
NHS trained Endocrinologist - KIMS Hospitals Bangalore! Founder of Mysugars.in, #Diabetes, #obesity #endocrinology
Joined April 2011
- Tweets 3,594
- Following 1,052
- Followers 1,526
- Likes 12,885
961 Photos and videos









Pinned Tweet

30 Jun 2025
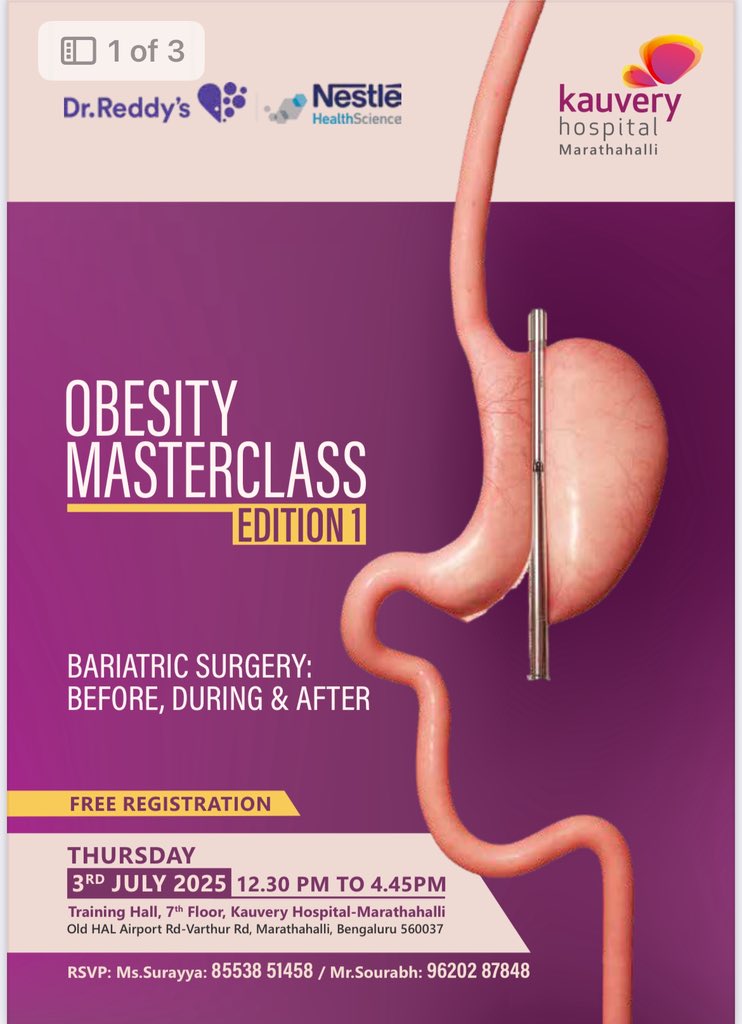
#bariatric surgery ….
What surgery for whom
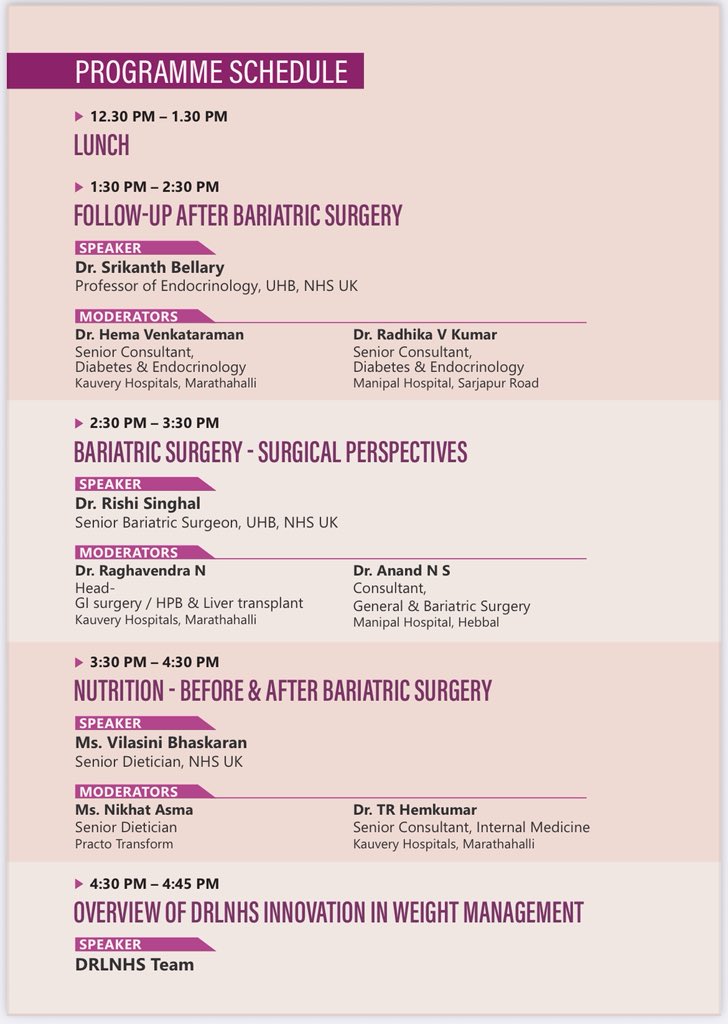
Managing nutrition in the run up to surgery
Long term follow up post surgery
Setting up a bariatric service at your centers…….
The marriage of #surgeons and #physicians and #dieticians …..
Come join us on the first of the #obesity masterclass series…at @KauveryB Marathalli
3rd July afternoon with Lunch
12-4.30 pm
Free to attend
RSVP below
The Before, during and After of Bariatric: / Metabolic surgery!
#surgeons #physicians #MedTwitter #dieticians #nutritionists #endocrinology #obesity #healthcare #education

