
221 Photos and videos












Rubén retweeted

May 31
🇬🇧 | El King's College Hospital en Londres ha inaugurado un jardín en la azotea para pacientes de cuidados críticos. Su primera paciente dijo que el espacio al aire libre le dio «un verdadero impulso para seguir adelante».
28
769
15,084
888,700
4 años de residencia que ya acaban. Feliz del viaje compartido y de todo lo aprendido. Nada acaba aquí, todo empieza.

No me lo creooo 🙈 Residente de Anestesiología y Reanimación en el Hospital Universitario Ntra. Sra. de la Candelaria, Tenerife!! 🥹😍 Vuelvo a una maravillosa tierra con muchas ganas e ilusión!

7
2
56
5,709
La salud mental entre residentes no es un problema futuro, ya está entre nosotros. Conviene, además de escuchar, actuar desde las instituciones para mejorar las condiciones laborales. Pasar del discurso a los hechos.
7
14
881
Rubén retweeted

May 26
Un residente de Anestesiología del Hospital Universitario de Canarias (Tenerife) ha perdido la vida, elevando a tres las muertes de médicos en formación en España durante este ejercicio.
La @AsociacionMIRe enmarca la tragedia en unas condiciones laborales críticas ➡️ tinyurl.com/5kyk54mb
17
111
211
35,949
Rubén retweeted

May 4
Corregir en privado y felicitar en público. Por ejemplo.

