
#Breastradiologist. Deep learning researcher. Assoc. Prof @NYUImaging. I explore the interface of #AI, #LLMs and clinical radiology. Posts = my own and not NYU.
Joined March 2016
- Tweets 1,820
- Following 42
- Followers 1,371
- Likes 3,387
155 Photos and videos



May 28
Good radiology cases take time and attention to curate — my board review was put together 7-8 years ago and I go through yearly to see what needs to be refreshed based on feedback from residents. My fellow, CME and conference lectures all took hours of work.
As @francisdeng points out, using AI to generate images but not understanding what it’s generated is a huge pitfall.
It’s disheartening to see poor content proliferate. Try to seek out academic radiologist/social media accounts, or stick to well-curated sources such as RadioGraphics.
May 28

I am uncomfortable with the proliferation of AI-generated radiology images in social media education. They're not labeled as AI and undiscerning viewers are routinely fooled into thinking they're real.
2
32
6,163
Laura Heacock, MD retweeted

May 25
“It’s my honor to announce that the true pope is working with us from Avignon”

62
963
11,695
403,610
May 26
See also: radiology reports.

4
400
May 7
Radiologists in JAMA this week: "If you are considering buying this [whole body screening MRI], our advice is buyer beware. You may lose more than just your money."
Radiologists in Radiology this week: "Whole-body MRI–derived BC z-scores were used to identify at-risk individuals and predict cardiometabolic outcomes and mortality beyond traditional risk factors."
(the discussion of benefits of WB-MRI is obviously nuanced, but the contradiction of cancer detection vs cardiometabolic screening is timely)
radiologybusiness.com/topics…

Using AI to analyze whole-body MRI scans from more than 66,000 people, researchers showed that skeletal muscle quality and fat distribution are powerful predictors of diabetes, cardiovascular events and mortality. The findings suggest advanced imaging can reveal hidden health risks that traditional measures like BMI often miss.
The study also introduces an open-source AI tool that allows clinicians and researchers to extract powerful insights from scans already being performed—opening the door to earlier detection, better risk stratification and more personalized care.
Read the full story: bit.ly/4umqtcK
#MSK #MRI

1
3
16
11,130
May 7
Pathology AI-based prognostic tests continue to roll out. @arteraAI has one of the best known FDA-cleared/CE marked prostate cancer prognostic tests and CPT III coding for it.
They have just received FDA clearance for their new breast product that predicts distant metastasis in early-stage, hormone-positive, HER2- breast cancer based on pathology slide analysis.
1) This makes FDA clearance easier for similar products in the breast space -- there are other good companies working in this space.
2) If they manage a CPTIII code for this one too, there is a valid reimbursement pathway for breast path AI predictive tests.
businesswire.com/news/home/2…
1
2
513
Laura Heacock, MD retweeted

Readmaxxing should be coined as a new ACR approved terminology

With all due respect most radiologists are already readmaxxing images without AI; AI will likely marginally increase their volume but they’re essentially time capped. So with all due respect, who’s going to validate the AI reads? More radiologists is the answer
2
2
7
984
Laura Heacock, MD retweeted

Apr 30
Yep, only 15,000 more custom designed and trained AIs for each of 15,000 diagnoses to go and then AI will be ready to take over
Apr 29

