
Radiation oncologist , NCIS
Joined June 2009
- Tweets 145
- Following 339
- Followers 117
- Likes 842
13 Photos and videos











Bala Vellay retweeted

Jun 4
It’s lovely to catch up with friends and collaborators from across the globe and specialties @ISRSy 2026!



1
1
20
690
Bala Vellay retweeted

Feb 19
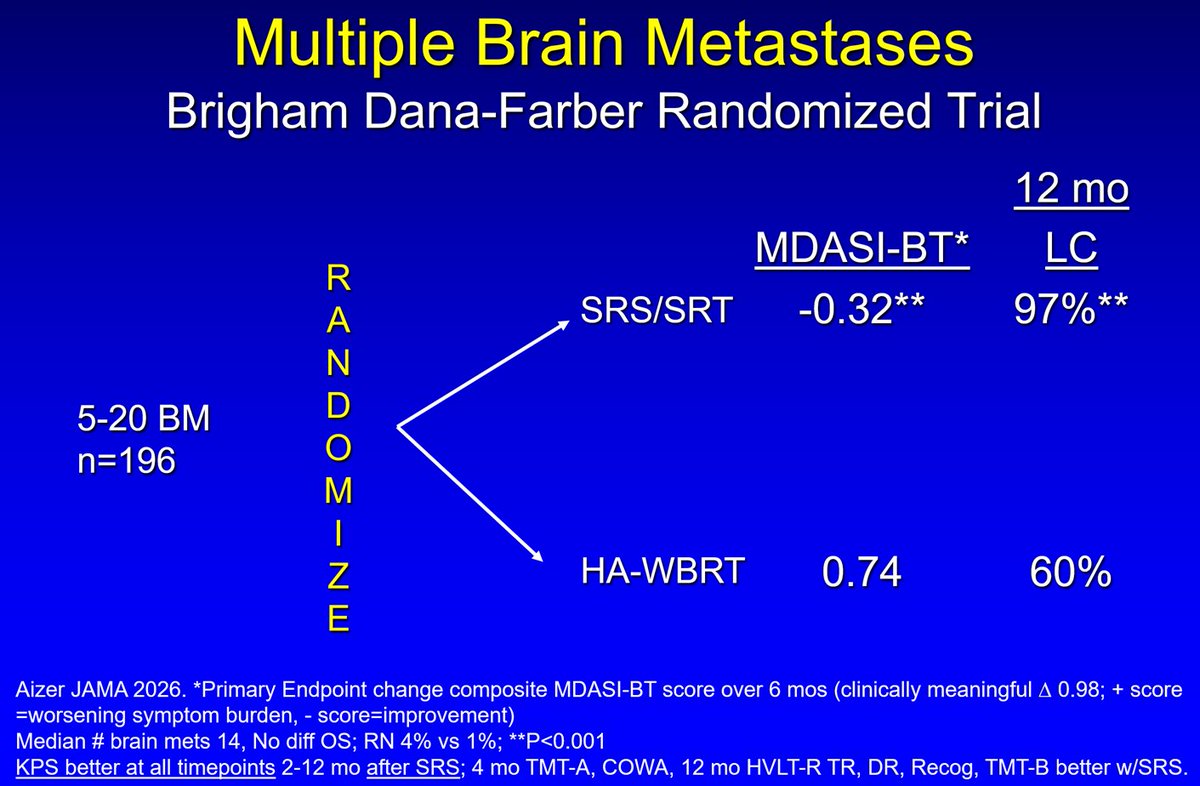
🚨🚨Multiple Brain Mets Randomized Trial🚨
· Significantly less symptom burden with SRS compared to HA-WBRT
· Better ADL, cognition & KPS after SRS
· SRS Standard of Care 5-20 brain mets
jamanetwork.com/journals/jam…
7
55
120
18,596
Bala Vellay retweeted
Feb 17
SRS for Cystic brain mets
1 Yr LC 71% (weighted ave volume ~6cc)
Cyst aspiration ↓↓ volume ~65%
tro.amegroups.org/article/vi…
1
3
7
542
Bala Vellay retweeted