7
28
1,045
114,621
Rubén retweeted

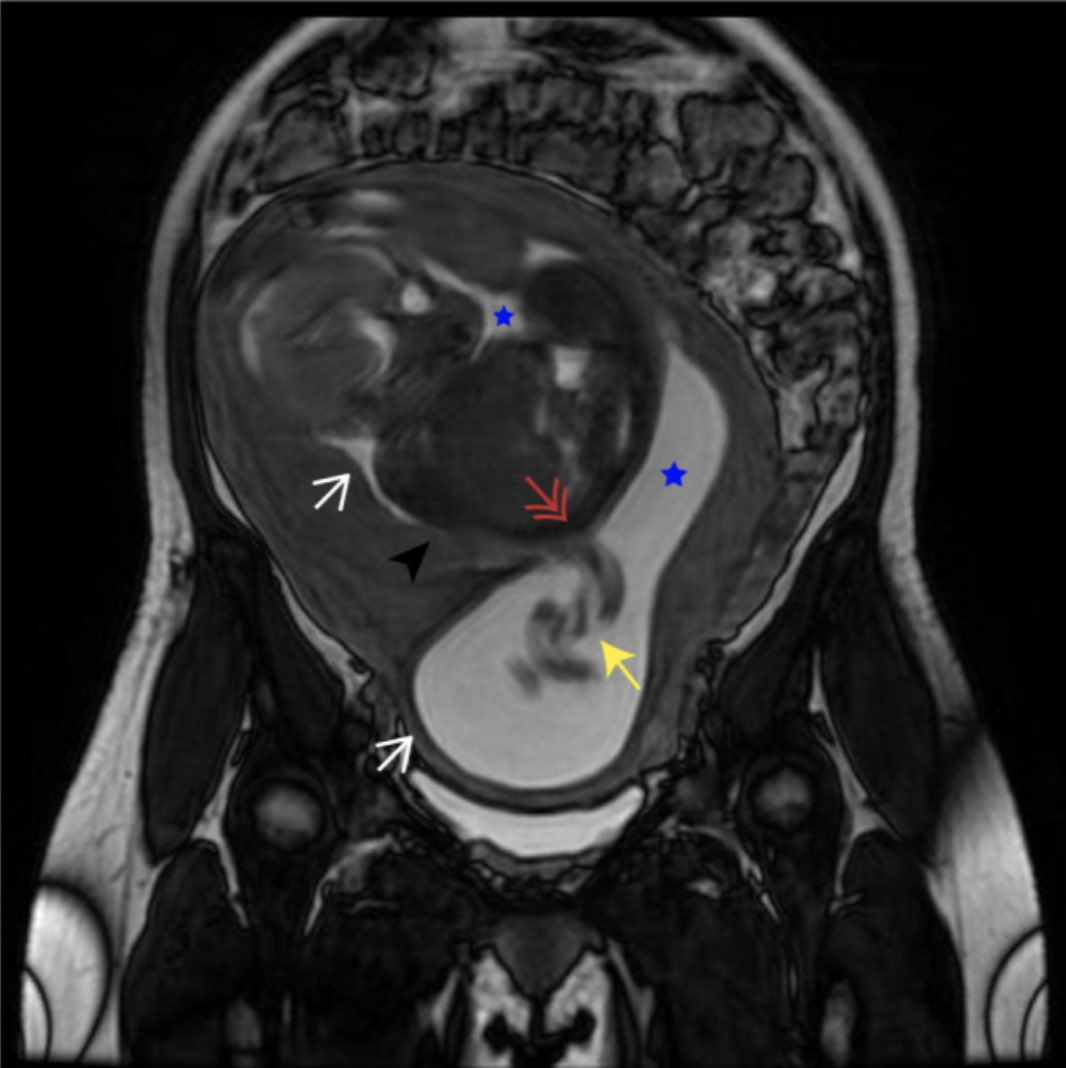
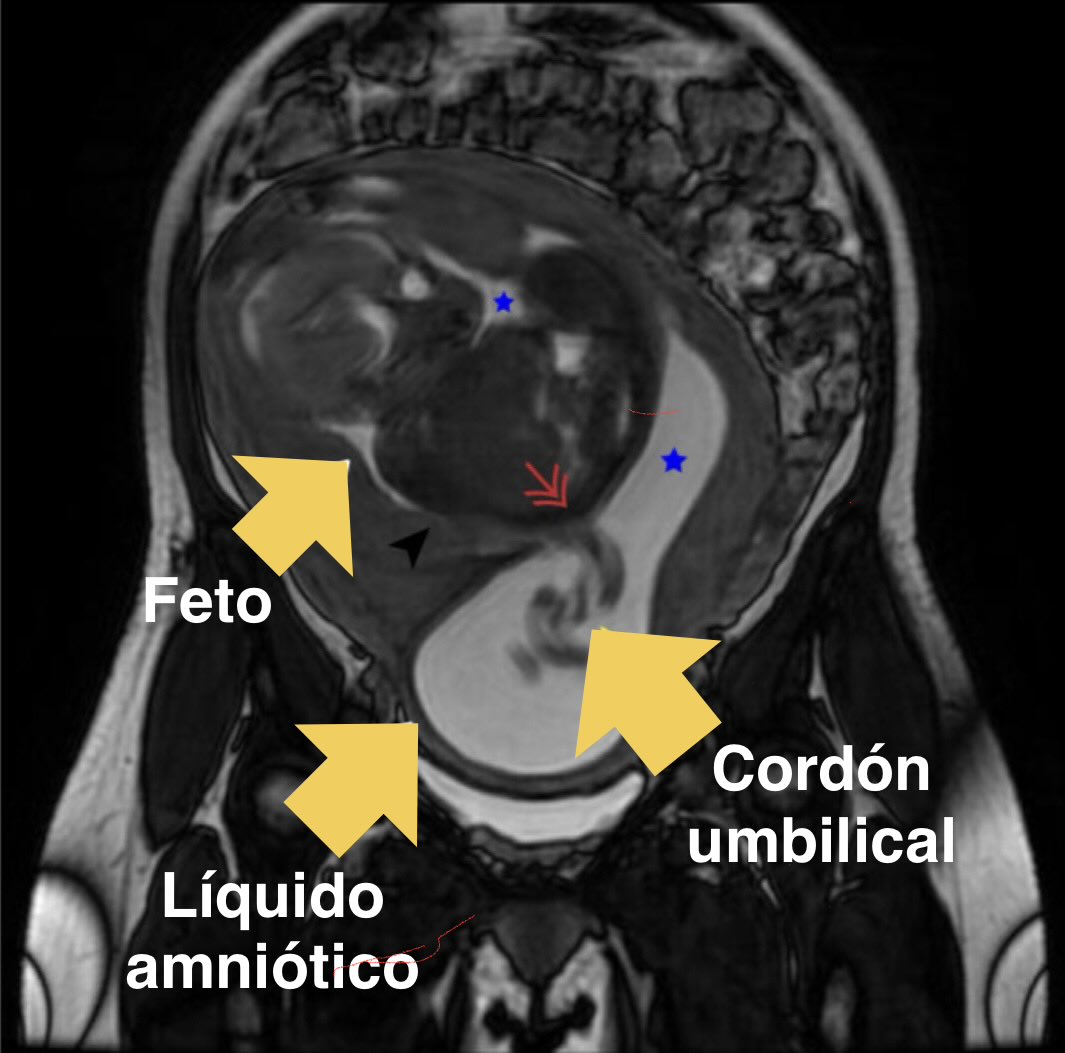
⚠️ Embarazo de MUY ALTO RIESGO  debido a una anomalía realmente excepcionaL... ¿sabrías decir cuál? 🤔
Hoy hablamos de un caso, absolutamente excepcional… pero afortunadamente, con final feliz 🤱🏻
Dentro #hilo 🧵🔥🔥🔥
#Obstetricia #CasoClínico
1
3
19
3,865

