
1. The first clip is arguably the most mainstream position, given the woman in the first video (Johanna Olson-Kennedy) is the current president of USPATH. I assume you know she refused to publish the results from a 2015 $10m NIH-funded study on puberty blockers; in 2024 she told the NYT she was delaying because she was worried the results would be "weaponized by opponents of gender-affirming care". The preprint of that study from May 2025 confirmed a null result — "trans kids" showed no significant improvement in mental health after 2 years on puberty blockers.
2. Regardless of whether Webberley is right — you and I both agree she isn't — she runs GenderGP. She's got her LLM "Genni" diagnosing kids with "gender dysphoria" over the internet, and she's medicalizing those kids, shipping puberty blockers and hormones around the world based on her clearly anti-scientific understanding.
3. You say "just a puberty blocker", but the president of USPATH didn't publish results because she knew they would be cited to stop kids from being put on puberty blockers. Surely you agree that that's very obviously motivated by ideology, not scientific rigor?
4. Jamie's story has been corroborated by multiple other people and attested to under oath.
1
1
34

CALLING FOR URGENT FEDERAL INVESTIGATION INTO WPATH
A thoroughly researched paper by E. Jensen examines whether the World Professional Association for Transgender Health (WPATH), the organization whose guidelines shape gender medicine practice worldwide, is experiencing what safety science calls an "organizational failure," meaning it is unable to recognize or fix ongoing safety problems. Initially submitted for review in February 2024, the paper has been expanded to a book, soon to be published by Paradox Press @pdxinstitute. We summarize with some key points in hopes that it sheds more light on the operations of WPATH.
WHAT IS AN ORGANIZATIONAL SAFETY FAILURE?
In workplace safety, when something goes wrong, investigators look for "root causes" or root cause analysis of the deeper organizational problems that allowed the incident to happen, not just the immediate event (OSHA, 2016). An organization in failure mode is one where root causes are either never identified or never fixed. This paper identifies six warning signs of this, illustrated with well-known examples:
- Ignoring science: Decisions are made that go against available evidence, often due to biases like confirmation bias (only seeing what supports existing beliefs) or the "halo effect" (trusting information from favored people regardless of its quality) (NSF, 2023).
- Blocking investigation: When problems are identified, the organization either prevents investigation or conducts a flawed one. The Rotherham child exploitation scandal is cited: approximately 1,400 children were sexually exploited over 16 years while a researcher who documented the problem had her funding cut for "implementation problems" (Alexis Jay OBE, 2014).
- Punishing those who speak up: Disagreement is silenced rather than addressed. The Boeing 737 MAX is cited: rather than fixing a known dangerous system (MCAS), Boeing and FAA personnel punished whistleblowers and obstructed investigations (Commerce Committee Majority Staff, 2020). The 1900 Galveston hurricane is another example: Cuba's weather service warned the US, but their communications were cut off because officials found the information unclear (Larson, 1999).
- Conflicts of interest: Leaders cannot objectively evaluate situations because of personal stakes: financial, relational, or otherwise (Emory A. Rounds, III, 2022).
- Training only from within: When leaders learn only from their own organization, they develop blind spots. Safety protocols fail to adapt to change, and a false sense of security develops.
- Dismissing or mistreating those affected: People harmed by the failure are ignored, mocked, or treated with condescension, preventing the problem from being recognized (John L. Bryan, 2008; Yates, 2015).
HOW DOES THIS APPLY TO "GENDER MEDICINE"?
This paper then examines WPATH's Standards of Care version 8 (SoC8, Coleman et al., 2022) through each of these warning signs.
Who Actually Needs These Treatments?
The paper points out that there is no objective test, no blood test, scan, or measurable characteristic, to determine who has a "gender identity" that will benefit from medical treatment. Diagnosis is based entirely on what the patient reports. More importantly, there is no way to predict whether someone's gender identity will remain the same after treatment. "Gender fluid" is a consideration, as well as "non binary". This matters because many of these treatments cause permanent changes to the body, including potential effects on fertility, bone health, cardiovascular health, brain structure, and sexual function (Wierckx et al., 2012; Bjørnebekk et al., 2021; Cheng et al., 2019; Levine, 2018; Dreher et al., 2018; Nassiri et al., 2020).
The paper also notes that WPATH's SoC8 contains no guidance on caring for people who detransition, individuals who underwent these treatments, and later regretted or reversed course (Cohn, 2023; Jorgensen, 2023; Clayton, 2023). Without studying these patients, the paper argues, the evidence base is fundamentally incomplete because only favorable outcomes are being captured.
How Many People Are Affected?
Estimating the number of people receiving "gender medicine" in the US is surprisingly difficult. Some patients are "correctly" coded through insurance with a "gender dysphoria" diagnosis. Others receive treatments coded under different diagnoses, a practice called "creative coding" (Grinberg et al., 2018; Santoro, 2022). Still others pay out of pocket entirely. A "gender dysphoria" diagnosis is also not always required (Olson, 2022; Wahlberg, 2023), and the formality of diagnosis varies widely (Plume, 2022; Chiang et al., 2023). Insurance-based estimates (such as Respaut and Terhune, 2022, reporting about 5,600 children treated from 2017–2021; Canner et al., 2018) only capture a fraction.
