
Co Director, Gay disabled Christian, LGBTIQ 🌈& disability advocate, author - views are my own - I am exploring @jpmasters@aus.social @jasonpmasters (Threads)
Joined August 2008
- Tweets 67,385
- Following 2,035
- Followers 3,622
- Likes 205,127
1,333 Photos and videos








Pinned Tweet

Just published an article on Medium around JK Rowling and the Transgender Community.
My thoughts as a response to JK Rowling's blog justification of her beliefs around transgender women. link.medium.com/MBb8mSwyi7
86
45
192
Do you want some help controlling your multiple AI tools. My free toolset is available from the link below and a quick overview video.
#AIControls

A little resource I have been working on
An educational video on a free documentation toolkit for non-technical users to manage AI-assisted tasks and activities without losing control. To download the free resource, go to github.com/JPMasters-AUS/ai-…
(Please be generous with the video; this is the first time I have used Final Cut Pro🫣. It is a lot more complicated than the tools I am used to, so I am learning on the job and am aware the video is a bit clunky in parts. Hopefully the next will be better.😀)
#Auspol2026 #AI #Documentation
youtu.be/gqPZes8hq8A?si=PSb2… via @YouTube
1
The double standard is a triple standard. Support for :
Iran
Ukraine
But 100% ignores the genocide of the Palestinian people and those in South Lebanon.
#Auspol2026
Jun 13

Australia on Iran:
"Attempts to kill, kidnap, harass, intimidate or otherwise attack people on our soil, undermine international norms. These actions must stop immediately."
Funny how Penny Wong never demands Israel "stop immediately" for far worse, evidenced violations #auspol

1
49
🇦🇺@JPMasters 'Strive for Equity' (He/Him/They) retweeted

Joining a big crowd here outside Bisalloy in the Illawarra to picket this site and stop steel exports that are being used to facilitate land theft and genocide - come down for an AUKUS teach in at 9pm ✊


21
151
491
3,452
🇦🇺@JPMasters 'Strive for Equity' (He/Him/They) retweeted

This afternoon @MaryKostakidis was awarded the Gary Webb Freedom of the Press Award by @unjoe @Consortiumnews Mary is the 3rd Australian recipient of this award.
Let’s celebrate Mary who stands tall in the face of those who try to silence her, and all of us 👏

28
391
1,017
10,238
🇦🇺@JPMasters 'Strive for Equity' (He/Him/They) retweeted

After a transgender woman lowers her level of testosterone, there is no inherent reason why her physiological characteristics related to athletic performance should be treated differently from the physiological characteristics of a non-transgender woman.


Under the recently passed (& now being considered by the Supreme Court) Idaho law, an individual whose sex is disputed for purposes of competing in athletic activities for women and girls is instructed to “verify the student’s biological sex” by providing a signed physician statement after an examination relying only on one or more of the following: the student’s reproductive anatomy, genetic makeup, or normal endogenously produced levels of testosterone.
None of these physiological characteristics alone or in any combination can “verify” sex, nor are any of them alone or in any combination accurate proxies for athletic advantage.
As noted above, one does not verify sex by a examining these characteristics, alone or in combination. A person’s sex is made up of multiple biological characteristics and they may not all align as typically male or female in a given person.
A person’s genetic make-up and internal and external reproductive anatomy are not useful indicators of athletic performance and have not been used in elite competition for decades.
A blood test is generally used to test circulating testosterone. The blood test does not distinguish between exogenous and endogenous testosterone. Exogenously administered testosterone can be identified with a urine test. However, the urine test will only determine that there is current use of exogenous testosterone. The urine test is not relevant when the person is not taking exogenous testosterone.
The urine test will not measure what endogenous testosterone levels would be absent suppression. For a person suppressing testosterone as part of a medically prescribed treatment plan for gender dysphoria, neither blood testing nor urine testing would specify testosterone levels without suppression. There is no way to test for “normally produced” endogenous testosterone without taking people off of prescribed medication, which would be dangerous.
Idaho’s new rule creates an outright bar based on endogenous testosterone without even specifying the endogenous serum testosterone level that one would need to demonstrate to “verify” sex.
Under the Idaho rule, no amount of reduction of one’s testosterone level could ever be adequate. Further more, people without active testosterone receptors experience none of the athletic impact of the hormone despite having high levels of circulating testosterone. They too would appear to be disqualified under Idaho’s rule.
The legislative findings for H.B. 500 contend that even after receiving gender-affirming hormone therapy, women and girls who are transgender have “an absolute advantage” over non-transgender girls. This assertion is based on speculation and inferences that have not been borne out by any evidence.
First, these arguments overlook the population of transgender girls and women who, as a result of puberty blockers at the start of puberty and gender affirming hormone therapy afterward, never go through a typical male puberty at all. These girls never experience the effects of high levels of testosterone and accompanying physiological changes. They go through puberty with the same levels of hormones as other girls and develop typically female physiological characteristics, including muscle and bone structure. Idaho’s law would bar them from participation in female athletics with absolutely no medical or scientific basis even based on the standards set forth in the legislative findings.
A transgender woman who has not gone through a typical male puberty is similarly situated to a woman with XY chromosomes who has complete androgen insensitivity syndrome, and it has long-been recognized that women with CAIS have no athletic advantage simply by virtue of having XY chromosomes.
The legislative findings also state that “benefits that natural testosterone provides to male athletes is not diminished through the use of puberty blockers and cross-sex hormones.
1-
6
4
16
528

