
CEO Brightsquid, Lawyer, Columbo Aficionado, Pizza Expert, Parent
Joined December 2008
- Tweets 1,348
- Following 447
- Followers 352
- Likes 864
49 Photos and videos











Rohit Joshi, MSc. JD retweeted

21 Feb 2025
You can’t take our country — and you can’t take our game.
48,124
43,753
368,972
55,042,550
Rohit Joshi, MSc. JD retweeted

3 Feb 2025
Starting today and until U.S. tariffs are removed, Ontario is banning American companies from provincial contracts.
Every year, the Ontario government and its agencies spend $30 billion on procurement, alongside our $200 billion plan to build Ontario. U.S.-based businesses will now lose out on tens of billions of dollars in new revenues. They only have President Trump to blame.
We’re going one step further. We’ll be ripping up the province’s contract with Starlink. Ontario won’t do business with people hellbent on destroying our economy.
Canada didn't start this fight with the U.S., but you better believe we're ready to win it.
19,720
8,430
68,446
8,031,550
Rohit Joshi, MSc. JD retweeted

5 Aug 2024
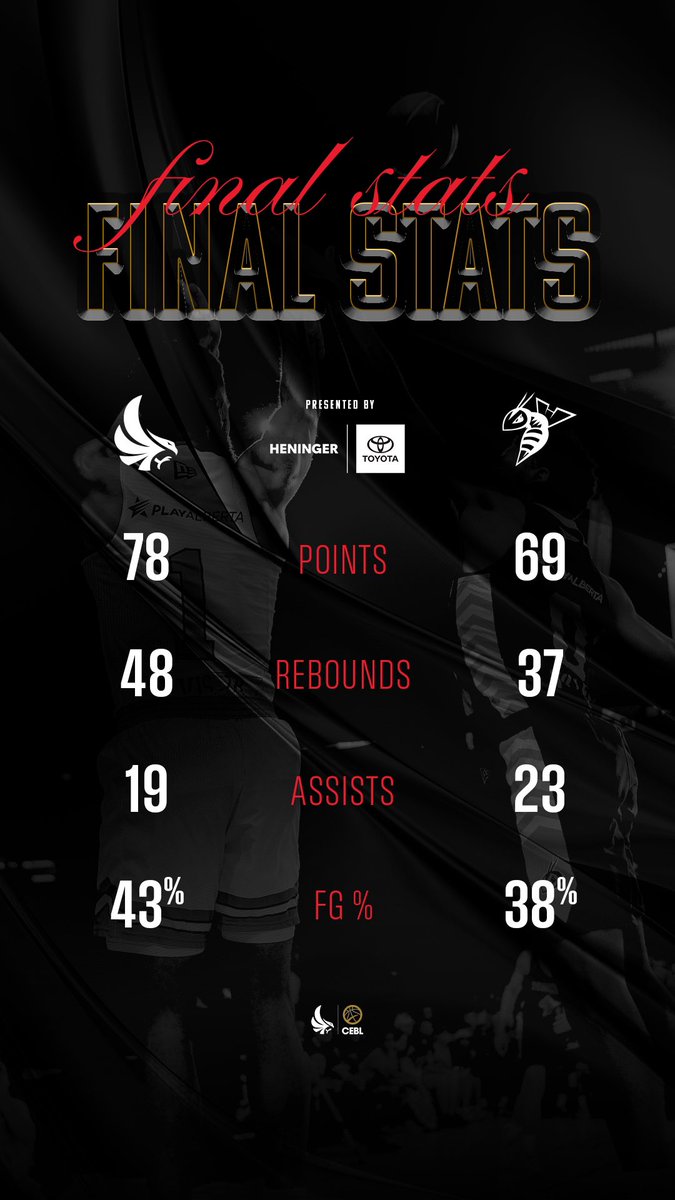
FINAL STATS PRESENTED BY @HeningerToyota. 🚗
#HomeTeam
2
21
994

Rohit Joshi, MSc. JD retweeted

26 Nov 2023
You really sparked a conversation @jflier, comments show the opposing points of view pretty well.
Best advice from my program director at @usask as a resident was that an MDs impact must be rooted in being clinically excellent.
12 years of rural practice has taught me however that folks who don’t see and address the inequitable circumstances that patients experience due to geography, socioeconomic status, racism, sexism, ableism, language, trauma, being labelled a problem patient, among many others are:
- at best, achieving less excellent care than they could
- at worst, being really crappy clinicians who cause harm with or without realizing it
Case in point, surgical teams who discharge patients post surgery to places where there’s no running water and instruct them to keep their wounds clean.
We have to find a way to do both, but you can’t be an excellent clinician without seeing and mitigating your patients life circumstances as best you can.
Imagine a lot of folks pick this up if they find good clinical mentors, but may have never framed it as an outcome of equity, diversity and inclusion.
24 Nov 2023

