
Learn point-of-care ultrasound (POCUS) and become a clinician of the modern era: buff.ly/NQNsl0L
Joined May 2020
- Tweets 2,754
- Following 280
- Followers 14,310
- Likes 466
881 Photos and videos






Pinned Tweet

8 Oct 2025
The hardcover version of The POCUS Textbook is officially released!!!!
Get a copy: amazon.com/dp/B0FV93KW7C/ref…
🏥100 Figures without abbreviations
💊Dozens of videos accessible by QR code with NO passwords and NO paywalls
🩹Step-by-step tutorials by Dr. Istrail for all experience levels.
@NephroP @Wilkinsonjonny @iceman_ex @POCUSpeek #foamed #meded #MedTwitter
4
17
3,232
POCUS Med Ed retweeted

Jun 10
I love POCUS and ECG. For interest, lets take a look at this case from more of an ECG perspective (with extra analysis of these ECGs by the Queen of Hearts @PMcardioApp):
1st ECG:
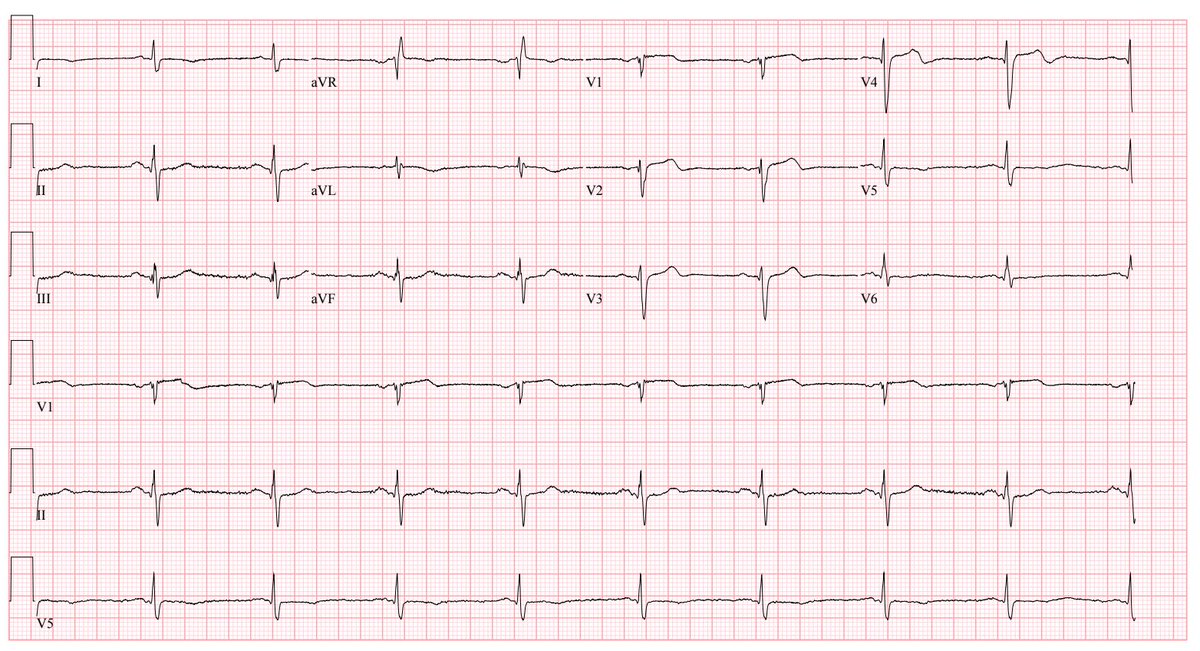
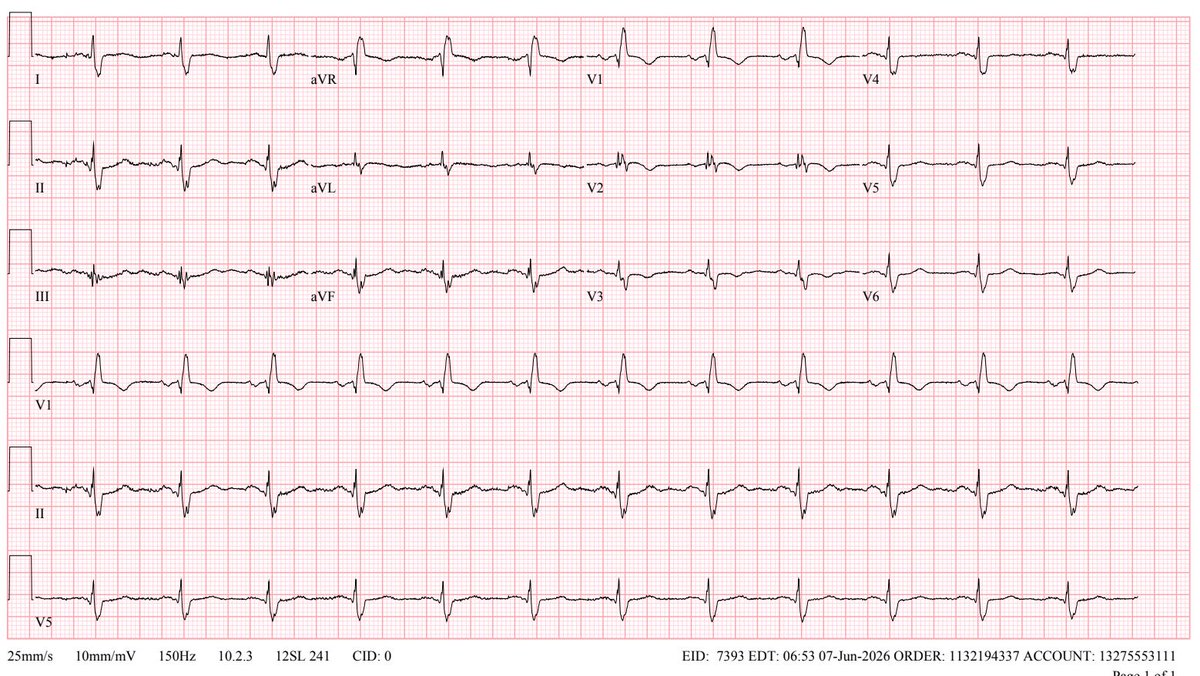
1⃣ NSR with RBBB
1⃣To my eye this is nonspecific (could be PE, CTEPH, or ischemia).
1⃣ The queen doesn't see ischemia either. But she does flag this as reduced LVEF (<40%) which is unexpected and should be a red flag that something weird is happening.
2nd ECG:
2⃣ RBBB has resolved and now we can discern ischemic STE with TWI in V1-V4. Resolving chest pain and emerging TWI suggest that he may have experienced a transient occlusion overnight with re-perfusion.
2⃣ Could the right precordial TWI be due to PE? It's possible but less likely. Absence of TWI in the inferior leads argues against PE. Significant STE with mild TWI seems more consistent with MI than PE.
2⃣ The queen flags this as a high-risk NSTEMI with 88% probability and continues to flag a reduced LVEF.
2⃣ At this point it's increasingly clear that we're dealing with LAD-territory ischemia. Transient LAD ischemia explains the transient RBBB seen on the 1st ECG (septal perforators from the LAD perfuse the right bundle). The queen keeps on telling us the EF is low. Cardiac cath needed.
In retrospect, I think the RBBB pattern may have camouflaged a subtle Wellens pattern in the first ECG.
Overall, the ECG and echo data play out in parallel.
Jun 10

Reason number 78958 why #pocus is so important: sometimes a patient has multiple acute diseases at the same time.
A middle-aged man presented with acute chest pain that woke him from his sleep. He had a recent DVT diagnosed 2 weeks prior and had been on Eliquis without missing any doses.