Among survivors of intracerebral hemorrhage, a single pill with three low-dose antihypertensive agents added to standard care was associated with a lower incidence of stroke and major cardiovascular events than placebo. Full TRIDENT trial results: nejm.org/doi/full/10.1056/NE…
Editorial: Blood-Pressure Control after Intracerebral Hemorrhage — An Unbroken Glass Ceiling nejm.org/doi/full/10.1056/NE…
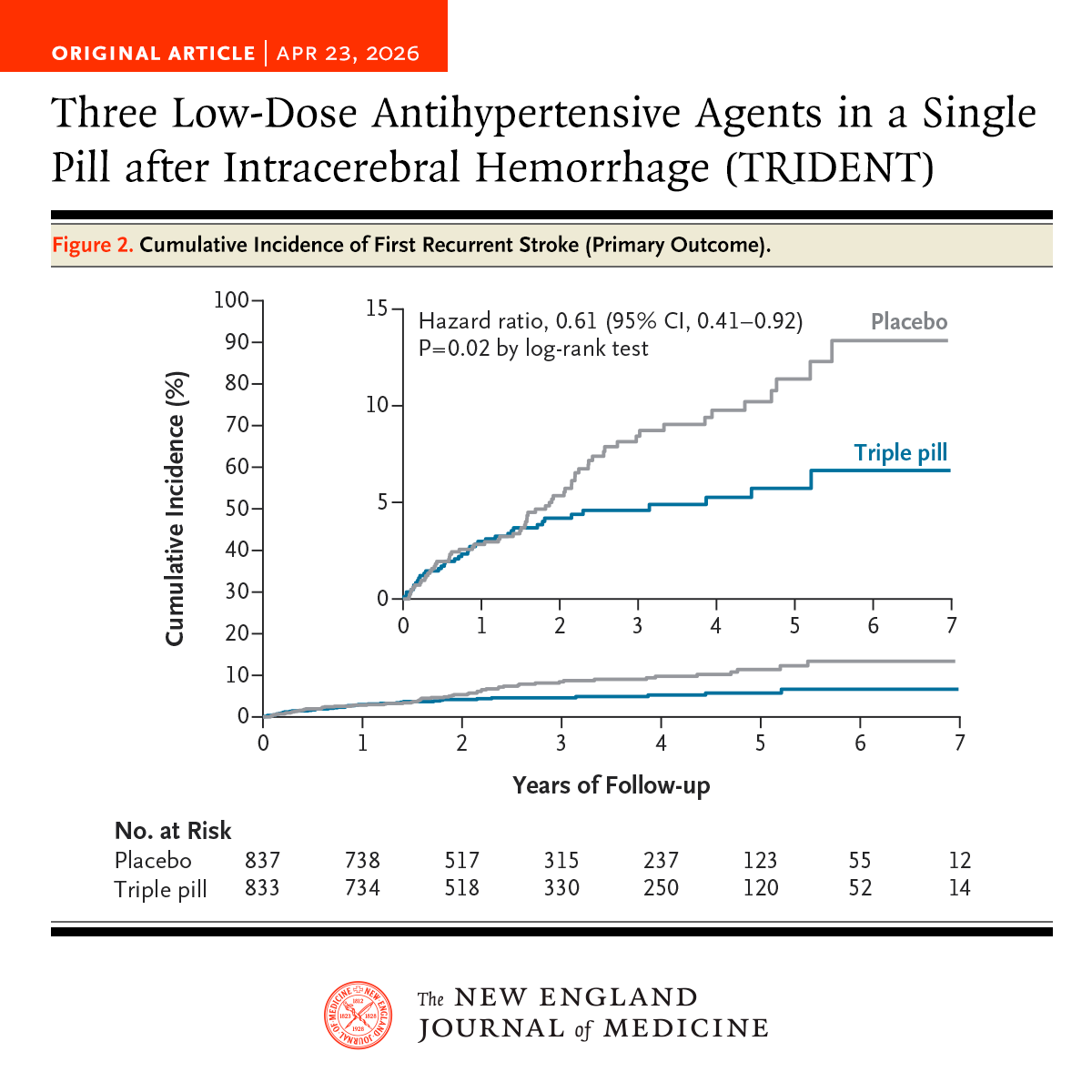
ALT Original Article | APR 23, 2026 Three Low-Dose Antihypertensive Agents in a Single Pill after Intracerebral Hemorrhage (TRIDENT) Figure 2. Cumulative Incidence of First Recurrent Stroke (Primary Outcome).
2
121
340
48,018
Rubén retweeted

