
156 Photos and videos








ROECSG (Rad Onc Education Collab Study Group) retweeted

May 28
It’s #radonc away rotation season! For #medstudents and junior #residents, here are my go-to resources in radiation oncology (1/2).


4
31
98
6,575
ROECSG (Rad Onc Education Collab Study Group) retweeted

Another ERAS season is upon us - now for the #Match2027
#medstudents tons of #Radonc ☢️ residency apps & interview programming advice in the coming months by the amazing groups ⬇️
@ACROresident @ARRO_org @ASTRO_org @RadoncROVER @ArsRocket @S_W_R_O @roecsg

The 2027 ERAS season has begun. Check out the 2027 ERAS residency timeline to stay on track this application season: students-residents.aamc.org/…
4
8
1,225

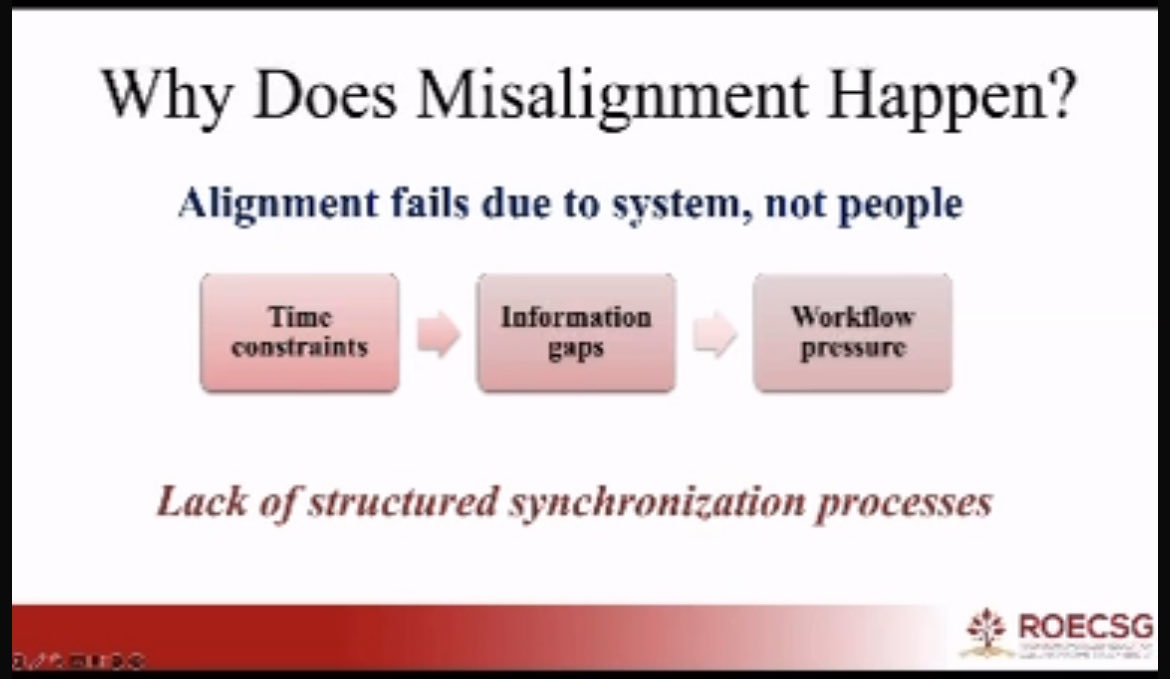
Minds must move as one before the beam does. 💡
Cognitive synchronization allows RT teams to think as one and is the formula for safer treatments.
A massive thank you to Reem Alahmadi for this initiative and presenting @roecsg by sharing the first phase of this project. 👏🏼
2
1
233

Thank you 🙏 to the amazing leadership team that made our 9️⃣th Annual ROECSG Spring Symposium a great success 👏
Symposium 🪑 @allisongardaMD
🥾 on the ground leaders & organizers including @d_golden @KimCorbinMD
Abstract 🪑 @JeremyPriceMD1 @LisaNiMD
1
5
437
Sneak Peek🫣 for Next Year's ROECSG Spring Symposium, which will be our 🔟th Annual Meeting
See you all in Indianapolis, IN 🏎️🏁
114
Thank you @ColinWestMDPhD the @MayoClinic Medical Director of Employee #wellbeing for the being the keynote speaker 🔑 of #ROECSG2026 with the talk on "From Burnout to Thriving in Medical Education and
Practice”. Excellent discussion on #burnout & #wellbeing
2
209
#ROECSG2026 highlighting our international presenters: Ireland 🇮🇪, Canada 🇨🇦,Qatar 🇶🇦, Germany 🇩🇪