The paper takes a practical approach, using published referral data from a single pediatric gender clinic and the known exponential growth in the number of referrals, consistent with data from multiple countries. The extrapolated single-clinic treated population was 378 (2019), 671 (2020), and 1,193 (2021). There were 33 of these clinics in 2014, meaning just two clinics with similar populations would exceed the entire Respaut and Terhune national estimate. A calculation was then undertaken that when a patient population reached a certain annual size, a new clinic needed to open. If the average among various clinics is around 121, then approximately 326 would be treating patients by 2021. This compared well with the 300-400 estimated by SEGM and Gender Mapper. Note that the medical group associated with the pediatric clinic is being sued by a detransitioner @CholeCole (Brockman v Kaiser, 2023).
Adding in Planned Parenthood's 41 gender medicine clinics, which treated over 74,000 patients across all ages in 2022 alone based on extrapolated data (Brock and Anderson, 2023; Sibarium, 2023), and using survey data on transgender identification rates (Herman et al., 2022; Jones, 2023) with US Census population figures (US Census Bureau, 2020) to estimate the pediatric-to-adult ratio, the paper estimates:
- Approximately 200,000 children have cumulatively received gender medicine treatments since 2015
- Approximately 650,000 adults in the same period
- A combined total of roughly 0.9 million people, with acknowledged uncertainty of ±50%
The paper predicts that the pediatric growth rate likely plateaued in 2022–2023 because the number of new clinics needed to sustain exponential growth became impractical. The author also notes that the Respaut and Terhune insurance database analysis captured roughly 6% of the estimated overall population, meaning 94% of pediatric "gender medicine" patients are either not using insurance or not receiving a "gender dysphoria" diagnosis before receiving treatments.
WPATH's Influence on Practice
The paper documents how WPATH's guidelines shape care broadly. The American Academy of Pediatrics' 2018 policy statement directly references WPATH (Rafferty, 2018) and this policy subject to a another detransitioner lawsuit (Ayala v. AAP, 2023, settled with Rafferty and dismissed against AAP). The Endocrine Society's guidelines were co-sponsored by WPATH (Hembree et al., 2017) and have been criticized by evidence-based medicine experts (Kaltiala et al., 2023; Block, 2023a). WPATH training is incorporated into physician education at universities (Kayode, 2023).
WHAT DOES THE EVIDENCE ACTUALLY SHOW?
Several countries have independently reviewed the evidence behind "gender medicine" for young people, and all reached similar conclusions:
- Finland (Council for Choices in Health Care, 2020): Found the evidence very low quality; required gender medicine to be delivered only through research clinics with experimental safeguards
- Sweden (Ludvigsson et al., 2023): Concluded gender medicine should be considered experimental and delivered only under strict research conditions
- United Kingdom (NICE, 2020): Found very low quality evidence for both puberty blockers and cross-sex hormones in children/adolescents
- Norway (Healthcare Investigation Board, 2023; Block, 2023b): Criticized the establishment of treatment guidelines without a systematic review first; classified treatment as experimental
- Denmark (Hansen et al., 2023): Changed its treatment policy based on safety concerns from insufficient evidence
The Cass Review interim report (2022) noted that an experiment is defined by a deliberate scientific framework, which is currently absent from "gender medicine" practice. Despite these findings, WPATH's SoC8 was developed using a consensus-based approach (Delphi method, where experts vote on recommendations) rather than strictly following the evidence. This distinction is acknowledged by WPATH leadership in their own communications. Note that this paper was submitted before the final Cass review, which also makes the same point.
ETHICAL CONCERNS
The paper raises several ethical issues:
The phrase "Do no harm" appeared in the ethics section of SoC version 7 (Coleman et al., 2012) but was removed from version 8.
Research spanning a decade has shown that most children with gender dysphoria naturally resolve their distress through puberty without medical intervention (Kaltiala-Heino et al., 2018). However, when children receive psychological affirmation that their cross-gender identity is correct, the vast majority continue to identify that way (Zucker, 2019), raising questions about whether the approach itself influences the outcome. A paper raising serious ethics concerns about current practices (Levine et al., 2022) preceded SoC8 but is not mentioned in it.
All medications used in gender medicine are prescribed "off-label", meaning they are not FDA-approved for this purpose (AMA, 2016). Pharmaceutical companies have repeatedly declined requests from doctors to seek FDA approval or conduct clinical trials for these uses (Terhune et al., 2022). The FDA may have been considering lowering its standards to encourage approval applications (Anonymous, 2023). Dresser and Frader (2009) have warned about the risks of off-label prescribing when substantial uncertainty exists. Meanwhile, some of these medications can cause permanent infertility, and animal models are rarely used to test outcomes first (Anacker et al., 2021; Guarraci et al., 2023; Hough et al., 2017).