Apr 20
I wrote this in a moment I never would have chosen. A sudden pause that made me see my life clearly.
The meaning of our work is profound. This experience simply helped me see more clearly what matters most.
“Time is Finite” JAMA
jamanetwork.com/journals/jam…
60
359
1,655
657,462
Rubén retweeted

Apr 18
Examiner les pupilles de quelqu’un après un trauma crânien pour savoir si c’est grave ou pas, si le quelqu’un n’est pas déjà inconscient par terre, ça ne sert à rien.
Un peu de neurologie à dérouler… patiemment
👇🏻
Apr 16

Nurse spots the danger, stops the fight, and gets booed by the crowd. She still smiled knowing she just prevented a tragedy!!
54
226
2,163
837,965
Rubén retweeted

Lo mejor que he visto escrito en JAMA hace años…

5
160
596
20,693
Rubén retweeted

💧 Albumin in the ICU: life-saving drug… or expensive myth?
We’ve been using it since the 1940s.
Yet in 2026 we still don’t fully agree when it actually helps.
🧠 First principle
Albumin is NOT just a volume expander.
It does much more:
▪️ Maintains oncotic pressure
▪️ Protects endothelium & glycocalyx
▪️ Modulates inflammation
▪️ Alters drug pharmacokinetics
➡️ It’s a biologically active molecule, not “fancy saline”
⚠️ The uncomfortable truth
👉 50-70% of albumin use is inappropriate
👉 In some studies: >90% misuse
Yes… even in modern ICUs
🔥 Where albumin actually WORKS
✔️ Hepatorenal syndrome (HRS)
→ Albumin terlipressin = better renal outcomes
✔️ Spontaneous bacterial peritonitis (SBP)
→ ↓ AKI ↓ mortality
✔️ Large-volume paracentesis
→ Prevents circulatory collapse
⚖️ Where evidence is… mixed
🟡 Septic shock
→ No mortality benefit vs crystalloids
→ BUT better hemodynamics in some patients
🟡 ARDS
→ Improves oxygenation (if hypoalbuminemic)
→ No survival benefit
🟡 Major surgery
→ ↓ fluids, ↓ complications
→ BUT watch renal risk (especially 20%)
🚫 Where you should think twice
❌ Traumatic brain injury
→ ↑ ICP
→ ↑ mortality
➡️ Albumin crosses disrupted BBB → worsens edema
💡 Key ICU insight
Albumin is NOT about:
❌ “giving protein”
❌ “correcting labs”
It’s about:
✔️ hemodynamics
✔️ endothelial integrity
✔️ patient selection
📉 Hypoalbuminemia matters
Every ↓10 g/L:
▪️ ↑ mortality
▪️ ↑ complications
▪️ ↑ length of stay
➡️ But correction ≠ automatic benefit
🎯 Clinical decision rule
Use albumin when:
✔️ Cirrhosis-related complications
✔️ Refractory shock after crystalloids
✔️ Severe hypoalbuminemia with instability
Avoid when:
❌ Routine resuscitation
❌ TBI
❌ “just low albumin”
🧠 Take-home
➡️ The question is NOT
“Does albumin work?”
➡️ The real question is
“In which patient, at which moment?”
📚 Rubio-Baines I et al. (2026)
Journal of Clinical Medicine
DOI: 10.3390/jcm15051981
ALT
1
86
290
18,553
Para reflexionar después del creciente aumento de problemas de salud mental en los últimos meses entre los médicos residentes, especialmente en Anestesiología.

