Solo practice nephrologist in the Golden State, husband, father, swimmer, skier, and landlocked surfer. #nephrology #solopractice #dialysis
- Tweets 951
- Following 1,978
- Followers 1,090
- Likes 1,414















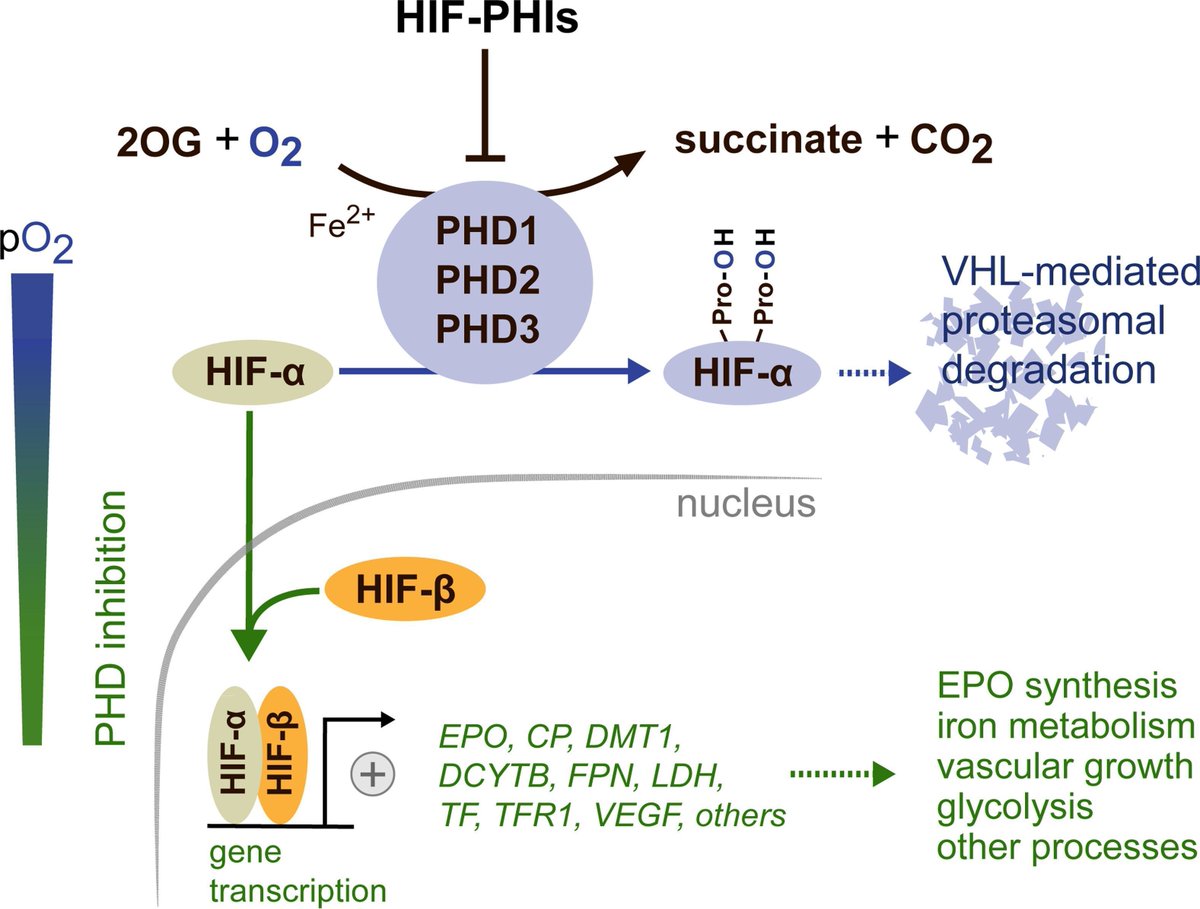
ALT Reversible HIF activation by pharmacological HIF-prolyl-hydroxylase inhibition. Schematic overview of hypoxia-inducible factor (HIF) regulation. The oxygen-sensitive HIF-α subunit is continuously synthesized and rapidly degraded under normoxic conditions. Proteasomal degradation of HIF-α is initiated by prolyl hydroxylase domain (PHD) dioxygenases and mediated by the von Hippel-Lindau (VHL)-E3-ubiquitin ligase complex. PHD dioxygenases, PHD1, PHD2 and PHD3 utilize molecular oxygen and 2-oxoglutarate (2OG) as substrates to hydroxylate the oxygen-sensitive HIF-α subunit at specific proline residues (Pro), with PHD2 being the main regulator of HIF activity in most cells.


