
Neonatologist | Digital Health | MedEdTech
Joined May 2025
- Tweets 87
- Following 318
- Followers 31
- Likes 630
Photos and videos
Narasimha Rao retweeted

Jan 14
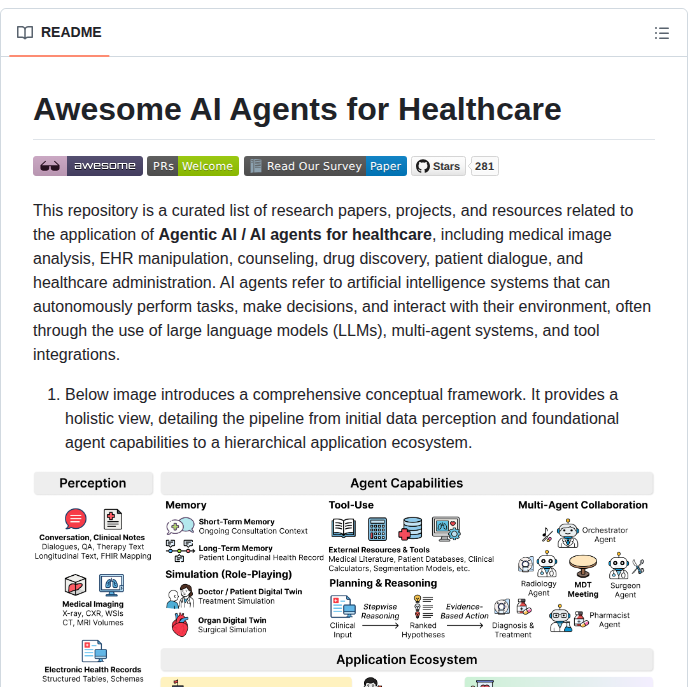
Curated list of research papers on agentic AI for healthcare
github.com/AgenticHealthAI/A…
26
177
1,191
72,475

Archimedes
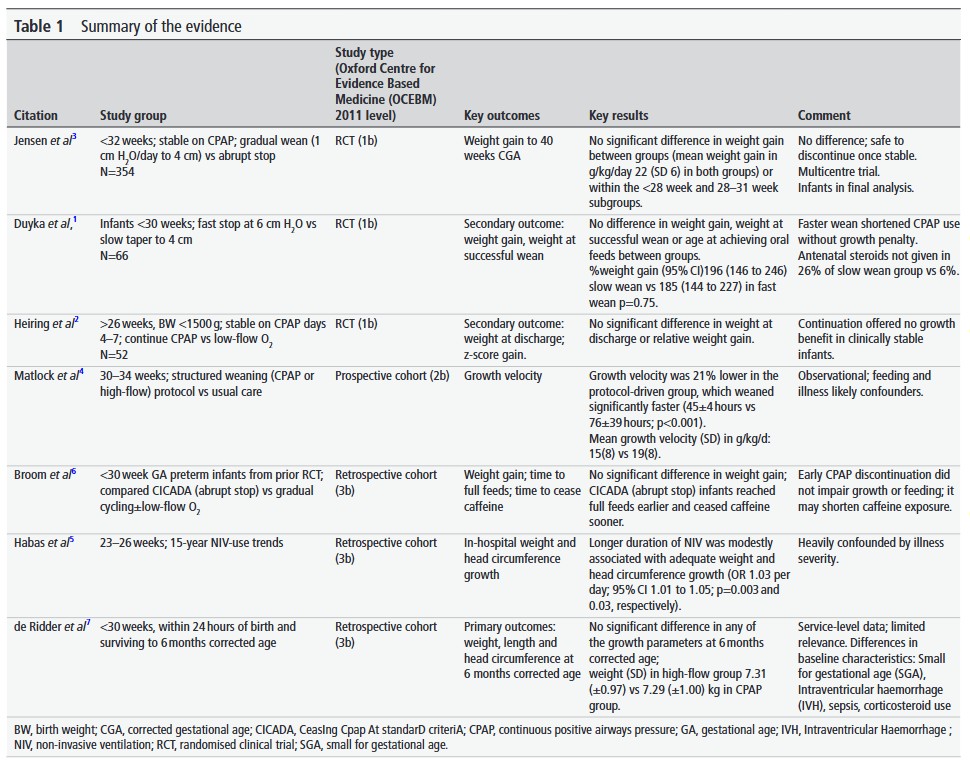
In preterm neonates, does extending non-invasive respiratory support beyond ventilatory needs improve growth?
Several papers out there to help: 4 RCT, 3 cohorts
adc.bmj.com/content/early/20…
4
6
635
Narasimha Rao retweeted