1
1
25
23,484


Jun 12
4
7
547
Jun 12
Jun 11

🚨 South Asians develop heart disease a full decade earlier than Europeans, at double the risk, and the calculators your doctor uses to assess you completely miss it.
The standard tools were not built for your biology.
And no, this is not just about diet or lifestyle.
🫀 Here is what the science actually says.
A landmark UK Biobank study published in Circulation (2021) looked at this directly. South Asians carried a hazard ratio of 2.03 for heart attack and stroke compared to Europeans. That is not a rounding error. That is double the risk. And the Pooled Cohort Equations, the calculator your doctor almost certainly used at your last visit, failed to detect it.
You could walk out of an office with a "low risk" label and be sitting on a ticking clock.
💓 The American Heart Association and ACC did not ignore this. Their 2018 cholesterol guidelines formally recognized South Asian ancestry as an independent cardiac risk-enhancing factor. Not a soft suggestion. A formal designation. That means South Asian heritage alone moves the needle on treatment decisions.
🔬 Why does this happen?
South Asians carry higher rates of insulin resistance even at normal BMI.
Lipoprotein(a), one of the most dangerous atherogenic particles, runs elevated in this population at baseline.
Visceral fat accumulates disproportionately, even in individuals who appear lean by Western standards.
Inflammation markers trend higher, independent of traditional risk factors.
Standard BMI cutoffs were built on European body composition data and systematically underestimate cardiometabolic risk in South Asians.
⚠️ This is the compounding problem. Every layer of risk assessment, from the BMI chart on the wall to the 10-year risk calculator on the screen, was calibrated on populations that do not look like you. The result is chronic underdiagnosis and delayed treatment in a group that can least afford the delay.
🩺 I am a cardiologist. I see South Asian patients in my practice who were told their numbers looked fine, came to me at 42 with significant coronary artery disease, and had no idea the standard workup had failed them. This is not rare. This is a pattern.
A patient who gets an advanced lipid panel including ApoB and Lp(a), a coronary artery calcium score, and an honest conversation about their ethnic risk profile at age 35 can catch disease at a stage where aggressive prevention changes the trajectory entirely.
That is the difference between a stent at 44 and a clean scan at 55.
❤️ Bottom line:
South Asian ancestry is not a footnote. It is a primary variable your cardiologist needs to account for.
The UK Biobank data covering hundreds of thousands of individuals confirms the risk is real, it is large, and standard calculators miss it.
If you are South Asian, ask your doctor specifically about ApoB, Lp(a), a coronary artery calcium score, and whether your 10-year risk estimate has been adjusted for your ancestry.
Do not wait for symptoms. This population gets disease earlier, and symptoms often arrive late.
The question is no longer whether South Asians face higher cardiac risk. The question is whether your doctor is actually acting on it.
#Cardiology #HeartDisease #HeartHealth #CardiovascularHealth #SouthAsianHealth #HeartAttackPrevention #LipoproteinA #ApoB #PreventiveCardiology #MetabolicHealth

12
1,352

Jun 11
Any #restaurants serving home style phulkas with dry veg subzis in South #Bengaluru?
26
39
14,834

🏆 From a 4-year-old diagnosed with Type 1 Diabetes to Grand Slam champion.
Alexander Zverev’s victory is a reminder that T1D is a challenge, not a limitation.
Behind every match are countless decisions about insulin, glucose, nutrition, and training.
Zverev was diagnosed at age 4 and has spoken openly about managing T1D throughout his career. He also launched the Alexander Zverev Foundation to support children living with type 1 diabetes worldwide.
🌍 More than 9 million people worldwide live with Type 1 Diabetes.
Today, they have another champion to look up to.
#T1D #Type1Diabetes #AlexanderZverev #GrandSlam #DiabetesAwareness

4
20
92
3,403


3
1
41
1,019