
Joined November 2021
- Tweets 32
- Following 8
- Followers 8
- Likes 18
12 Photos and videos











21 Nov 2024
I'm Azalia. Big #weeb Began college at 14, grad at 20. Keto biochemistry and metabolism research. Also a pro Biochem Technical Writer, VA violin mandolin. Snake owner Guyanese-American who enjoys non-standard concepts. It gives me a chance to cogitate on IRL mythological lore!
1
2
138
21 Nov 2024
Attention Royal Court! My Discord is science.mage
Dues to your feudal lord?
linktr.ee/science.mage
77
21 Nov 2024
I'm Azalia. Big
#ENTP Began college at 14, grad at 20. Keto biochemistry and metabolism research. Also a pro Biochem Technical Writer, VA violin mandolin. Snake owner Guyanese-American who enjoys non-standard concepts. It gives me a chance to cogitate on IRL mythological lore!
1
108
science.mage retweeted

10 Sep 2023
━━━━━━━━━━━
劇場版
魔法少女まどか☆マギカ
〈ワルプルギスの廻天〉
2024年 冬 公開
━━━━━━━━━━━
youtu.be/AXpnlROHu78
#魔法少女まどかマギカ
1,161
140,800
236,103
30,242,764
science.mage retweeted

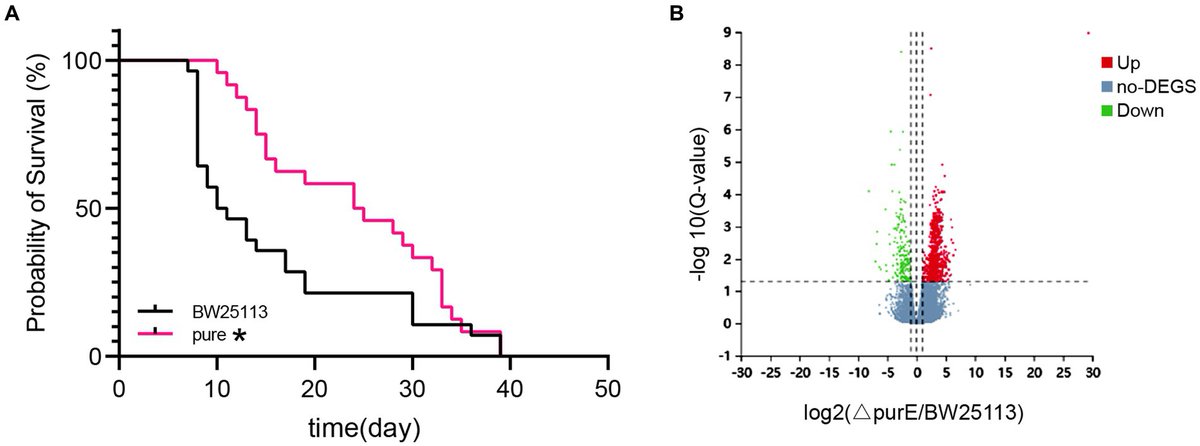
Insights into the genetic influences of the microbiota on the life span of a host
🔎Insight into “genetic influences of the microbiota on the life span of a host and a basis for developing anti-aging probiotics and drugs.”
frontiersin.org/articles/10.…
@FrontMicrobiol
5
13
1,725
science.mage retweeted
Cheers🍻to @aubreydegrey: From inception, RMR(2) proposed protocols had strong elements
1⃣Combinatorial design to explore potentially additive, even synergistic: combos (❌antagonistic ones)
2⃣Naturally aged🐁
3⃣HET3🐁
4⃣Suitable rapa dosing @ 42PPM👀👇
x.com/agingdoc1/status/16041…🧑⚕️

I like the combinatorial design. Even ITP is @ 2’s (eg rapa ACA) but exploring ⬆️ additive effects of knowns is a good start *&*🤞 the list of Tx will grow.
Rapa as baseline @ 42PPM was a good move. Much too easy to claim synergy with agents given @ sub-maximal (eg 14PPM) doses.
1
2
11
3,171
science.mage retweeted

