
Breast & gyn med onc @valleyhealthnj. Opinions my own. Host of INTERLUDE podcast. 📗 BEYOND THE PINK (2026). Patient education on Instagram.
Joined December 2017
- Tweets 5,317
- Following 1,204
- Followers 3,932
- Likes 7,558
518 Photos and videos











Eleonora Teplinsky, MD, FASCO retweeted

The last point is that what the #OPTIMA trial hammered home is the we truly overprescribe chemotherapy (especially anthracycline based chemo) to ER breast cancer patients and in that molecularly low risk 40 patient population ovarian suppression and aromatase inhibitor is just as effective as chemo and less toxic. Our field needs to move towards de-escalating chemotherapy in ER disease (including premenopausal) and utilizing targeted therapy (ovarian suppression and aromatase inhibitors are some of the 1st targeted therapies). No more overuse of chemo in this population. It doesn't help!
2
14
38
3,278
Eleonora Teplinsky, MD, FASCO retweeted

📣COME JOIN this NEW innovative open discussion format, no didactics, just practice changing exchange. enjoy food/drinks & maybe win the raffle!
Libretto 432
Harmoni 6
Crown
Atypical EGFR
ADC updates
Tarla & more
⏱️ 6/10 wed 6-8:40 pm
@mjeng21 @MSKCancerCenter @MSK_DeptOfMed

Post-#ASCO26 discussion happening next week 6/10.
Join @ipreeshagul, @ElaineShumMD, @mjeng21, @nickrohsmd & me to discuss key #lungcancer updates!
Register now: registration.onclive.com/sta…
5
13
1,048

roche.com/media/releases/med…
FDA expected to make decision on girdestrant in early stage BC by November 30, 2026!
3
19
2,136
So excited to share that my book is out on 9/29/2026!! Pre-order here a.co/d/0bdFkY8Q 🩷
1
2
21
774
Eleonora Teplinsky, MD, FASCO retweeted

From chemotherapy de-escalation and oral SERDs to metastatic triple-negative breast cancer and GLP-1 medicines, @drteplinsky breaks down some of the biggest breast cancer research updates from #ASCO26, what they could mean for breast cancer care, and the questions researchers are still working to answer.
🎧 Listen now: bit.ly/4dTmk9r
#ASCO26 #BreastCancer #CancerResearch #BreastCancerWarrior