30 Dec 2025
Academia isn't a calling—it's a job. Stop glorifying burnout. Clock in, do great work, clock out. Your worth isn't measured in unpaid overtime



78
520
2,182
736,421
Bala Vellay retweeted
31 Dec 2025
GTV=tumor bed residual
CTV=GTV 5mm
DMax Center/Edge Cord/Brainstem 55Gy/67Gy
DMax Optics 62Gy
1
4
348
Bala Vellay retweeted
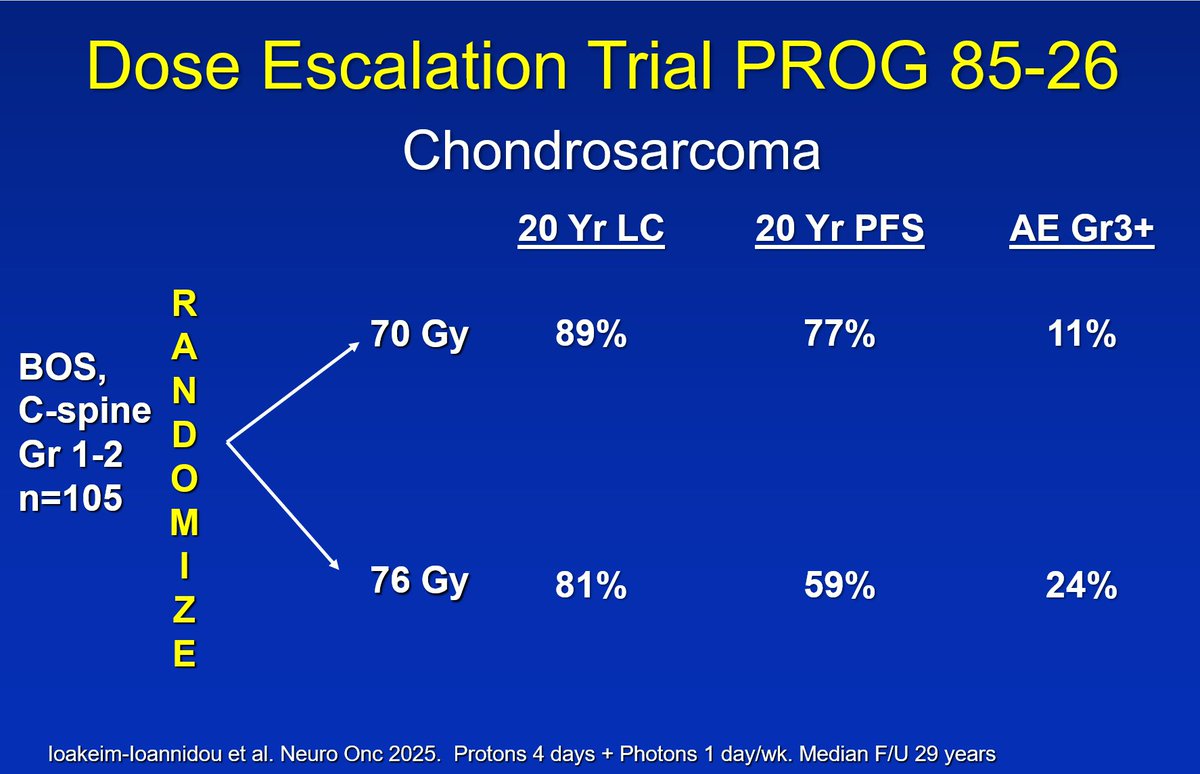
31 Dec 2025
Any benefit dose escalation for chondrosarcoma?
NO according to this randomized trial
academic.oup.com/neuro-oncol…
3
8
22
2,819
Bala Vellay retweeted