Jan 7
CRP -a story we all live daily (but rarely understand)
Today I asked my student:
“What is CRP? What is its normal function?”
He said confidently: “Sir, it’s an acute-phase reactant. It increases in infection.”
Then I asked:
“What do you mean by acute-phase reactant?”
He paused… thinking… stuck.
And honestly-most of us would also pause if we had to explain it properly.
Because we order CRP every day to “see inflammation”…
…but many of us don’t know CRP’s real identity.
So let’s see. 👇
First: why the name C-reactive?
Because CRP was discovered as a serum factor that reacted with the “C-polysaccharide” of pneumococcus during acute infection.
Second: what is CRP, conceptually?
CRP is a pattern recognition receptor (PRR)—but unlike TLR/CLR (membrane) or RLR (cytosolic)…
👉 CRP is a soluble, secreted PRR that patrols from the bloodstream.
What does this “soluble PRR” recognize?
Signals of danger: microbes damaged self.
CRP binds targets like phosphorylcholine on microbes and on apoptotic/necrotic membranes—basically, “this needs cleanup.”
Then CRP does the work:
🧹 Opsonization (tags for phagocytosis)
🧩 Classical complement activation (via C1q)
➡️ Better clearance of debris & immune complexes.
Now the clinical beauty: CRP kinetics.
CRP is made fast—rises by ~6 hours, peaks around ~48 hours after a stimulus.
The golden fact most people miss:
CRP has a constant half-life ~19 hours (in health and disease).
So the CRP value mainly reflects how much the liver is producing, i.e., inflammatory drive.
So when should you repeat CRP?
If you want the repeat to mean something, match biology:
✅ Repeat in 24–48 hours to judge trend/response (rise/peak/fall dynamics).
When is repeating too early?
<12 hours usually adds noise, not insight—CRP hasn’t had time to change meaningfully given its kinetics and half-life.
CRP isn’t just “an acute phase reactant.”
It’s a secreted PRR complement-linking opsonin a real-time reporter of inflammatory production.
We order it daily.
It’s worth knowing what it really does.
👉 #MedTwitter #RheumTwitter #Immunology #CRP #ClinicalPearls #MedEd @DrAkhilX @IhabFathiSulima @CelestinoGutirr @Urchilla01 @schowardjd
10
60
224
16,738
Narasimha Rao retweeted

31 Dec 2025
Delighted on publication in Archives of diseases of Childhood on review of evidence for ‘Use of NIV to support growth in preterm neonates’ on last day of 2025! @ADC_BMJ @EBNEO
Thanks to my co-authors Johanna Baker & @polythenia for collaboration.
doi.org/10.1136/archdischild…
1
2
14
594
Narasimha Rao retweeted