For a medical society, or a medical school, to prioritize "social justice" over medical expertise is to declare themselves unfit for their professional roles.
16
46
195
71,747

13 Oct 2023
I’ll miss the long dash too - but it was never at 1pm. (Alberta)
11 Oct 2023

I'll sure miss the long dash.
92
Rohit Joshi, MSc. JD retweeted

12 Oct 2023
Wow, what a day!
Thank you to everyone who joined us, and to all of our moderators and panelists for providing such valuable insight for our community!
A special thank-you to our lunch sponsor, @albertacounsel; and our event supporters, @EdmontonUnltd and @kiwiProAV!
#yegSW23

2
6
216
Rohit Joshi, MSc. JD retweeted
4 Oct 2023
Edmonton Startup Week begins next week! With 5 days of workshops, presentations, and socials, there will be plenty of opportunities to engage with the Edmonton Region's talented and innovative minds.
Interesting in health? Check out our event on Oct 11 ➡️ bit.ly/3Q2vQfD

4 Oct 2023

The excitement is building! Getting ready to celebrate 10 years of Edmonton Startup Week with @EdmontonUnltd and support from @ABInnovates! #startup #Yeg #Innovation #HealthTech

1
2
6
858

Library Drops Dewey Decimal System By Organizing All Titles Under ‘B’ For Books bit.ly/46cDv1a

36
725
8,158
879,900
18 Jun 2023
I lost a family member to ALS and I know first hand what incredible determination you and your family have to “Improvise and Overcome”. Well done Chris & family.
18 Jun 2023

I did today what the doctor suggested 4 years ago on this day. Watched my son’s Little League playoff game. Listened to a podcast while lying in the sun. Worked on my laptop, Cut the grass. That is, I did what brings me joy. Year 4 living with #ALS cut that list down. A lot. 1/3

87
5 Jun 2023
Congratulations to my son Arjun Joshi on his convocation last week from the University of Calgary. Special shout out to the University of Calgary Chancellor Jon Cornish, CFA for making one of his biggest fans feel extra special. lnkd.in/g-9GpN7B
57
24 May 2023
Wishing the Surge all the best for their inaugural game on Sat afternoon. See you there! lnkd.in/gA-DQ3W2
25
Rohit Joshi, MSc. JD retweeted

10 May 2023
I assumed the anger on my timeline over Canada’s new passport was overblown but it’s not. This is outrageous.
It’s so big.
Who approved this.

302
234
2,571
228,245
Rohit Joshi, MSc. JD retweeted

4 May 2023
Thank you @bchimss for giving me the opportunity to lead the discussion on the enabling innovation. I had so much fun with the panel and appreciate how open and honest the discussion was! This demonstrates the true value of the public-private-academic partnerships!

Wow! This is a great group of panelists moderated by @chrisjcarvalho to discuss Healthcare Innovation Enablers
Featuring Luke Brodie, Ka-Hay Law, Kevin Samra, Matthew Millar, Dr.Sylvain Moreno
#bchimss2023

1
6
179
Rohit Joshi, MSc. JD retweeted

12 Apr 2023
April 12 is the International Day of Pink! The 2SLGBTQIA community is no stranger to the bullying and violence that stem from hateful beliefs. Discrimination harms, diversity strengthens! United, we stand a chance.
#DayofPink
#LGBTQ
#mentalhealth
#antibullying
#pride

1
2
136
Rohit Joshi, MSc. JD retweeted

12 Mar 2023
After conferring with his mentor via zoom, Barney makes his pitch to @UCalgary VPR, @WilliamGhali, for a research chair to advance work on the mental health benefits of belly rubs & shoe destruction. #academia #dogs #SundayVibes

2
3
28
1,818
Rohit Joshi, MSc. JD retweeted

21 Feb 2023
In budget 2023, Alberta's government is proposing to invest over $2 billion to strengthen the province's primary health care system - the most ever in Alberta's history. Modernizing the health care system will stabilize and strengthen primary health care across the province.

62
43
139
46,057
Rohit Joshi, MSc. JD retweeted
13 Feb 2023
This deserves a retweet.
13 Feb 2023

Previously unseen footage of antibodies on their way to fight an infection
3
17
125
18,753
Rohit Joshi, MSc. JD retweeted

13 Feb 2023
I have a 9-year old pal with special needs who loves his truck. But it has stopped working and they don’t make them anymore. Anyone have one they would be willing to part with to make him happy?

ALT Toy yellow truck.
45
357
943
337,083