31 Dec 2025
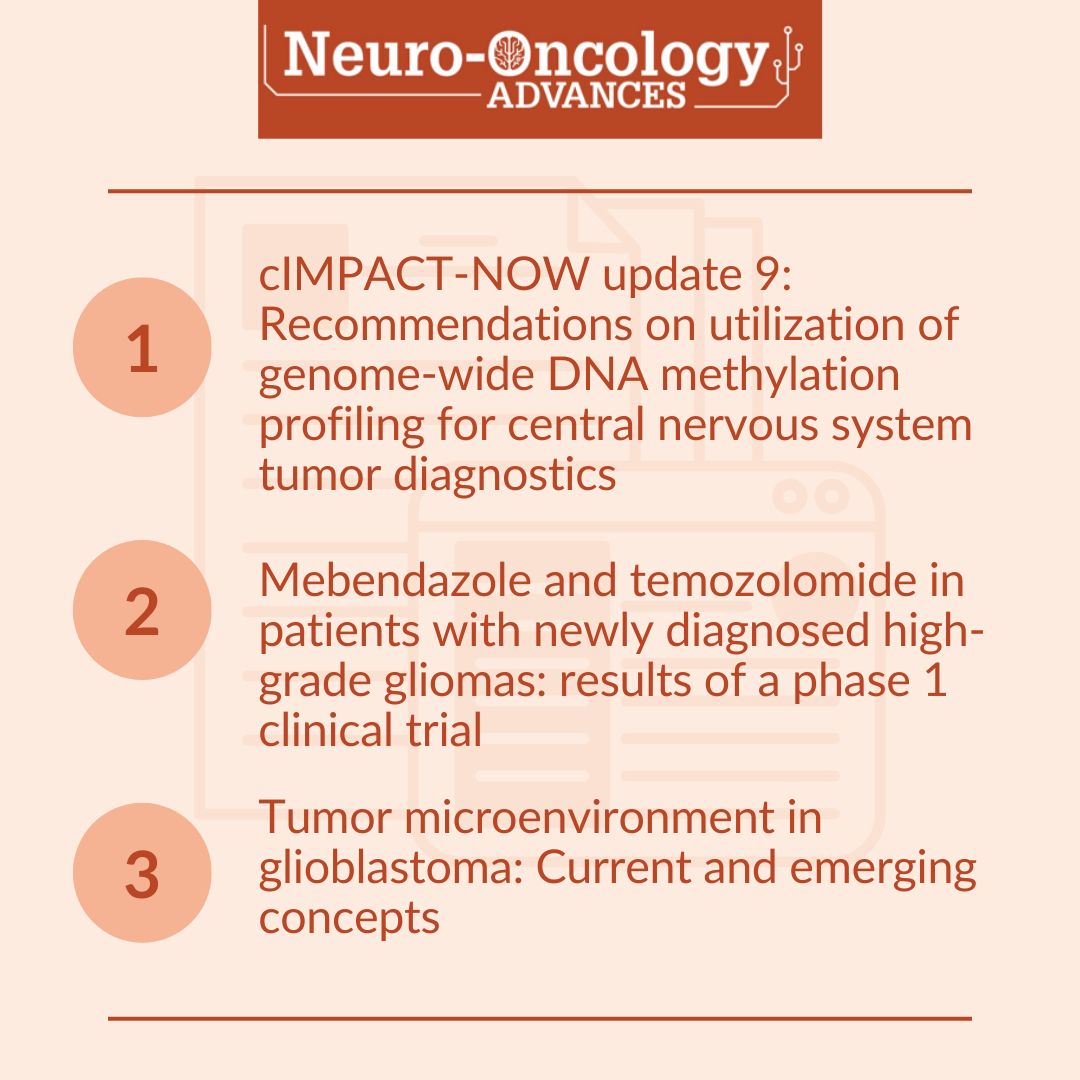
What are people reading? Here are three of our most visited articles over the past few months! 
Read them now here: bit.ly/3un7GEJ
4
5
1,472
Bala Vellay retweeted