24 Dec 2025
Holy shit… University of Alberta just solved one of AI’s biggest healthcare problems 🤯
They built a framework called Reason2Decide that makes medical AI actually explain its decisions, not hallucinate rationales after the fact.
And It works with models 40x smaller than GPT-4.
Here’s why this matters for clinical AI 👇
Models are trained to explain “correct” answers.
But in real use, they must explain their OWN predictions, which can be wrong.
This mismatch is called exposure bias.
It’s why explanations often don’t match decisions.
Doctors notice. Trust breaks.
The solution is Reason2Decide.
A two-stage training framework:
Stage 1: Teach the model how to explain medical decisions.
Stage 2: Gradually shift from explaining gold-standard answers to explaining its own predictions.
The model learns to be honest, not just confident.
The clever mechanism is called Task-Level Scheduled Sampling.
During training:
• Start with 0% self-predictions
• Gradually ramp to 90%
• Never hit 100% to avoid error amplification
The model literally learns to explain itself.
he results on real clinical data are wild.
Clinical triage with 170k real nurse notes:
T5-Large Reason2Decide
• 60.58 F1
• Beat all fine-tuning baselines
• Beat Qwen-3-32B with a model 40× smaller
On PubMedQA:
• 60.28 F1
• 96% accuracy
Prediction alone isn’t enough.
The explanations must actually align.
Reason2Decide scored highest on:
• BERTScore (semantic similarity)
• BLEU (surface quality)
• LLM-as-Judge correctness
When the model said “Go to ED now,” the rationale actually justified it.
Here’s the surprising part.
Stage 1 used only LLM-generated rationales.
No human-written explanations.
Result?
It still outperformed models trained on human rationales.
Synthetic explanations can replace expensive human annotations in medical AI.
Why this matters for healthcare AI:
Trust: Doctors can verify the reasoning.
Safety: Misaligned explanations get caught.
Cost: 40x smaller models are deployable in hospitals.
Scale: Works with synthetic training data.
Explainable AI that actually explains.
The limitation they openly admit: “All predictions and rationales are decision-support tools and require human verification.”
This is the right mindset.
Augment clinicians.
Don’t replace them.
What Reason2Decide proves:
• Small models can beat foundation models
• Explanations can match predictions
• Synthetic rationales can work
• Real clinical deployment is possible
Paper: “Reason2Decide: Rationale-Driven Multi-Task Learning”
Hasan et al., University of Alberta

45
176
968
64,952
Narasimha Rao retweeted

21 Dec 2025
Everyone is missing what this study actually says to parents.
The graph shows two paths to the same destination. The yellow line (early specialization) gets there faster in the early years. The blue line (multi-disciplinary) gets there slower but breaks through to world-class.
The key insight: individuals who perform best at a young age are usually not the same people who later reach the world-class level.
This came from 34,839 top performers across four domains: Nobel laureates, Olympic medalists, elite chess players, and renowned classical composers.
The researchers found three consistent patterns.
First, the best kids and the best adults are mostly different people.
Second, future world-class performers showed gradual development and weren’t among the best in their age group.
Third, they didn’t specialize early but engaged in multiple disciplines.
The research team proposes three mechanisms that explain why breadth beats depth.
The search-and-match hypothesis suggests that exposure to multiple disciplines increases the likelihood of eventually finding the best personal fit.
The enhanced-learning-capital hypothesis proposes that learning in diverse areas strengthens overall learning capacity, making it easier to continue improving later at the highest level within a chosen field.
The limited-risks hypothesis argues that engaging in multiple disciplines reduces the chance of setbacks such as burnout, unhealthy work-rest imbalances, loss of motivation, or physical injury.
That third one matters enormously. Specialized athletes are 2.25 times more likely to get overuse injuries than multi-sport athletes. The American Academy of Pediatrics, AOSSM, and American Medical Society for Sports Medicine all recommend against early specialization before age 15 for most sports.
The lead researcher, Arne Güllich from RPTU University Kaiserslautern-Landau, puts it bluntly: “Don’t specialize in just one discipline too early. Encourage young people by providing opportunities to pursue different areas of interest, and support development in two or three disciplines.”
The two or three disciplines don’t need to be related. Language and mathematics. Philosophy and geography. The researchers cite Einstein pursuing physics and violin.
The connection between domains seems to build cognitive infrastructure that pure depth cannot replicate.
Here’s what makes this uncomfortable for parents. The early specialization path produces visible results faster. Your kid looks better at age 10. They make the travel team. They win the tournament. The graphs cross and diverge later, around peak performance age, when the multi-disciplinary kids start pulling ahead.
The entire youth talent ecosystem runs on selecting early performers and accelerating them. Travel leagues, elite academies, showcase tournaments. Every incentive pushes toward specialization.
But the research shows this system is optimizing for the wrong metric.
It produces great 14-year-olds, not great 24-year-olds.
The practical takeaway: let your kid play three sports until at least middle school.
Let them quit the piano and try drums. Let them be mediocre at several things instead of great at one thing. The data says this approach produces both more elite performers and fewer burnout casualties.
The hardest part is watching other kids pass yours on the yellow line while trusting the blue line catches up.
19 Dec 2025