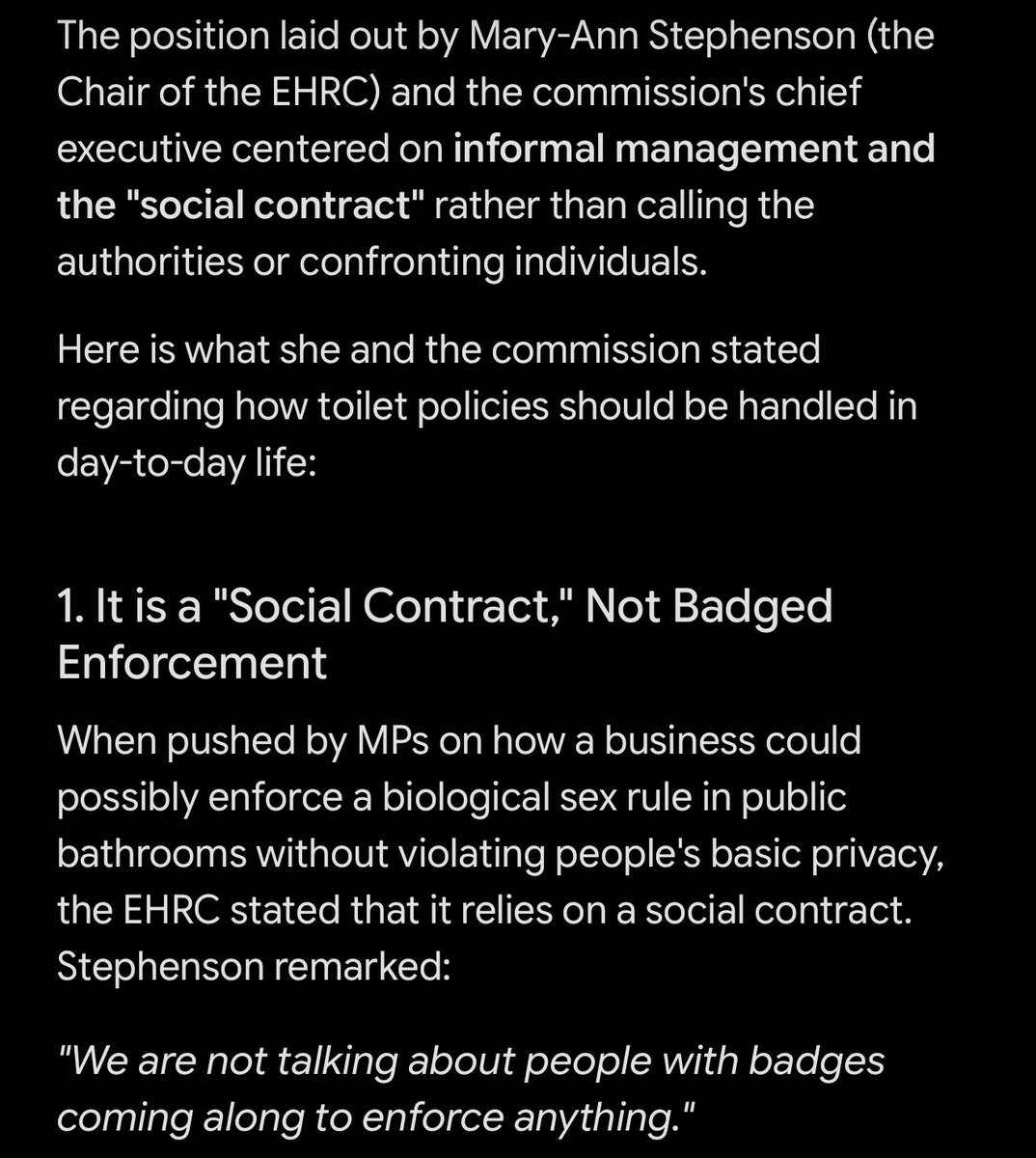
This below

Don’t listen to the TERFs.
Here is the head of the EHRC confirming that there is no toilet ban.
It is not illegal for trans women to use women’s toilets, or trans men to use men’s.
1
31
🇦🇺@JPMasters 'Strive for Equity' (He/Him/They) retweeted
The United Kingdom is a signatory to the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW), having ratified the international human rights treaty in April 1986.
By being a party to CEDAW, the UK is legally obligated to:
•Eliminate discrimination against women and girls across all areas of life, including employment, education, and public life.
•Ensure women are protected against gender-based violence, biases, and stereotypes.
The Australian Sex Discrimination Act 1984 (SDA) was enacted to give effect to Australia’s international obligations under the UN Convention on the Elimination of All Forms of Discrimination Against Women.
In the trial, the defence (Grover) argued that CEDAW only recognised biological sex and that the SDA's protection of "gender identity" was inconsistent with the treaty's definition of "women."
The Federal Court found that Australia's interpretation of CEDAW does not prevent it from broadening domestic protections to cover gender identity, and that both the SDA and Australia's CEDAW obligations protect transgender women from discrimination based on their gender identity.
The factor that persuaded the Federal Court was that the United Nations Human Rights Committee which is the one that’s empowered to hear complaints about violence under the treaty had accepted that gender identity is an other status for the purpose of article 26, the list of examples when this occurred is set out in the judgment and those examples range from 2012 to 2023 the Federal Court held that article 26 created an obligation for parties to the convention to prohibit discrimination on a number of grounds which quote may readily extend to gender identity unquote. This then provided the treaty obligation which triggers the application of the external affairs power to support the relevant provisions of the Sex Discrimination Act that addresses gender identity.