159
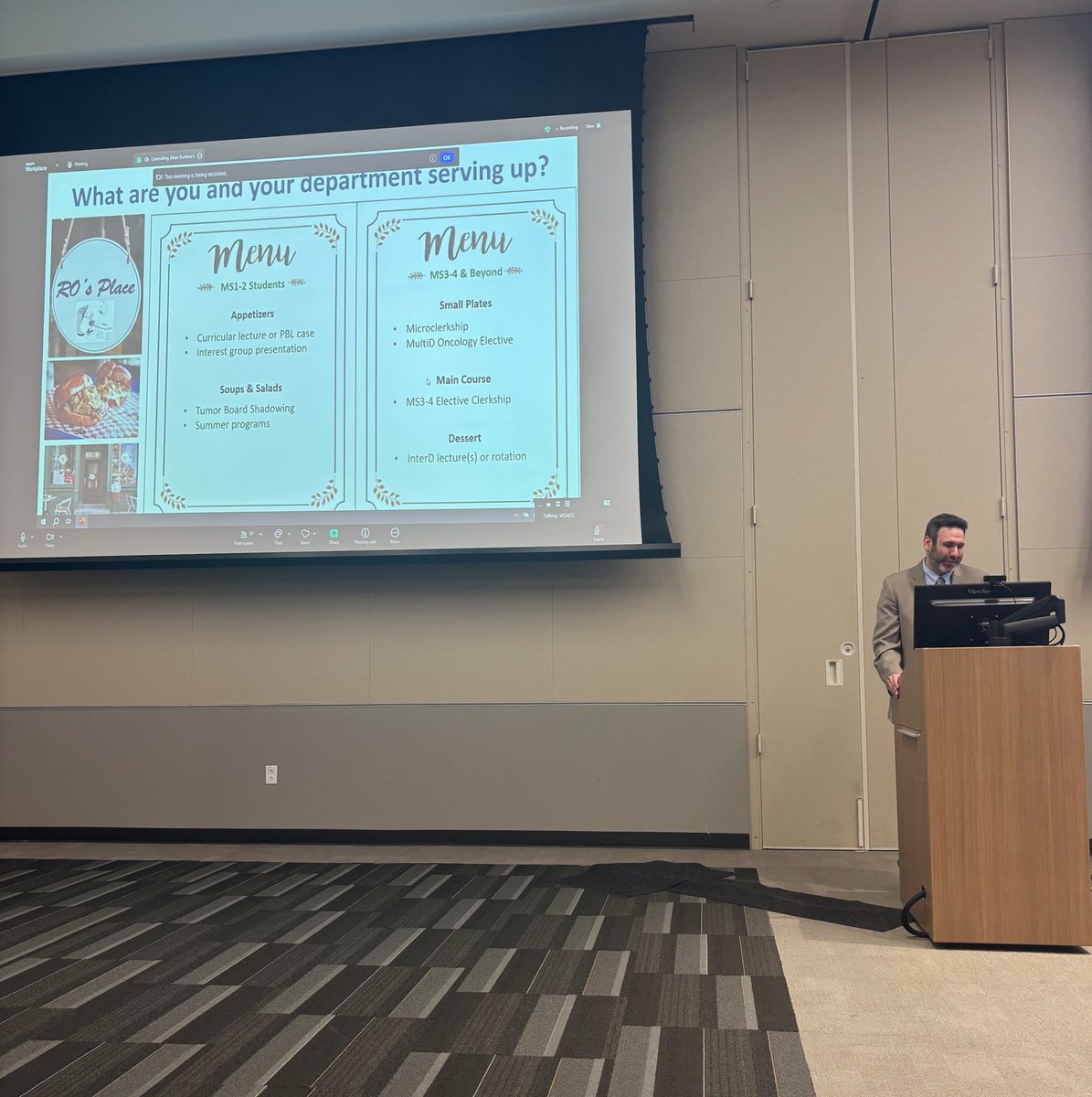
Updates from our 4 working groups 📑#roecsg2026
UGME @JillGunther @StevenGrunstein
