
art director turned NYC paramedic. currently attempting to medic at higher altitudes in CA. airway nerd. first pass success is hot. 0pINiOnS mY OwN 🤡
Joined January 2016
- Tweets 1,556
- Following 822
- Followers 1,025
- Likes 5,299
377 Photos and videos






kathryn chadason retweeted

7 May 2025
Hey EMS docs/fellows, there is a job opening for an EMS medical director with a cool system. Let me know if you can't find the link or any questions. Let people know.
Ping @NoobieMatt @ResusPadawan @emtrnmd @benabo @mowwyjane
joinfdny.com/careers/current…
1
4
10
1,003
kathryn chadason retweeted

2 May 2025
But what about EMS???? Asking for a few thousand friends. #EMS #payparity
1 May 2025

I'm a blue-collar mayor, and our administration is proud to support the blue-collar workers who keep our city running.
We settled contracts with 100% of our city's uniformed workforce to make sure public servants get the pay and benefits they deserve this May Day and every day.
5
20
799
kathryn chadason retweeted

PAC is now available in Europe with upcoming events in Germany and Austria. Check it out! theprotectedairway.com/2025/…
4
15
1,031
kathryn chadason retweeted

2 Apr 2025
Even if no obvious clinical or procedural gaps exist, dig into:
🔍 Clinical reasoning nuance
🎭 Communication with patients/families
🤝 Team dynamics
🧠 Efficiency, prioritization, resilience
These are advanced skills that benefit from coaching.
1
1
1
151
kathryn chadason retweeted

18 Mar 2025
So by all means, push the next big breakthrough. But don’t forget the places that won’t see it for years. Because no algorithm is coming to intubate at 3 AM. No AI is staffing the fluorescent hallways. People are.
10
57
645
11,770
kathryn chadason retweeted
1 Mar 2025
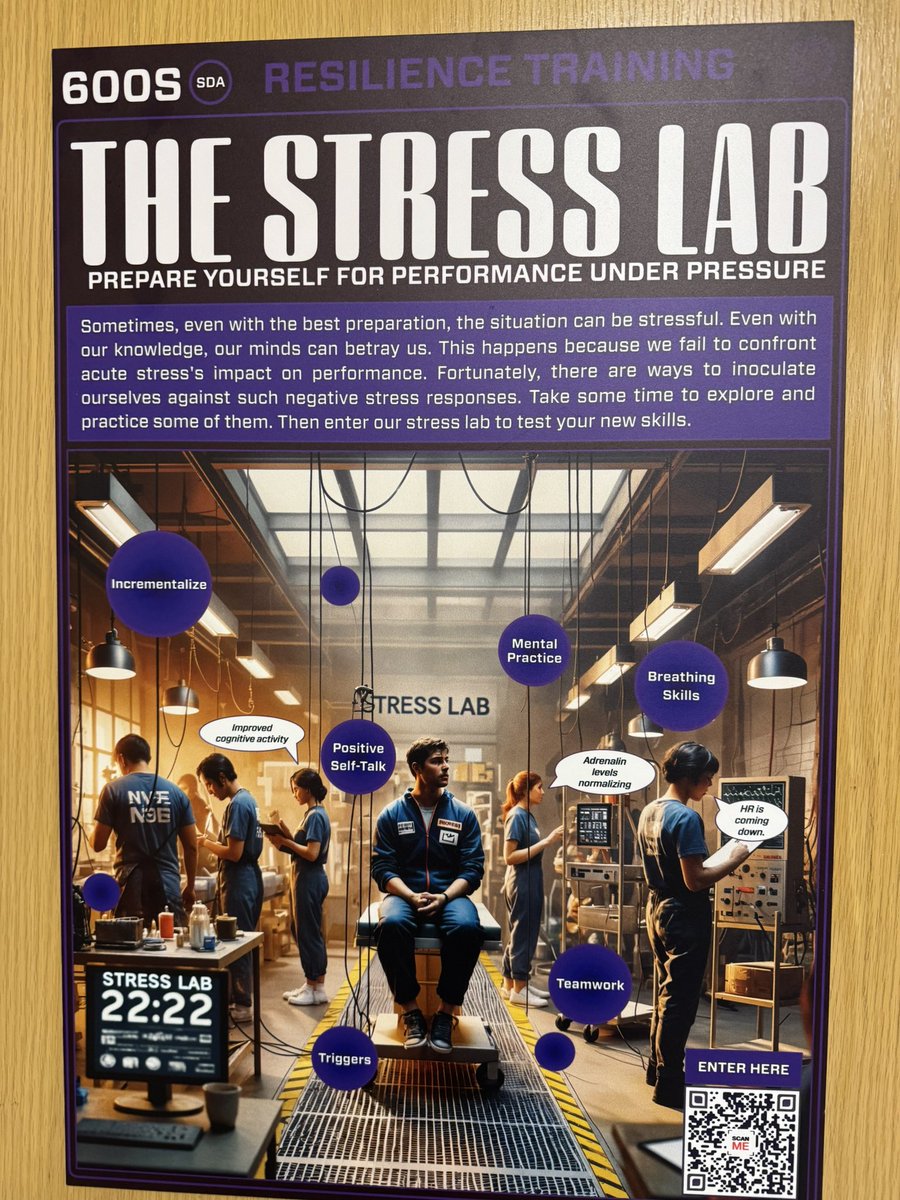
Protected Airway Course 2025 is all about innovation & teamwork - proud to be faculty doing Stress Lab 2.0 with a fantastic group of multidisciplinary clinicians. High-stakes airway management meets stress inoculation!

