

Jun 13
Cardiac therapy is entering a delivery-first era.
Many advanced therapies for cardiovascular disease already exist—small molecules, biologics, siRNA, mRNA, CRISPR systems, extracellular vesicles, AAV gene therapy, and nanoparticles.
But the bottleneck is simple:
How do we get the therapy to the heart, and not the liver/spleen?
A new European Heart Journal state-of-the-art review summarizes the emerging toolkit for cardiac-targeted delivery.
Core strategies:
Intracoronary delivery
Direct catheter-based delivery can raise local myocardial exposure, especially during PCI, but it remains invasive and difficult to repeat.
Cardiotropic AAV vectors
AAV9/SERCA2a, AAV-LAMP2B, MOG1, SOCS3, VEGF/Ang1, and CRISPR-based approaches show promise, but translation is limited by immune responses, liver uptake, dose toxicity, and packaging constraints.
Extracellular vesicles
EVs can be engineered with cardiac-homing peptides or membrane cloaking to increase uptake in cardiomyocytes, fibroblasts, and ischemic myocardium.
Microbubbles ultrasound
Ultrasound-targeted microbubble destruction enables local release of genes, drugs, or cells with spatial control.
Nanoparticles
Lipid, polymeric, metallic, inorganic, and nanomotor platforms are being designed for mRNA/siRNA delivery, anti-fibrotic therapy, anti-inflammatory targeting, and cardiac repair.
The key insight:
Cardiac targeting is not just “organ delivery.”
It requires three levels of precision:
heart accumulation → disease-region localization → cell-type-specific delivery
The future of cardiovascular therapeutics may depend less on discovering one more drug, and more on engineering the right delivery system:
right payload,
right cardiac compartment,
right cell type,
right timing.
Reference:
Liu et al. “Cardiac-targeted delivery of advanced medical therapies for heart disease.” European Heart Journal 2026. DOI: 10.1093/eurheartj/ehag432.

3
12
403

You're in denial cause you can only see labels. You can't accept Ventura as ugly cause that would undermine your whole woke pyramid structure.
You are rejecting reality for your own microbubble of slacktivism.
Let ugly characters be called ugly.
37
SonoThera retweeted

Jun 11
'Microbubble" gene therapy startup SonoThera raises $125 million bizjournals.com/sanfrancisco… via @SFBusinessTimes
1
2
46

Jun 9
Nivea Bright Oil Clear 5 in... thaiglowstore.com/products/n… via @https://x.com/ThaiGlowStore
✨ Say hello to a fresh cleansing experience with NIVEA Bright Oil Clear 5 In 1 Microbubbles Deep Clean Foam. Rich microbubble foam helps leave your skin feeling clean, smooth, and refreshed after every wash.
#FacialCleanser #FreshSkin #Skincare
32
Clay Davenport retweeted

Jun 6
An example of microcavitation or microbubble formation due to rapid contractile motion of the LAA- visualized during a Concomitant procedure. Typically seen as a dense cloud of bright whites dots that dissipate rapidly as they move away from the source. #epeeps #LAAC
2
9
768


Sebze ve meyvelerde maksimum hijyen,
Ozon gazı ve microbubble pompa teknolojisi ile artık mümkün.
🧪 Daha yüksek dezenfeksiyon,
💧 Homojen ve etkili yıkama.
Microbubble teknolojisi sayesinde ozon gazı-su karışımı en verimli seviyeye ulaşır.
#GıdaGüvenliği #OzonTeknolojisi

1
1
16
𝙼𝚘𝙼𝚘𝚖𝚎𝚊𝚠 |ωΦ) retweeted

Jun 4
wts
- Avocado Super Boost Microbubble Foam
- mami Rice Happy Bright Microbubble Foam
ซื้อแยก หลอดละ 175 บาท
เซ็ทละ 350
(ส่งฟรี)
สนใจ DM
#MamiFirstHappyMomentWithTui
#MamixTuiChayatorn #ช้อปช่วยติ่ง #ส่งต่อเครื่องสำอาง


2
1
2,305

Jun 4
FARMSTAY Collagen Facial 2 In 1 Bubble Wash & Mask | Gentle Microbubble Pore Cleansing Makeup Remover Daily Facial Non-Irritating Comfortable Long Lasting Hydration Korean Skincare, 3.38 Fl Oz
verifiedpricedrops.com/farms…

13

Jun 3
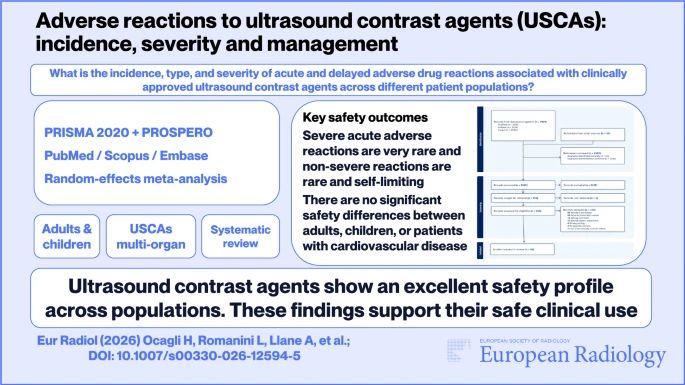
If contrast agents had a “gentle giant” category, would ultrasound microbubbles be in it? 🫧🩻
An exhaustive systematic review and meta-analysis of 74 studies encompassing over one million adults and 36,000 children evaluated the incidence of adverse drug reactions across all clinically approved microbubble agents. The data confirms an exceptional safety profile, demonstrating that severe acute reactions occur in just 6 per 100,000 adults and 16 per 100,000 children, with no significant safety differences between contrast brands or high-risk cardiovascular populations.
"I highly recommend bookmarking this definitive safety review to confidently guide and support your daily contrast-enhanced ultrasound protocols. This paper strongly reinforces CEUS as a safe and valuable contrast-enhanced imaging option, but also reminds us that “very safe” does not mean “no preparation needed”. Clear protocols and readiness for rare severe reactions remain essential." - Amit Gupta
buff.ly/LCfBlyK (Honoria Ocagli et al.)
1
78

#JCardiol 87(5): 459-67, 2026
Therapeutic ultrasound...
Highlights 1/3
☑️Ultrasound–microbubble therapy enhances reperfusion in acute myocardial infarction.
☑️Sonothrombolysis dissolves thrombi, while sonoperfusion restores microvascular flow.
doi.org/10.1016/j.jjcc.2026.…
by A.E. K
52

Groundwater oxidization by microbubbles for sand filtration
#microbubble #oxidization
1
19

Microbubble hull tech proves a simple drag-reduction idea can cut shipping fuel use by up to 10%, making maritime transport far more efficient and lower-emission.
1
82

May 29
I know. The dark nasty goose poop, algae coated pool was so much better than a beautiful blue reflective, microbubble enhanced reflecting pool. 🙄
1
48
386

May 28
สนุก สดชื่น และเต็มไปด้วยพลังดีๆ ตลอดงาน mami GRAND OPENING—the feel-good moment ในฐานะพรีเซ็นเตอร์โฟมล้างหน้ามามิ Avocado Super Boost Microbubble Foam
So fresh and full of good energy!
ขอบคุณที่มาสนุกกันครับ
FUN. FRESH. FREE. NATURALLY.

38