WPATH's own evidence review, conducted before SoC8 was published, stated: "We could not draw any conclusions about death by suicide" (Baker et al., 2021). Yet claims about suicide risk are frequently used to justify urgent treatment (Jensen, 2022), and the SoC does not distinguish between suicide risk before versus after treatment, an important distinction given that some of the medications themselves are associated with increased depression risk. "Gender diversity" caused by factors not treatable with gender medicine, such as homosexuality (Steensma et al., 2013) or autism (Churcher Clarke and Spiliadis, 2019), would not be expected to show reduced suicide risk from these treatments. Jackson (2023) supports this finding. The best available analysis on suicide in the UK pediatric gender service population (Biggs, 2022) is not mentioned in SoC8.
The Eunuch Chapter: A Case Study in Weak Evidence
Chapter 9 of SoC8, which addresses "eunuch" identity, is examined in detail as an example of the quality of evidence underlying the guidelines. Nearly every non-pharmaceutical citation in the chapter comes from the Eunuch Archive, an online fetish database. The cited sources include:
- A single case report where the method of psychiatric evaluation was not described (Hermann and Thorstenson, 2015)
- An opinion piece (Wassersug and Lieberman, 2010)
- A popular press article that was not peer-reviewed (Hay, 2021)
- A book about writing fictional eunuch characters (Lieberman, 2018)
- A journal article where none of the reference links functioned (Wibowo et al., 2016)
- A journal article with only three references total — a census, a textbook, and a photo essay (Mukhopadhyay and Chowdhury, 2009)
No data is presented supporting the eunuch identity in children. The Eunuch Archive contains writings involving minors (Gluck, 2022a). The chapter's lead author (T.W. Johnson, listed as 12th author on Coleman et al., 2022) has been documented as having a personal sexual interest in the subject matter (Gluck, 2022b), raising conflict of interest concerns. The paper argues that a systematic review of this chapter would likely not retain any of these citations.
How WPATH Responds to Criticism
The paper reproduces a full April 2023 letter from WPATH President Dr. Marci Bowers (Bowers, 2023) and analyzes it against the six failure characteristics:
- Detransitioners are not mentioned anywhere in the letter. The SoC repeats that detransition is rare when the actual rate is unknown.
- The letter's content is predominantly political, discussing "anti-trans" legislation, conservative politics, gun control, book banning, and Harvey Milk, with very little addressing medical evidence or patient safety.
- The Finnish, Norwegian, and Danish evidence reviews and policy changes are not acknowledged. The Florida review of available evidence (Brignardello-Peterson and Wiercioch, 2022) is not directly addressed.
- European restrictions are characterized as having been "cherry-picked" by US conservatives, without engaging with the substance of those reviews' findings.
- The Missouri Attorney General's actions, which were triggered by whistleblower evidence from a pediatric gender clinic (Bailey, 2023) and sought to require gender medicine to follow experimental research safety rules, are characterized simply as political attacks.
- Dr. Eli Coleman's quoted defense of SoC8 explicitly acknowledges the consensus-based methodology. The unscientific approach of SoC8 development was also discussed by Dahlen et al. (2021).
- A recent publication claiming that withholding WPATH-recommended care constitutes "maltreatment" (Georges et al., 2024) is cited as an example of insular training's impact, with its citations suffering from selection bias.
Shortly after SoC8 was first published on September 6, 2022, a revised version appeared on September 15 with nearly all age recommendations removed. The explanation, provided by committee member Amy Tishelman, was that age recommendations needed to be removed to avoid exposing practitioners to lawsuits while enabling insurance coverage for treatments. One age recommendation remained: phalloplasty was not recommended for youth under 18 due to high complication rates.
What Happens to People Who Raise Concerns?
The paper documents professional consequences for those who question WPATH's approach, drawing parallels to FAA retaliation against Boeing whistleblowers and hostility toward the Rotherham researcher. Kenneth Zucker, a psychologist who specialized in "gender medicine" for decades, was fired by the Centre for Addiction and Mental Health for asserting there was insufficient evidence behind their "best practices" (aligned with WPATH SoC). He was later exonerated and received an apology and settlement (Hayes, 2018). The paper states that questioning the safety of WPATH SoC can be expected to negatively impact one's career, and notes that the medical content of the paper itself was edited by an anonymous researcher in the field for this reason.
CONCLUSION
The paper concludes that WPATH meets all six criteria for organizational failure: decisions contraindicated by science, blocked scientific inquiry, suppressed dissent, conflicts of interest, insular training, and hostility toward those affected. "Gender medicine" as currently practiced is characterized, rightfully so, as dangerous, with an estimated 0.9 million people at risk (vastly underestimated in our opinion), and the paper calls for a formal safety investigation into the WPATH Standards of Care.
We thank E. Jensen for this important analytical paper, and encourage you to read it in full, below. We, at Colorado Principled physicians, and E. Jensen, implore the federal government to seriously investigate WPATH for organizational failure, and the exponential harm to vulnerable adults and minors who have been experimented on due to their "guidelines".
Brilliant work, @acsengsafety!
@zaelefty @ptelephant @ftc @potus @gop @GOPoversight @TheDemocrats @ConceptualJames @CollinRugg @swipewright @donoharm @govrondesantis @thejusticedept @hhsgov
#WPATH #WPATHFILES #USPATH #genderidentity #genderaffirmingcare #medicalethics #ethics #MedTwitter #MEDX #medicine