A massive new study on peak performance included 34,000 international top performers: Nobel laureates, renowned classical music composers, Olympic champs, and the world’s best chess players. It shows early specialization is a trap, and the road to greatness is long and varied.

61
534
2,613
392,182
Narasimha Rao retweeted

7 Dec 2025
If you or someone you know is interested in joining a neonatology fellowship in a good US program, please DM me. Some programs are looking for candidates. Our program is fully filled with excellent candidates. I'm trying to help other programs recruit. #neotwitter
3
3
15
1,018
Narasimha Rao retweeted

3 Dec 2025
💬 Viewpoint: The Joint Commission and Coalition for Health AI have issued guidance on responsible #AI use in health care, but without a unified evaluation system, US hospitals face liability and efficiency challenges as AI adoption expands.
ja.ma/48ALE2t
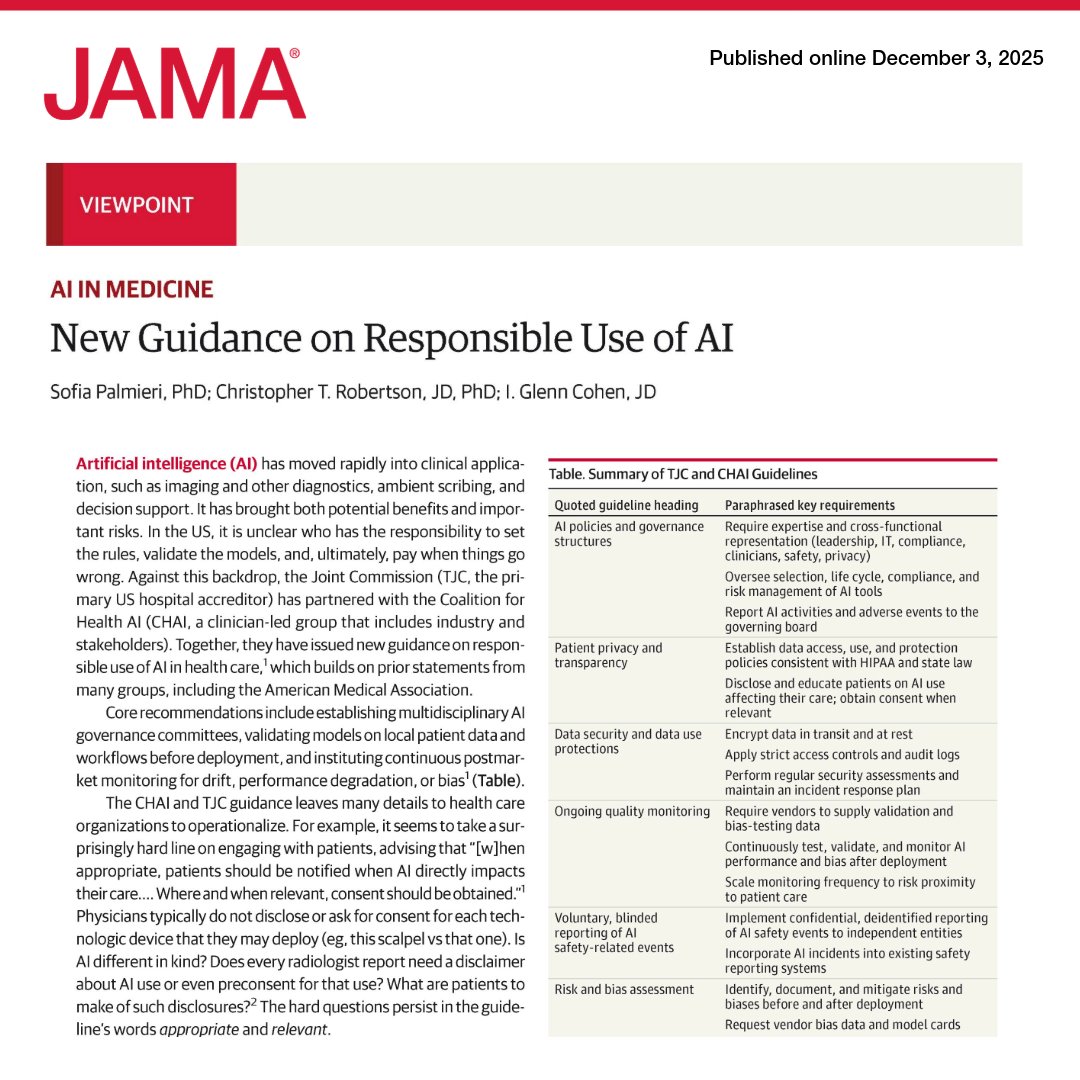
ALT JAMA viewpoint on "New Guidance on Responsible Use of AI" by Sofia Palmieri et al. Published December 3, 2025. Includes summary table of TJC/CHAI guidelines: AI policies, patient privacy, data security, quality monitoring, risk assessment.
6
94
297
29,272
Narasimha Rao retweeted

