
Nobody brought up flashy passes but you. And by you assuming my use of the word “Dimer” as flashy passes you typed this whole comment not knowing you wrong lmaooo
2
メゾヒエラルキーの物質科学【学術変革領域研究(A)】 retweeted

[カバー紹介][Editor's Choice]
biradical, imidazole dimer, negative photochromism
阿部二朗先生 @AoyamaGakuinU (青山学院大学)
#OnTheCover #FreeAccess
academic.oup.com/chemlett/ar…
8
481
Materials Science of Meso-Hierarchy retweeted
[Editor's Choice]
biradical, imidazole dimer, negative photochromism
Article by Prof. Jiro Abe @AoyamaGakuinU (Aoyama Gakuin University)
#OnTheCover #FreeAccess
academic.oup.com/chemlett/ar…

4
3
511

Bunu her yerde söylüyorum ama herkes 6 ayda bir D- dimer kan tahlili yaptırsın . Bu tahlil kan da ki pıhtı düzeyini belirliyor
24

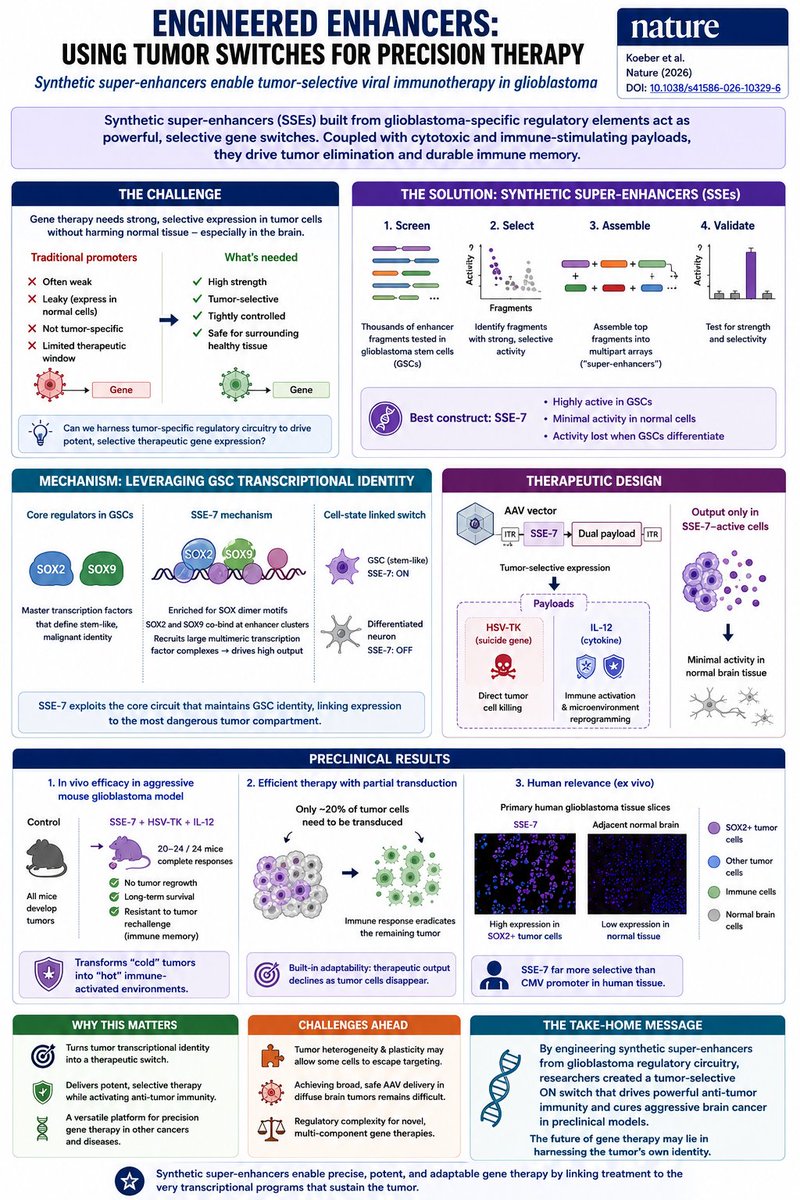
What if a tumor could activate its own destruction?
A new Nature study introduces a powerful concept:
Synthetic super-enhancers (SSEs) engineered from tumor-specific regulatory circuitry can function as highly selective genetic ON switches inside cancer cells.
The team focused on glioblastoma, one of the most lethal brain cancers.
Instead of targeting a mutation, they targeted a cell state.
The key insight
Glioblastoma stem cells (GSCs) depend on a core transcriptional network centered on:
• SOX2
• SOX9
These factors define the stem-like, therapy-resistant tumor compartment.
Researchers screened thousands of enhancer fragments, identified those selectively active in GSCs, and assembled them into multipart synthetic super-enhancers.
The best construct:
SSE-7.
Why SSE-7 is different
Traditional promoters are often:
❌ weak
❌ leaky
❌ insufficiently selective
SSE-7 behaved more like a biological logic gate:
Tumor stem cell state → ON
Normal differentiated brain cells → OFF
Its activity rapidly disappeared when GSCs differentiated, linking expression directly to the malignant stem-like state.
Mechanism
Biochemical and genomic analyses revealed:
SOX2 SOX9 cooperate at enhancer clusters enriched for SOX dimer motifs.
SSE-7 recruits large multimeric transcription-factor complexes and integrates developmental and signaling-state inputs.
In essence:
tumor identity becomes the switch.
Turning the switch into therapy
The investigators loaded SSE-7 into an AAV vector carrying two payloads:
🧨 HSV-TK (suicide gene)
🔥 IL-12 (immune-stimulating cytokine)
Only cells activating SSE-7 expressed the payload.
The result:
Tumor cells killed themselves.
At the same time, IL-12 converted the tumor microenvironment from immunologically “cold” to “hot,” activating antitumor immunity.
The preclinical outcome
In an aggressive syngeneic glioblastoma mouse model:
• established tumors regressed rapidly
• 20–24 of 24 treated animals achieved complete responses
• no tumor regrowth was detected during long-term follow-up
• mice resisted subsequent tumor rechallenge, indicating durable immune memory
One of the most striking observations:
Only ~20% of tumor cells needed to be transduced.
The immune response eliminated the remaining disease.
Human relevance
In ex vivo human glioblastoma tissue slices:
SSE-7 activity was strongly enriched in SOX2-positive tumor cells and markedly reduced in adjacent normal brain tissue.
Compared with a constitutive CMV promoter, expression became dramatically more tumor-restricted.
Why this matters
Most cancer gene therapies try to target:
a mutation
or
a surface marker.
This study targets something deeper:
the transcriptional identity of the tumor itself.
The broader implication is exciting:
If tumor-specific enhancer circuitry can be mapped,
then synthetic super-enhancers could become programmable genetic switches for:
• cancer-selective immunotherapy
• cell-state–specific gene therapy
• precision delivery of toxic payloads
• adaptive tumor microenvironment reprogramming
The future of oncology may not simply be finding new drugs.
It may be engineering gene circuits that activate therapy only where the cancer is.
Reference
Koeber et al. Synthetic super-enhancers enable precision viral immunotherapy. Nature (2026). DOI: 10.1038/s41586-026-10329-6.
1
32