GME with Dr. Jordan Holmes
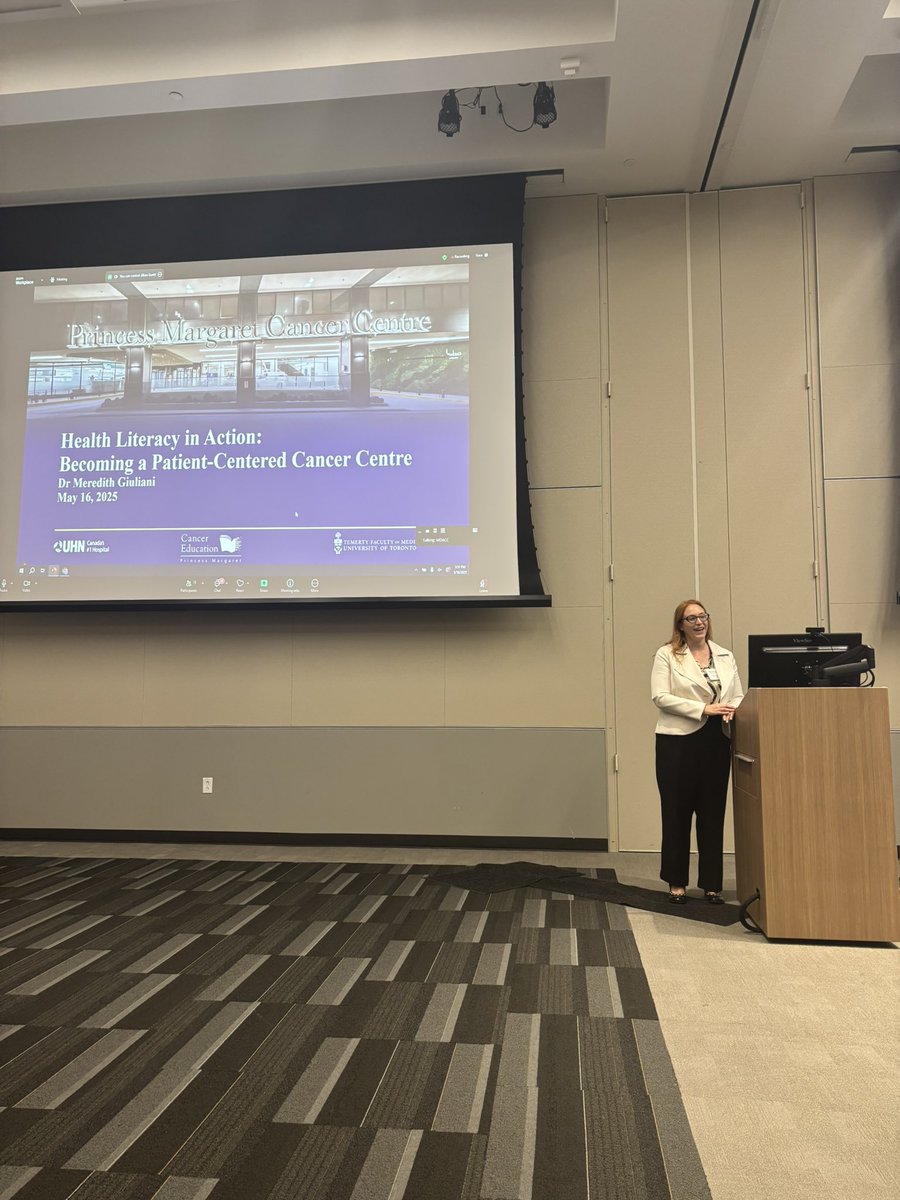
Patient Education @JieJaneChen
AI @leah_minnie