His vitals were normal, and his initial ECG is shown below. His high-sensitivity troponin was mildly elevated, and his BNP was normal.
@im_crit_ @NephroP @RJonesSonoEM
2
9
46
8,089
Jun 10
Reason number 78958 why #pocus is so important: sometimes a patient has multiple acute diseases at the same time.
A middle-aged man presented with acute chest pain that woke him from his sleep. He had a recent DVT diagnosed 2 weeks prior and had been on Eliquis without missing any doses.
His vitals were normal, and his initial ECG is shown below. His high-sensitivity troponin was mildly elevated, and his BNP was normal.
@im_crit_ @NephroP @RJonesSonoEM
6
10
41
11,753
Jun 10
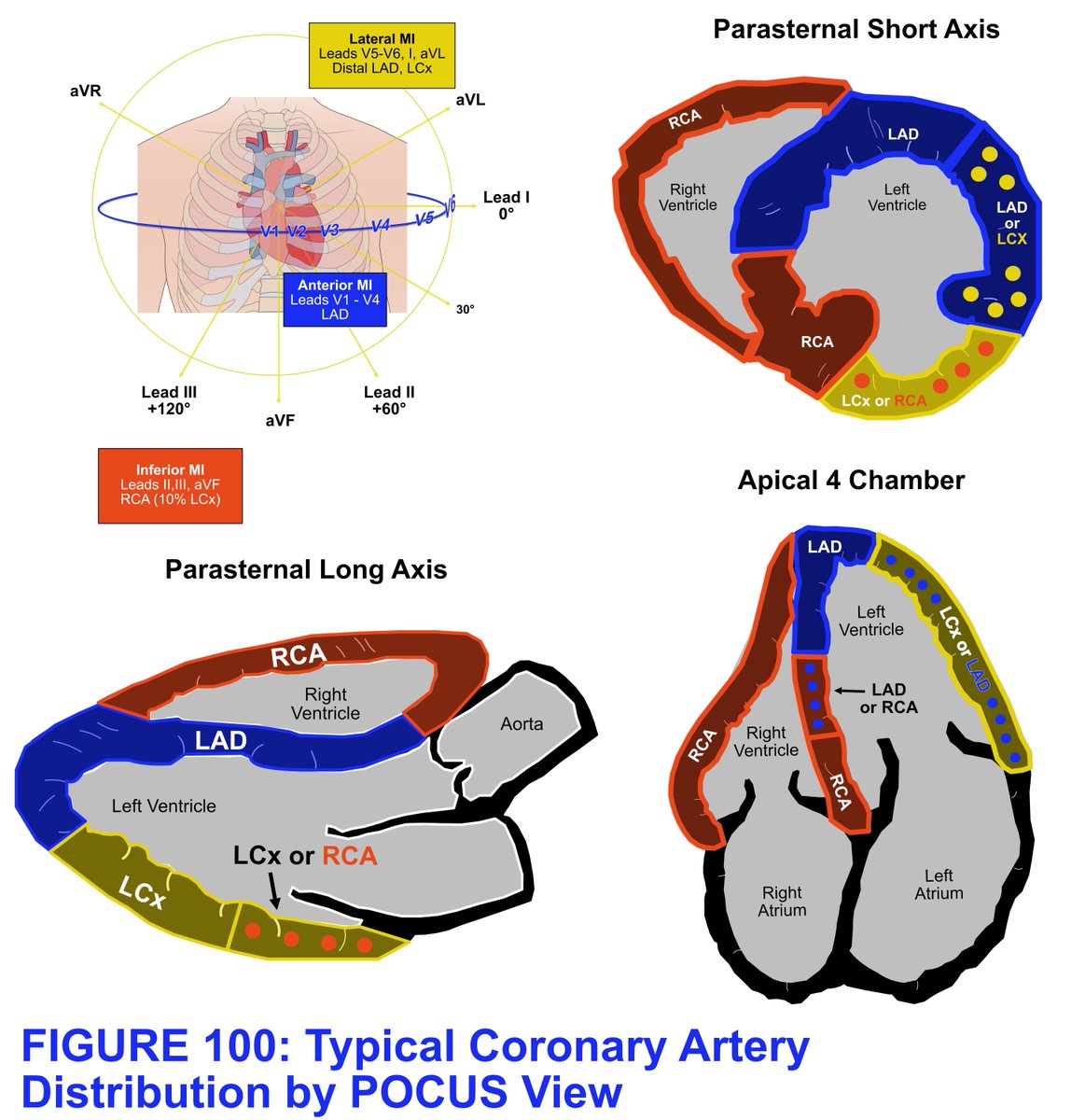
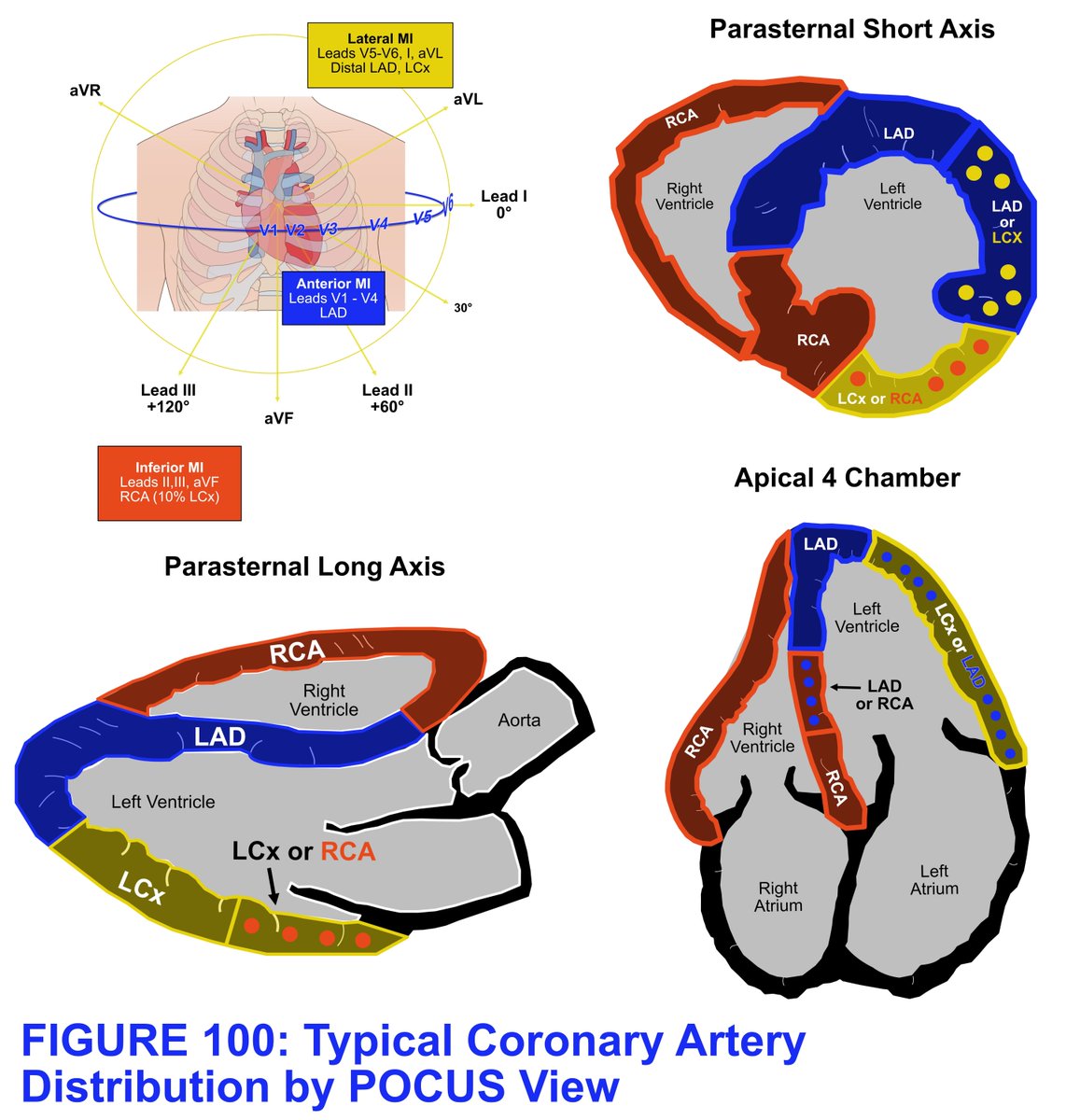
With this information, the cardiology team was consulted. He underwent an urgent left and right heart catheterization, which showed a completely occluded Left anterior descending artery with TIMI 0 flow and normal pulmonary pressures. A stent was placed, and his chest pain resolved.