Midlevel asks if I can see the patient before she’s about to discharge
Just in case I think she should add on a d-dimer
1
4
872


11h
Part -7
🔸I've been taking Nattokinase for 26 years, at the recommendation of my MD, for preventative measure when diagnosed with Atrial Fibrillation. I have done very well all these years, no longer have episodes of a-fib and last years my tests showed absolutely no calcifications in my cardiovascular system...at the age of 71. I have no bruising on my skin and if there is some indication of bruising or bleeding longer than usual, I cut back on my 7 days a week dose for a while. Wish I could find out the desired and recommended dose, but still have done very well after having taken it for so many years. I've had noundesirable side effects ever from this supplement!
🔸I’m in my 30’s, not overweight, and have had no previous cardiac issues. After my second exposure to covid, I started having tachycardia. I ended up going to the ER and had hallmark signs of covid as well as an elevated d-dimer, though no blood clots were found. I started taking nattokinase 4000FU a day and I strongly believe it is what brought my heart-rate back down to normal. It no longer gets randomly high throughout the day and doesn’t shoot up during exercise like it was before.
1
32

Damian Lillard
6’2 DEEP-RANGE SHOT CREATOR
💎HOF
• Limitless Range
• Agent 3
🥇GOLD
• Handles For Days
• Deadeye
• Space Creator
🥈SILVER
• Dimer
🎞️ FILM NOTES
• One of the best deep shooters ever
• Elite late-game shot creator
What badge would you upgrade?
37



The medical authorities told doctors not to do D-Dimer tests for micro-clotting after the covid 19 death jab.
Fore-knowldge is evidence of a crime.
Police please a bring a case to court.
10