31 Dec 2025
As we close 2025, the Neuro-Oncology field saw a plethora of scientific advances. I have tried to summarize the top 4 in my opinion in this thread. Which do you think was the most impactful? Let me know what I missed! X only allows 4 options :)
41%
FUS BBB disruption GBM
18%
Serial GBM biopsies
29%
RANO RESECT IDHm Gr2
12%
EGFR IL13R2 CART GBM
17 votes • Final results
2
2
11
860
Bala Vellay retweeted

29 Sep 2025
Register now for the next FREE #RSSwebinar on "The Role of Metastasis-Directed Therapy for Oligometastases and Oligoprogression in Breast Cancer" on 10/9 at noon ET featuring @drspdavid, @r_glicksman and @WinstonVuong; moderated by @radicalonc. therss.org/education/webinar…

8
10
2,122
Bala Vellay retweeted

7 Sep 2025
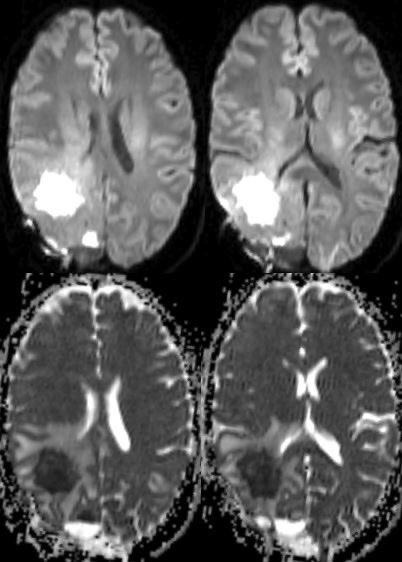
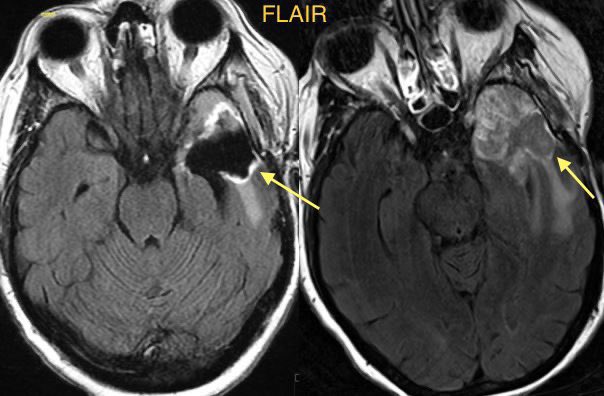
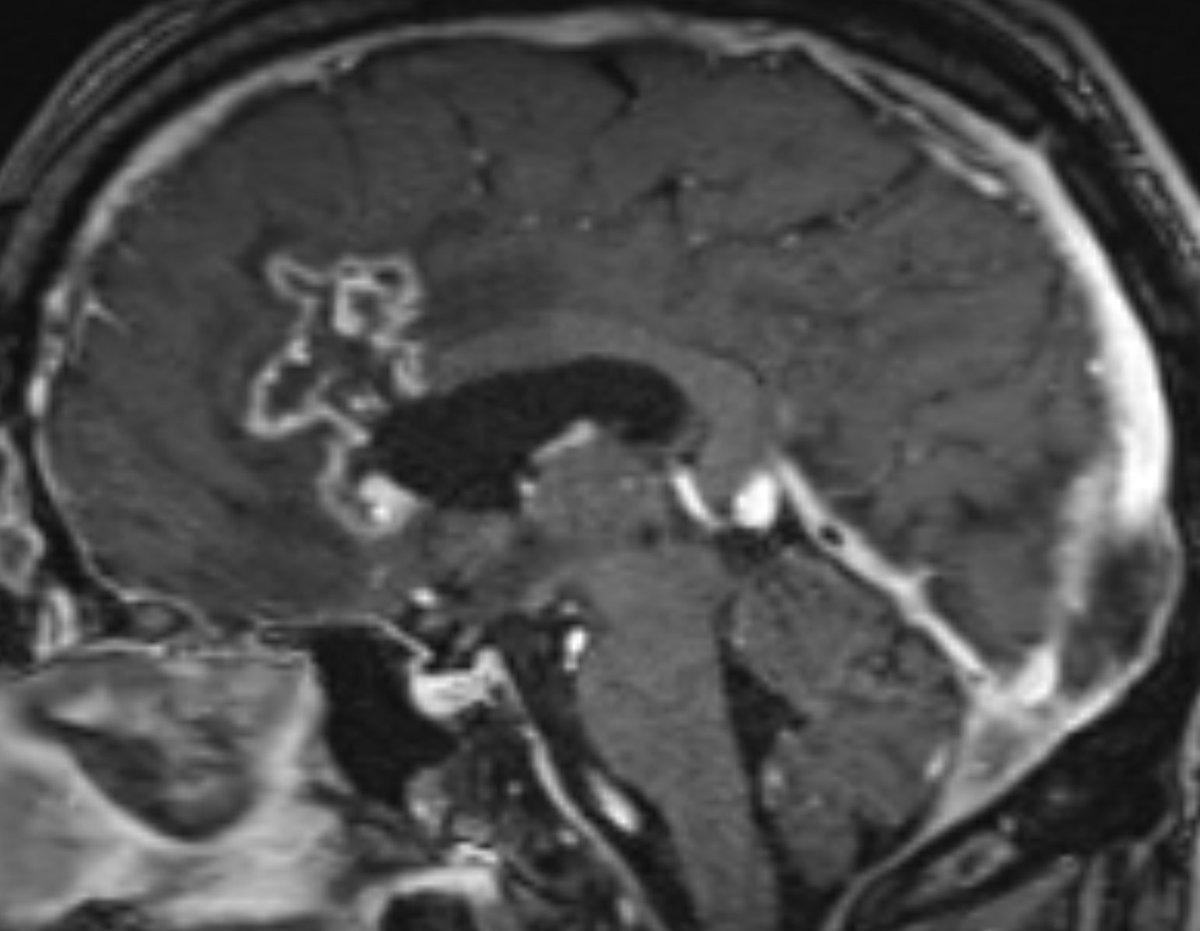
⭐️ Tips for distinguishing treatment change from tumor progression from my own experience and the literature ☢️
**Sorry for the long and very complicated post!**
#Neurosurgery #Neurology #radres #futureradres @TheASNR @UMiamiHealth #MRI @Radiopaedia #ENT #Medicine @PennRadiology