So that’s how the train of reasoning worked out.
share.google/4UMkrJ0aYu8uLY1…
1
4
10
260
RT @IndiaWilloughby: The UK is no better than Russia. Show trials.
Trans people were stripped of legal recognition last April by the UKSC,…
126
🇦🇺@JPMasters 'Strive for Equity' (He/Him/They) retweeted

Jun 13
“We live in a system where if you fight so that they don't kill any more children, you're a "terrorist" — while those who drop the bombs on those children are applauded.”
Jun 13

En Reino Unido, los jueces sionistas condenaron a más de 25 años de prisión a 4 activistas de Palestine Action, por luchar contra el genocidio en Gaza y lograr boicotear las fábricas de drones Elbit de "Israel".
Vivimos en un sistema donde si luchas para que no maten más niños eres un "terrorista"... mientras los que ponen las bombas a esos niños son ovacionados en la Casa Blanca.
11
247
448
4,767
🇦🇺@JPMasters 'Strive for Equity' (He/Him/They) retweeted
Oh gee, another coincidonk!!
Just after Indonesia says ‘NO’ to US military flight access over Indonesian territory, guess what, US funded student groups start up street riots again.
Just like clockwork.
This time the theme colour is YELLOW — for this latest in orchestrated US-sponsored Colour Revolutions!
Watch for more reporting of the ‘chaos’ in Indonesia, until the US gets its own way and gets its flight access — so it can squeeze the Malacca Strait closed to choke Chinese trade.
bbc.com/news/articles/cqx18d… @abcnews
89
1,029
2,071
45,397

Prof Jeffrey Sachs, American economist and public policy analyst. Columbia University:
"AUKUS is designed to bill the Australian taxpayers and enrich the US military industrial complex. You have been had Australia, sorry to tell you. And your politicians should own up it."