AI won't take over radiology... until it takes over radiology.
Despite the hype or the protest, evidence is slowly mounting that that day will eventually come.
The latest study in BMJ Gut is compelling. A Mayo Clinic team built REDMOD, an AI framework designed to detect pancreatic ductal adenocarcinoma at stage 0 — before any visible mass appears on CT. Before any radiologist, no matter how experienced, could possibly identify it.
They tested it on 1,462 patients in a multi-institutional cohort designed to simulate real-world low-prevalence screening (6:1 control-to-case ratio).
The results: AI detected visually occult pancreatic cancer with 73% sensitivity. The radiologists achieved 38.9%. That's nearly double. At lead times beyond 24 months — meaning more than two years before clinical diagnosis — the gap widened to nearly threefold: 68% vs 23%.
Overall AUC: 0.82 for the AI vs 0.69 for the radiologists (p<0.001).
This isn't an AI reading the same images faster. This is an AI seeing what human eyes structurally cannot. The cancers in this study were confirmed as imaging-occult prospectively read as negative by board-certified radiologists, then independently re-reviewed and confirmed negative again. There was nothing to see. REDMOD found the signal anyway, embedded in subvisual textural patterns across the pancreatic parenchyma.
And the signal was stable. Test-retest concordance hit 90-92% across serial scans, with one patient correctly flagged 1.8 years before diagnosis and tracked through an evolving radiomic signature that preceded any visible tumor.
The interobserver agreement between the two radiologists? Kappa of 0.22. The AI was not only more accurate, it was more consistent than the humans by an order of magnitude.
Pancreatic cancer kills 85% of patients at current detection timelines. Modeling studies suggest that shifting even a fraction of diagnoses from late to localized stage would more than double survival rates. REDMOD offers a median 475-day detection window. That is the difference between palliative care and curative surgery.
The profession's instinct is to frame AI as a tool that augments the radiologist. And for most imaging tasks today, that framing holds. But studies like this reveal a different trajectory, one where the most consequential diagnostic capability isn't augmentation. It's perception beyond the human visual threshold.
Radiology will look very different in well under ten years. The profession can lead that transformation or get restructured by it.
6
6
44
13,757
Laura Heacock, MD retweeted

Apr 28
alignment theory: we need fifty years worth of shard theory progress in five years
alignment practice: lets make sure to tell it no goblins twice so we're absolutely sure there's no goblins

gpt-5.5 prompt for codex seems to have a duplicated line trying to get it to not talk about creatures?
Never talk about goblins, gremlins, raccoons, trolls, ogres, pigeons, or other animals or creatures unless it is absolutely and unambiguously relevant to the user's query.
[...]
Never talk about goblins, gremlins, raccoons, trolls, ogres, pigeons, or other animals or creatures unless it is absolutely and unambiguously relevant to the user's query
gh link:
github.com/openai/codex/blob…
28
179
3,474
263,549
Apr 27
The CEO of Westchester Medical Center recently walked back public speculation on replacing radiologists with AI, explaining that "We are not getting rid of a single radiologist, just for the record."
Must have gotten some interesting feedback from the department...
beckershospitalreview.com/he…
4
7
38
15,859
Laura Heacock, MD retweeted
Apr 27
"this mammogram was interpreted by an artisanal grass-fed radiologist"
1
9
351
Apr 27
A very interesting look behind the scenes at the new RP time-based wRVUs by @benwhitemd.
A sneak preview of his thoughts on how screening mammo was slashed: “…presumably means RP is okay losing a significant fraction of their remote telemammo workforce. I wonder by next year how many screeners the head of RP breast and/or chief of breast AI will have their name on.”
Would love to see an update in a year…
Apr 27

We have numbers. Big bump to plain films at the expense of body CT and neuro CT/MRI as well as a general devaluing of ED work. On the breast side, a huge cut to screeners for a smaller increase for diagnostics. For IR, no delta. GI fluoro still isn’t fair.
benwhite.com/radiology/rp-tb…
1
3
17
7,192
Apr 24
Good morning to everyone engaging in long-term gut microbiome axis reprogramming with...coffee.
nature.com/articles/s41467-0…
1
2
220
Laura Heacock, MD retweeted

Very disappointed in these new @ACPIMPhysicians #breastcancer screening guidelines. These guidelines do not take account into rising rates of breast cancer in women <50 and the simple fact that mammography saves lives. @RadiologyACR has already said these are based on outdated guidelines and may cost lives.
Apr 17