1
2
6
360
Eleonora Teplinsky, MD, FASCO retweeted

Jun 2
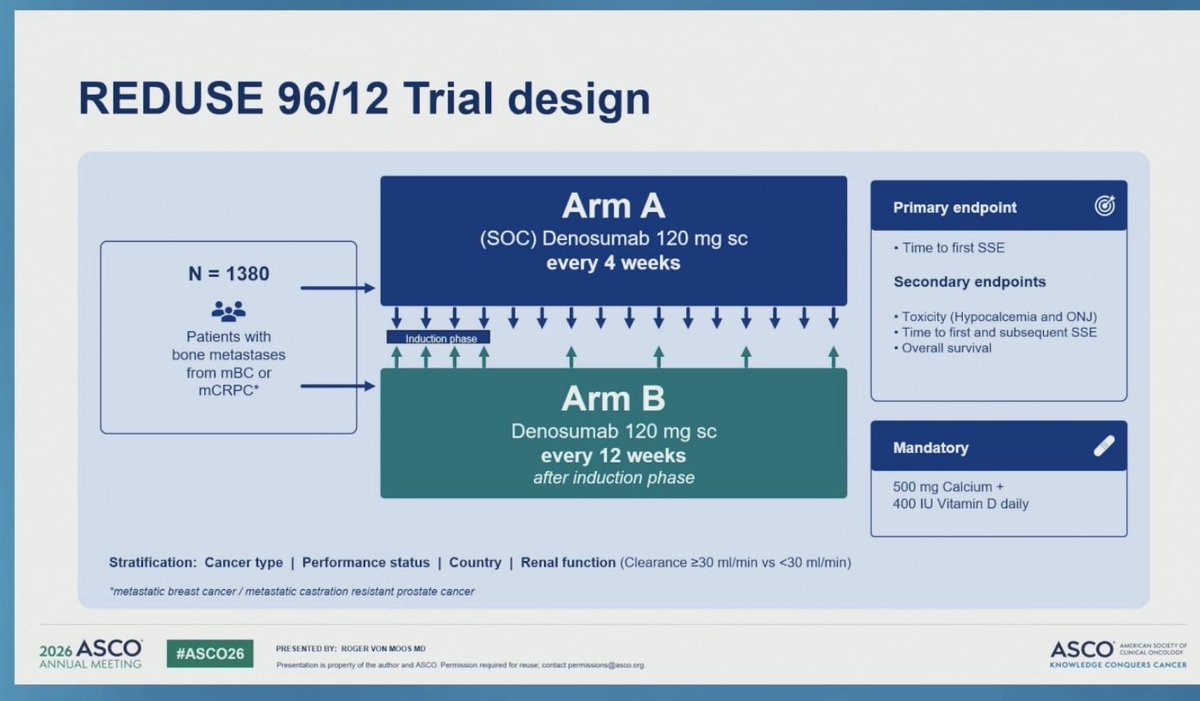
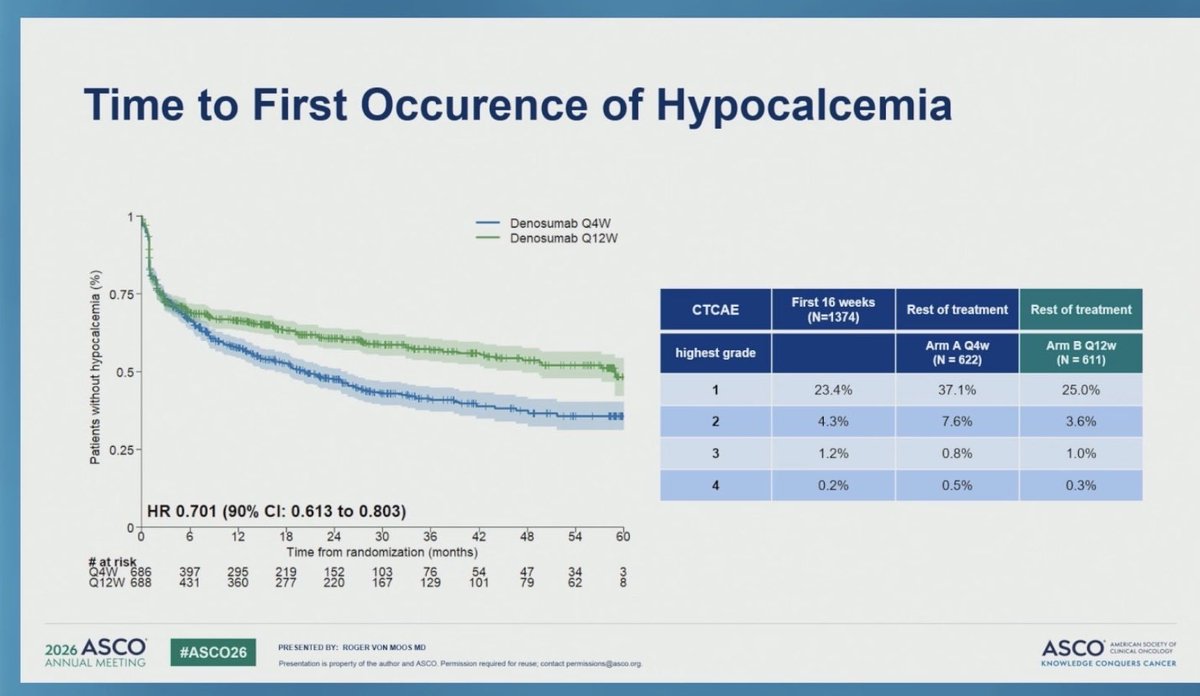
Practice-changing de-escalation data from REDUSE 96/12 at #ASCO2026.
• Phase III non-inferiority trial (N=1380); 57% had metastatic breast cancer
• Denosumab 120 mg Q12W after induction vs standard Q4W
• Calcium 500 mg Vitamin D 400 IU daily mandated
Key findings:
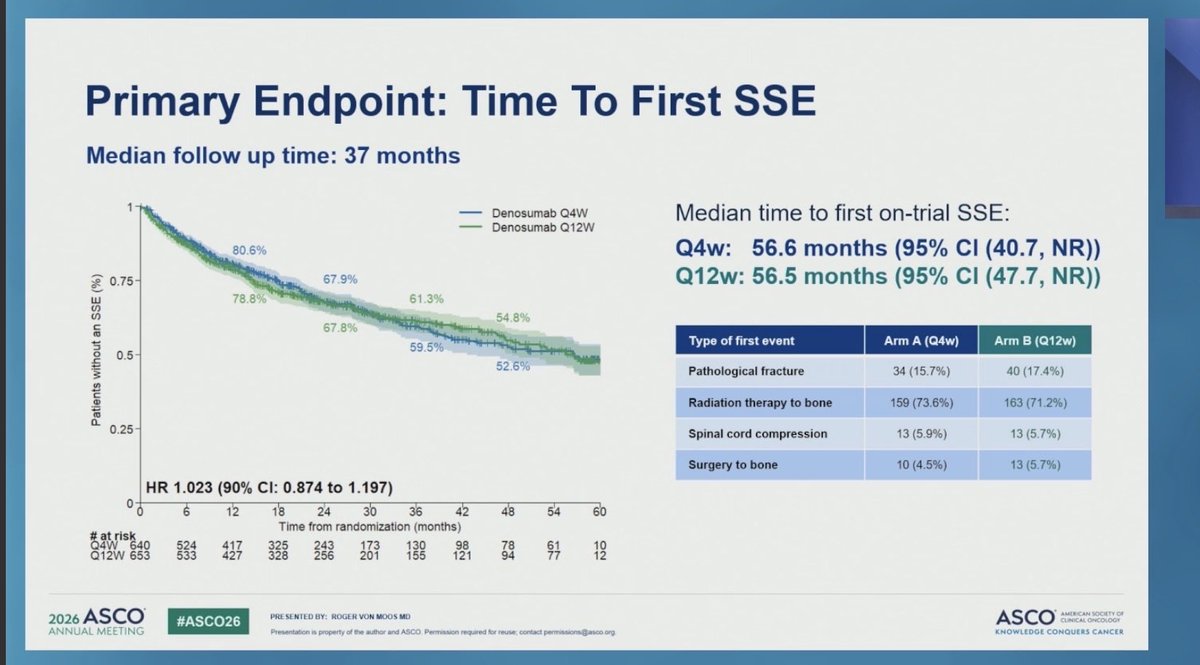
• Q12W was non-inferior for prevention of symptomatic skeletal events (56.5 vs 56.6 months; HR 1.02)
• Lower rates of hypocalcemia (HR 0.70)
• ~25% reduction in ONJ
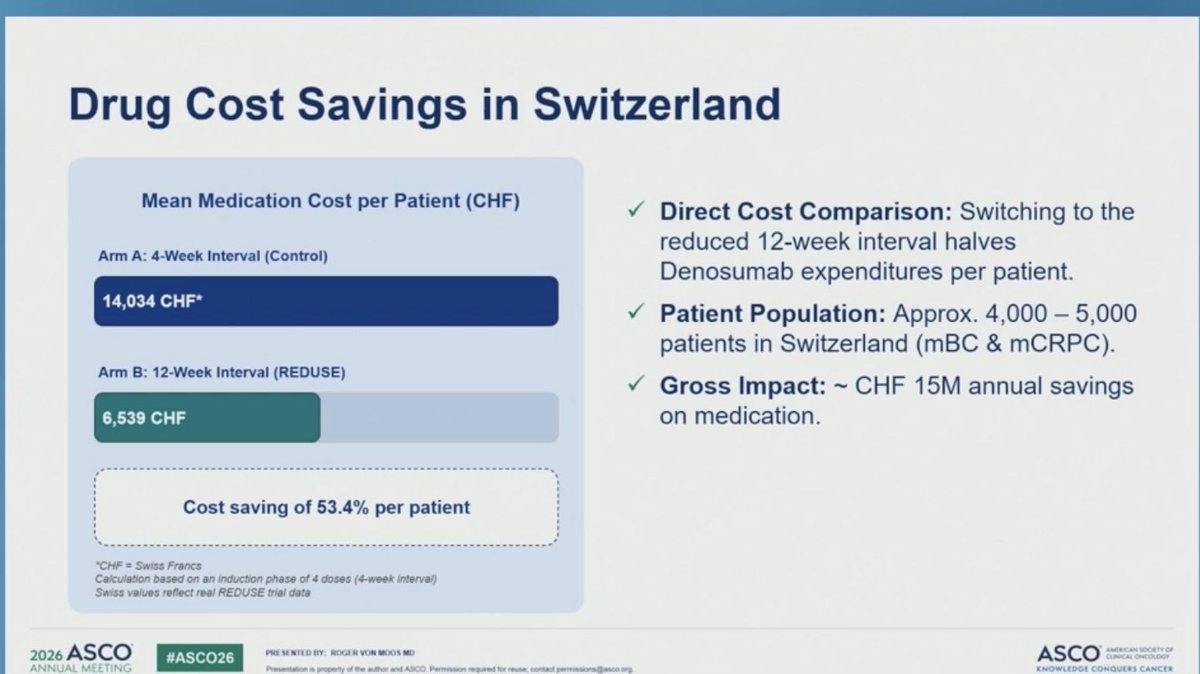
• Swiss analysis showed a 53% reduction in costs, likely even greater in the US
This study reinforces my current practice of extending denosumab dosing intervals. Less treatment, lower toxicity, lower cost, and no loss of efficacy.
#BreastCancer #BoneMetastases #Denosumab #ASCO2026 @muschollings
4
10
2,779
Eleonora Teplinsky, MD, FASCO retweeted