1
3
508
Jun 10
This was a remarkable case in which the patient's signs and symptoms were all clearly explained by his admitting diagnosis. However, he had another more urgent issue that probably would not have been detected for at least 24 more hours if his troponin continued to rise or his complete echocardiogram had been completed.
THIS is why #pocus is so important!!
To learn more about how to use POCUS in a case like this, consider getting a copy of The POCUS Textbook: buff.ly/ihLPypC
2
490
POCUS Med Ed retweeted

Jun 8
Consent✅
"I’m at the Point of Breaking – Hang 10, take it thighs-an easy, I’m Hunting for a solution"
Runner, surfer
Massive ramp up in marathon training – rapid onset medial mid to lateral burning thigh pain (see pain map below) with low grade parasthesiae
Exacerbated by deep knee flexion and running beyond 20 mins and a faster pace
Struggled further on surfing holiday in prone on board and kneeling
MRI excluded femoral bone stress injury and no adductor injury or knee intra-articular / ligamentous injury
OE –
Meniscal and ligamentous testing normal
Lumbar spine and hip joint cleared
POCUS video reel –
Adductor magnus tendon & wider musculature normal
Saphenous nerve swollen at mid Hunter’s canal point – almost same calibre as the adjacent femoral artery! (point of maximal tenderness with probe pressure - Tinel's positive)
US guided hydrodissection (LS) – soft tissue planes around SN seen to open up effectively
Post procedure – complete abolition of pain on treadmill running and deep squats for the first time in 8 months (excuse the language)