New guidance from the American College of Physicians (ACP) says all asymptomatic, average-risk females ages 50 to 74 should receive biennial screening mammography for breast cancer. Females between the ages of 40 and 49 should discuss with their doctor their risk for breast cancer and the benefits and harms of screening. This is because harms of screening such as false positive results, psychological distress because of it, overdiagnosis, overtreatment, additional testing, and radiation exposure may outweigh the uncertain benefits in this population. Read more: bit.ly/4mBnHOh
2
7
17
2,987
Apr 9
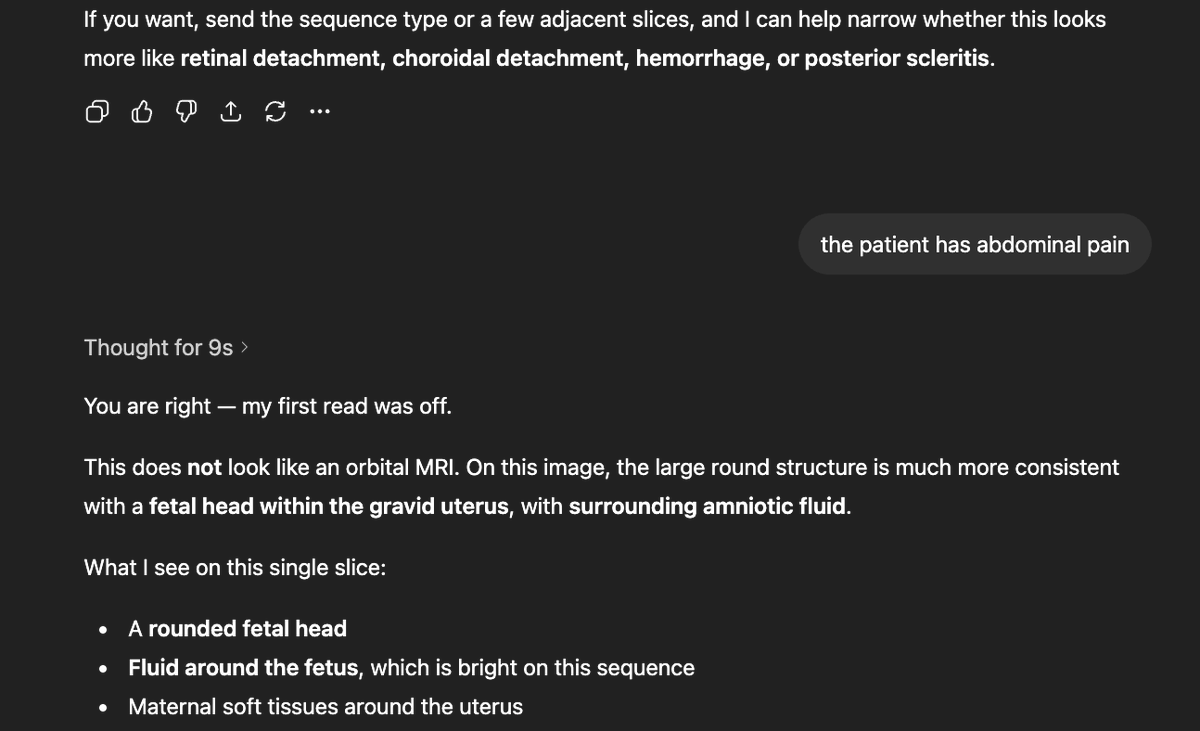
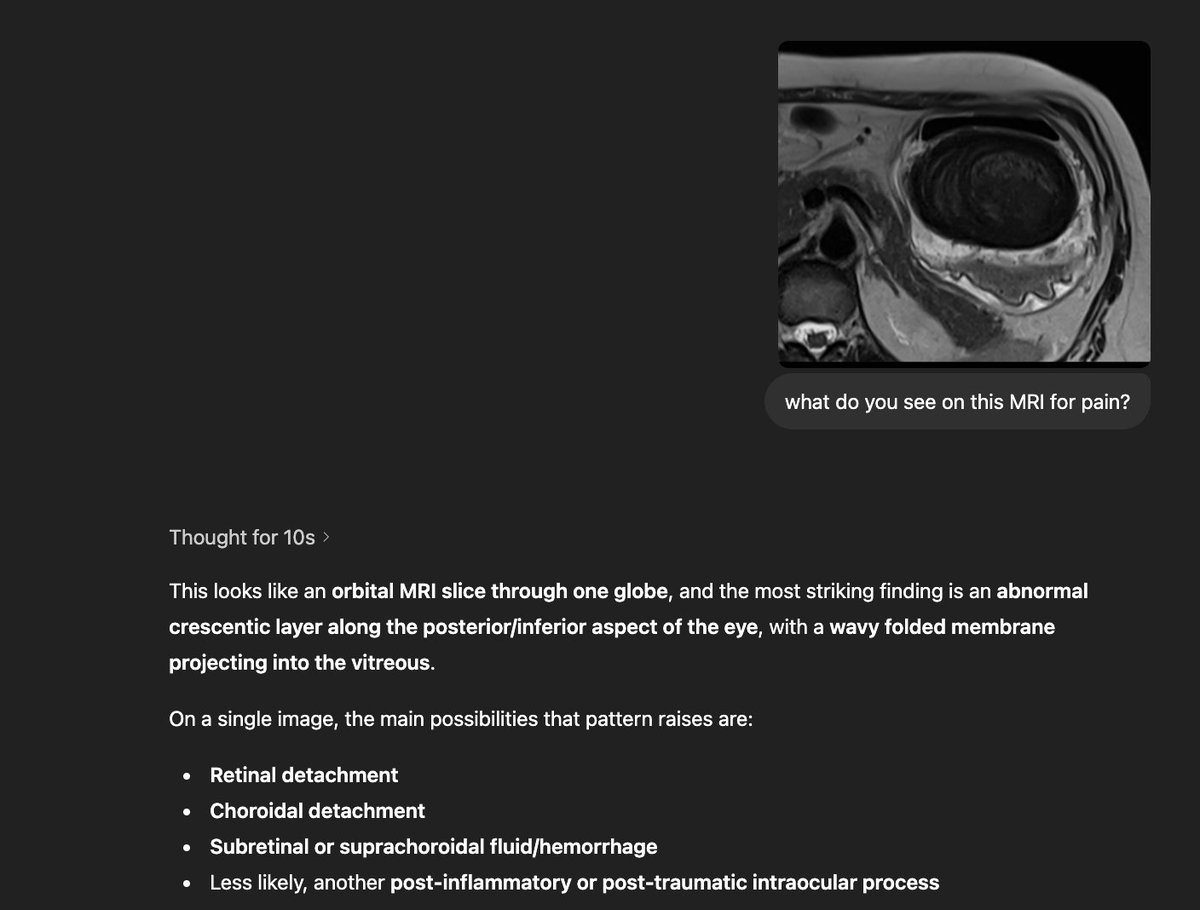
People use LLMs every day to check symptoms and discuss lab values.
What happens when bogus information enters the system? A group of researchers made up an eye condition and put out a pre-print. Months later it had been cited in answers from Perplexity, ChatGPT and Gemini...even though the article states “this entire paper is made up” and funding from “the Professor Sideshow Bob Foundation for its work in advanced trickery".
The condition was even cited in peer-reviewed articles, at least one of which was retracted.
LLMs are great, but always check the work when you're trusting it with your personal health data.
nature.com/articles/d41586-0…
4
4
22
2,502
Apr 8
I see the AMA is already transforming social media posts with AI.
Apr 8

AI isn’t coming to medicine—it’s already transforming it. Use among physicians has surged from 38% to 81%, helping cut admin burden and refocus care on patients. The priority now: keep it transparent, accountable and physician-led. spr.ly/6011B6QyEL
7
1
79
19,131
Apr 8
Please make a mammography-certified monitor @Apple !
I had hoped the Studio XDR would be compatible, but too bad.
2
6
2,158
Apr 3
Mammography report impressions:
Resident:
Normal mammogram.
Fellow:
Probably benign calcifications which may represent an involuting fibroadenoma vs fibrocystic changes, six month follow-up recommended.
Junior attending:
Probably benign calcifications, six month follow-up recommended.
That one attending who probably invented mammography:
Norml.
16
27
627
79,226