3
9
837
kathryn chadason retweeted

3 Mar 2025
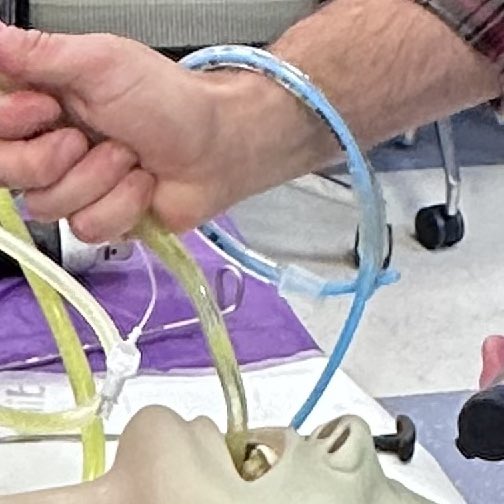
Had a blast helping out with the Protected Airway Collaborative this past weekend. DL, VL, FONA, SALAD, BEEF SALAD, and more! Learning with expert educators on innovative sims and cadaveric models was a great way to spend the weekend. And hanging with airway nerds!

1
5
41
2,226
kathryn chadason retweeted
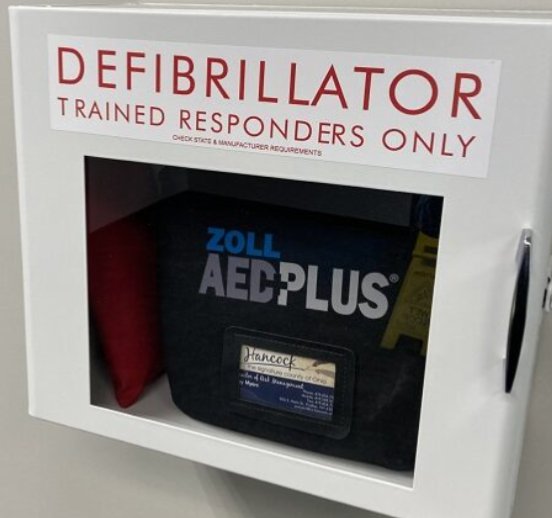
20 Feb 2025
Saw an AED at school today with a warning like this.
We wonder why bystander AED use is so low? We deter people from using it!
16
14
105
17,380
kathryn chadason retweeted