92
925
1,748
14,608
A little resource I have been working on
An educational video on a free documentation toolkit for non-technical users to manage AI-assisted tasks and activities without losing control. To download the free resource, go to github.com/JPMasters-AUS/ai-…
(Please be generous with the video; this is the first time I have used Final Cut Pro🫣. It is a lot more complicated than the tools I am used to, so I am learning on the job and am aware the video is a bit clunky in parts. Hopefully the next will be better.😀)
#Auspol2026 #AI #Documentation
youtu.be/gqPZes8hq8A?si=PSb2… via @YouTube
7
🇦🇺@JPMasters 'Strive for Equity' (He/Him/They) retweeted

Jun 13
Angus Taylor caught clueless in WA, unable to name the very electorate he’s holding a press conference in.
“Do you not know the seat you’re standing in right now?”
“Seriously do you not know…?”💥🔥
No he doesn’t 🤣 Staggering. #auspol
169
572
1,942
66,016
🇦🇺@JPMasters 'Strive for Equity' (He/Him/They) retweeted
Jun 13
Raf Epstein calls out blatant favouritism media gives Pauline Hanson
“She could never say ‘show me the good Jews”
“She says that about Muslims”
“If she said that about Jews there’d be a discussion on this couch whether or not she should be prosecuted under hate laws”💥🎯 #auspol
239
1,242
5,095
180,974
Conservative Christian around the world continue to protest against LGBTIQA people, which is an act against the teaching of Jesus.
The ongoing use of religious as a cover of hate and darkness has to continue to called out.
The current attack on transgender people in Australia, is part of a global anti-transgender movement funded by conservative Christians in the USA.
British gay’s have not been allowed to enter the USA as spectators for the @FIFAWorldCup!
For those suggestion that the US attack on transgender people won’t be extended to the broader LGBTIQA community are living in a fairly land.
#Auspol2026 #ligbtiqaHumanRights
ground.news/article/lgbtq-qu…
35
It is unfortunate that in the state of the world and the corruption in both the USA and @FIFAWorldCup, the @guardian decided to publish such offensive dribble.
#MykeBartlett’s article would make sense in a ‘normal’ world. I know they are passionate about this sport and coach a kids league (according to previous articles).
However, such an article shouldn’t sweep under the rug any of the following:
- The USA rejecting team personnel from entering the USA
- The USA rejecting one of the world’s top soccer referees
- The USA rejecting an Australian citizen on arrival to be a spectator
- The USA allowing a World Cup player into the USA even though they are an alleged rapist (on multiple charges).
This is before we get to:
- The racist approach to who can and can’t enter the USA to play or spectate
- The authoritarian approach to who can and can’t enter the USA to play or spectate
- The fact that the USA has attacked at least three countries so far this year, none of whom have attacked the USA in recent years.
- The USA’s ongoing support of the genocide being committed by the Israeli Government in both Gaza, the West Bank and Lebanon.
- The fact that the US Government is randomly putting into prison US citizens and others without any due process.
Glorify the World Cup and @FIFAcom as much as you like, but they are enabling a fascist and authoritarian regime to continue their practices. It is the German Olympics all over again.
#Auspol2026
theguardian.com/commentisfre…
151
Not unexpectedly, the USA allow an alleged rapist @FIFAWorldCup player into the US!
@Socceroos this is what your attendance is supporting, racism and alleged rapist.
#Auspol2026
theguardian.com/football/202…
42
🇦🇺@JPMasters 'Strive for Equity' (He/Him/They) retweeted

Jun 12
Women have been saying for years that there is a growing backlash against gender equality, and every time the conversation comes up we’re told we’re imagining it.
Now the United Nations is saying it.
According to a UN report, nearly 1 in 4 countries reported setbacks in women’s rights and gender equality. Hundreds of millions of women and girls are living in conflict zones, violence against women remains widespread, and UN officials are warning about a growing backlash against women’s rights worldwide.
The part that stands out to me isn’t even the statistics. It’s that women have been raising concerns about misogyny, online hostility toward women, violence, and attacks on reproductive rights for years, only to be dismissed as overreacting.
If the UN Secretary-General is warning about the “mainstreaming of misogyny,” maybe it’s time to stop pretending these concerns came out of nowhere.
Do you think women’s rights are genuinely facing setbacks, or do you think organizations like the UN are exaggerating the problem?

250
2,544
6,462
112,083
🇦🇺@JPMasters 'Strive for Equity' (He/Him/They) retweeted

Jun 11
🚨 WTF?! A USS Liberty survivor drops a massive bombshell.
He confirms they were threatened with prison or worse if they ever spoke about the Israeli attack.
Another veteran explicitly states "Israel owns us" after being ignored by Congress for 59 years. Total betrayal!
Jun 11

🚨 DISGUSTING: Patriot Rep. Thomas Massie exposes how the Washington establishment completely ignored the USS Liberty survivors for 59 years!
He reveals these brave men, now in their 80s, still have Israeli shrapnel in their bodies that sets off Capitol metal detectors.
549
24,509
76,308
2,234,777