Dos médicos estadounidenses (Simon G. Talbot y Wendy Dean) ya expresaron que el agotamiento que sufrían los médicos no era realmente burnout, sino que se trataba de un daño moral profundo.
"Para garantizar que médicos compasivos, comprometidos y altamente cualificados lideren la atención al paciente, los directivos del sistema sanitario deben reconocer y admitir que esto no es agotamiento profesional o burnout. Los médicos se están quitando la vida a un ritmo alarmante (el doble que en el ejército), lo que indica que algo funciona muy mal en el sistema.
La solución SIMPLE de establecer programas de bienestar para médicos... no resolverá el problema. Tampoco lo hará una atención basada en equipos, horarios flexibles, mindfulness, meditación, técnicas de relajación... Ninguna de estas medidas está orientada a cambiar los patrones institucionales que infligen lesiones morales...
Los médicos deben ser tratados con respeto, autonomía y la autoridad necesaria para tomar decisiones... Los mandatos de arriba-abajo en la práctica médica son degradantes y, en última instancia, ineficaces".
98

#CardioToVascSEDAR
📊 Según J Cardiothorac Vasc Anesth (2025), las desaturaciones cerebrales medidas con NIRS no se asociaron con delirium tras cirugía cardiaca
🔗 pubmed.ncbi.nlm.nih.gov/4000…
@JCVAonline

4
6
749
Rubén retweeted

Apr 16
🏥El Hospital La Candelaria incorpora un quirófano en Paritorio con una inversión superior a 650.000 euros
(va 🧶)
1
1
12
2,376
Rubén retweeted

In a multinational cohort of ARDS patients, PaO2/FIO2 ratio was not associated with mortality and had poor prognostic utility, while driving pressure (ΔP) and the 4ΔP RR index outperformed other variables in predicting mortality bit.ly/4gp3ZSo
1
12
45
4,709
Rubén retweeted

Desde la Organización Médica Colegial lamentamos profundamente el fallecimiento de un médico residente en Barcelona este fin de semana.
Trasladamos nuestro más sentido pésame a su familia, compañeros y amigos.
Todo es poco en el compromiso que debemos asumir para cuidar la salud mental de nuestros profesionales. No podemos mirar hacia otro lado.

7
33
80
12,107
Rubén retweeted
🫀 Diuretic Resistance in Cardiorenal Syndrome: Are We Treating the Wrong Target?
A recent review in Frontiers in Cardiovascular Medicine challenges a deeply ingrained paradigm in heart failure management:
👉 That congestion is simply a “fluid problem.”
In reality, diuretic resistance (DR) is not failure of therapy, it is failure of understanding physiology.
🔬 The Core Insight
Up to 1 in 3 HF patients will not respond adequately to loop diuretics.
But the mechanism is not just “insufficient dose.”
It is a multisystem adaptive response:
↓ Renal perfusion ↑ venous congestion
Tubular remodeling (distal sodium avidity)
Neurohormonal activation (RAAS, SNS)
Chloride depletion → a neglected driver of resistance
👉 We are not dealing with “volume overload”
👉 We are dealing with a sodium-retentive, neurohormonally activated organ
⚠️ The Clinical Mistake
We still rely on:
Weight
Fluid balance
Creatinine
These are late, indirect, and often misleading markers.
Meanwhile, the kidney has already adapted.
📊 The Paradigm Shift
The paper reinforces a critical transition toward:
1. Physiology-guided monitoring
Urinary sodium (UNa) at 1-2h
Urine output kinetics
POCUS (VExUS, lung ultrasound)
2. Mechanism-based therapy
Sequential nephron blockade
Chloride repletion (not just sodium restriction)
Early combination strategies
3. Phenotype-specific management
Not all HF is the same:
Right heart failure → venous congestion-driven DR
CKD → pharmacokinetic tubular limitations
Obesity → hidden congestion inflammatory sodium retention
Frailty → narrow therapeutic window
👉 Same drug, different physiology, different response
🧠 The Take-Home Message
Diuretic resistance is not a pharmacologic problem.
It is a systems physiology problem.
And until we treat:
Renal perfusion
Venous congestion
Electrolyte signaling (chloride!)
Patient phenotype
👉 We will continue escalating doses…
👉 …instead of improving outcomes.
🚀 My Perspective
We are moving toward a future where:
UNa replaces weight as the primary feedback loop
POCUS becomes mandatory, not optional
If you're managing HF patients daily:
Are you still chasing urine… or understanding the kidney?
📃Reference
Aletras, G., etc al. Frontiers in Cardiovascular Medicine, 12, 1731305.
doi.org/10.3389/fcvm.2025.17…
ALT
1
91
279
16,215
Rubén retweeted

El Hospital de La Candelaria, en Tenerife, cumple 60 años. El centro ha sido referente en trasplantes hepáticos.
👉 rtve.es/play/videos/telecana…
6
15
1,060