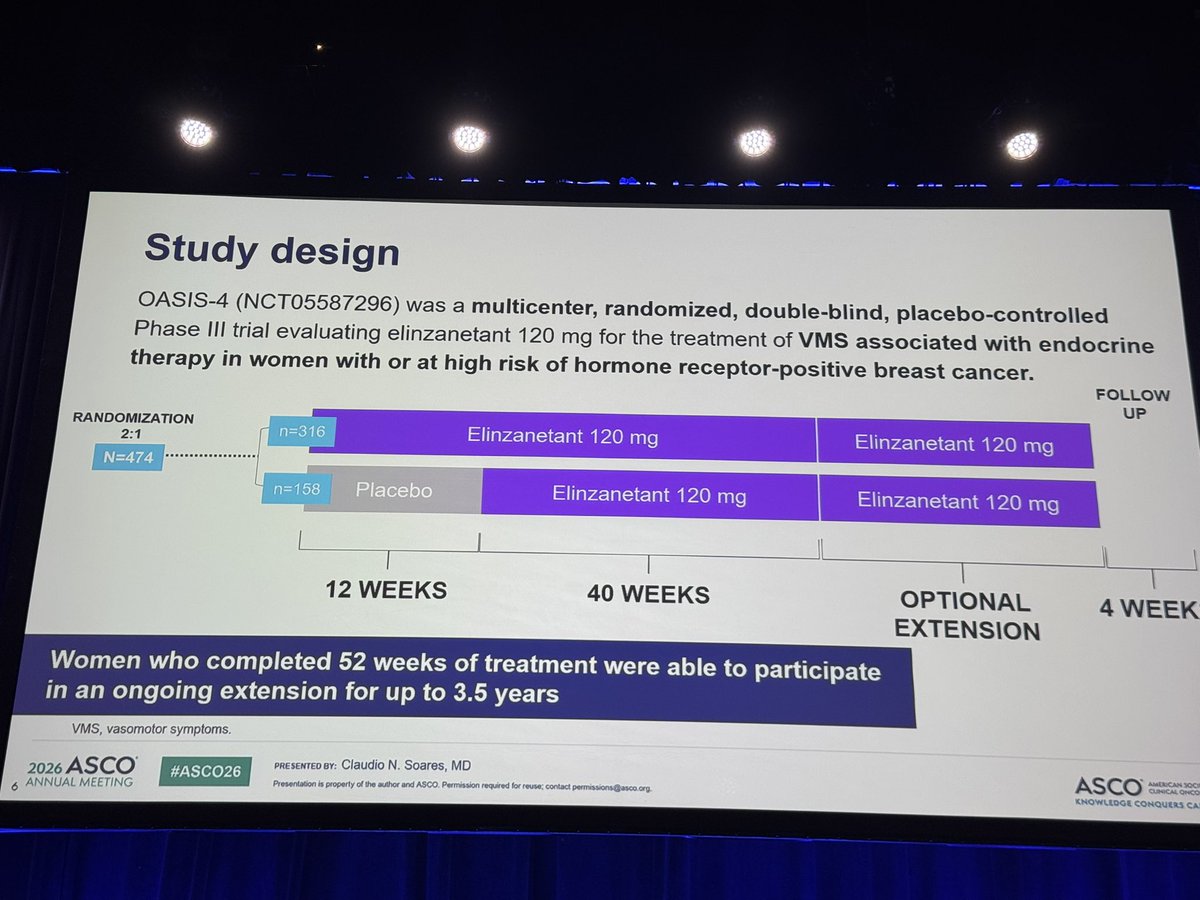
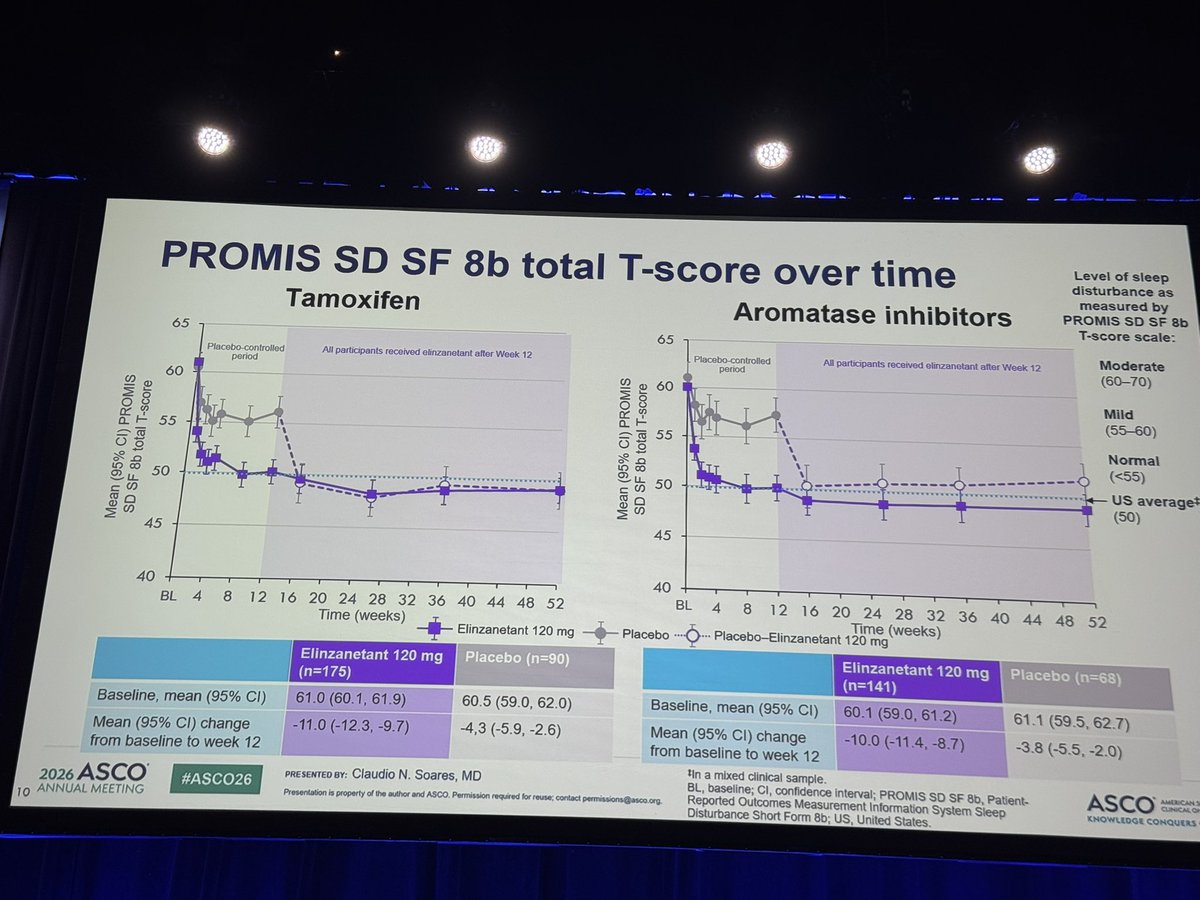
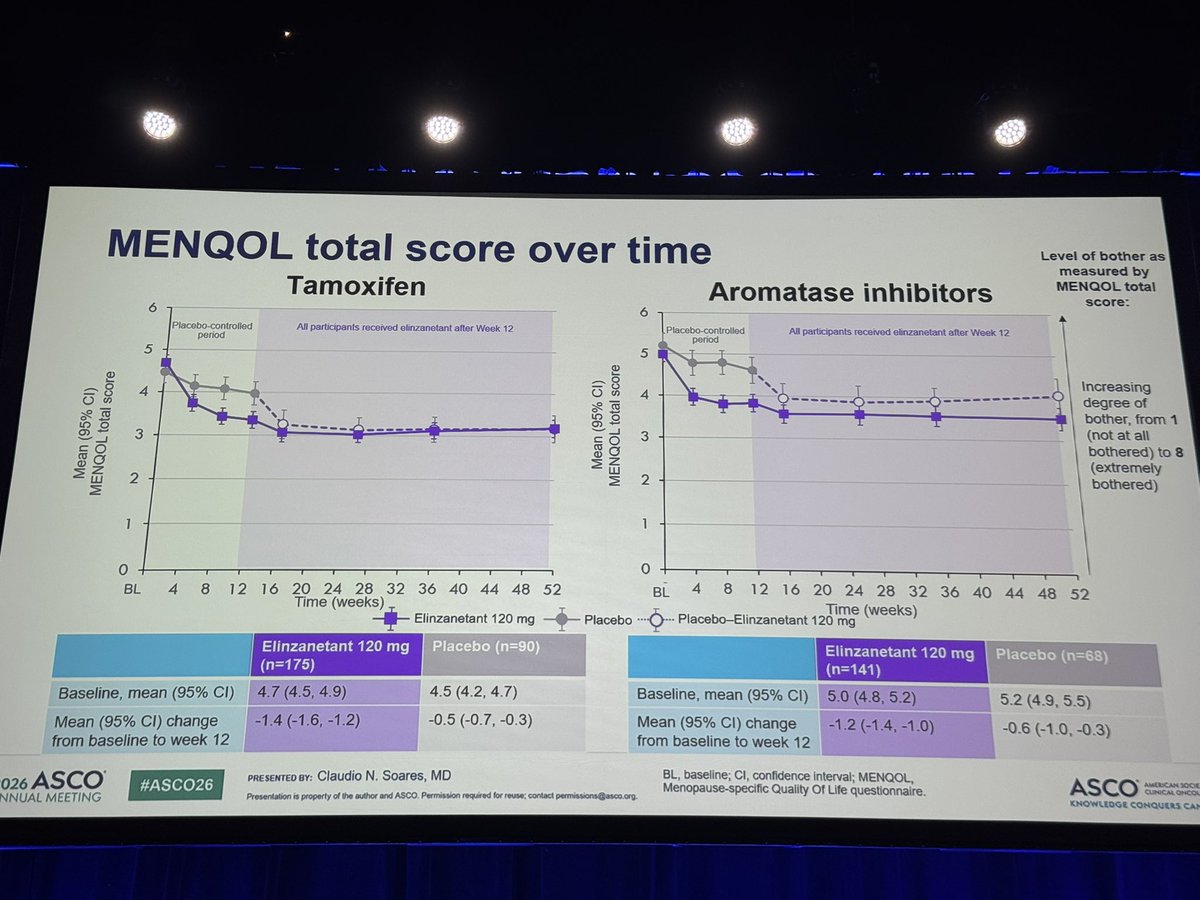
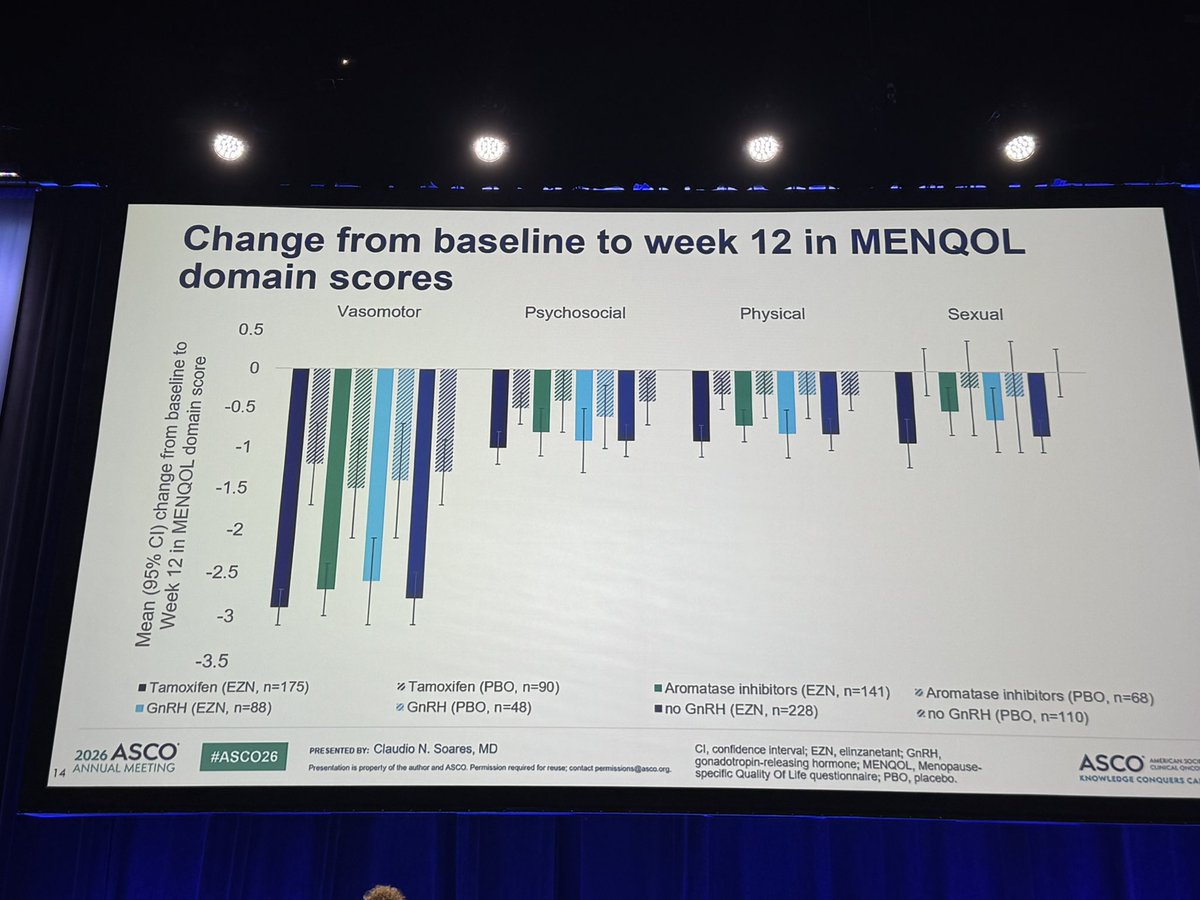
#elizanetant improves not only vasomotor symptoms but also sleep for patients on all types (tamoxifen, AI, and GNRH ) endocrine therapy for #bcsm
#ASCO26
2
23
51
7,850
Eleonora Teplinsky, MD, FASCO retweeted