1
2
334
ROECSG (Rad Onc Education Collab Study Group) retweeted

May 15
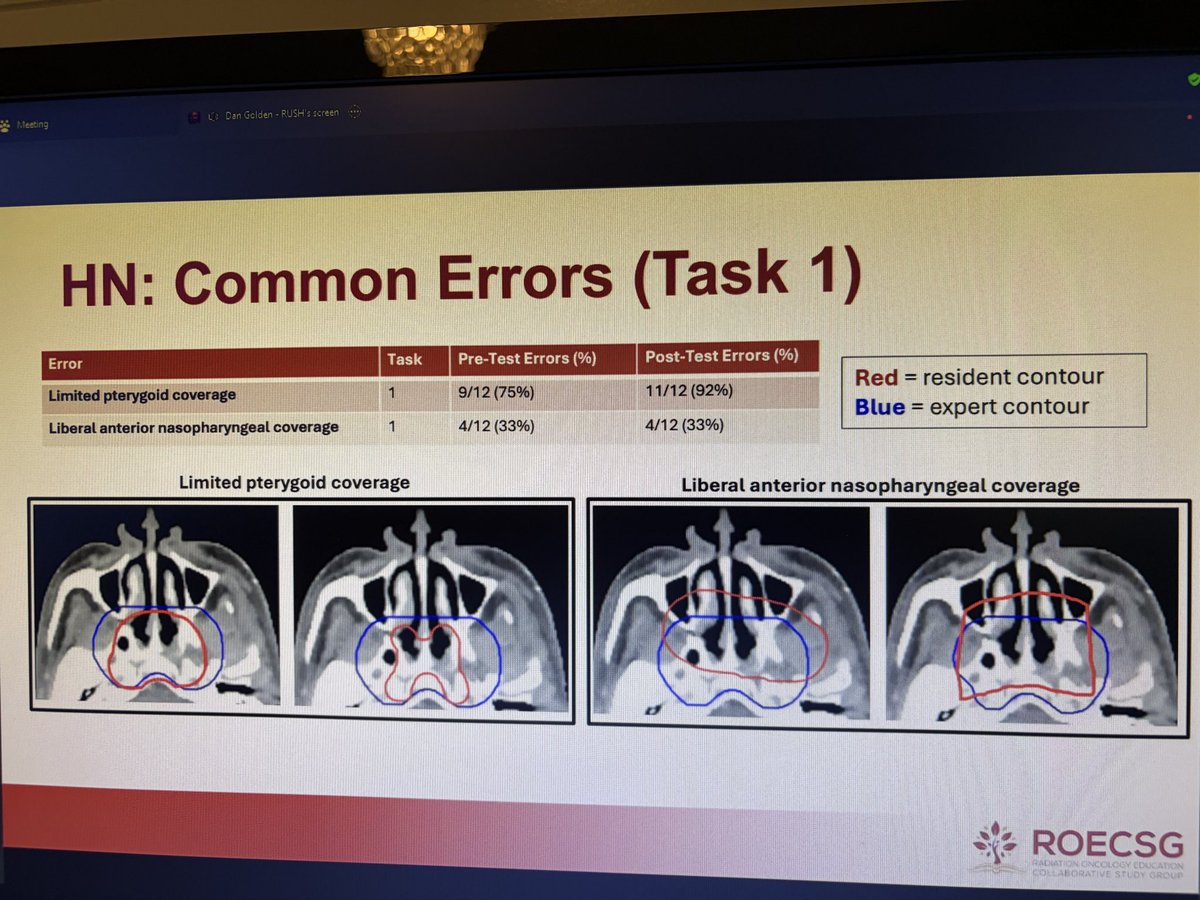
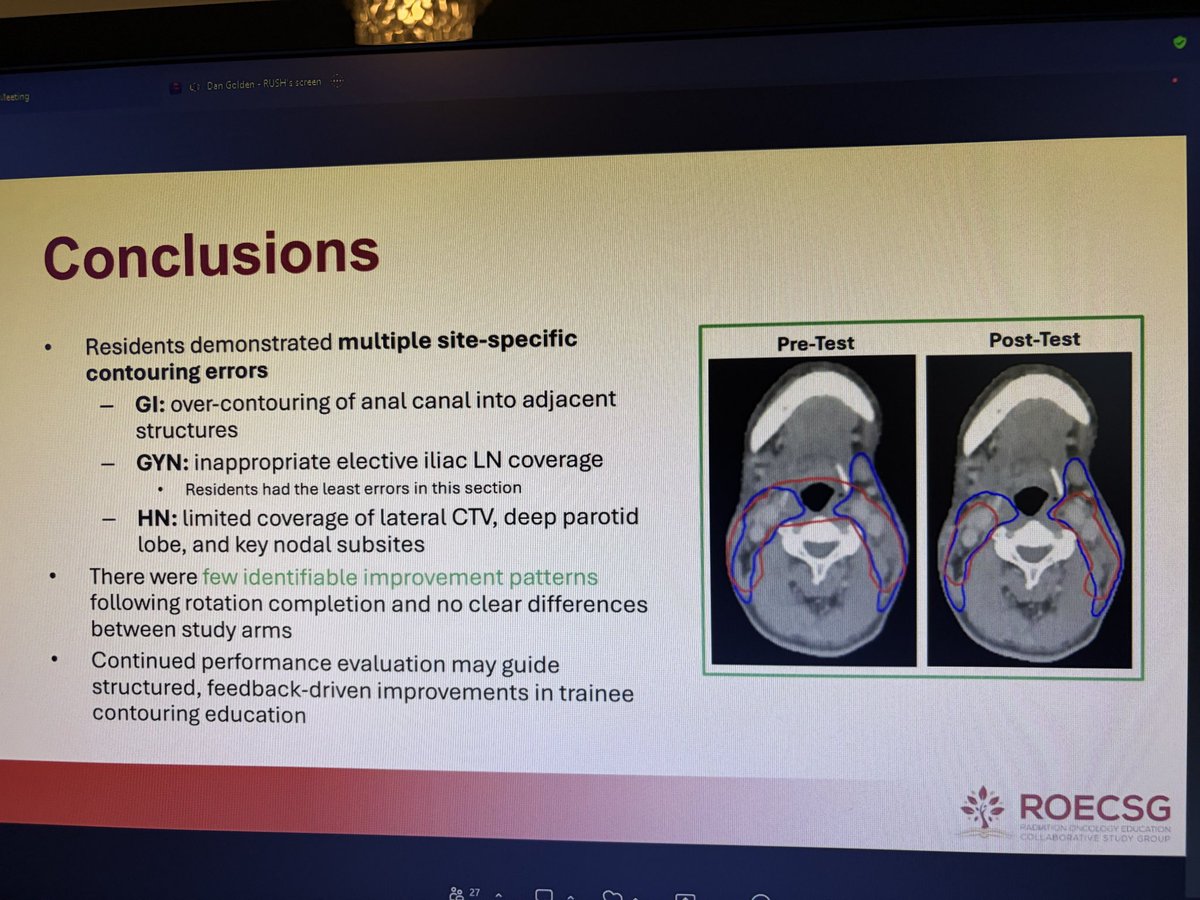
Great talk from @UCSDRadMed MS4 Hieu Nguyen on our contouring education work at @roecsg 2026
1
4
297
Excellent inaugural patient advocate session #ROECSG2026 with Morgan Newman, moderated by @allisongardaMD
Discussion on the patient experience and needs for patient engagement through the treatment 🩹 and survivorship 🗓️
2
3
291
Off to the races #ROECSG2026 @MayoClinic with introductory remarks from our @roecsg chair @d_golden and symposium chair @allisongardaMD