26 Nov 2025
Mark your calendar for this excellent session on the 5th of December by @Rupa_HariGopal talking about ductal dynamics in #CDH
Look forward to an amazing session!
@CardioNeo
@NeoHemodynamics
@CDHUK_CHARITY
Registration:
Link for registration
us06web.zoom.us/webinar/regi…
3
4
1,708
Narasimha Rao retweeted

20 Nov 2025
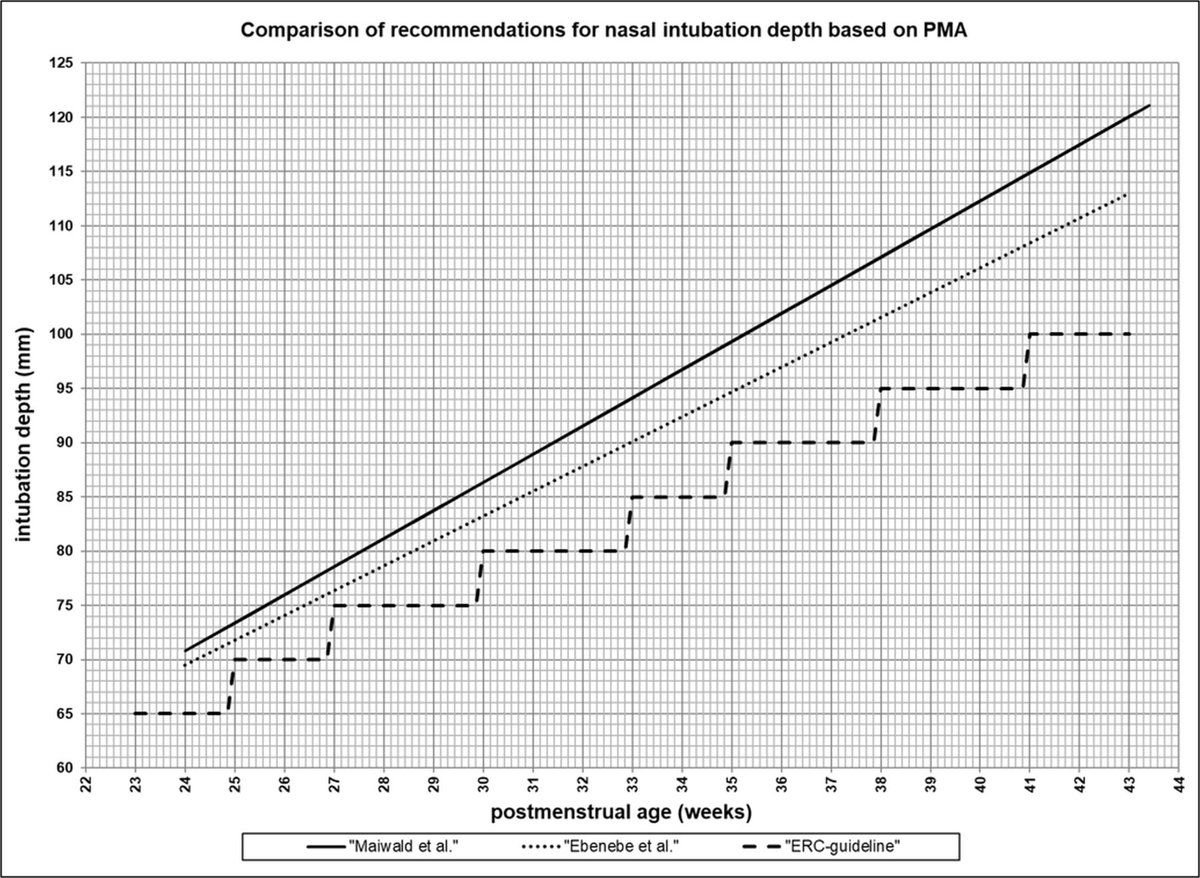
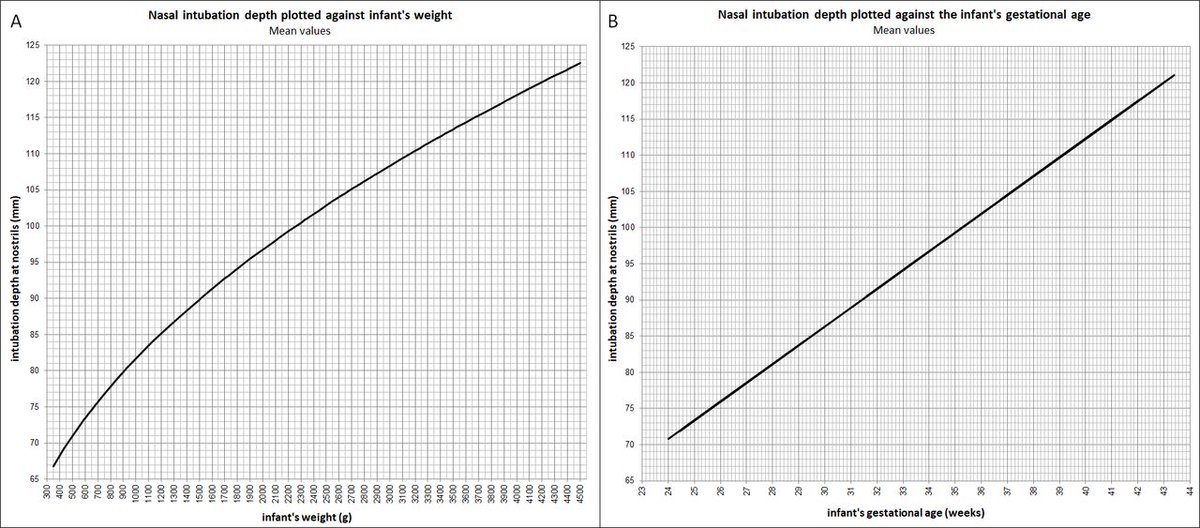
I don't do nasal intubations, but if I did, I would use work like this to guide my ETT depth. New paper prospectively evaluating the depths for accuracy. A 🧵keep looking ⬇️ @EBNEO @NICU_Musings @Research4Babies @neosatyan @NeoConsortium fn.bmj.com/content/early/202…
2
6
7
749
Narasimha Rao retweeted
20 Nov 2025
I don't do nasal intubations, but if I did, I would use work like this to guide my ETT depth. New paper prospectively evaluating the depths for accuracy. A 🧵 @EBNEO @NICU_Musings @Research4Babies @neosatyan @NeoConsortium fn.bmj.com/content/early/202…
3
4
240
Narasimha Rao retweeted