16 Aug 2023
this is me btw. when you're being mean to me, this is who you're being mean to


111
5,988
57,498
2,189,658
science.mage retweeted
Do we need “longevity medicine.” Is it different than traditional medicine?
I unpack a bit (click “show more” to see the full post).
While medicine is medicine, perhaps explicitly introducing such concepts foster clarifying & focusing progress within health delivery models👨🏻⚕️👇
I think you're asking a very good question Brad, one I contemplate a lot as both a physician (not necessarily PCP) and someone interested in and active following aging biology research. These are my biases, and also my strengths as they both have some perspective to offer I think.
1⃣I believe that evidence-based primary care at its best (and integral to its mission) is indeed interested in "boosting longevity" and "extending healthspan.
2⃣Indeed, core to effective primary care services and objectives of the profession are (your words): "covering prevention, wellness, and treatment of common illnesses."
3⃣So far so good. Subsequent to that there's a lot to unpack precisely what it is we are discussing and targeting "Why rebrand it to longevity?" I'll do my best here, as a starting point what needs to clarified before we do your profound question the full justice that it deserves.
4⃣One element is that primary care attempts preventative medicine and lifespan/healthspan extension as best it can. Discussions of "longevity medicine" - when they are appropriately responsible - in my estimation must acknowledge this reality.
5⃣However following such acknowledgement, it is reasonable to observe much of (not all) primary care follows an acute care model whereby a patient presents with a medical problem, and a diagnoses are appraised, and therapy is initiated. Now it's that primary, secondary, and tertiary prevention are integrated into good medical systems. Thus we monitor for hypertension, hyperlipidemia, HgBA1c etc and a good PCP will even notice a rising trend even prior to hitting diabetes or prediabetes and may act sooner. Nevertheless the focus tends to be after crossing certain thresholds (eg near prediabetic or prehypertensive) as opposed to starting with what may be the optimal levels of these biomarkers and sustaining them.
6⃣ [Controversies: Earlier adoption of "optimal aging phenytypes" and Medicine 3.0 strategies]: One counterargument of intervening to sustain the optimal value rather than setting higher threshold is levels of evidence. The more subtle the aberration, the harder it is to establish reasonable evidence-based guidelines. I am sympathetic to this, and strong proponent of evidence-based medicine. The challenge remains in areas that matter "playing it safe" and being even more conservative has a low cost and risk. This is a medicine 3.0 framework as dubbed by Peter Attia and described in his book Outlive. Now I think this *should* be part of primary care visits and to an extent (since every PCP is different) its already out there. But verbiage such as "longevity medicine" has the potential for creating a common language around such a medical construct.
Surveillance screening not yet meeting evidence-based consensus is sometimes used in this setting as well (Do annual MRIs have favorable risk/benefit profiles? We do have some early evidence in this regard. Most of medicine looks for more clarity before widespread adoption... indeed there are reasonable arguments for either perspective IMHO)
So for these phenomenon: do we need a separate word for it? I think it helps to define what we mean- as long as we are clear with our definitions, I am happy.
7⃣Aging Biomarkers: Another branding emphasis of some circles who describe themselves as longevity medicine emphasizes instead the use of aging biology tracking biomarkers such as methylation clocks. These are not yet adequately validated for solitary use in trials IMHO, but progress is being made. I would like to see a panel of measures (including functional markers which have face validity and are mechanistically transparent) evolve and get better validated. At this time we are in early days, and most clinicians are waiting for better validation (or else not even aware of them). I believe provided overpromises are avoided (we cannot say whether in a particular individual that a slower biological aging pace for example means they are doing something right), it is reasonable for some providers/patients to use as one "possible" datapoint gently steering soft endpoints. They need to be taken with a grain of salt as we do other better validated clinical markers with their own ROC sensitivity/specificity/PPV/NPV characteristics. In essence the point here is not whether or not I agree on their use in practice, but rather acknowledging early adaptors may reasonably (with proper counseling and context) use preliminary data responsibly.
8⃣ "Geroprotectors": Another perspective is the use of "off-label" therapies that may or may not translate to healthspan/longevity extension in humans. These tend not to be part of primary care medicine. But they can be. Branding and verbiage are once again subjective, it is clarity that matters. New words that capture specific *elements* of existing paradigms can have utility in some settings. Not simply marketing (unfortunately I observe it plays a role in various settings), but intelligent discussions too.
9⃣ What are we targeting? Animal models suggest that most interventions in medicine that target specific disease pathologies, even when they extend average lifespan do so only by preventing *premature* mortality. Here the mean lifespan rises but not the maximum. This is the case, at least in rodents, for my favorite "longevity medicine" - exercise. It's possible that's the best we can do without new tools. This contrasts with rapamycin which extends median and maximum survival, many argue via plausability intervening in aging biology itself rather that one of many downstream sequela/silos of that process.
This is theoretical only. Rapamycin may have far less impact than exercise. It's possible it does not work at all in humans are that risks outweightbenefits (I personally am more optimistic that at least a subpopulation and perhaps many are more likely to benefit WRT healthspan /- max LS). Nevertheless as a matter of paradigm what's key to this point is what's being targeted. Longevity medicine may focus on bridging the gap to the clinic (such as your rapa trial) in efforts to clinically validate putative geroprotectors from animal models to translation in humans. Hopefull that will work.
Ultimately I'm a verbiage agnostic but would like us to utilize responsibility the little data we do have, transparently without overpromising, and support the important research needed bridging true longevity medicine progress.... in your primary care docs office and throughout!
-@agingdoc1 🧑⚕️
2
4
1,465
20 Jul 2023
1 May 2023