2
106
Schedule 📆 for our Annual ROECSG Spring Symposium below 👇
roecsg.org/symposium2026/
1
2
268
⏰🚨There is still time to register for our Annual ROECSG Spring Symposium 2026 happening this friday (5/15) - hybrid options including in-person in Rochester @MayoClinic @MayoRadOnc or virtually 💻
See you there!
redcap.rush.edu/redcap/surve…
3
194
ROECSG (Rad Onc Education Collab Study Group) retweeted

Mar 8
Radiotherapy Review in NEJM:
“Underuse and refusal of indicated radiotherapy have been shown to increase cancer-specific mortality and the risk of death in both curative and palliative settings”
nejm.org/doi/full/10.1056/NE…
2
48
136
8,294
ROECSG (Rad Onc Education Collab Study Group) retweeted
Feb 19
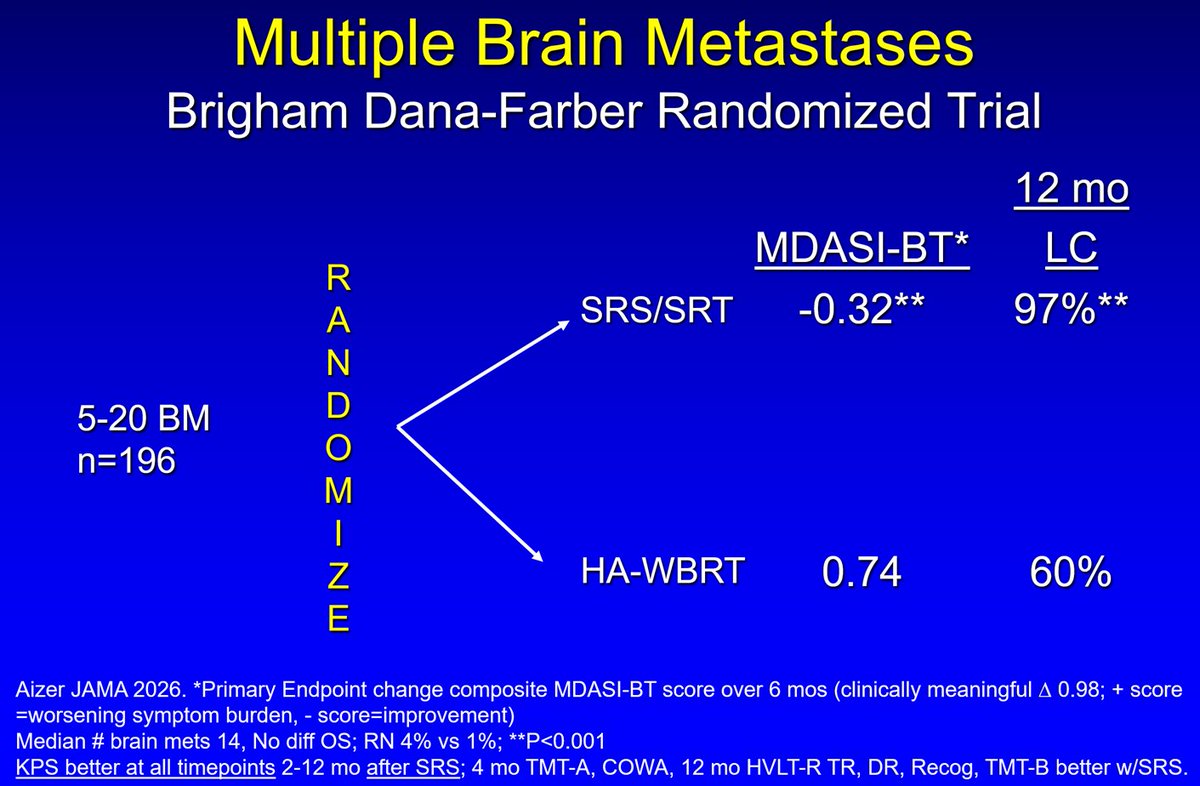
🚨🚨Multiple Brain Mets Randomized Trial🚨
· Significantly less symptom burden with SRS compared to HA-WBRT
· Better ADL, cognition & KPS after SRS
· SRS Standard of Care 5-20 brain mets
jamanetwork.com/journals/jam…
7
55
120
18,596
ROECSG (Rad Onc Education Collab Study Group) retweeted