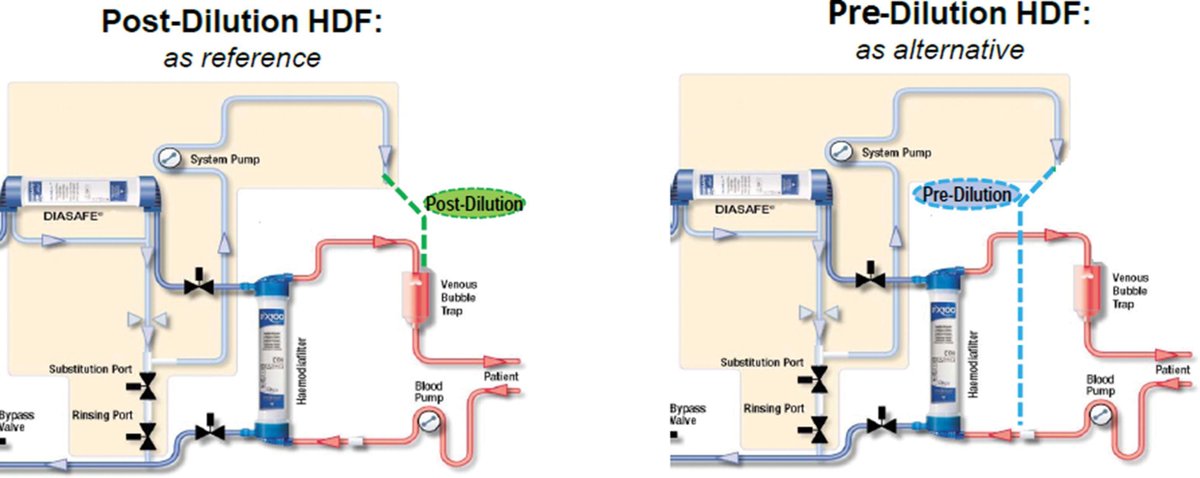
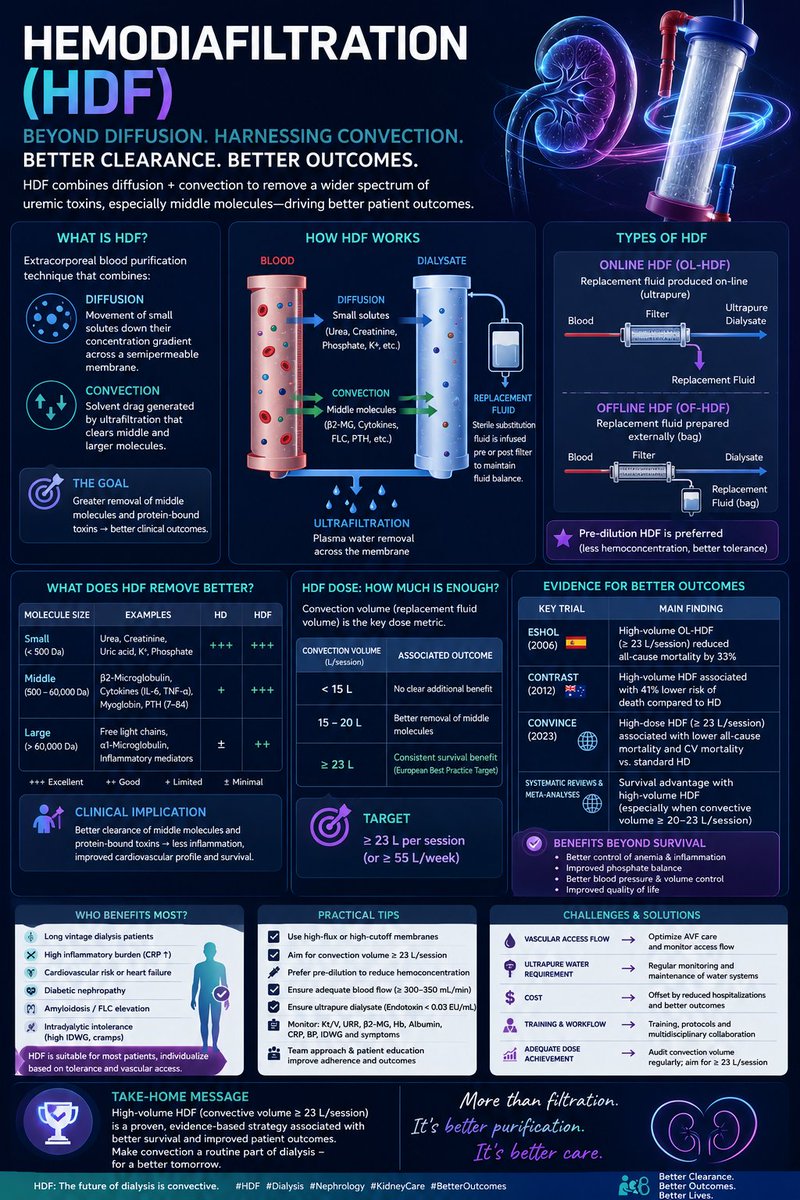
ALT Dilution Modes in Hemodiafiltration. Released under a CC BY 3.0 license from Imamovic et al





ALT