16 Feb 2025
My new #SALADSim will be at the NYP Protected Airway Course March 1st. theprotectedairway.com/

3
4
20
1,550

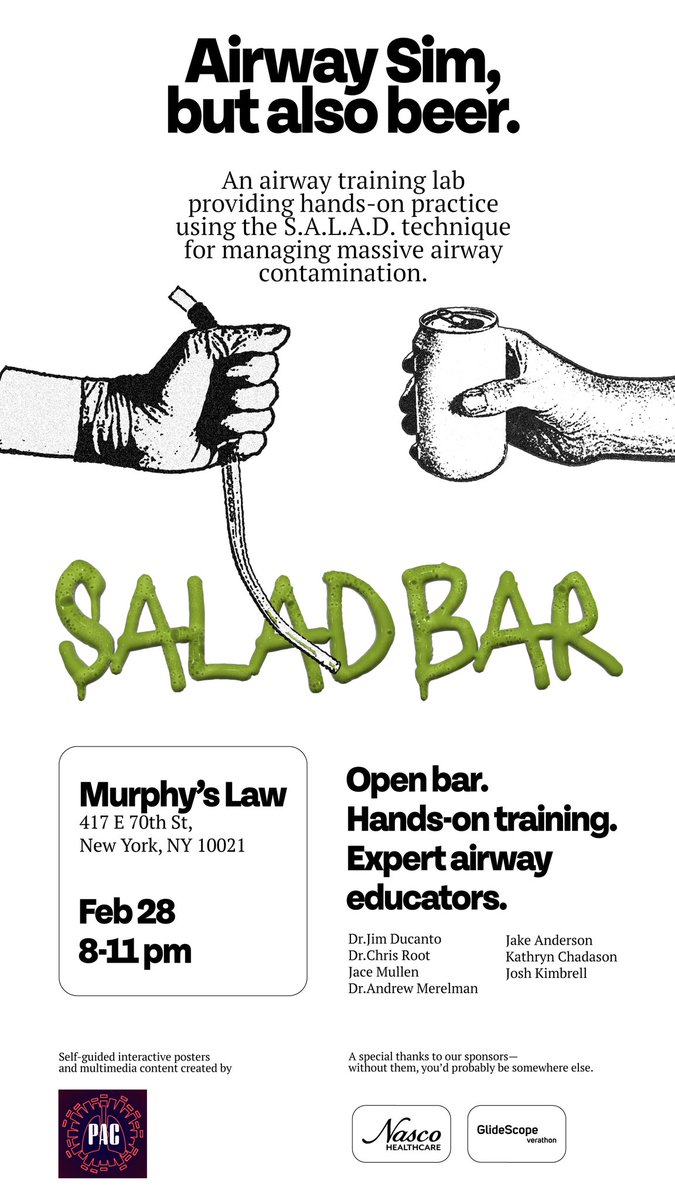
18 Feb 2025
Cuz are you really that good at S.A.L.A.D. if you can't do it with a beer in hand?
Beyond stoked for this event alongside some of my fav airway wizards @jducanto @JaceMullen @ChrisRootMD @amerelman @joshkimbre & interactive posters @ProtectedAirway
RSVP
Www.saladbar.events
3
15
984
5 Nov 2024
#medtwitter #medictomd doomscrolling distraction activity:
Any recommendations for MCAT prep books etc? Preferably on the thorough side vs. refresher material #artschool for undergrad lol
figured I’d start getting familiar w the content as I’m chipping away at my post bacc🤓
2
10
734
29 Oct 2024
love that my pre-calc teacher keeps referring to the founding mathematicians we’re learning about as our “great-great-grand professors”
1
5
377
20 Oct 2024
Now that I’m at a job where “safety naps” are encouraged Im realizing how silly&unsafe it was for my prev EMS gig to write u up/threaten to fire u if u got caught napping b/w calls. I know, it’s a PR thing, but maybe posting on a street corner for 16 hrs is the issue, not naps?🫶
3
7
69
3,450
kathryn chadason retweeted
15 Oct 2024
Perhaps a dangerous question to ask, but… any Philadelphia based paramedics out there that can facilitate a ride along next week for me, as I’m attending and presenting at the American Society of Anesthesiology next week in Philadelphia? If I’m going to be of further assistance to Paramedicine I need to see what you’re up against.
8
4
25
4,808
kathryn chadason retweeted

14 Oct 2024
for patients who are legit trying to die from bradycardia, I advocate using epinephrine 1st
epinephrine is more reliably effective & honestly just a better anti-death medication
I've seen patients arrest while folks were messing around w/ atropine
more:
emcrit.org/pulmcrit/epinephr…
14 Oct 2024

Bradycardia
Anyone with symptomatic bradycardia gets atropine as the "best initial step". This means mainly hypotension, syncope or altered mental status. If symptoms of hypo-perfusion persist, then the answer is "pacemaker."
11
23
210
41,313
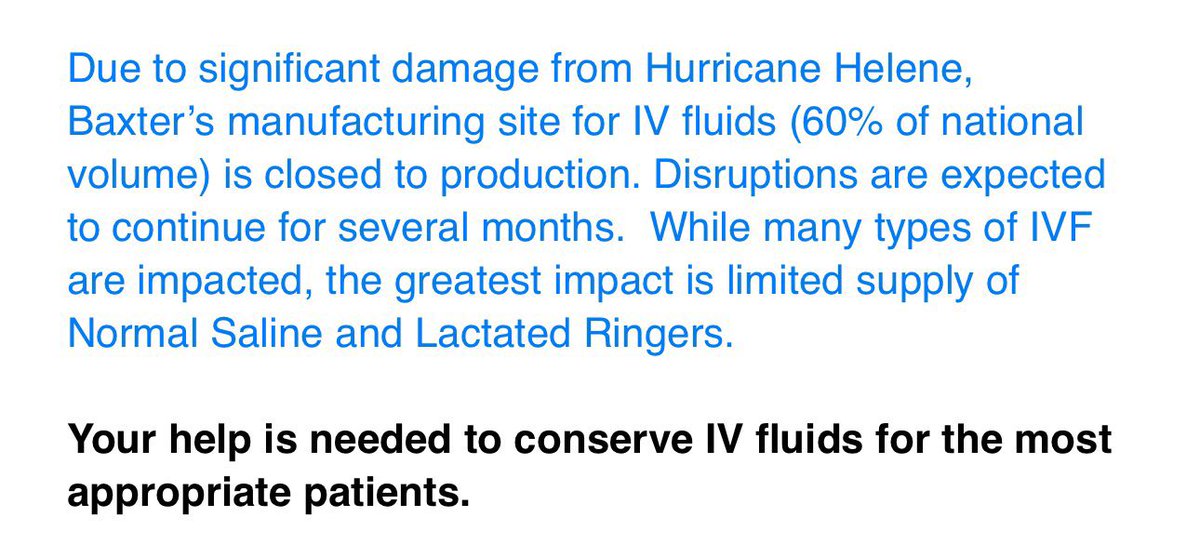
4 Oct 2024
Well, this’ll be fun 🫠
3 Oct 2024