4
28
64
11,005

May 18
Above was 2017 USPATH conference. More on psychiatrist Karasic in this thread, including announcement of new recordings from the most recent American Psychiatric Association conference.
May 18

Yesterday Jack Turban and Dan Karasic spoke at the American Psychiatric Association's conference. They believed they could say whatever they wanted and you would not hear it.
They were wrong.
Drops tomorrow 5/18 on Informed Dissent.
3
7
624
May 18
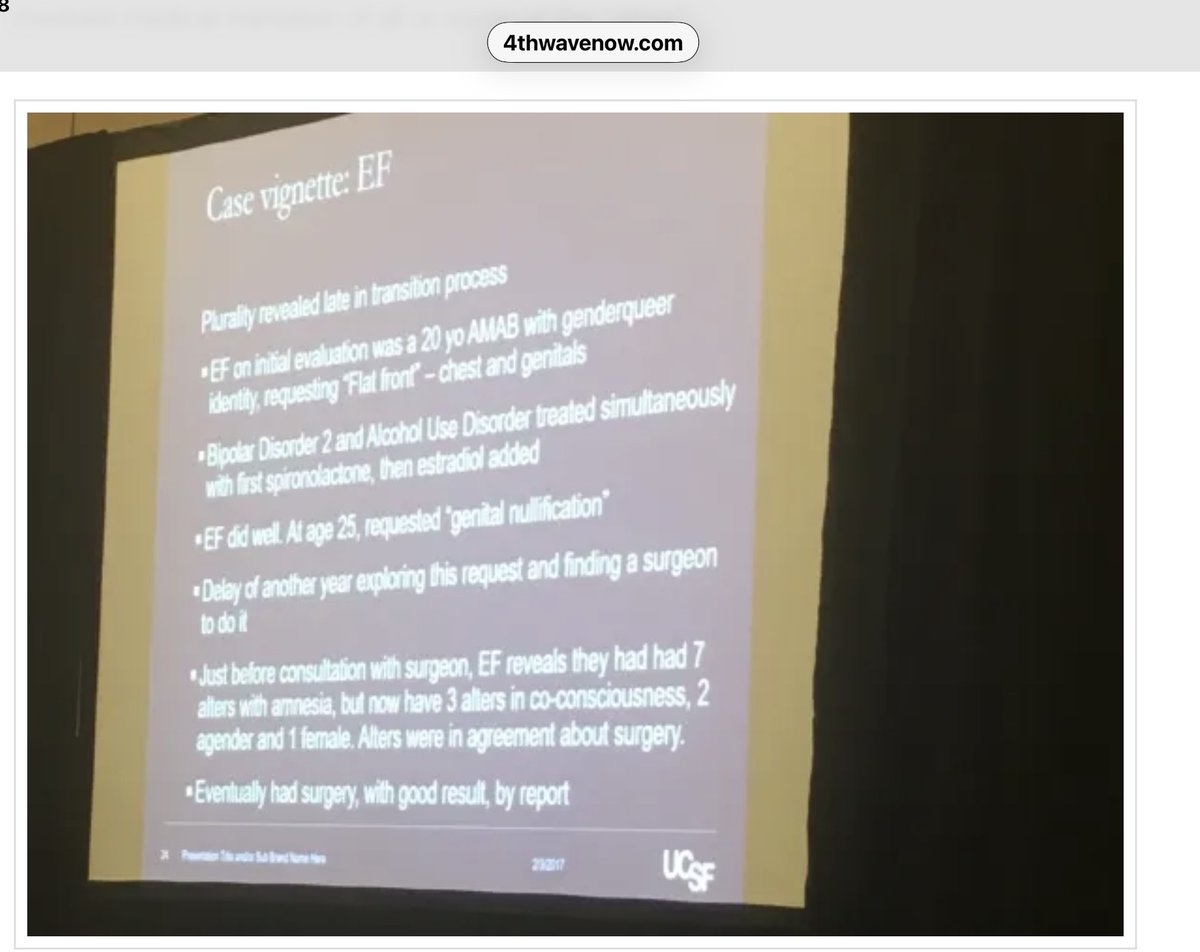
Most people have no idea how far "informed consent" has gone. Dan Karasic, prominent psychiatrist in the gender-affirming world, has promoted hormones & surgical interventions for profoundly disturbed patients for over a decade--as in this case (slide, USPATH 2017). Link below⬇️
2
2
13
356

May 1
11.4.1 ローラ・エドワーズ=リーパーとエリカ・アンダーソン