Pearls -
This area is diagnostic ‘No Man’s Land’ – ie, if there is no femur bony pathology, and in the absence of trauma, it can only really be neural
‘Adductor splint syndrome’ – a form of bone stress injury – is one of the key medial thigh pain differentials in runners
Research links –
‘Surfer's neurapraxia - an uncommon surfing injury of the saphenous nerve’
pubmed.ncbi.nlm.nih.gov/3897…
‘Adductor insertion avulsion syndrome (thigh splints): spectrum of MR imaging features’
pubmed.ncbi.nlm.nih.gov/1151…

9
16
134
16,061
Jun 8
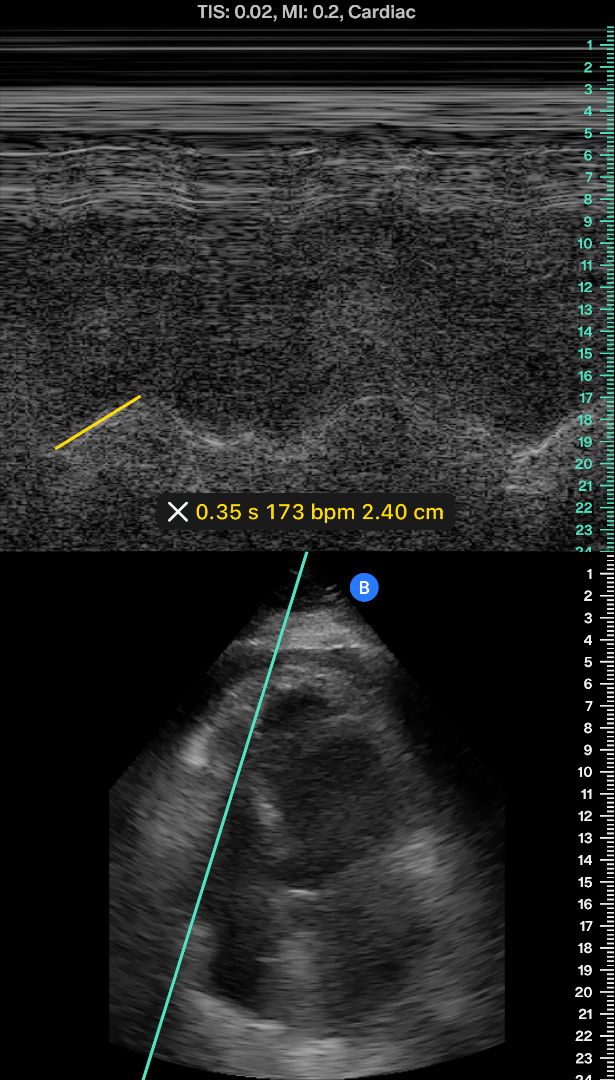
When a pulmonary embolism is large enough to obstruct flow, the right ventricle strains against the resistance, and its response is measurable at the bedside with POCUS.