Denosumab every 12 w after induction was non-inferior to every 4 w for skeletal-related events, with less hypocalcemia/ONJ and >50% reduction in drug costs.
A great example of how smarter de-escalation can maintain efficacy while improving safety, convenience, and value for patients‼️
#ASCO2026 #bcsm @OncoAlert
9
10
1,694
Eleonora Teplinsky, MD, FASCO retweeted

Jun 1
Eleanor the hardworking @ASCO elephant had a busy day Sunday @ #asco26 - press conference, education session, CDK study investigator meeting, National Cancer Grid India discussion, exhibit hall &
President’s reception. Phew! @cspramesh @ManjuSengar7 @LGM_Biostats @AbbyRosenbergMD

1
11
42
1,543
Eleonora Teplinsky, MD, FASCO retweeted

Jun 1
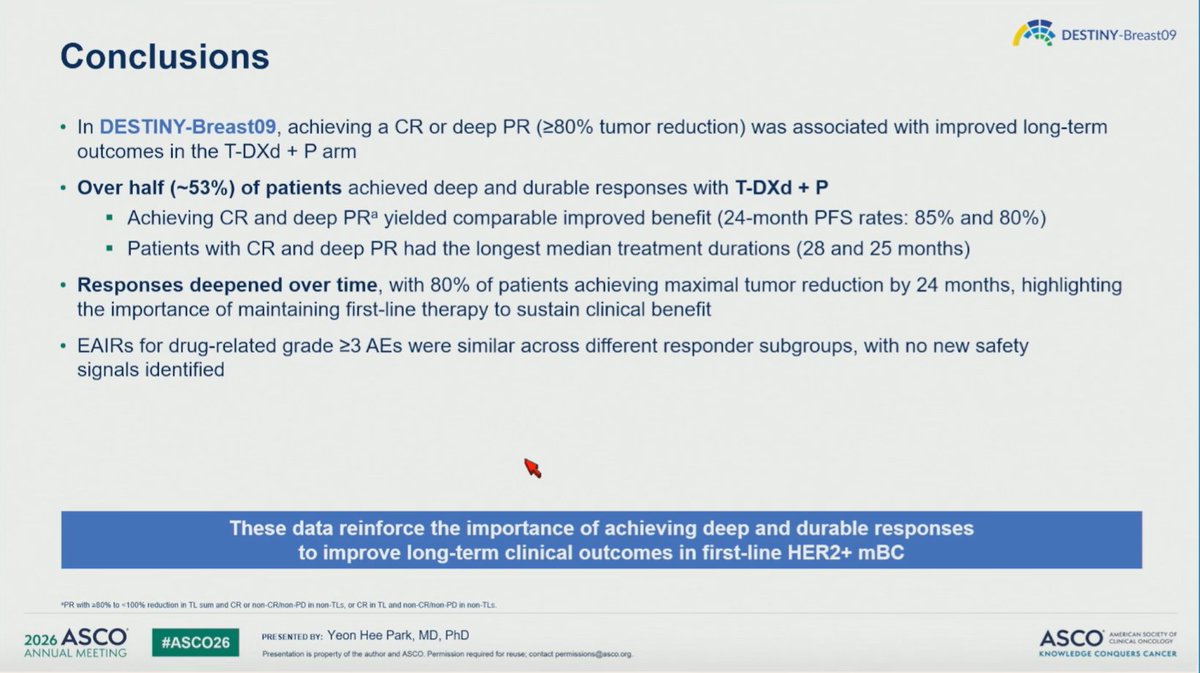
This speaks to a longer induction than 6-8 cycles…
May 31

#ASCO26
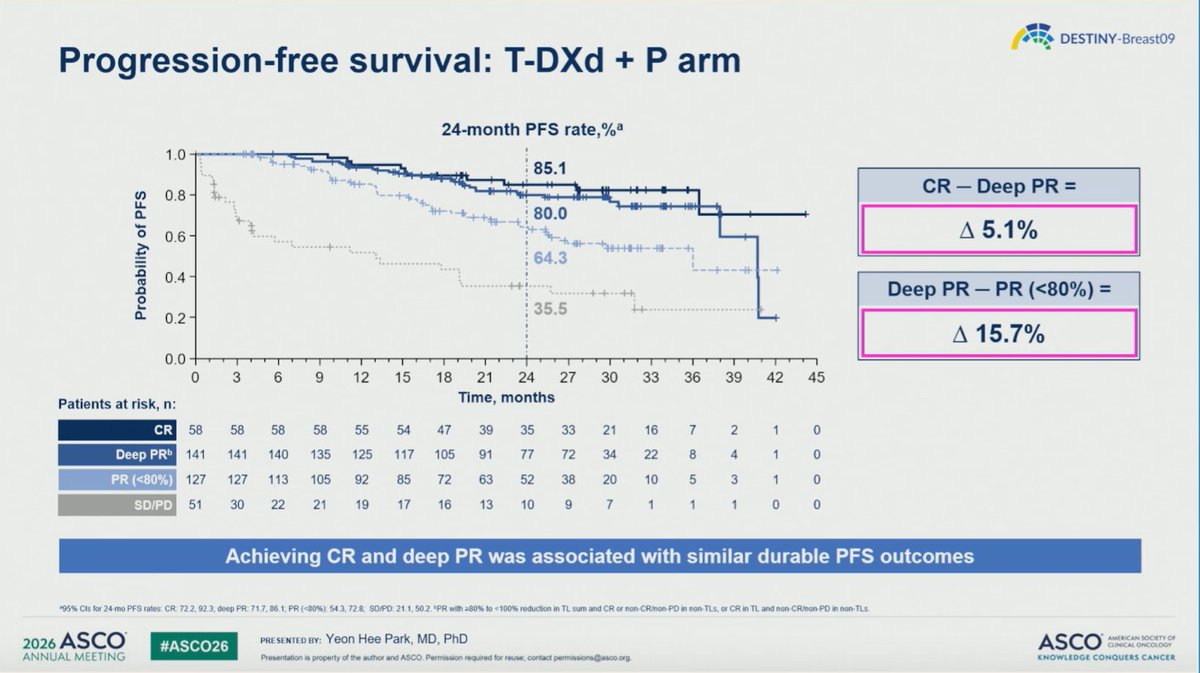
DESTINY-Breast09: With 1L T-DXd pertuzumab in HER2 mBC, responses deepened over time; median time to CR was 8.4 months, tumor nadir ~11 months, and >50% achieved CR/deep PR with durable 24-month PFS of 85% and 80%.