Covid in 2012. 6 patients.
Patient 1 (63 years old): Admitted April 26, 2012 after 14 days in the mine. Developed fever, dry cough progressing to bloody sputum, dyspnea, aching limbs, and headache. Rapid progression to severe interstitial pneumonia with ground-glass opacities. Died after 12 days in hospital on May 7, 2012 from respiratory failure.
Patient 2 (42 years old): Admitted April 25, 2012 after 14 days exposure. Similar symptoms: high fever, cough with sputum, severe breathing difficulty. Progressed to ARDS requiring mechanical ventilation, lymphocytopenia, elevated D-dimer, and pulmonary thromboembolism. Died after 48 days on June 12, 2012.
Patient 3 (45 years old): Admitted April 27, 2012 after 14 days in the mine. Severe symptoms including persistent high fever, productive cough, profound dyspnea. Longest hospitalization among the deceased at 109 days. Developed ARDS, immune cell depletion, and complications leading to death on August 13, 2012.
Patient 4 (46 years old): Admitted April 26, 2012 after 14 days exposure. Severe course with fever, cough, dyspnea, ARDS requiring mechanical ventilation, clotting issues, and low oxygenation. Underwent thymectomy on June 27, 2012. Survived after 137 total days, discharged improved on September 10, 2012.
Patient 5 (30 years old): Admitted May 2, 2012 after only 5 days in the mine. Milder symptoms of fever, cough, and fatigue. Shorter course with lymphocytopenia but no ventilation needed. Discharged alive after 26 days on May 28, 2012.
Patient 6 (32 years old): Admitted April 26, 2012 after 4 days exposure. Similar mild symptoms to patient 5. Recovered steadily and discharged after 32 days on May 28, 2012.
Summary: All patients shared initial symptoms of fever, cough, dyspnea, myalgia, and headache after cleaning bat guano.
Older patients with longer exposure (patients 1-4) developed severe bilateral interstitial pneumonia, ground-glass opacities, ARDS, lymphopenia, and secondary infections. The three oldest died from respiratory failure or related complications. The two youngest had shorter, milder illnesses and recovered quickly. Patient 4’s survival despite severity is notable due to extended supportive care including ventilation, antithrombotics, and thymectomy.

How Covid was treated in 2012. 6 patients.
All patients: ganciclovir antiviral, acyclovir antiviral, methylprednisolone steroid, meropenem antibiotic, vancomycin antibiotic, caspofungin antifungal, fluconazole antifungal.
Patients 2, 3, 4: mechanical ventilation.
Patients 2 and 4: warfarin antithrombotic, low molecular weight heparin antithrombotic.
Patient 4: thymectomy performed on June 27, 2012 and survived.
Patients 1, 2, and 3 deceased.
Patients 4, 5, and 6 survived.
2
1
11
1,014

Resolving a decades-long puzzle: what integrins in the cell junction are doing without classical extracellular matrix ligands: doi.org/10.1172/JCI190552
Pipsa Saharinen & team present angiopoietin-2 (ANGPT2) in complex with the TIE2 receptor tyrosine kinase and α5β1-integrin via advanced structural biology techniques.
The cover image shows a trimeric complex of ANGPT2 dimer bound to TIE2 and integrin α5 domains via asymmetric fibrinogen like domains. Image credit: Pipsa Saharinen, Kumar Ponna and Martina Trevisani.
#LymphaticEndothelium

2
4
15
1,566

4- Senin sisteminde prokoagülan eğilim var mı?
Kanında trombin üretimi artıyor mu?
Fibrinojen yüksek mi?
D-dimer anlamlı mı?
Trombositler yüksek, düşük veya fonksiyonel olarak aşırı aktif mi?
CRP/ferritin gibi inflamasyon belirteçleri pıhtılaşmayı besliyor mu?
Homozistein yüksek mi?
Lipoprotein(a) yüksek mi?
Antifosfolipid antikorları var mı?
Protein C, protein S, antitrombin III eksikliği var mı?
Faktör V Leiden veya protrombin mutasyonu gibi genetik zemin var mı?
HbA1c, insülin direnci, trigliserid, ürik asit, karaciğer yağlanması endoteli bozuyor mu?
3
42
3,933
3- 3. Trombin–fibrin sistemi fazla mı çalışıyor?
Pıhtının merkezinde trombin vardır. Trombin artarsa fibrinojen fibrine döner, fibrin ağı oluşur ve damar içinde pıhtı iskeleti kurulur. Bu yüzden D-dimer, fibrinojen, PT, aPTT, trombosit sayısı gibi testler bize sistemin nereye eğildiğini gösteri

1
2
41
2,717