2021年、米国初の小児ジェンダークリニックの創設心理学者であるローラ・エドワーズ=リーパー(Laura Edwards-Leeper)と、臨床心理学者であり、米国トランスジェンダーヘルス専門家協会(USPATH)の元会長であるエリカ・アンダーソン(Erica Anderson)は、米国で最初の著名な内部告発者となりました。ワシントン・ポスト紙への寄稿で、エドワーズ=リーパーとアンダーソンは、思春期の若者が十分な心理的評価や検討を経ることなく医療介入を「性急に受けさせられている」と警告しました。「精神保健医療機関やジェンダー医療クリニックへの紹介が殺到し、個々の患者の治療を社会的な寛容さの試金石とみなす政治的風潮と相まって、多くの医療従事者がずさんで危険な治療を行っている」(60)と彼女たちは記しました。
ワシントン・ポスト紙に掲載された記事を受けて、USPATHは、WPATHがSOC-8を最終決定するまでの間、アンダーソン氏が報道機関に発言することを一時停止するよう求めました。アンダーソン氏はこれに抗議して同組織を辞任しました(61)。
ジャーナリストのアビゲイル・シュライアー氏(Abigail Shrier)とのインタビューで、アンダーソン氏は、現在のPMT(小児医療移行)のアプローチは「ずさんな医療行為」を伴い、若者が後に後悔するような決断を下す可能性があると警告しました。アンダーソン氏と同様にトランスジェンダーであることを公言している婦人科医かつ外科医のマーシー・バワーズ氏(Marci Bowers)も、同じインタビューで同様の懸念を表明しました。
バワーズ氏は、医療介入は当初は有望に見えたものの、実際には以前のアプローチと比べてより良い、あるいは同等の結果さえも得られていないと指摘しました。バワーズ氏は特に、これらの介入が生殖能力、性的健康、そして患者の親密さを経験する能力に及ぼす長期的な影響について懸念を表明しました(62)。
アンダーソンとエドワーズ=リーパーは、現在この分野で主流となっている「ジェンダー肯定」アプローチを批判しながらも、少なくとも一部の子供や思春期の若者は医学的な移行から恩恵を受けると信じています。バワーズはWPATHの指導部に対し詳細な謝罪文を送付し(63)、2022年から2024年まで同組織に留まり、会長を務めました。
1
8
16
1,037