3
9
31
5,369
Eleonora Teplinsky, MD, FASCO retweeted

May 31
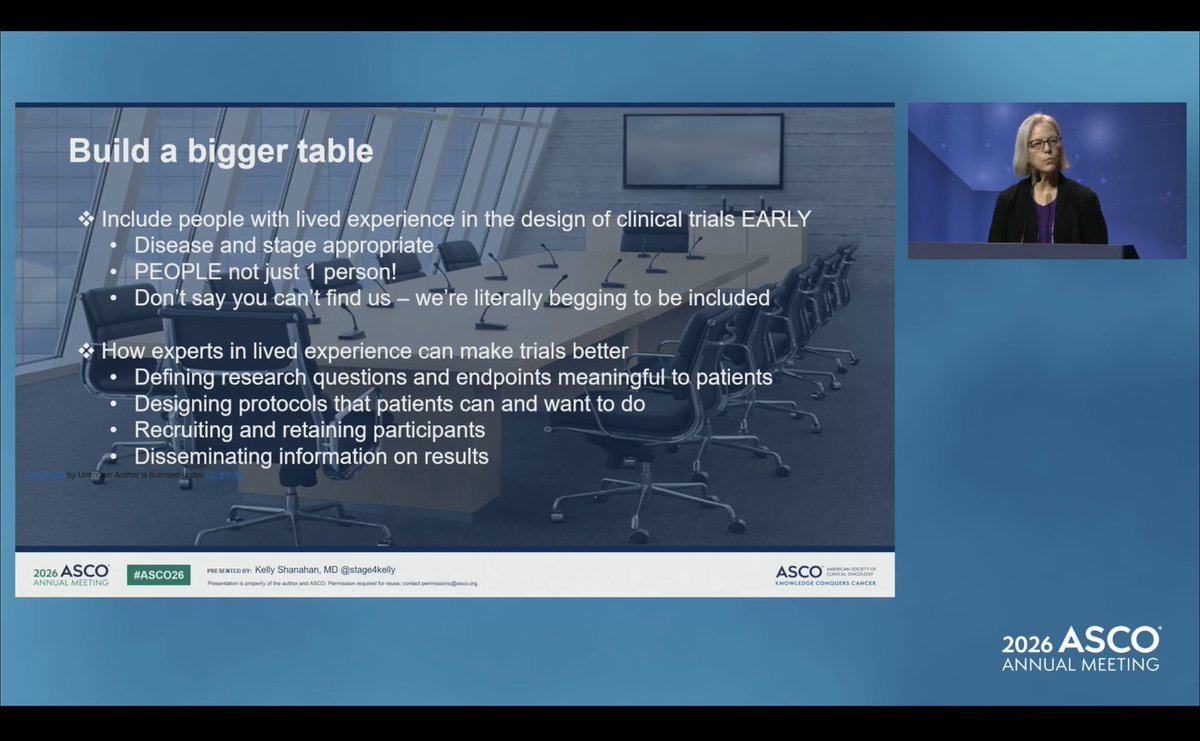
One of my favorite slides from @stage4kelly’s @ASCO talk this a.m. Sadly unable to attend live, but watched the recording & delivering congrats, 🙌🏻 & standing 👏 from afar, my friend!
Kelly did an outstanding job representing the #MBC community on the BIG stage, highlighting the importance of meaningful endpoints, transparent toxicity data, & including people with lived experience early in #clinicaltrial design.
Patients aren’t just trial participants, & never “subjects,” but ultimate stakeholders.
“Build a bigger table.”
Exactly!🩷🩵💚
#ASCO26
#bcsm
#PatientAdvocacy

Thank you @ErikaHamilton9 for your unwavering support and for suggesting me to the #ASCO26 program committee
4
5
22
1,726
Ending out #ASCO26 with a fantastic time at the President’s Reception!! @ARosen380 @msheenmd @JenSchwartzIUSM


1
2
14
448
Thank you @OncLive for a fantastic Women in Oncology event today!!! 📸 with some of the amazing women who attended! @mabelonc @DrReshmaMahtani @SaraNunneryMD @cancerfashion @DrKEMcCann @DrSAHaddad #ASCO26