1
1
83
20 Jul 2023
No makeup needed when you're on a sphere orbiting a gaseous mass and your favorite snack is raw lemons from age 3
#nomakeup #distichiasis #blackwomen #twostrandtwists #gnight #thanks #blerd #blerdette #yum #twitter #good #mutant #sometimes #wow #uwu
1
143

science.mage retweeted
Ketosis, Salt, and Water: Novel Mechanistic Insights into Diet and Mineralocorticoid Metabolism
academic.oup.com/jcem/articl…
2
6
1,069
science.mage retweeted
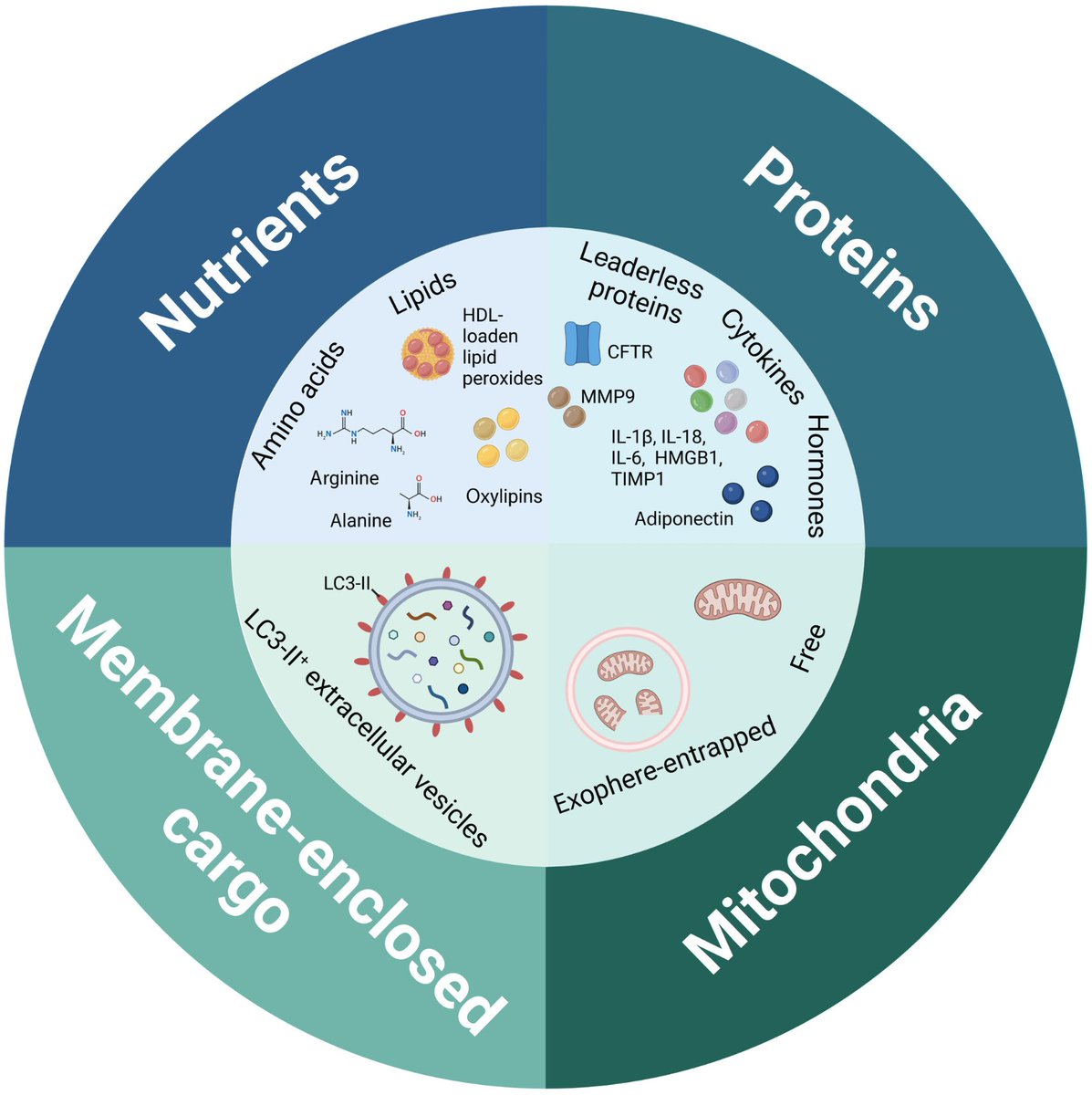
Autophagy orchestrates the crosstalk between cells and organs
@pileticklara @AlsalehAgingLab @aksimonlab
embopress.org/doi/full/10.15… @emboreports
7
17
2,061
20 Jul 2023
Look at our boy OR ELSE #kyle #snek #snekkiestsnek #reptile #reptiletwitter #cutesnakes #pets #pettwiter #uwu #uwuest
110
20 Jul 2023
Clean your mirror-no jutsu
#mirror #shipuuden #fun #coslay #cosplay #not #hobbies #blerd #blerdettes #blerdgirls #please #stop #me #naruto #cloudvillage #hidden #missingnin #akatsuki #usa #BlackGirlMagic
1
69
20 Jul 2023
Cloud missing-nin at a "Wear something you never get to wear" party #missingnin #akatsuki #naruto #coslay #cosplay #animu #blerd #blerdette
55
1 May 2023
1
1
353