Apr 11
"Embodiment Goals"
In recent years, activists in pediatric gender medicine world have pushed the field away from treating gender dysphoria and toward a service-minded meeting of the youth's “embodiment goals.”
As I recently wrote for @CompactMag, this term “intertwines metaphysics with plastic surgery,” and “was uttered ten times” in the 2023 USPATH conference session I featured in this Substack:
Apr 10

“One Session May Be Sufficient.” How Activist Providers Want to Overhaul Assessments for Youth Gender Transitions
benryan.substack.com/p/one-s…
I obtained a video of a 2023 conference presentation regarding a youth-gender-care assessment model that casts doubt on more traditional methods and seeks to service “embodiment goals.”
9
12
59
6,781
Apr 9
In this WPATH conference video, Natasha Johnson, a pediatrician at McMaster University in Canada, argues that parents' concerns about putting their child on gender-transition drugs should essentially be discounted in favor of the child's wishes.
Johnson was behind the activist effort to get evidence-based medicine expert Gordon Guyatt to kowtow after his team published their systematic review of gender-transition interventions last year: archive.is/20250903011815/un…
To read my article in @CompactMag about the 100s of videos I obtained from the World Professional Association for Transgender Health (WPATH) and its US offshoot, USPATH: compactmag.com/article/how-g…
I am in the process of publishing the most notable videos on my Subsack:
benryan.substack.com/p/i-obt…
2
6
36
4,211
Apr 3
The Evolution of the @ACLU's Chase Strangio From 2021 to 2025:
On engaging with critics:
2021, at the conference of the US branch of the World Professional Association for Transgender Health (USPATH): “[D]ecisions to engage with people like @AbigailShrier…are going to cost people lives”
2025, to the @NYTimes' Ross Douthat @DouthatNYT: “I’ve always been open to dialogue.”
On sex-based competitiveness in sports:
2021, at USPATH: There are “so-called fundamental differences between boys and girls, between men and women.”
2025, to Douthat: “I accept the premise that, in the aggregate, men have athletic advantages in a majority — though not all — sports.”
On trans inclusion in sports:
2021, at USPATH: “[W]hen you have young people who know who they are, we should absolutely not be undermining that by telling them they have to participate in sports based on their assigned sex at birth.”
2025, to Douthat: “I am not disputing that there are conversations to be had about how we manage the inclusion of trans people in sports.”
To see the full USPATH video, go to the quote tweet:
Apr 3
Chase Strangio's 2021 Warning: 'Decisions to engage with people like Abigail Shrier…are going to cost people lives.'
benryan.substack.com/p/chase…
I obtained 100s of conference videos that the World Professional Assoc. for Transgender Health fought to shield, including one in which Mr. Strangio contradicted his recent claims to Ross Douthat.
8
25
98
10,925
Apr 2
Sean Moundas, a psychologist, at the 2022 WPATH conference asserted that age limitations on youths' access to gender-transition drugs represents “adultism bias.”
To read my article in @CompactMag about the 100s of videos I obtained from the World Professional Association for Transgender Health (WPATH) and its US offshoot, USPATH: compactmag.com/article/how-g…
I am publishing the most notable conference videos on my Substack: benryan.substack.com/p/i-obt…
4
7
62
6,493
Apr 1
“Any form of ageism is unethical,” Simona Giordano, a bioethicist at the Univ of Manchester and WPATH ethics committee member, said in 2022 regarding providing gender-transition interventions to minors. “Refusing to treat someone because they are too young is as unjust as refusing to treat someone because they are too old. Decisions shouldn’t be based on age, but on capacity to benefit from treatment.”
To read my article in @CompactMag about the 100s of videos I obtained from the World Professional Association for Transgender Health (WPATH) and its US offshoot, USPATH, scroll up.
9
32
115
19,720
Apr 1
OHSU Performed Vaginoplasties On 17 Year Olds
Oregon Health & Science University urologist Dr. Geolani Dy said that for “a lot” of the hospital’s young patients, the timing of a vaginoplasty (a surgery that includes castration) “will fall around the seventeen-, eighteen-year-old age range.”
Dr. Dy said this during a presentation at the 2021 conference of the US offshoot of the World Professional Association for Transgender Health, USPATH.
See the main post in the thread for my article in @CompactMag and my companion post with dozens of clips like this one.
15
62
226
49,391
Apr 1
Ren Massey, a Georgia psychologist, suggested bringing in line parents wary of gender-transition interventions by introducing the specter of a CPS call. “There are at least some child protective service workers who are willing to enforce the need for affirmation by parents, at least with social transition needs, names, pronouns, etc.,” Massey said. “Even letting parents know that if that’s true where you are practicing, that might get their attention a little bit.”
To read my article in @CompactMag about the 100s of videos I obtained from the World Professional Association for Transgender Health (WPATH) and its US offshoot, USPATH: compactmag.com/article/how-g…
I will be publishing the most notable conference videos on my Subsack: benryan.substack.com/p/i-obt…
8
45
148
13,307
Apr 1
Johanna Olson-Kennedy: “I think that a lot of this conversation...gets talked about through a lens of ‘How can we make sure people are really trans,’ right? And ‘They’re not going to regret their decision later?’” But “that’s actually not the discussion that I’m interested in participating in," she said. "I’m interested in discussing and having a conversation about giving the very best possible care to trans young people—the care that they need and deserve.”
To read my article in @CompactMag about the 100s of videos I obtained from the World Professional Association for Transgender Health (WPATH) and its US offshoot, USPATH: compactmag.com/article/how-g…
I will be publishing the most notable conference videos on my Subsack: benryan.substack.com/p/i-obt…
5
27
112
19,975
Apr 1
Kellan Baker counseled against saying “gender-affirming care.” Messaging research indicated that when people hear it, he said, “they think ‘trans kids in the driver’s seat.’” But he said this was an accurate assessment. “I think we all support trans kids in the driver’s seat because it’s their bodies, it’s their lives,” he said.
“But when you think about folks who don’t know trans people, they are very scared by the idea that young people are making irreversible decisions and that no one else has any oversight over those decisions.”
To read my article in @CompactMag about the 100s of videos I obtained from the World Professional Association for Transgender Health (WPATH) and its US offshoot, USPATH: compactmag.com/article/how-g…
I will be publishing the most notable conference videos on my Subsack: benryan.substack.com/p/i-obt…
8
21
113
26,447