2
3
18
1,528
Eleonora Teplinsky, MD, FASCO retweeted

May 31
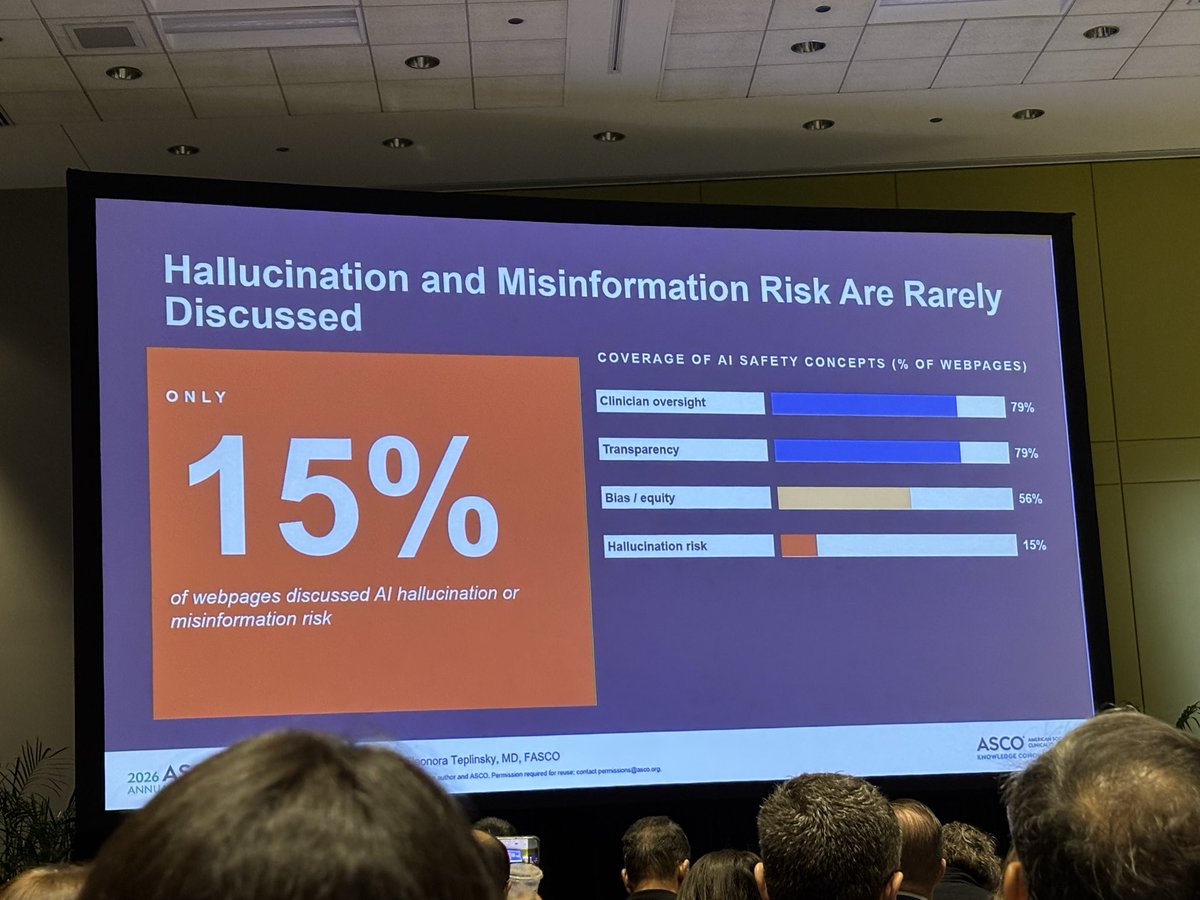
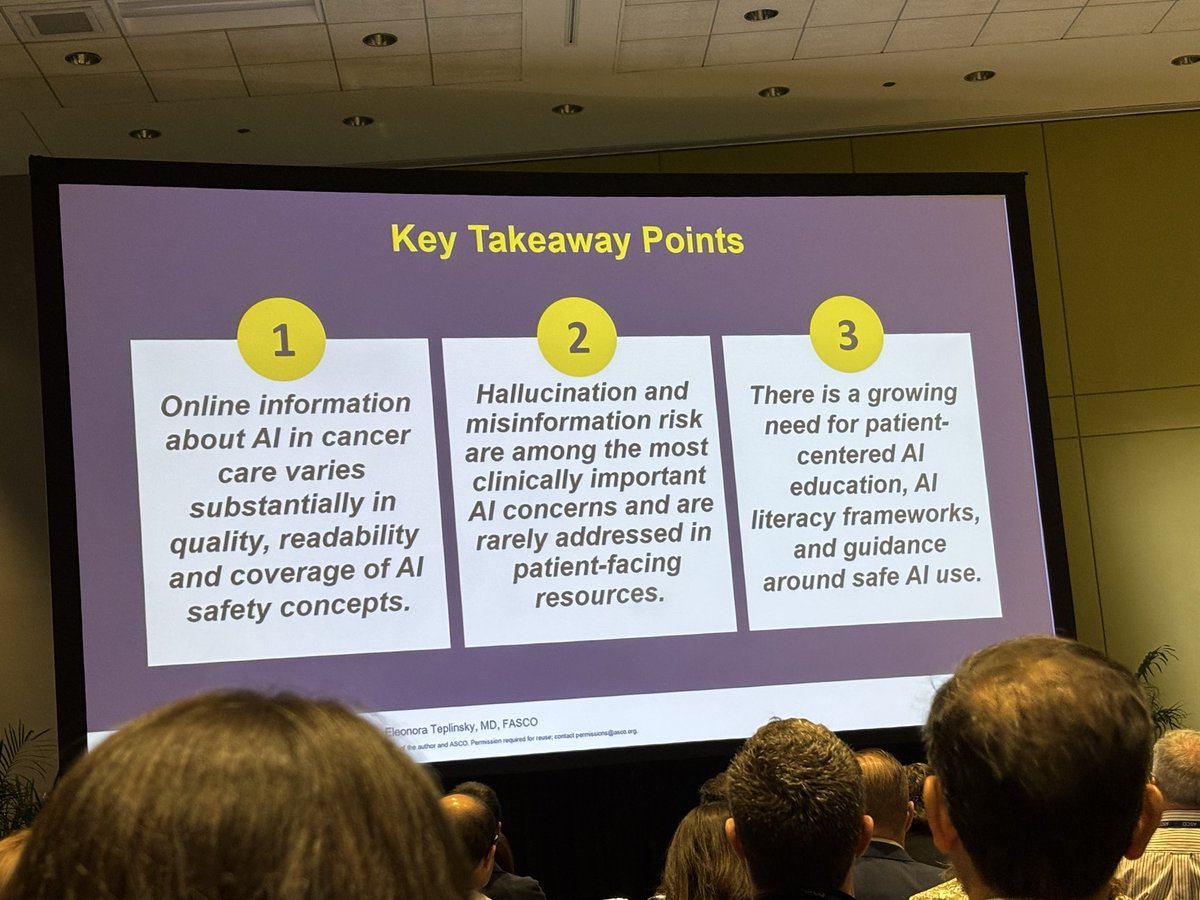
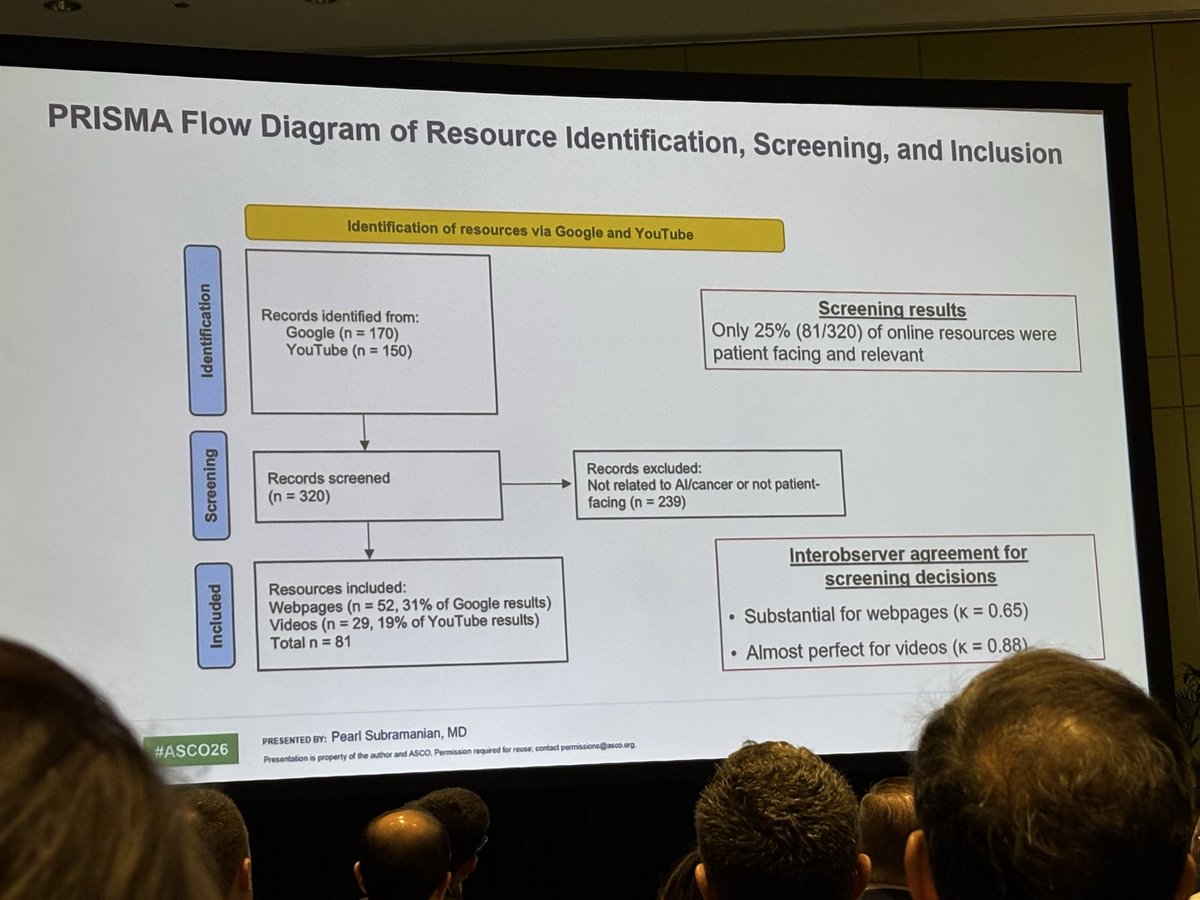
As AI becomes increasingly integrated into cancer care, are patients being given the information they need to make informed decisions?
Today at #ASCO26, @drteplinsky shared findings from a cross-sectional analysis exploring gaps in patient-facing information on AI in oncology and discusses the impact these gaps may have on trust, engagement, and participation in AI-informed care and clinical trials.
@ASCO #AI #AIinOncology