19 Nov 2025
BAPM has shared a notice from the HM Coroner regarding the findings of an index case.
You can read the notice here> bapm.org/articles/safety-ale…
6
4
856
Narasimha Rao retweeted
10 Nov 2025
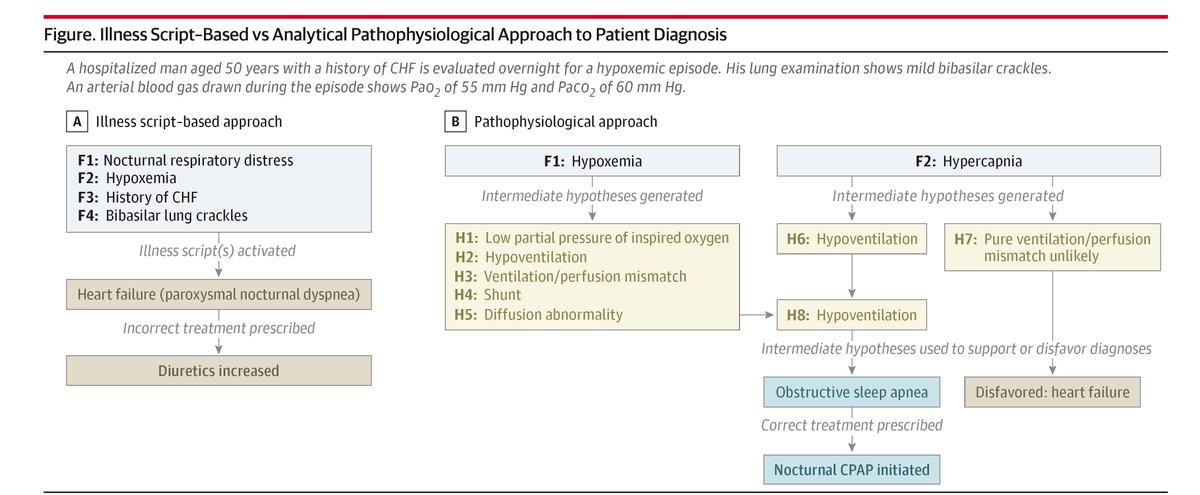
💬 Viewpoint: Medical education should shift from pattern recognition to critical thinking and pathophysiological reasoning to reduce diagnostic errors and adapt to #AI advancements. #MedEd
ja.ma/3Jp7yMH
13
164
492
91,344
PICC lines will move when a neonate's limb is moved
Median 13.5 mm when hip is flexed
Prospective POCUS observational study fn.bmj.com/content/early/202…

