
Full Video: youtu.be/4cizO9eRgYw?si=wniX…
1
929
Incorporating anthropology early in the design phase is critical. Watch our #TEDMEDconversations with @ProfHeidiLarson, MA, PhD, Professor of Anthropology & Risk, and @marckoska, OBE, Co-Founder of Apiject. #Covid19 #ProductDesign #MedicalAnthropology
youtu.be/4cizO9eRgYw?si=lZmm…
3
984
What did COVID teach us about product design? Watch our #TEDMEDconversations with @ProfHeidiLarson MA, PhD, Professor of Anthropology & Risk, and @marckoska OBE, Co-Founder of Apiject. #TEDMEDcommunity #Covid19 #ProductDesign #ProductDevelopment
youtu.be/4cizO9eRgYw?si=G6cM…
1
837