The findings are specific. Their absence does not rule out PE, but their presence is highly informative.
2
11
41
2,100
Jun 8
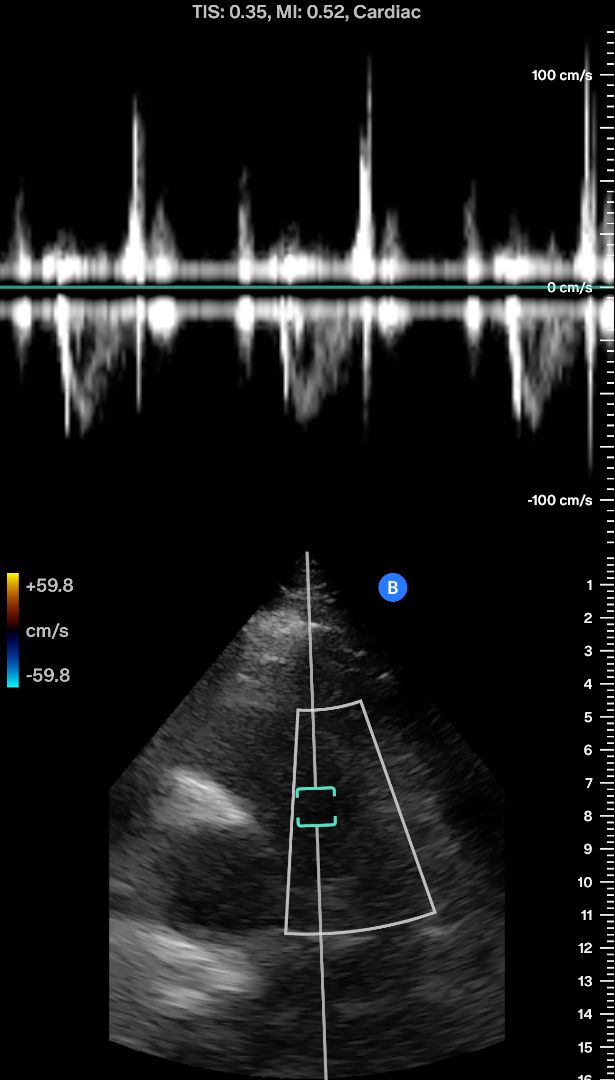
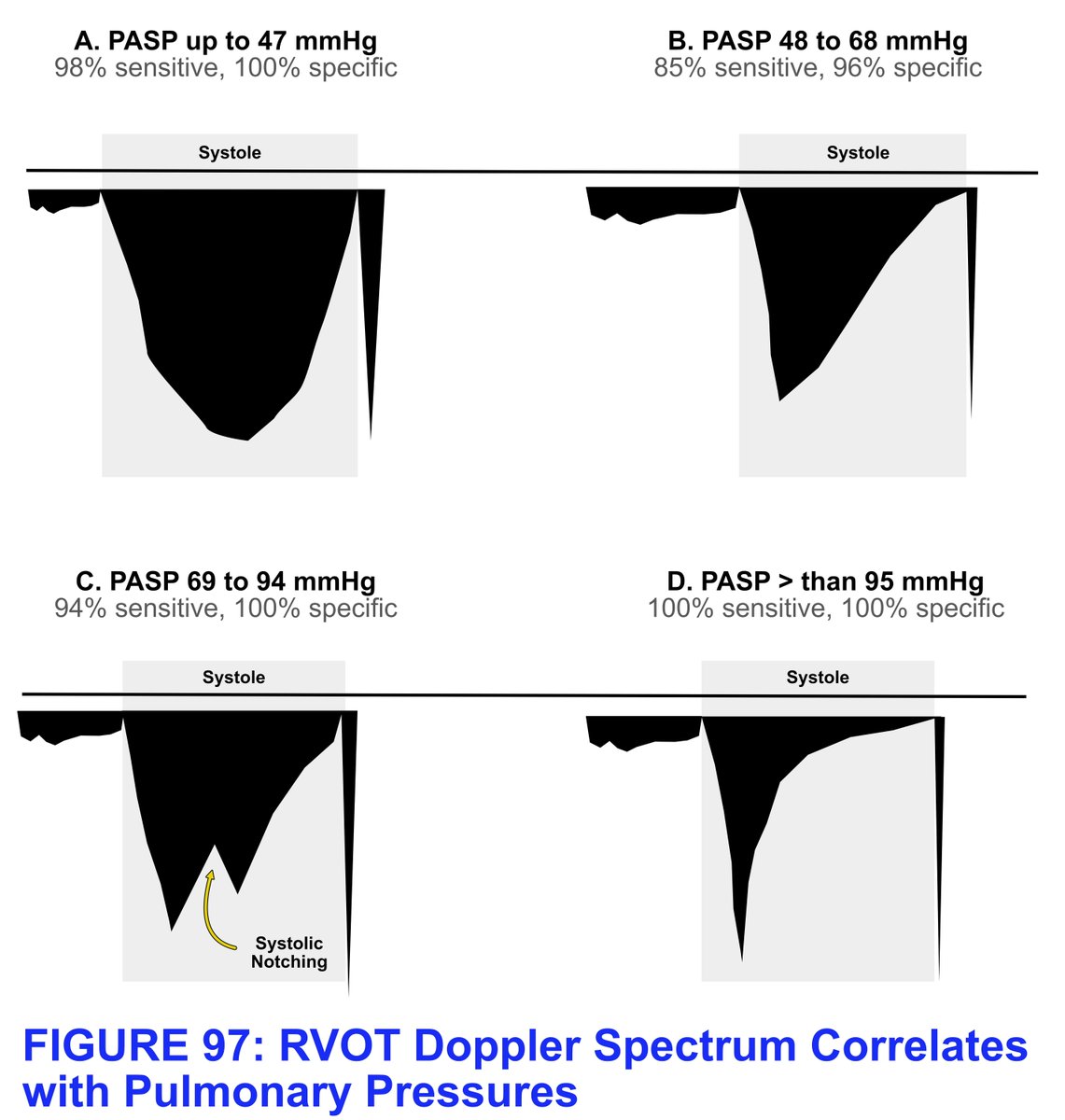
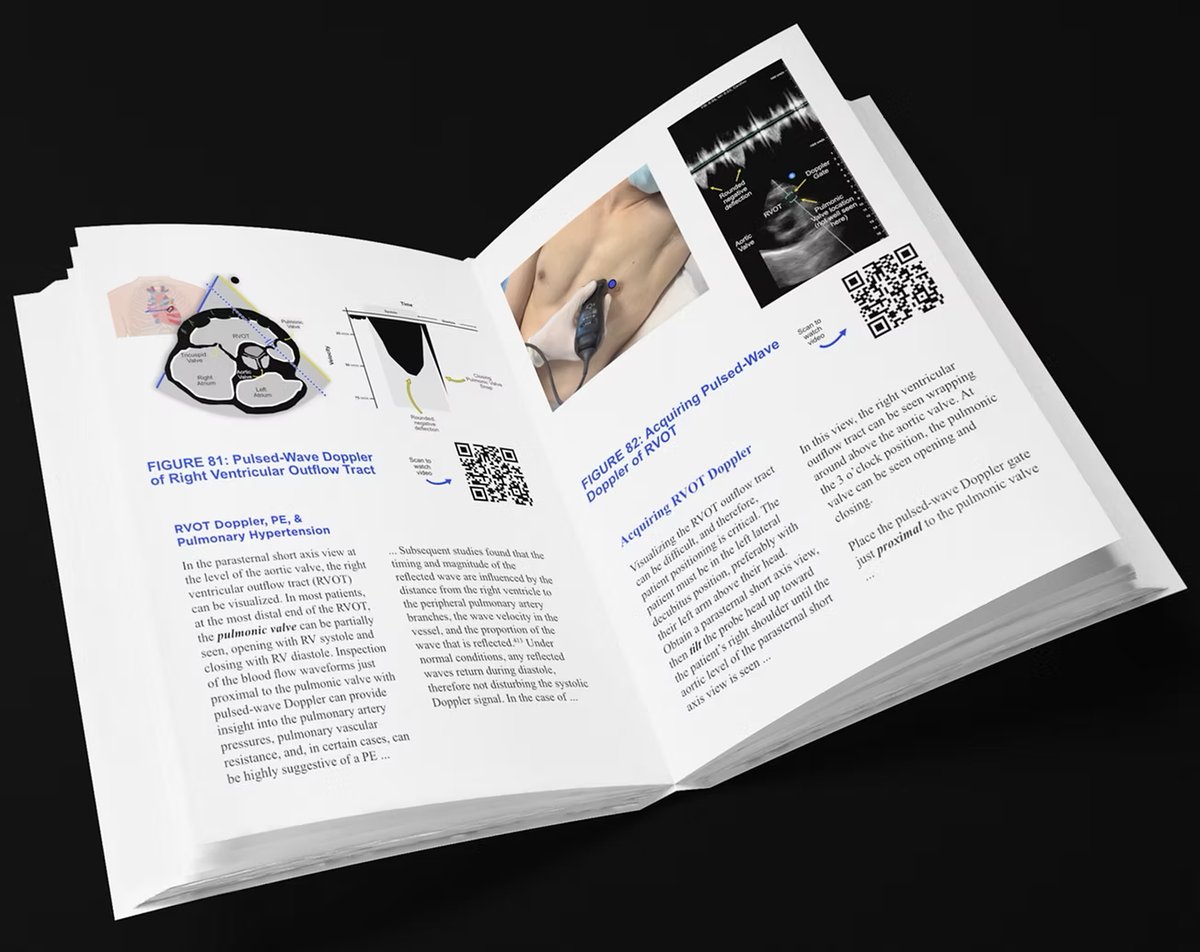
Another underutilized tool is using pulsed-wave Doppler of blood flow in the right ventricular outflow tract. This interrogates the blood exiting the RVOT and entering the pulmonary artery.
As pressures rise, the RVOT Doppler envelope assumes 4 distinct shapes that are highly correlated with pulmonary artery pressures.
1
1
170
Jun 8
To learn more about right ventricular assessment and pulmonary hypertension with POCUS, get a copy of The POCUS Textbook — a complete guide to point-of-care ultrasound of the blood vessels, heart, and lungs.
buff.ly/ihLPypC
1
144