5
13
736
Narasimha Rao retweeted

6 Nov 2025
For infants undergoing therapeutic hypothermia, I obtain Echocardiography:
@EBNEO @nicupodcast @CardioNeo @NeoHemodynamics @Research4Babies @NeoHeartSociety
37%
Routinely on all
17%
Only if ⬇️ BP
40%
Only if ⬇️ BP and/or ⬆️O2
7%
Other (please comment)
30 votes • Final results
2
311
Narasimha Rao retweeted
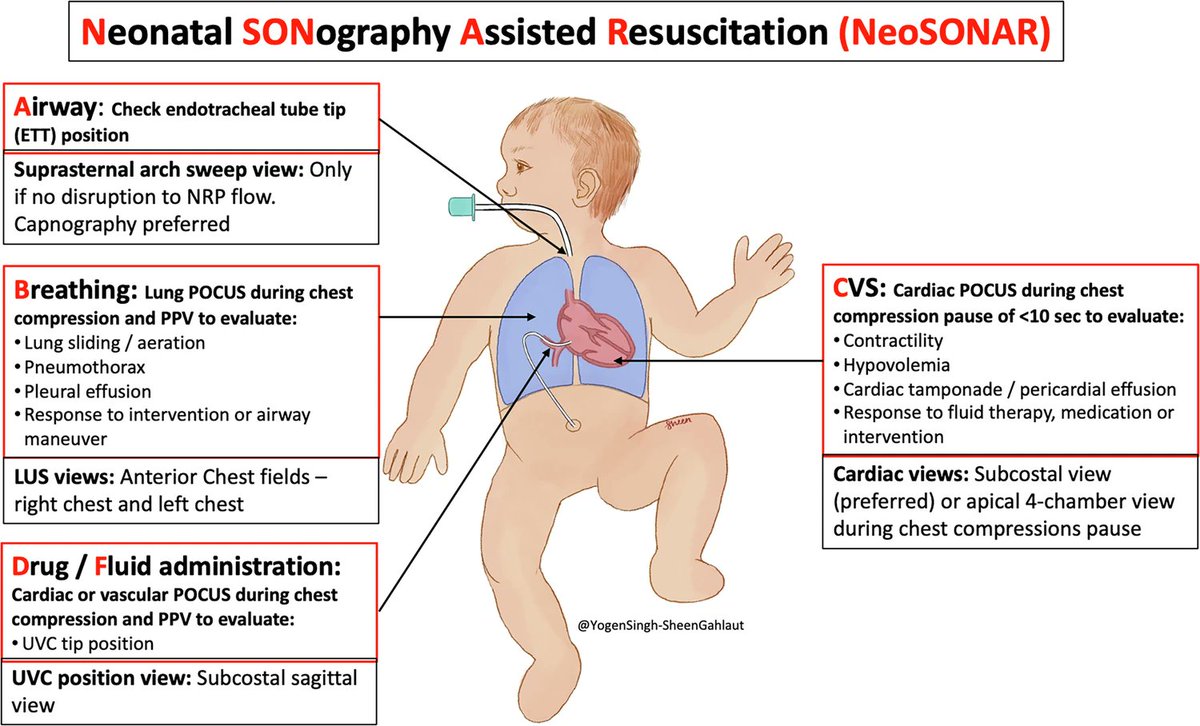
5 Nov 2025
NeoSONAR for Neonatal Resuscitation? A thought provoking article on uses for POCUS ultrasound in code situations for neonates. Maybe one day @dryogensingh @neosatyan. Not convinced more technology in the DR is what we need. Invest in training people.
nature.com/articles/s41372-0…
@EBNEO
1
9
32
1,780
Narasimha Rao retweeted

30 Oct 2025
Autism and vaccines? Should we worry? #vaccines #autism
youtu.be/mtsdJ5-yh3k
Would love your comments
1
1
128
Narasimha Rao retweeted
16 Oct 2025
All about neonatal ventilation-a compilation of my ventilation series lectures.
youtu.be/llIoyiwFTrQ
Registration link for Neovent courses med-train.com/course-details…
1
1
165
Narasimha Rao retweeted

14 Oct 2025
Protocol comparing active cooling methods in neonatal transport. Thanks @TheKids_AU @HopeforHIE @BetsyPilon and @PCHFWA for funding trial and equipment. Early care by transport teams matters #neonataltransport #foamneo #neoebm
trialsjournal.biomedcentral.…
4
11
821

14 Oct 2025
RT @NeoResearch_Net: #Neonatal #GI #Nutrition
High-quality AXR & photo need for eLearning
Non-profit, non-commerce
Bile #blood stool, vo…
4