17
44
213
21,800
Bala Vellay retweeted
18 Aug 2025
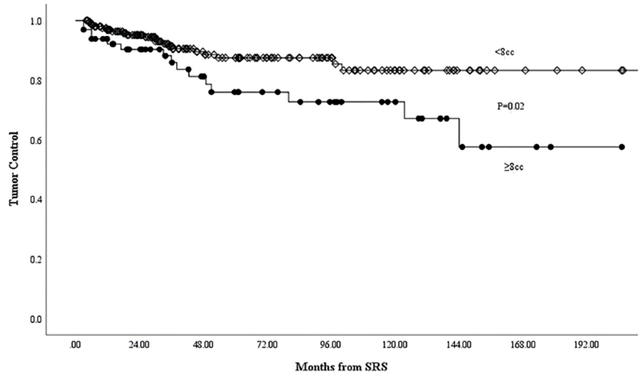
SRS for Trigeminal Schwannoma
· Median 13 Gy
· Median vol 4 cc
· LC 95%
· Symptom Improve 45%
· 9% ARE
journals.lww.com/neurosurger…
1
6
25
1,697
Bala Vellay retweeted

19 Aug 2025
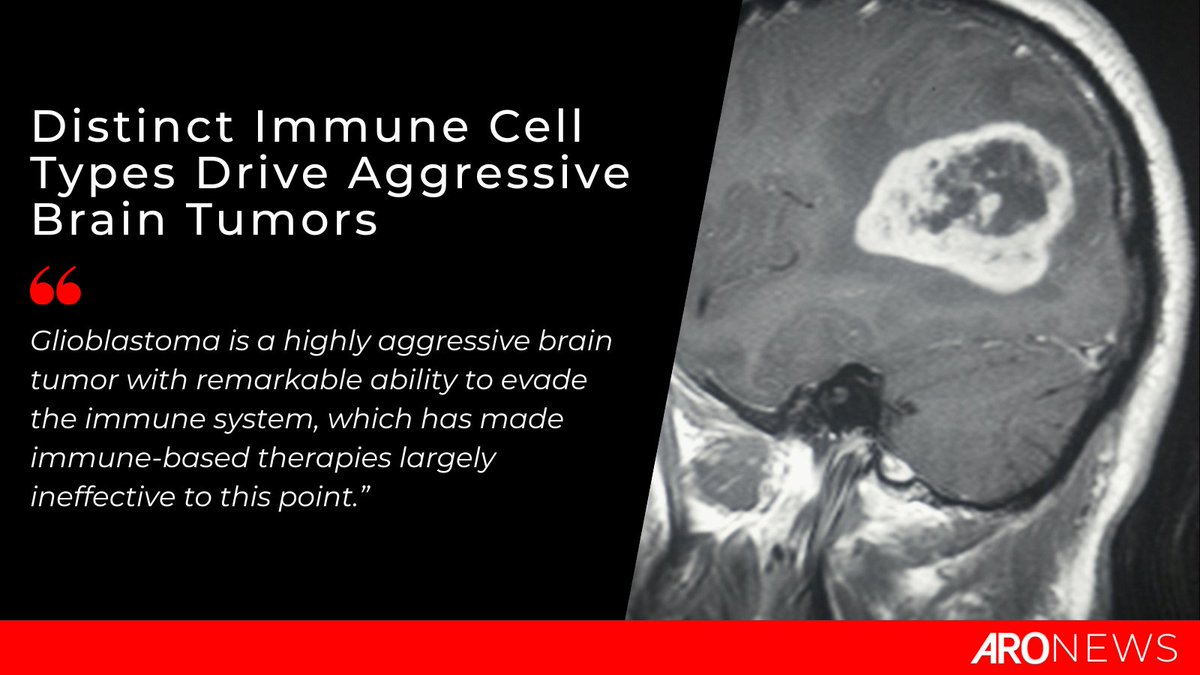
Check out the rest of this article ➡️ bit.ly/4oJxnGW
#RadOnc #RadOncNews #BrainTumors
@hopkinskimmel @HopkinsMedicine
4
6
541
Bala Vellay retweeted
13 Jul 2025
It’s wonderful catching up with medical school buddy/ roommate/ co-intern, mentee and friends @NUSMedicine in a social visit! The hospital food is amazing there. @radicalonc

1
13
504

19 Oct 2024
Enjoying my first #EANO2024. Thrilled to share the stage with heavy hitters Prof Helen Shih and Prof Marion Smits in the Radiation Necrosis session. Thank you @gminniti2012 for the invitation!



9
982
Bala Vellay retweeted
9 Oct 2024
Feel honored to have worked with @JYangMDPhD and to be working with @VenurVyshak @fredhutch ! You guys are like CNS brothers!
9 Oct 2024

Star-studded panel talking about LMD! @JYangMDPhD @Perlmutter_CC @VenurVyshak @fredhutch @UWMedicine Alvord Brain Tumor Center

2
1
13
1,196
Bala Vellay retweeted

28 Aug 2024
We have engaged radiation oncologists, medical physicists, and implementation scientists to explore the potential of real-time RT dose modulation.
I would like to thank the corresponding authors @thedeanh, @radicalonc, and @AgataBlasiak for their guidance on this work.
28 Aug 2024