1
2
159
Eleonora Teplinsky, MD, FASCO retweeted

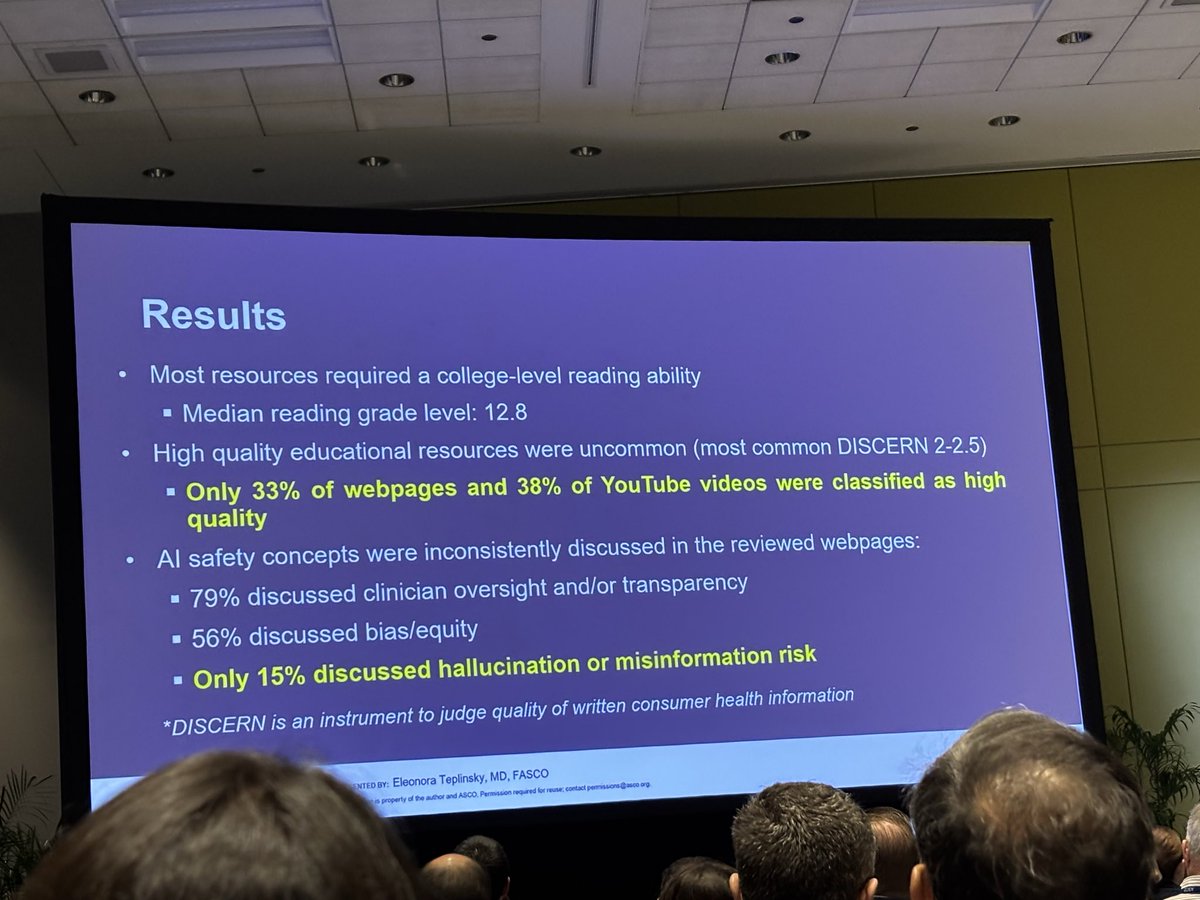
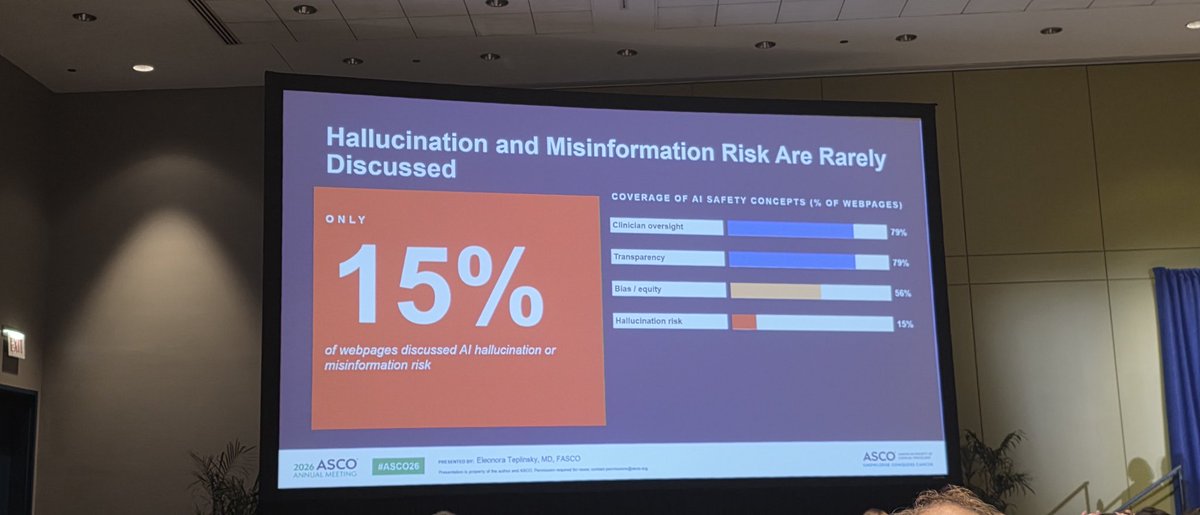
Fresh data from #ASCO26 shows a massive blind spot: online resources about AI in cancer care are largely low-quality & completely omit the risks of AI hallucination & misinformation.
We need a major push for AI literacy to protect patients! 🛑🤖 #OncTwitter #CancerCare #meded
1
7
13
898
Eleonora Teplinsky, MD, FASCO retweeted

May 31
@drteplinsky Great conclusion ‼️
🤔 What are we doing to avoid this?
#ASCO26 #digitalhealth #AAOCDigital
3
7
243
Come to our session - Oncology 2.0: How Artificial Intelligence Is Closing the Information Gap—Or Is It? Starting 9:45 CST, S102! -going to be a great discussion! @MatthewKurianMD #ASCO26
1
4
337
Eleonora Teplinsky, MD, FASCO retweeted

#ASCO2026 is off to a great start! I was honored to chair this session: “Optimizing Breast Cancer Survivorship: Addressing Lifestyle, Weight Management, and Psychological Health.”It was wonderful to speak alongside experts Sophie Lebel,PhD, @SherryShenMD, & @LauraCarfang. #bcsm


4
13
548

#asco26. Key data from the exciting LidERA study in premenop pts presented by Schmid. Benefit x menopausal status & most Rx with tam in control received LHRHa. Less d/c due to pain. Longer FU needed for medium risk. Q - combo with CDK4/6i or instead? More data T/F @OncoAlert
2
9
22
2,001
Eleonora Teplinsky, MD, FASCO retweeted
🔑 Take aways from @ASCOPres address
“If a pt cannot get the treatment they need or cannot make it to the center to get care, it’s a unmet promise. How can we keep our promise?”
“Toxicity is acceptable , ONLY if it’s acceptable to the pt”,
YES TO THIS 🙌🏽

11
19
715