Mar 11
NEW: At a USPATH conference in 2021, Dr. Jens Berli of Oregon Health & Science University talked about offering mastectomy to 15–16-year-old girls who "have not finished their growth spurt," and "even if there is a chance that the patient would not need surgery in a year."
Dr. Berli is among the handful of gender surgeons who recently launched a pressure campaign against the American Society of Plastic Surgeons after the medical group advised its members not to perform gender surgeries on adolescents under age 19.
@wpath @USPATH1 @DrJensBerli @OHSUNews @ASPS_News
17
74
224
25,511

Feb 27
Oh, look, @LGBCourage @genspect @donoharm @OurDutyUSA @APApsychiatric is having pseudoscientist Jack Turban and @uspath president Maddie Deutsch speak on the evidence base of “transgender healthcare” for children, adolescents and adults at the conference this year…
1
3
86

This is a man. He is a former WPATH board member and president
of USPATH, and has helped transition many children.
Feb 6

I’m the psychologist expert witness who worked with Fox Varian and her attorney to win the case in New York. As I testified, he was wholly unqualified, failed to observe standards of care and simply blew it with a 16 year questioning her gender.
2
8
268
Feb 6
She caused a major paroxysm in USPATH over that interview that led to her walking away in disgust and the leadership putting a moratorium on its members talking to the press.
1
10
290

Feb 6
No. I’ve never worked “for” WPATH. I was on the Board and President of USPATH, but became disaffected years ago.
1
1
52
4,882

Jan 14
メモ。
EPATH,WPATH,USPATHの、未成年への思春期抑制剤投与に関するPATHWAYS試験に対する倫理的懸念表明の共同声明。
Jan 13

🚨Breaking🚨
WPATH has publicly raised ethical concerns regarding the UK puberty blockers trial.
Even a trans activist organisation brought into disrepute for medical malpractice thinks this trial is harmful, yet Wes Streeting cracks on.
Incredible.
epath.eu/epath-wpath-and-usp…
1
3
9
472