I for one am looking forwards to improvising volume resuscitation with a continually rotating bevy of weird fluids.
what do we have today? plasmalyte? one third normal saline with phos? 5% albumin? hetastarch? gelofusine? 23% saline drizzled over D5W? LFG
4
581
4 Oct 2024
If this ever gets put into pre hospital use I will exclusively be referring to it as
“trauma hummus”
thank you @joshmcgoo
3 Oct 2024

Trauma Hummus
3
326
1 Oct 2024
Never fully grasped the phrase
“if you’ve seen one ems system you’ve seen ONE ems system”
until moving NYC->CA & having to get accredited in 5 counties in order to work out of ONE hems base location
I get the diff needs for rural vs urban but wow are we a disjointed bunch 🤡
1
1
11
921
1 Oct 2024
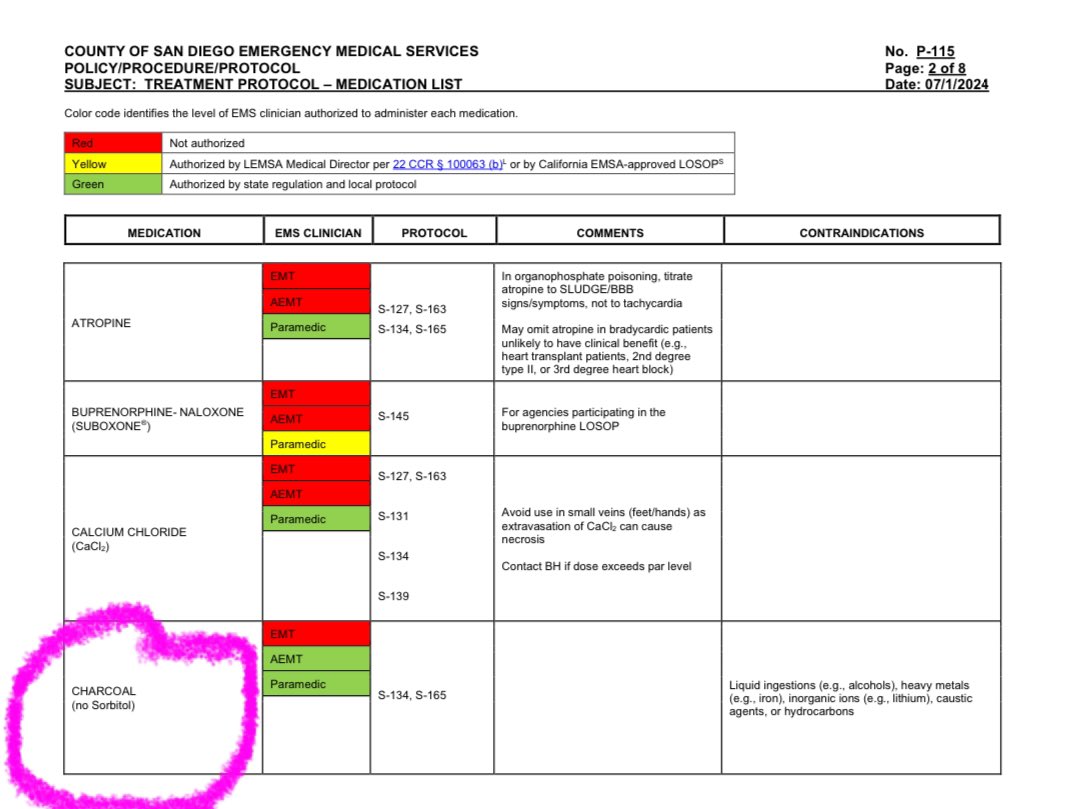
EMTs txp-ing us from LZ to ER just told me they don’t carry AEDs or glucometers…but hey, at least they have activated charcoal???🤡
I’ve come to terms w. the fact that EMS scope in SoCal is basically medical malpractice but this is a new lvl of WTF…
Why is it SO bad here? :(
5
10
1,655
1 Oct 2024
Are there EMS services in ur area that don’t carry AEDs?
1%
Yes
47%
No
52%
How is this a question?
77 votes • Final results
2
2
2
730