Did you read get a chance to read one of our latest on 🧒🏽resident versus 👩🏽⚕️faculty 💭perceptions of treatment planning review🖥️ by @RachelJimenezMD & team?
advancesradonc.org/article/S…
Once you read it 👆🏽, check out the editorial 👇🏽by our #MedEd expert @d_golden!
Part 1️⃣:
🚀Congrats to Boyd et al on an important study examining how radiation oncology trainees learn radiation treatment plan (RTP) evaluation in the US.
This is core competency work—and long overdue. 👏
📊 Study design: Survey of residents faculty at 14 ACGME-accredited hashtag#radonc programs about RTP evaluation education.
Survey included:
✅ multiple choice
✅ Likert responses
✅ free-text responses
📬 Survey distribution:
👩⚕️ 169 residents
👨🏫 79 faculty
Response rates:
📌 Residents: 43%
📌 Faculty: 28%
For this population, that’s a reasonable response rate.
⭐ Key finding: Residents report substantially less RTP education than faculty report providing.
56% of residents felt they had inadequate exposure to RTP review.
Yet…
🧠 85% of faculty reported reviewing ≥50% of treatment plans with residents.
That’s a striking discrepancy.
🧑⚕️ Important nuance: PGY5s report adequate exposure (as shown in Figure 1).
So exposure may improve with seniority—but the earlier years matter too.
🧠Competency perceptions diverged as well:
More than half of residents did not feel competent in RTP evaluation
vs
~90% of faculty felt residents were competent
That gap matters for training confidence and readiness🏃🏽♀️.
🧩 This isn’t unique to radonc.
Similar “learners report less teaching than teachers report delivering” patterns exist across education research.
This is often called a “perception gap.”
Why does the perception gap happen❓
Because learners don’t always experience certain activities as “teaching,” even if educators believe they are teaching in the moment.
🔥 Key concept: Feeling of learning ≠ actual learning.
Students may feel they’re not learning during active engagement—even when measurable learning improves.
So subjective impressions must be interpreted cautiously.
Boyd et al also identified common barriers to RTP evaluation:
⏰ time constraints
📅 schedule misalignment
📈 competing clinical demands
😐 lack of interest (either party)
Classic “education vs workflow” collision.
Some barriers are fixable with intentionality.
Example:
Faculty can set aside protected RTP review time daily/weekly. Even if a plan is already approved, reviewing it still has huge educational value.
⚠️ As with all survey studies, bias is a risk:
📌 Response bias:
- Residents who feel undertaught may be more likely to respond
- Faculty who value teaching may also be more likely to respond
Another important limitation: social desirability bias.
Faculty may feel pressure to report higher teaching engagement because “good educators teach.”
This could inflate reported teaching frequency.
So what can we do with these findings?
🚨First: teaching & learning is a two-way street.
Faculty should be explicit about when they are teaching RTP evaluation—not just doing it.
Example:
Running into dosimetry, quickly reviewing a plan, then sprinting out 🏃♂️.
…may not register as teaching to a resident.
But simply reframing can change everything.
Try saying:
🗣️“Let’s take 2 minutes to review this plan and discuss how we approach it.”
Same activity. Totally different educational signal. ✅
Structure helps.
Faculty are encouraged to use a rubric-based verbal framework (ex: FCB-CHOPS) to guide consistent plan review teaching.
Consistency builds pattern recognition.
Why rubrics work:
1️⃣When residents repeatedly hear a structured process, they internalize it.
2️⃣Over time they develop their own mental checklist for RTP evaluation.
That translates into:
📌 competence
📌 confidence
📌 independence
🛑But it’s not all on faculty.
Residents: you can also proactively engage educators.
Ask for structured review:
☑️“Can we quickly walk through this plan using the rubric?”
(Respectfully… and preferably not while your attending is juggling 17 fires 🔥)
Residents should also seek other expert educators:
💡 dosimetrists
💡 physicists
Many are thrilled to teach—and often have unique perspectives on plan quality and tradeoffs.
🎯 Bottom line:
Boyd et al highlight that RTP evaluation—an essential residency skill—may be undertaught or under-recognized as being taught in many programs.
Take-home message for 👩🏽⚕️faculty:
✅ Engage residents in plan review intentionally
✅ Label teaching explicitly
✅ Use structured frameworks consistently
Take-home message for 🧒🏽residents:
✅ Be proactive
✅ Request structured review
✅ Learn from the entire team (physics/dosimetry included)
👏 Overall: Important study actionable implications.
If we want confident independent attendings, we need deliberate, visible, consistent RTP evaluation education—starting early.
#RadOnc #MedEd #ResidencyTraining #RadiationOncology
@ASTRO_org
4
8
1,043

Calling Global Radiology Educators! 📢
The Derek Harwood-Nash International Fellowship offers 6–12 weeks of study at leading North American institutions, with funding support and opportunities to build lasting collaborations.
Enhance your expertise. Bring new knowledge home.
Apply by July 1: bit.ly/48RJBoI

9
34
4,155
📢#ROECSG26 Spring Symposium abstract submissions are due on Monday 2/23/26. Check out the link below for information about the upcoming symposium including abstract guidelines, an amazing keynote speaker, and date/location details (5/15/26 @MayoClinic @MayoRadOnc).
#radonc #meded
roecsg.org/symposium2026/
4
4
597

Last day to apply is TOMORROW 2/13! Join ARRO exec!

🚨It's time for nominations for the 2026-2028 ARRO Executive Committee!
Current PGY-2 and PGY-3 residents - apply via email by Friday Feb 13th! See below for more information:
nam12.safelinks.protection.o…
4
3
952