Check out this seminar taking us through a perspective article 'Radiation therapy with phenotypic medicine: towards N-of-1 personalization': cassyni.com/events/SXa4uR2nF… #radiotherapy #RadiationOncology
1
4
169

Bala Vellay retweeted
23 May 2024
External Beam Radiation Therapy for Palliation of Symptomatic Bone Metastases: An ASTRO Clinical Practice Guideline - Practical Radiation Oncology @ASTRO_org @FacRadOncology @RCRadiologists @ESTRO_RT @caro_acro_ca practicalradonc.org/article/…
19
35
2,324
Bala Vellay retweeted

2 May 2024
Max Heart Rate Testing & The 220-AGE Formula
By @JohnHellemans
David is an experienced 68-year-old runner. On the advice of his running buddies, he finally capitulated and invested in a heart rate monitor. A week later, he came to see me in a panic, announcing that there was something wrong with his heart. His daughter, a fitness instructor, calculated his maximum heart rate with the still widely used ‘MHR=220-age’ formula. At 68 years of age, that made his MHR 152.
Based on that information, she told him to keep his heart rate around 115 for steady runs and his harder runs under 145. However, Dave had difficulty keeping his heart rate in the recommended zones. While it felt ‘steady’, his heart rate was 140, and when he encountered a hill, it shot up to 160 without trying too hard.
I asked him how he felt during the run. He answered, ‘I felt fine, but now I am not so sure about that anymore, and I am reluctant to resume training.’
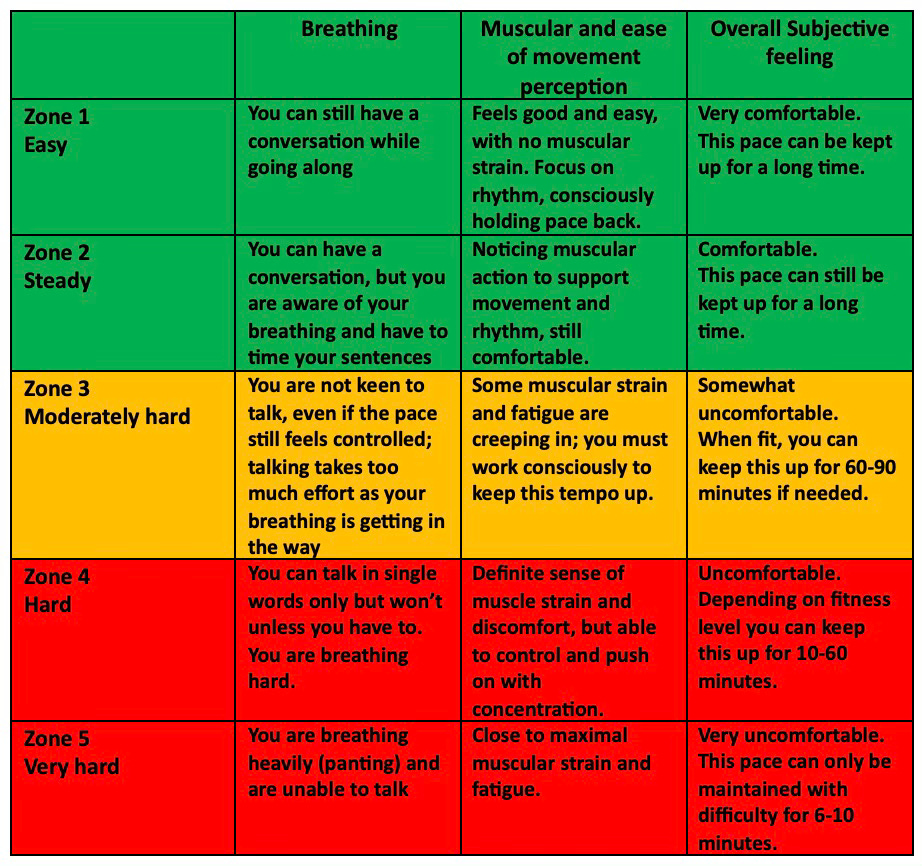
I listened to his heart, which sounded regular, with a resting rate of 64. His blood pressure was normal. He appeared in good health and was on no medication. I put him on a treadmill and gradually ramped up his speed every three minutes, asking him repeatedly to score his perceived effort on a score of 1-5 (1=easy, 2=steady, 3=mod hard, 4=hard and 5=very hard) while monitoring his heart rate.
▪️His heart rate quickly increased and was 140 in what he perceived as his steady zone (Zone 2). He looked comfortable.
▪️When I ramped up the speed to his calculated MHR of 152, he scored 2.5-3. He still looked comfortable.
▪️I increased the treadmill's speed a bit more, and his heart rate shot up to 170, while he scored 3.5-4, which is moderately hard to hard.
▪️I let him sit there for a bit, and his heart rate drifted up to 176 after a couple of minutes. He nodded when I asked if he could go a bit faster.
▪️I wound the treadmill up another notch and told him he could stop when he felt close to maximum effort. His heart rate increased to 182 before he pushed the treadmill's red ‘stop’ button.
After this workout, his heart rate returned to below 120 within one minute, suggesting excellent aerobic fitness. His heart rate had been regular all the way through the test. I reassured him and sent him home with his new heart rate zones based on the combination of his subjective score and his heart rate response during the test, as well as the following explanation:
The ‘MHR=220-age’ formula was introduced by Dr William Haskell and Dr Samuel Fox in 1970 when heart rate monitoring was gaining traction. This formula was not developed from original research but resulted from observation based on data from approximately 11 references of published or unpublished scientific compilations. It pointed merely to the average decline in heart rate for a large study population.However, the formula soon found traction in the fitness industry because of its simplicity (who can’t subtract their age from 220….). Even reputable organisations like the American College of Sports Medicine (ACSM) and the American Heart Association have promoted its use for many years. Polar Electro, the first company to popularise heart rate monitors, popularised the formula worldwide by including it in their guidelines.
Dr Haskell, one of the formula's creators, has since remarked about its widespread use, stating it was never intended to be a rigid training rule for individual patients and athletes. He confirmed that the formula applies to the average maximum heart rate of a large group of people and does not apply to the individual as there is significant variety in individual MHR. Dave is a good example, with a calculated MHR of 152 but a true MHR of 182 .
We know that our MHR reduces with ageing due to a combination of weakening of the heart muscle, an increase in resistance of the peripheral blood vessels and a reduced ability to respond to signals from the nervous system. While the exact rate of decline can vary among individuals, a commonly cited estimate is that our maximum heart rate decreases by approximately one beat per minute per year from age 30. This means that a person's maximum heart rate at 40 might be about ten beats per minute lower than it was at 30, and so on. However, this decline in MHR can be influenced by factors such as fitness level, genetics, and overall health. Regular exercise, especially aerobic exercise, can play a significant role in maintaining cardiovascular health and potentially slowing the decrease in maximum heart rate associated with ageing.
To get an accurate reading of your maximum heart rate, run or bike up a hill for 4-6 minutes in zones 4-5, and when you feel you can’t go on much longer, put in an extra effort (sprint). Look at your heart rate monitor before you keel over; that is your maximum heart rate.
The 6-minute test, as described in previous articles in Endurance Essentials, is also a good measure of getting close to your MHR.
To do a proper maximum heart rate test, you must be healthy and have some basic fitness. If you are over the age of 35 and new to exercise, we recommend that you get a doctor's clearance first. The alternative is to have a submaximal test with a fitness professional, as they can extrapolate an estimation of your MHR from the feedback they get from the test.
The original of this article can be found on Endurance Essentials. Use the links in my profile to subscribe to all of our content.
17
14
120
20,838
6 Apr 2024
Singapore Radiological Society AGM and social night, at alumni association.
Photo with the 2023 EXCO
1
1
173